Investigation of Interactive Activity of Electro-Acupuncture on Pharmacokinetics of Sildenafil and Their Synergistic Effect on Penile Blood Flow in Rats

 , ,
, , 
Abstract
:1. Introduction
2. Results
2.1. Analytical Method Validation for Sildenafil
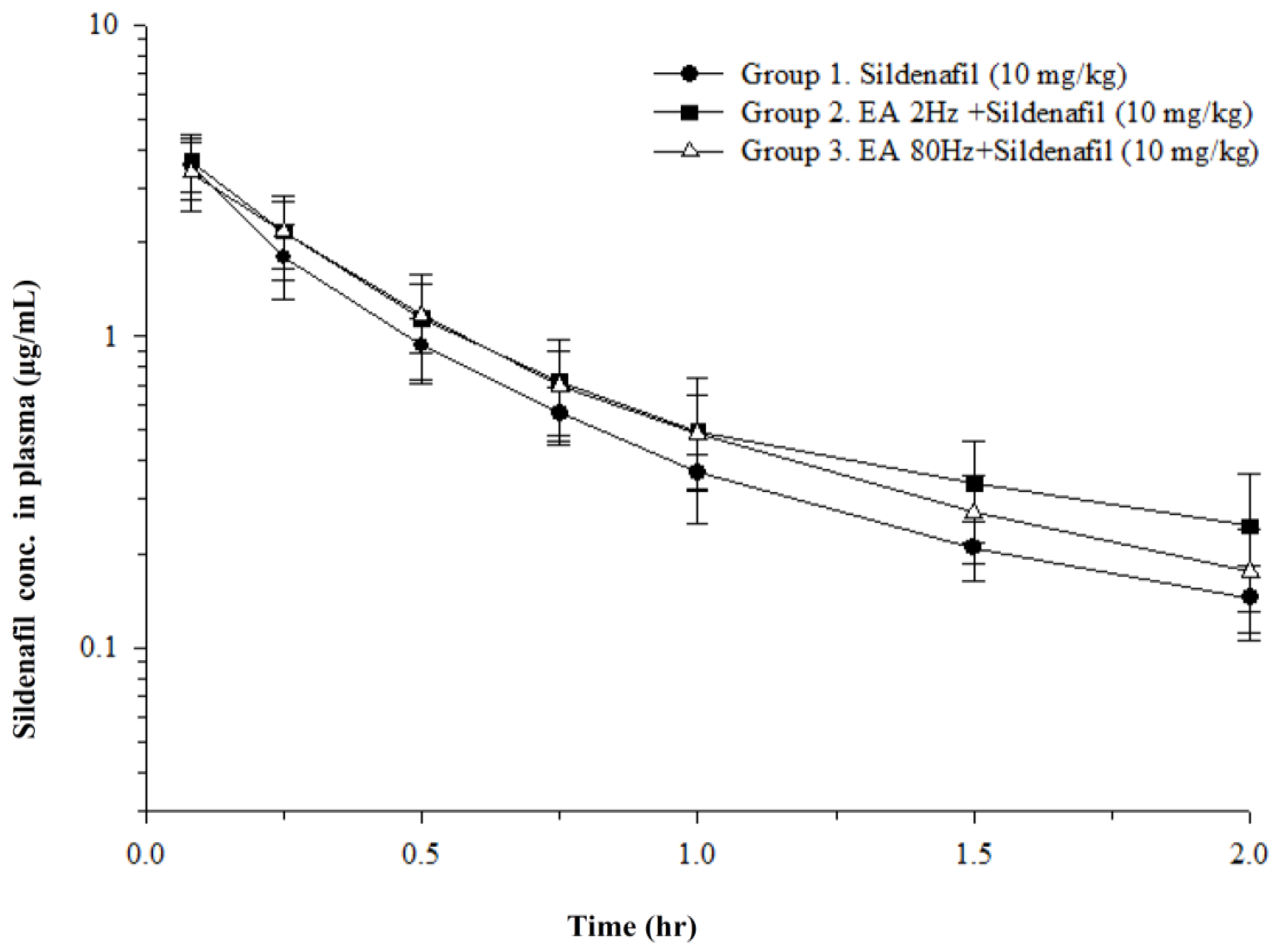
2.2. Effect of Sildenafil and EA on the Pharmacokinetic Parameters
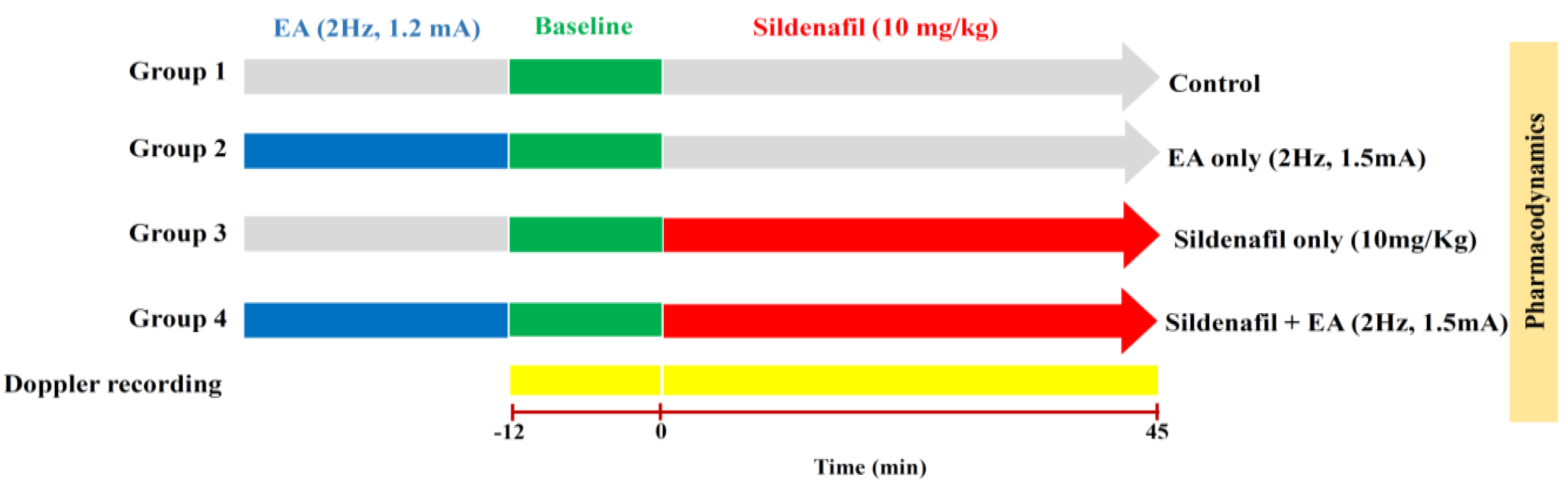
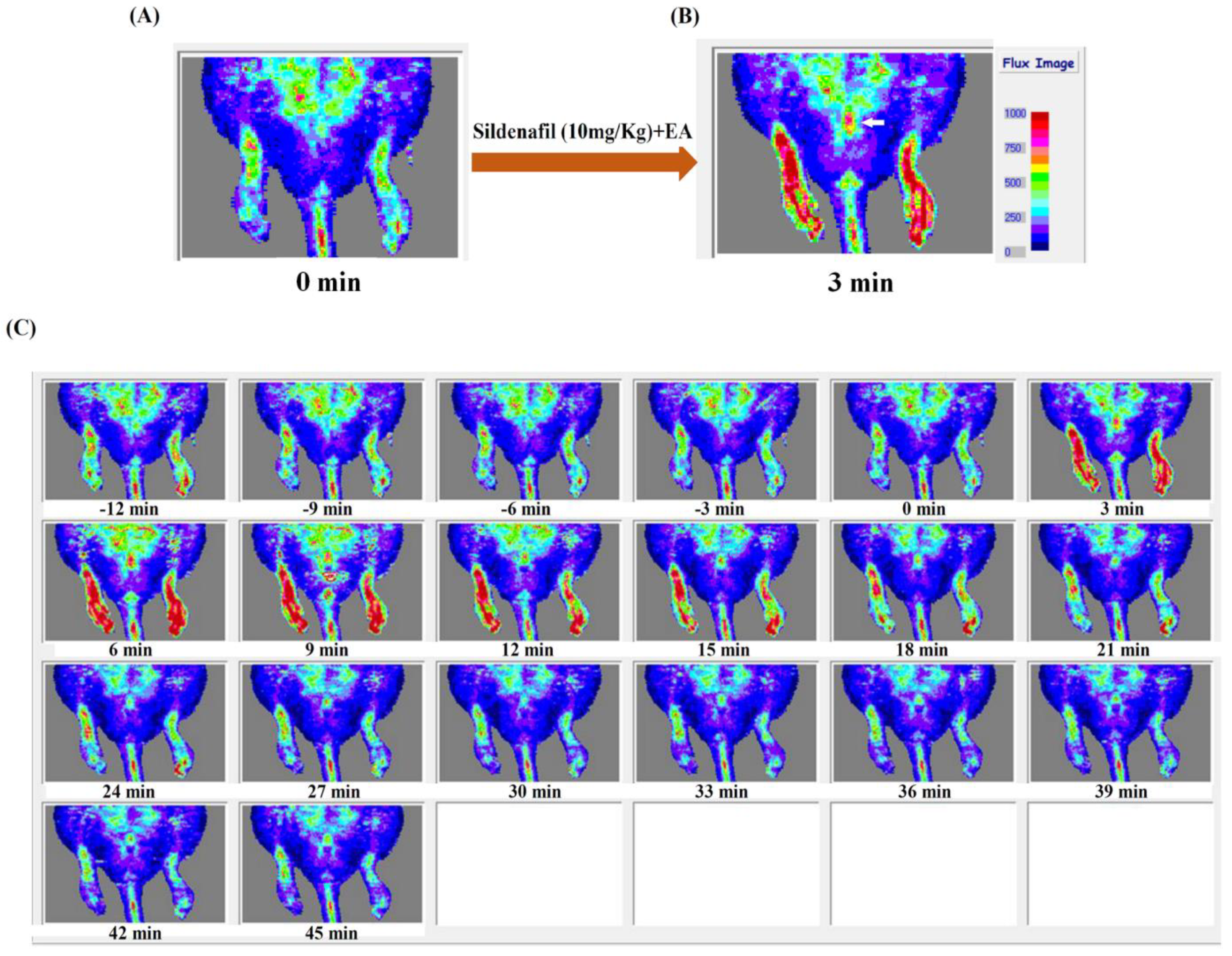
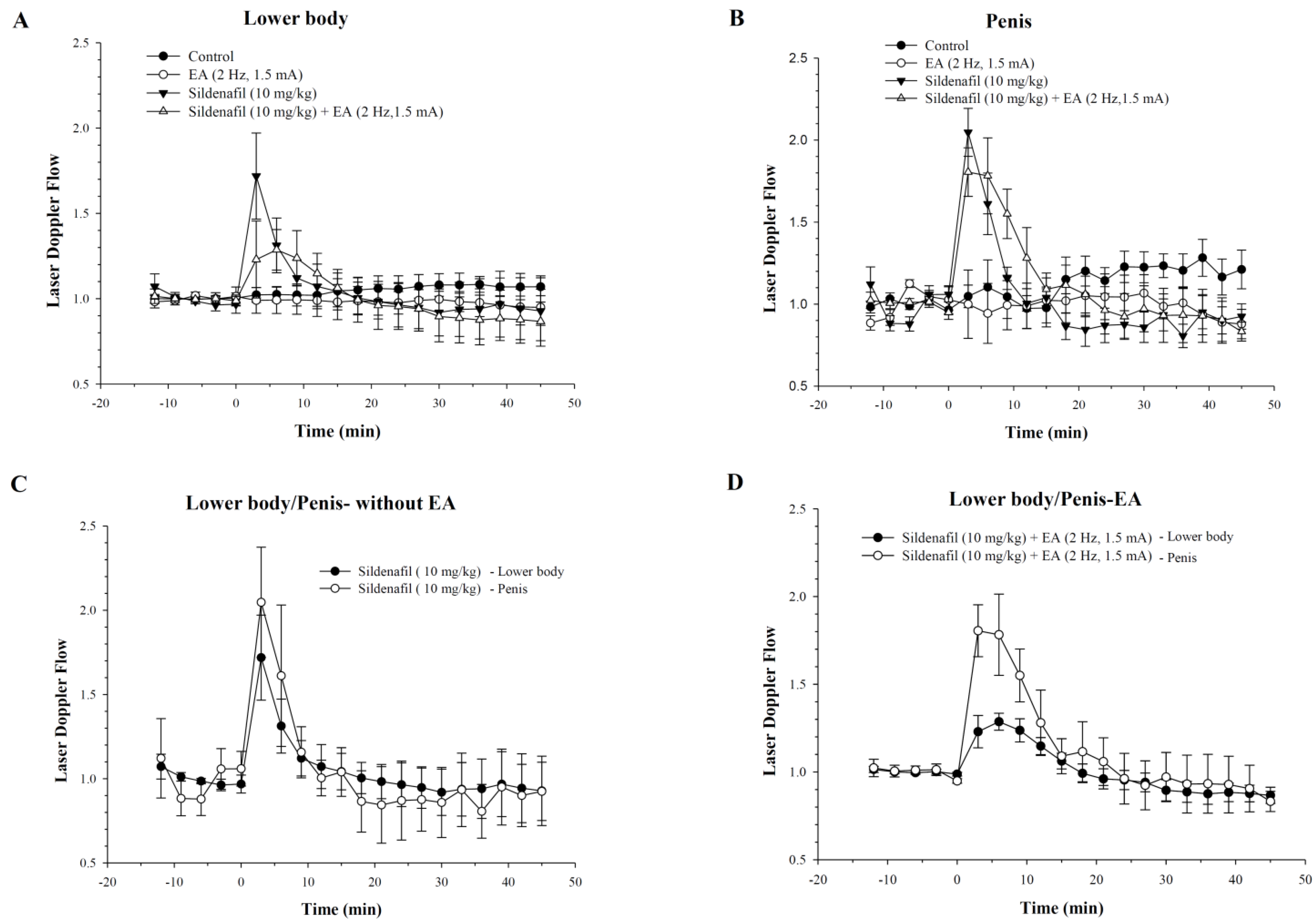
2.3. Efficacy of Sildenafil and EA on Pharmacodynamics Parameters
3. Discussion
4. Materials and Methods
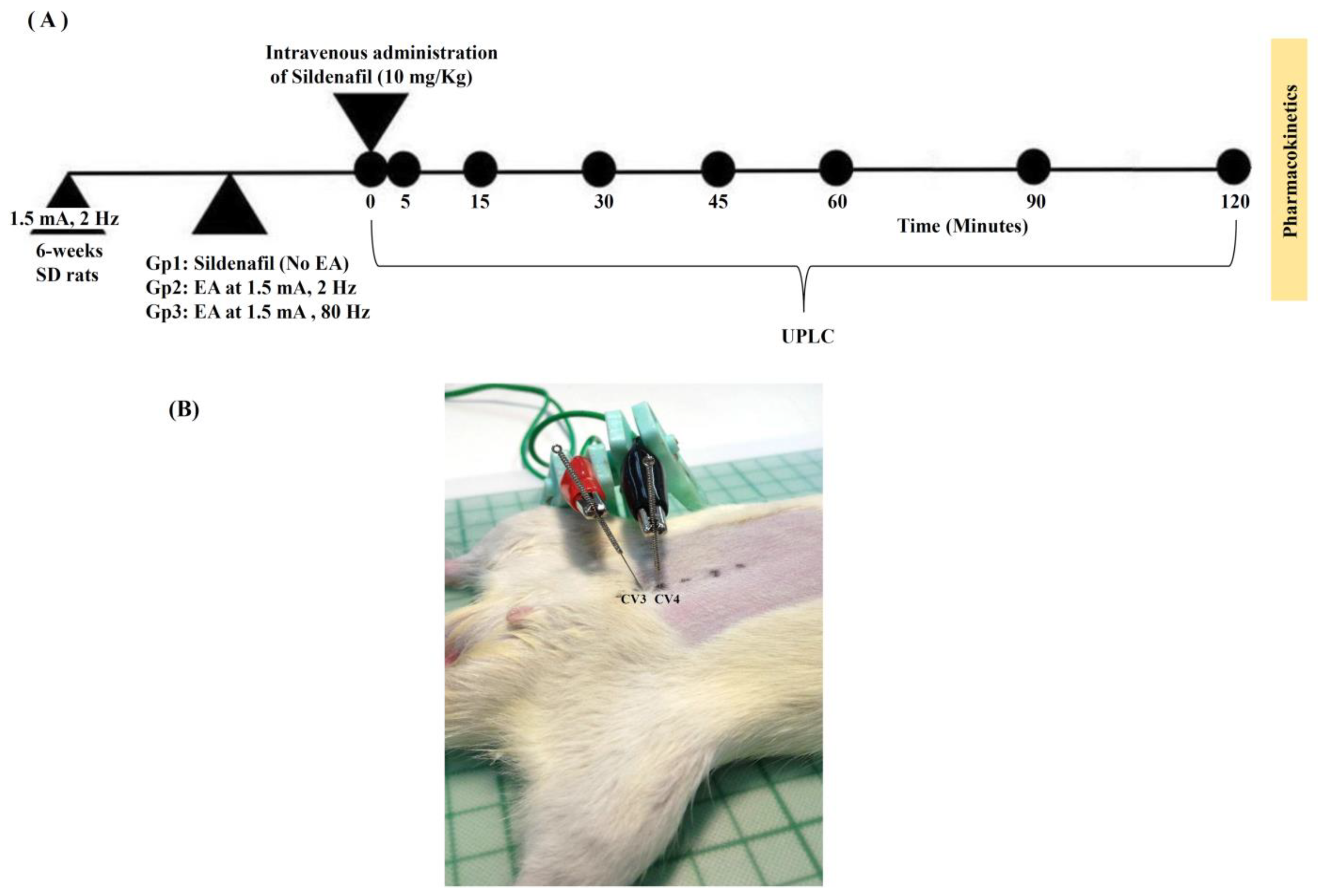
4.1. Animals and Study Design
4.2. UPLC-UV Instrumentation
4.3. Sildenafil and Electro-Acupuncture (EA) Administration
4.4. Pharmacokinetics Parameters
4.5. Measurement of Blood Flow in Lower Body and Rat Penis
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA 1993, 270, 83–90. [Google Scholar]
- McMahon, C.G. Erectile dysfunction. Intern. Med. J. 2014, 44, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Lue, T.F. Erectile dysfunction. N. Engl. J. Med. 2000, 342, 1802–1813. [Google Scholar] [CrossRef] [PubMed]
- Tharyan, P.; Gopalakrishanan, G. Erectile dysfunction. Clin. Evid. 2006, 15, 1227–1251. [Google Scholar]
- Cui, X.; Zhou, J.; Qin, Z.; Liu, Z. Acupuncture for Erectile Dysfunction: A Systematic Review. BioMed Res. Int. 2016, 2016, 2171923. [Google Scholar] [CrossRef] [PubMed]
- Lowe, G.; Costabile, R.A. 10-Year analysis of adverse event reports to the Food and Drug Administration for phosphodiesterase type-5 inhibitors. J. Sex. Med. 2012, 9, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Aung, H.H.; Dey, L.; Rand, V.; Yuan, C.S. Alternative therapies for male and female sexual dysfunction. Am. J. Chin. Med. 2004, 32, 161–173. [Google Scholar] [CrossRef] [PubMed]
- Mao, J.J.; Kapur, R. Acupuncture in primary care. Prim. Care 2010, 37, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Kho, H.G.; Sweep, C.G.; Chen, X.; Rabsztyn, P.R.; Meuleman, E.J. The use of acupuncture in the treatment of erectile dysfunction. Int. J. Impot. Res. 1999, 11, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.; Yu, J. Sweet Bee Venom Pharmacopuncture May be Effective for Treating Sexual Dysfunction. J. Pharmacopunct. 2014, 17, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Dharmananda, S. Dry needling in orthopedic physical therapy practive. Orthop. Phys. Ther. Pract. 2004, 16, 15–20. [Google Scholar]
- Lin, J.G.; Lo, M.W.; Wen, Y.R.; Hsieh, C.L.; Tsai, S.K.; Sun, W.Z. The effect of high and low frequency electroacupuncture in pain after lower abdominal surgery. Pain 2002, 99, 509–514. [Google Scholar] [CrossRef]
- Liu, Z.; Liu, Y.; Xu, H.; He, L.; Chen, Y.; Fu, L.; Li, N.; Lu, Y.; Su, T.; Sun, J.; et al. Effect of Electroacupuncture on Urinary Leakage Among Women With Stress Urinary Incontinence: A Randomized Clinical Trial. JAMA 2017, 317, 2493–2501. [Google Scholar] [CrossRef] [PubMed]
- Torres-Rosas, R.; Yehia, G.; Pena, G.; Mishra, P.; del Rocio Thompson-Bonilla, M.; Moreno-Eutimio, M.A.; Arriaga-Pizano, L.A.; Isibasi, A.; Ulloa, L. Dopamine mediates vagal modulation of the immune system by electroacupuncture. Nat. Med. 2014, 20, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Lei, H.; Toosizadeh, N.; Schwenk, M.; Sherman, S.; Karp, S.; Sternberg, E.; Najafi, B. A Pilot Clinical Trial to Objectively Assess the Efficacy of Electroacupuncture on Gait in Patients with Parkinson’s Disease Using Body Worn Sensors. PLoS ONE 2016, 11, e0155613. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.M.; Lin, C.F.; Ting, H.; Chang, C.C.; Lin, Y.J.; Lin, T.B. Electroacupuncture at Hoku elicits dual effect on autonomic nervous system in anesthetized rats. Neurosci. Res. 2002, 42, 15–20. [Google Scholar] [CrossRef]
- Natali, A.; Bartolini, M.; Lucarini, S.; Vignolini, G.; Nelli, F.; Menchi, I. Statistical evaluation of hemodynamic effects of regular use of sildenafil on the human corpora cavernosa. Urol. Int. 2009, 82, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Hsueh, T.Y.; Wu, Y.T.; Lin, L.C.; Chiu, A.W.; Lin, C.H.; Tsai, T.H. Herb-drug interaction of Epimedium sagittatum (Sieb. et Zucc.) maxim extract on the pharmacokinetics of sildenafil in rats. Molecules 2013, 18, 7323–7335. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.T.; Shaw, L.H.; Wu, Y.T.; Tsai, T.H. Interaction of acupuncture and electroacupuncture on the pharmacokinetics of aspirin and the effect of brain blood flow in rats. Evid. Based Complement. Altern. Med. 2013, 2013, 670858. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.K.; Ackland, M.J.; James, G.C.; Muirhead, G.J.; Rance, D.J.; Wastall, P.; Wright, P.A. Pharmacokinetics and metabolism of sildenafil in mouse, rat, rabbit, dog and man. Xenobiotica 1999, 29, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Meng, F.; Jia, Y.; Zhao, X. Clinical research on the therapeutic effect of the electro-acupuncture treatment in patients with depression. Psychiatry Clin. Neurosci. 1998, 52 (Suppl. 6), S338–S400. [Google Scholar] [CrossRef] [PubMed]
- Casimiro, L.; Barnsley, L.; Brosseau, L.; Milne, S.; Robinson, V.A.; Tugwell, P.; Wells, G. Acupuncture and electroacupuncture for the treatment of rheumatoid arthritis. Cochrane Database Syst. Rev. 2005, 4, CD003788. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Xie, Y.; Zhang, Q.; Xu, N.; Zhong, H.; Dong, H.; Liu, L.; Jiang, T.; Wang, Q.; Xiong, L. Transcutaneous electric acupoint stimulation reduces intra-operative remifentanil consumption and alleviates postoperative side-effects in patients undergoing sinusotomy: A prospective, randomized, placebo-controlled trial. Br. J. Anaesth. 2014, 112, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Aloe, L.; Manni, L. Low-frequency electro-acupuncture reduces the nociceptive response and the pain mediator enhancement induced by nerve growth factor. Neurosci. Lett. 2009, 449, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Qu, F.; Burrows, E.; Yu, Y.; Nan, R. Acupuncture can improve absorption of baicalin from extracts of Scutellaria baicalensis Georgi in rats. Phytother. Res. 2009, 23, 1415–1420. [Google Scholar] [CrossRef] [PubMed]
- Tseng, T.-Y.; Tsai, T.-H. Measurement of unbound geniposide in blood, liver, brain and bile of anesthetized rats: An application of pharmacokinetic study and its influence on acupuncture. Anal. Chim. Acta 2004, 517, 47–52. [Google Scholar] [CrossRef]
- Wu, C.Y.; Benet, L.Z. Predicting drug disposition via application of BCS: Transport/absorption/elimination interplay and development of a biopharmaceutics drug disposition classification system. Pharm. Res. 2005, 22, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Boxenbaum, H. Interspecies variation in liver weight, hepatic blood flow, and antipyrine intrinsic clearance: Extrapolation of data to benzodiazepines and phenytoin. J. Pharmacokinet. Biopharm. 1980, 8, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Steers, W.D. Pharmacologic treatment of erectile dysfunction. Rev. Urol. 2002, 4 (Suppl. 3), S17–S25. [Google Scholar] [PubMed]
- Wang, C. Phosphodiesterase-5 inhibitors and benign prostatic hyperplasia. Curr. Opin. Urol. 2010, 20, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.E.; Thompson, C.S.; Dashwood, M.R.; Khan, M.A.; Jeremy, J.Y.; Morgan, R.J.; Mikhailidis, D.P. Nitric oxide and penile erection: Is erectile dysfunction another manifestation of vascular disease? Cardiovasc. Res. 1999, 43, 658–665. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Groups | Sildenafil (10 mg/Kg) and Electro-Acupuncture (mA, Hz) Dose |
|---|---|
| Group 1 | Sildenafil (10 mg/Kg) only |
| Group 2 | Sildenafil (10 mg/Kg) + EA (1.5 mA, 2 Hz) |
| Group 3 | Sildenafil (10 mg/Kg) + EA (1.5 mA, 80 Hz) |
| Parameters | C0 (μg/mL) | t1/2 (min) | AUC (min μg/mL) | Cl (mL/min/kg) | Vss (mL/kg) | MRT (min) |
|---|---|---|---|---|---|---|
| Group 1 | 5.0 ± 1.0 | 43 ± 22 | 110 ± 15 | 92 ± 11 | 3866 ± 2450 | 41 ± 23 |
| Group 2 | 4.8 ± 0.8 | 52 ± 27 | 137 ± 52 | 86 ± 44 | 3544 ± 831 | 50 ± 22 |
| Group 3 | 4.3 ± 1.3 | 43 ± 10 | 124 ± 27 | 84 ± 20 | 3544 ± 787 | 43 ± 6 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, A.C.; Yeh, K.-Y.; Cheng, Y.-Y.; Dubey, N.K.; Chiu, A.W.; Tsai, T.-H. Investigation of Interactive Activity of Electro-Acupuncture on Pharmacokinetics of Sildenafil and Their Synergistic Effect on Penile Blood Flow in Rats. Int. J. Mol. Sci. 2018, 19, 2153. https://doi.org/10.3390/ijms19082153
Huang AC, Yeh K-Y, Cheng Y-Y, Dubey NK, Chiu AW, Tsai T-H. Investigation of Interactive Activity of Electro-Acupuncture on Pharmacokinetics of Sildenafil and Their Synergistic Effect on Penile Blood Flow in Rats. International Journal of Molecular Sciences. 2018; 19(8):2153. https://doi.org/10.3390/ijms19082153
Chicago/Turabian StyleHuang, Andy C., Kuei-Ying Yeh, Yung-Yi Cheng, Navneet Kumar Dubey, Allen W. Chiu, and Tung-Hu Tsai. 2018. "Investigation of Interactive Activity of Electro-Acupuncture on Pharmacokinetics of Sildenafil and Their Synergistic Effect on Penile Blood Flow in Rats" International Journal of Molecular Sciences 19, no. 8: 2153. https://doi.org/10.3390/ijms19082153
APA StyleHuang, A. C., Yeh, K.-Y., Cheng, Y.-Y., Dubey, N. K., Chiu, A. W., & Tsai, T.-H. (2018). Investigation of Interactive Activity of Electro-Acupuncture on Pharmacokinetics of Sildenafil and Their Synergistic Effect on Penile Blood Flow in Rats. International Journal of Molecular Sciences, 19(8), 2153. https://doi.org/10.3390/ijms19082153