Diagnostic and Prognostic Potential of MicroRNA Maturation Regulators Drosha, AGO1 and AGO2 in Urothelial Carcinomas of the Bladder

 , and
, and
Abstract
:1. Introduction
2. Results
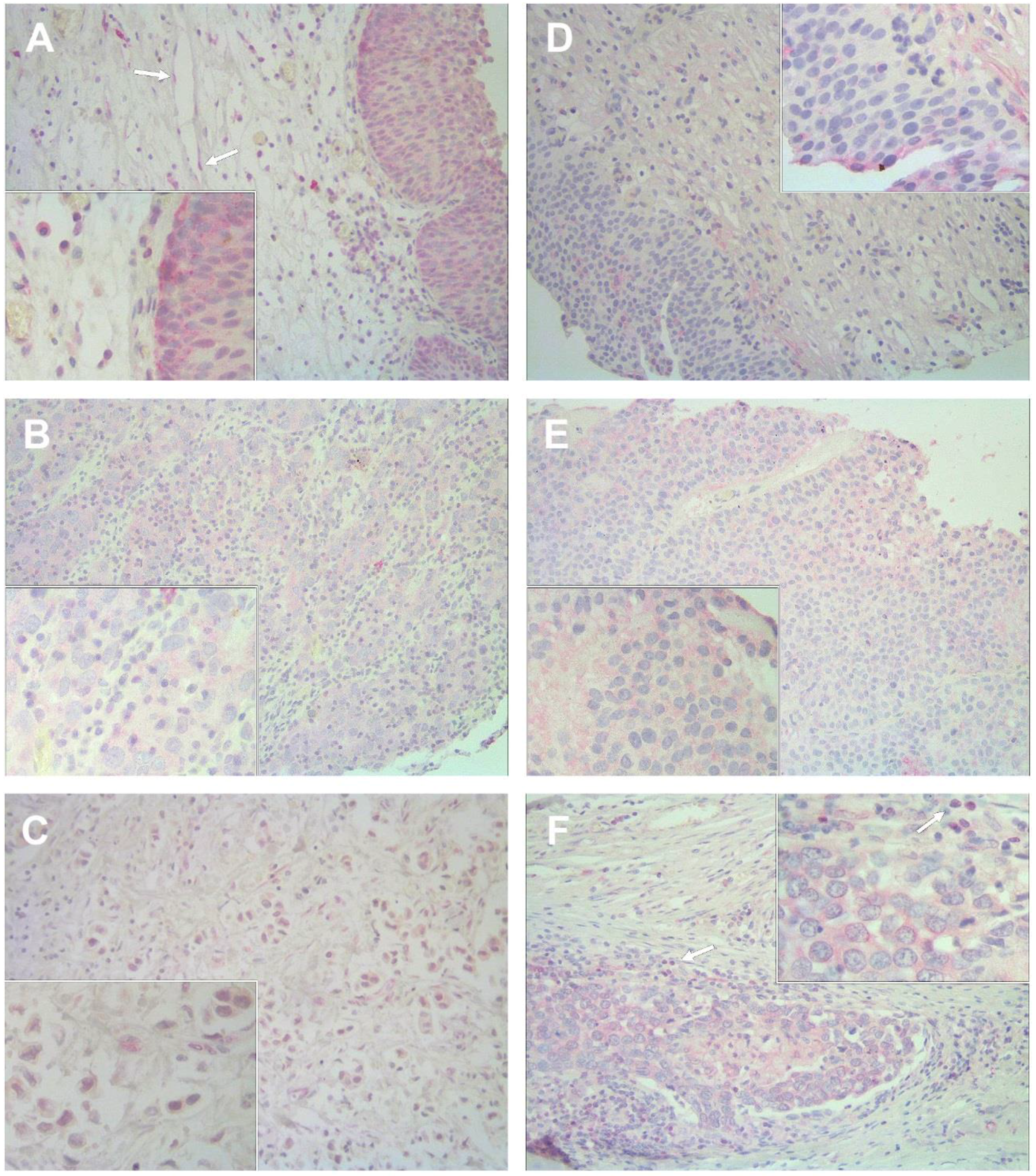
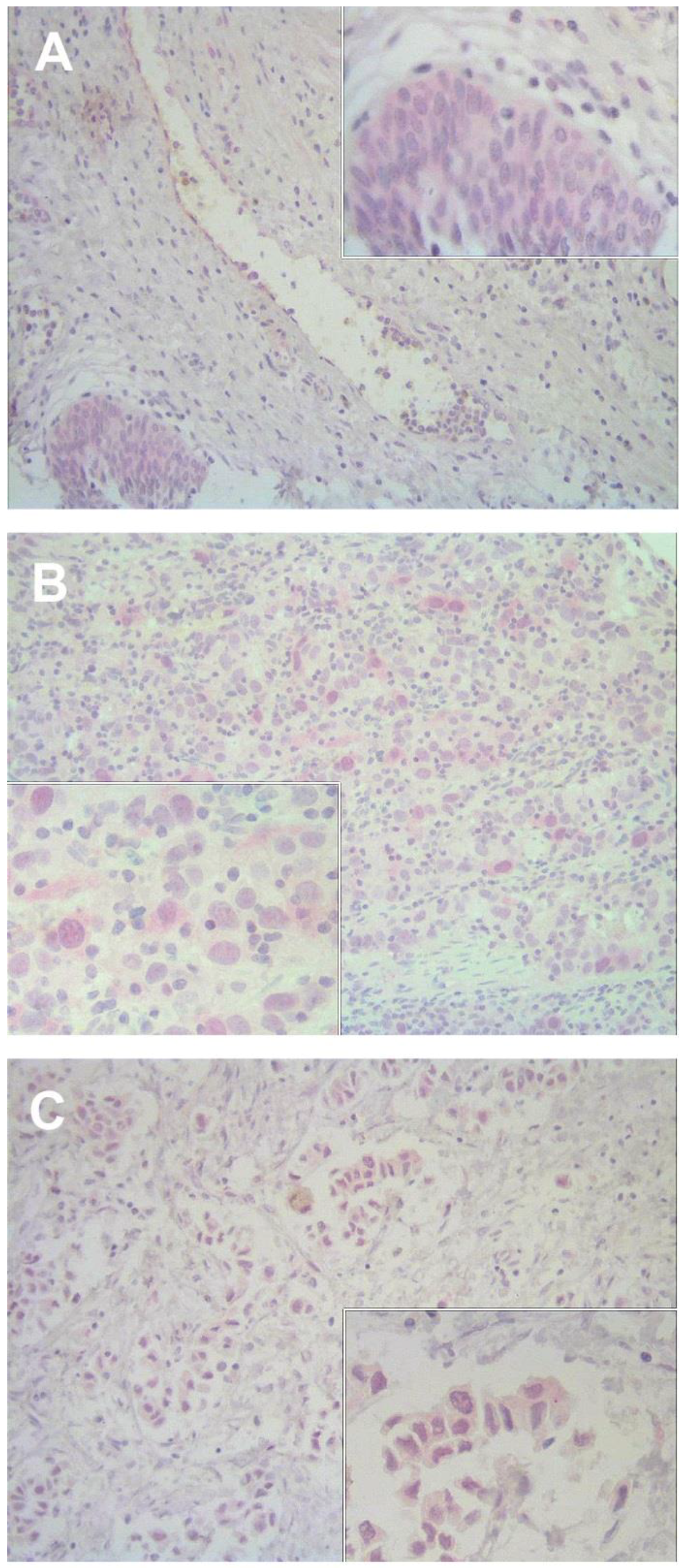
2.1. Immunostaining Pattern of AGO1, AGO2, and Drosha Expression in Bladder Tissue
2.2. AGO1, AGO2 and Drosha Expression in Bladder Carcinomas Compared to Non-Malignant Tissue and Association with Clinicopathological Parameters
2.3. Association of AGO1, AGO2 and Drosha Expression with Patient Survival
3. Discussion
4. Materials and Methods
4.1. Tissue Sample Selection
4.2. Construction of Tissue Microarray
4.3. Immunohistochemistry
4.4. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; He, X.L.; Teng, X.D. Understanding the molecular pathogenesis and prognostics of bladder cancer: An overview. Chin. J. Cancer Res. 2016, 28, 92–98. [Google Scholar] [PubMed]
- Mohammed, A.A.; El-Tanni, H.; El-Khatib, H.M.; Mirza, A.A.; Mirza, A.A.; Alturaifi, T.H. Urinary Bladder Cancer: Biomarkers and Target Therapy, New Era for More Attention. Oncol. Rev. 2016, 10. [Google Scholar] [CrossRef] [PubMed]
- Bartel, D.P. MicroRNAs: Genomics, biogenesis, mechanism, and function. Cell 2004, 116, 281–297. [Google Scholar] [CrossRef]
- Calin, G.A.; Croce, C.M. MicroRNA signatures in human cancers. Nat. Rev. Cancer 2006, 6, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Dong, F.; Xu, T.; Shen, Y.; Zhong, S.; Chen, S.; Ding, Q.; Shen, Z. Dysregulation of miRNAs in bladder cancer: Altered expression with aberrant biogenesis procedure. Oncotarget 2017, 8, 27547–27568. [Google Scholar] [CrossRef] [PubMed]
- Mitash, N.; Tiwari, S.; Agnihotri, S.; Mandhani, A. Bladder cancer: Micro RNAs as biomolecules for prognostication and surveillance. Indian J. Urol. 2017, 33, 127–133. [Google Scholar] [PubMed]
- Hata, A.; Kashima, R. Dysregulation of microRNA biogenesis machinery in cancer. Crit. Rev. Biochem. Mol. Biol. 2016, 51, 121–134. [Google Scholar] [CrossRef] [PubMed]
- Cheloufi, S.; Dos Santos, C.O.; Chong, M.M.; Hannon, G.J. A dicer-independent miRNA biogenesis pathway that requires Ago catalysis. Nature 2010, 465, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Liu, M.; Feng, Y.; Xu, Y.F.; Che, J.P.; Wang, G.C.; Zheng, J.H.; Gao, H.J. Evaluation of Argonaute protein as a predictive marker for human clear cell renal cell carcinoma. Int. J. Clin. Exp. Pathol. 2013, 6, 1086–1094. [Google Scholar] [PubMed]
- Bian, X.J.; Zhang, G.M.; Gu, C.Y.; Cai, Y.; Wang, C.F.; Shen, Y.J.; Zhu, Y.; Zhang, H.L.; Dai, B.; Ye, D.W. Down-regulation of Dicer and Ago2 is associated with cell proliferation and apoptosis in prostate cancer. Tumor Biol. 2014, 35, 11571–11578. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.Q.; Huang, J.H.; Liu, M.; Yang, F.P.; Li, W.; Wang, G.C.; Che, J.P.; Zheng, J.H. Argonaute 2 is up-regulated in tissues of urothelial carcinoma of bladder. Int. J. Clin. Exp. Pathol. 2014, 7, 340–347. [Google Scholar] [PubMed]
- Zhang, Z.; Zhang, G.; Kong, C.; Bi, J.; Gong, D.; Yu, X.; Shi, D.; Zhan, B.; Ye, P. EIF2C, Dicer, and Drosha are up-regulated along tumor progression and associated with poor prognosis in bladder carcinoma. Tumor Biol. 2015, 36, 5071–5079. [Google Scholar] [CrossRef] [PubMed]
- Sand, M.; Skrygan, M.; Georgas, D.; Arenz, C.; Gambichler, T.; Sand, D.; Altmeyer, P.; Bechara, F.G. Expression levels of the microRNA maturing microprocessor complex component DGCR8 and the RNA-induced silencing complex (RISC) components argonaute-1, argonaute-2, PACT, TARBP1, and TARBP2 in epithelial skin cancer. Mol. Carcinog. 2012, 51, 916–922. [Google Scholar] [CrossRef] [PubMed]
- Vaksman, O.; Hetland, T.E.; Trope, C.G.; Reich, R.; Davidson, B. Argonaute, Dicer, and Drosha are up-regulated along tumor progression in serous ovarian carcinoma. Hum. Pathol. 2012, 43, 2062–2069. [Google Scholar] [CrossRef] [PubMed]
- Adams, B.D.; Claffey, K.P.; White, B.A. Argonaute-2 expression is regulated by epidermal growth factor receptor and mitogen-activated protein kinase signaling and correlates with a transformed phenotype in breast cancer cells. Endocrinology 2009, 150, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Yoo, N.J.; Hur, S.Y.; Kim, M.S.; Lee, J.Y.; Lee, S.H. Immunohistochemical analysis of RNA-induced silencing complex-related proteins AGO2 and TNRC6A in prostate and esophageal cancers. APMIS 2010, 118, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Chen, L.; Barlogie, B.; Stephens, O.; Wu, X.; Williams, D.R.; Cartron, M.A.; van, R.F.; Nair, B.; Waheed, S.; et al. High-risk myeloma is associated with global elevation of miRNAs and overexpression of EIF2C2/AGO2. Proc. Natl. Acad. Sci. USA 2010, 107, 7904–7909. [Google Scholar] [CrossRef] [PubMed]
- Pop-Bica, C.; Gulei, D.; Cojocneanu-Petric, R.; Braicu, C.; Petrut, B.; Berindan-Neagoe, I. Understanding the Role of Non-Coding RNAs in Bladder Cancer: From Dark Matter to Valuable Therapeutic Targets. Int. J. Mol. Sci. 2017, 18, 1514. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): Explanation and elaboration. PLoS. Med. 2012, 9, e1001216. [Google Scholar] [CrossRef] [PubMed]
- Jafarnejad, S.M.; Sjoestroem, C.; Martinka, M.; Li, G. Expression of the RNase III enzyme DROSHA is reduced during progression of human cutaneous melanoma. Mod. Pathol. 2013, 26, 902–910. [Google Scholar] [CrossRef] [PubMed]
- Papachristou, D.J.; Sklirou, E.; Corradi, D.; Grassani, C.; Kontogeorgakos, V.; Rao, U.N. Immunohistochemical analysis of the endoribonucleases Drosha, Dicer and Ago2 in smooth muscle tumours of soft tissues. Histopathology 2012, 60, E28–E36. [Google Scholar] [CrossRef] [PubMed]
- Passon, N.; Gerometta, A.; Puppin, C.; Lavarone, E.; Puglisi, F.; Tell, G.; Di, L.C.; Damante, G. Expression of Dicer and Drosha in triple-negative breast cancer. J. Clin. Pathol. 2012, 65, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Sugito, N.; Ishiguro, H.; Kuwabara, Y.; Kimura, M.; Mitsui, A.; Kurehara, H.; Ando, T.; Mori, R.; Takashima, N.; Ogawa, R.; et al. RNASEN regulates cell proliferation and affects survival in esophageal cancer patients. Clin. Cancer Res. 2006, 12, 7322–7328. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Oosterlinck, W.; Sylvester, R.; Kaasinen, E.; Bohle, A.; Palou-Redorta, J.; Roupret, M. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder, the 2011 update. Eur. Urol. 2011, 59, 997–1008. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Jung, M.; Burkhardt, M.; Stephan, C.; Schnorr, D.; Loening, S.; Jung, K.; Dietel, M.; Kristiansen, G. Increased CD59 protein expression predicts a PSA relapse in patients after radical prostatectomy. Prostate 2005, 62, 224–232. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics (n = 112) | n (%) |
|---|---|
| Age, years A | |
| <69 | 52 (46.4) |
| ≥69 | 60 (53.6) |
| Sex | |
| female | 31 (27.7) |
| male | 81 (72.3) |
| Tumor characteristics | |
| pT stage B | |
| pTa | 42 (37.5) |
| pT1 | 20 (17.9) |
| pT2 | 26 (23.2) |
| pT3 | 18 (16.1) |
| pT4 | 6 (5.4) |
| WHO grade B | |
| low | 37 (33.0) |
| high | 75 (67.0) |
| Operative method | |
| TUR-B | 85 (75.9) |
| RTX | 27 (24.1) |
| Follow up, months C | |
| Mean | 56 |
| Median | 53 |
| Range | 3–200 |
| Status after follow-up time C | |
| alive | 67 (60.9) |
| dead | 43 (39.1) |
| Characteristics | Nonmalignant n (%) | NMIBC n (%) | MIBC n (%) |
|---|---|---|---|
| Argonaute 1 | 30 (100) | 60 (100) | 38 (100) |
| negative | 22 (73.3) | 23 (38.3) | 30 (78.9) |
| positive | 8 (26.7) | 37 (61.7) | 8 (21.1) |
| p value A | 0.003 | 0.774 | |
| Argonaute 2 | 34 (100) | 61 (100) | 48 (100) |
| negative | 27 (79.4) | 21 (34.4) | 15 (31.3) |
| positive | 7 (20.6) | 40 (65.6) | 33 (68.8) |
| p value A | <0.001 | <0.001 | |
| Drosha | 35 (100) | 61 (100) | 45 (100) |
| negative | 23 (65.7) | 8 (13.1) | 23 (51.1) |
| positive | 12 (34.3) | 53 (86.9) | 22 (48.9) |
| p value A | <0.001 | 0.255 |
| AGO1 n = 98 | AGO2 n = 109 | Drosha n = 106 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Para-meters | neg | pos | p value | neg | pos | p value | neg | pos | p value |
| n (%) | 53 (54.1) | 45 (45.9) | 36 (33.0) | 73 (67.0) | 31 (29.2) | 75 (70.8) | |||
| Age, years A | |||||||||
| <69 | 23 (23.5) | 21 (21.4) | 0.839 B | 17 (15.6) | 33 (30.3) | 1.000 B | 15 (14.2) | 36 (34.0) | 1.000 B |
| ≥69 | 30 (30.6) | 24 (24.5) | 19 (17.4) | 40 (36.7) | 16 (15.1) | 39 (36.8) | |||
| Sex | |||||||||
| female | 14 (14.3) | 12 (12.2) | 1.000 B | 10 (9.2) | 20 (18.3) | 1.000 B | 8 (7.5) | 22 (20.8) | 0.815 B |
| male | 39 (39.8) | 33 (33.7) | 26 (23.9) | 53 (48.6) | 23 (21.7) | 53 (50.0) | |||
| pT stage | |||||||||
| pTa | 18 (18.4) | 23 (23.5) | 0.001 C | 17 (15.6) | 24 (22.0) | 0.437 C | 3 (2.8) | 38 (35.8) | <0.001 C |
| pT1 | 5 (5.1) | 14 (14.3) | 4 (3.7) | 16 (14.7) | 5 (4.7) | 15 (14.2) | |||
| pT2 | 15 (15.3) | 5 (5.1) | 9 (8.3) | 16 (14.7) | 10 (9.4) | 13 (12.3) | |||
| pT3 | 13 (13.3) | 1 (1.0) | 5 (4.6) | 12 (11.0) | 12 (11.3) | 6 (5.7) | |||
| pT4 | 2 (2.0) | 2 (2.0) | 1 (0.9) | 5 (4.6) | 1 (0.9) | 3 (2.8) | |||
| NMIBC | 23 (23.5) | 37 (37.8) | <0.001 B | 21 (19.3) | 40 (36.7) | 0.838 B | 8 (7.5) | 53 (50.0) | <0.001 B |
| MIBC | 30 (30.6) | 8 (8.2) | 15 (13.8) | 33 (30.3) | 23 (21.7) | 22 (20.8) | |||
| WHO grade D | |||||||||
| low | 15 (15.3) | 20 (20.4) | 0.138 B | 14 (12.8) | 22 (20.2) | 0.392 B | 6 (5.7) | 30 (28.3) | 0.045 B |
| high | 38 (38.8) | 25 (25.5) | 22 (20.2) | 51 (46.8) | 25 (23.6) | 45 (42.5) | |||
| AGO1 E | |||||||||
| neg | - | - | - | 21 (21.9) | 31 (32.3) | 0.025 B | 22 (23.7) | 27 (29.0) | <0.001 B |
| pos | - | - | - | 8 (8.3) | 36 (37.5) | 5 (5.4) | 39 (41.9) | ||
| AGO2 E | |||||||||
| neg | 21 (21.9) | 8 (8.3) | <0.001 F | - | - | - | 11 (10.7) | 23 (22.3) | 0.649 B |
| pos | 31 (32.3) | 36 (37.5) | - | - | - | 19 (18.4) | 50 (48.5) | ||
| Drosha E | |||||||||
| neg | 22 (23.7) | 5 (5.4) | <0.001 F | 11 (10.7) | 19 (18.4) | 0.644 F | - | - | - |
| pos | 27 (29.0) | 39 (41.9) | 23 (22.3) | 50 (48.5) | - | - | - | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rabien, A.; Ratert, N.; Högner, A.; Erbersdobler, A.; Jung, K.; Ecke, T.H.; Kilic, E. Diagnostic and Prognostic Potential of MicroRNA Maturation Regulators Drosha, AGO1 and AGO2 in Urothelial Carcinomas of the Bladder. Int. J. Mol. Sci. 2018, 19, 1622. https://doi.org/10.3390/ijms19061622
Rabien A, Ratert N, Högner A, Erbersdobler A, Jung K, Ecke TH, Kilic E. Diagnostic and Prognostic Potential of MicroRNA Maturation Regulators Drosha, AGO1 and AGO2 in Urothelial Carcinomas of the Bladder. International Journal of Molecular Sciences. 2018; 19(6):1622. https://doi.org/10.3390/ijms19061622
Chicago/Turabian StyleRabien, Anja, Nadine Ratert, Anica Högner, Andreas Erbersdobler, Klaus Jung, Thorsten H. Ecke, and Ergin Kilic. 2018. "Diagnostic and Prognostic Potential of MicroRNA Maturation Regulators Drosha, AGO1 and AGO2 in Urothelial Carcinomas of the Bladder" International Journal of Molecular Sciences 19, no. 6: 1622. https://doi.org/10.3390/ijms19061622