Differentiated Thyroid Cancer—Treatment: State of the Art


Department of Nuclear Medicine, University of Regensburg, 93053 Regensburg, Germany
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Int. J. Mol. Sci. 2017, 18(6), 1292; https://doi.org/10.3390/ijms18061292
Submission received: 6 April 2017
/
Revised: 5 June 2017
/
Accepted: 5 June 2017
/
Published: 17 June 2017
(This article belongs to the Special Issue Current Knowledge in Thyroid Cancer—From Bench to Bedside)
Abstract
:Differentiated thyroid cancer (DTC) is a rare malignant disease, although its incidence has increased over the last few decades. It derives from follicular thyroid cells. Generally speaking, the prognosis is excellent. If treatment according to the current guidelines is given, cases of recurrence or persistence are rare. DTC requires special expertise by the treating physician. In recent years, new therapeutic options for these patients have become available. For this article we performed a systematic literature review with special focus on the guidelines of the American Thyroid Association, the European Association of Nuclear Medicine, and the German Society of Nuclear Medicine. For DTC, surgery and radioiodine therapy followed by levothyroxine substitution remain the established therapeutic procedures. Even metastasized tumors can be cured this way. However, in rare cases of radioiodine-refractory tumors, additional options are to be discussed. These include strict suppression of thyroid-stimulating hormone (also known as thyrotropin, TSH) and external local radiotherapy. Systemic cytostatic chemotherapy does not play a significant role. Recently, multikinase or tyrosine kinase inhibitors have been approved for the treatment of radioiodine-refractory DTC. Although a benefit for overall survival has not been shown yet, these new drugs can slow down tumor progression. However, they are frequently associated with severe side effects and should be reserved for patients with threatening symptoms only.
1. Introduction
Patients with differentiated thyroid carcinoma have an excellent prognosis. The multimodal therapeutic approach is risk-adapted to achieve optimal treatment of differentiated thyroid cancer (DTC) and to minimize treatment-related morbidity. The treatment includes surgery (near-/total thyroidectomy) usually followed by remnant ablation using radioiodine according to the guidelines of the American Thyroid Association (ATA) and European Association of Nuclear Medicine (EANM) as well as a risk-stratified follow-up including hormone substitution.
However, in patients with primary or secondary radioiodine-refractory thyroid carcinoma the prognosis becomes significantly poorer. External beam irradiation may be used for locoregional control. Receptor tyrosine kinase inhibitors (TKIs) have shown clinical effectiveness in iodine-refractory DTC.
In this review, we present the current state of treatment of DTC.
2. Epidemiology and Classification
DTC is a rare disease with mostly excellent prognosis. The appearance of DTC depends on age, sex, family history, radiation exposure and many other factors [1]. DTC occurs in 7–15% of patients with thyroid surgery. In the year 2014, approximately 63,000 new cases of DTC were diagnosed in the US [2] compared to 2009 with only 31,200 new cases. In Germany there are about 6000 new cases of DTC per year. The growing incidence of thyroid cancer and the tumor shift to diagnosis of smaller tumors is due to the increased usage of diagnostic methods, such as ultrasound of the neck [3].
Differentiated thyroid cancer includes papillary and follicular cancer that derive from thyrocytes and express the sodium iodine symporter. DTC represents the majority (90%) of all types of thyroid cancer [4]. One study predicts that papillary thyroid cancer will become the third most expensive cancer in women, with costs of US$ 19–21 billion in the US in 2019 [5].
Worldwide, there are many clinical practice guidelines for diagnosis, therapy and follow-up of DTC. The European Thyroid Association (ETA) published new guidelines for the management of DTC in 2013 [6]. The Society for Nuclear Medicine and Molecular Imaging and European Association of Nuclear Medicine published their most recent guidelines for radioiodine therapy of differentiated thyroid cancer in 2012 and 2008, respectively [7,8]. The Japanese Association of Endocrine Surgeons and the Japanese Society of Thyroid Surgeons recently reviewed their guidelines in 2014 [9]. The new ATA guidelines for management of differentiated thyroid cancer for adults were published in 2015 [10]. The updated ATA guidelines for management of DTC for children were also published in 2015 [11].
The risk classification of DTC using multiple staging systems is based on a combination of the size of the primary tumor, specific histology, extrathyroidal spread of the tumor and the age at diagnosis. It helps to predict the risk of local recurrence and developing metastases and the mortality in patients with DTC. The TNM classification depends on the size of primary tumor, the number and localization of metastatic lymph nodes and number of distant metastases (Table 1) [12]. The American Joint Committee on Cancer (AJCC) uses the combination of TNM Classification and an age of more than 55 years at diagnosis as risk factor [13]. The differentiation of lymphatic invasion and angioinvasion is of high importance, because angioinvasion is associated with an intermediate risk of recurrence. A common risk-stratification of DTC is based on the TNM classification (see also Section 4.2) [14]:
- high-risk group: pT3, pT4, each N1, all M1;
- low-risk group: pT1b, pT2, cN0/pN0, cM0;
- very low risk-group: pT1a, cN0/pN0, cM0.
The American Thyroid Association defines in their current guideline a stratification based on the risk of structural disease recurrence [10]:
- high-risk group: gross extrathyreoidal extension, incomplete tumor resection, distant metastases, or lymph node >3 cm;
- intermediate-risk: aggressive histology, minor extrathyreoidal extension, vascular invasion, or >5 involved lymph nodes (0.2–3 cm);
- low-risk: intrathyreoidal DTC, ≤5 lymph nodes micrometastases (<0.2 cm).
In the last few years new molecular and genetic biomarkers, such as BRAF (V600E), phosphatidylinositol 4,5-bisphosphate 3-kinase catalytic subunit α (PIK3CA), tumor protein p53 (TP53), RAC-α serine/threonine-protein kinase 1 (AKT1) and telomerase reverse transcriptase (TERT) became more important for the management of diagnosis, therapy and observing of DTC. The role of RAS is discussed controversally. Table 2 shows the impact of the two well-evaluated molecular markers BRAF and TERT [15]. Some of these alterations might be interesting molecular targets for new therapies.
2.1. Papillary Thyroid Cancer
Papillary thyroid carcinoma (PTC) is the most common form of DTC. Histologically it is a tumor of follicular cells of the thyroid gland with characteristic nuclear signs. There are more than 10 histological variants of papillary thyroid cancer documented, can be seen in Table 3 [16,17]. Due to this microscopic diversity, different risk stratifications are needed.
The tall cell variant is one of the tumor entities with unfavorable outcome. This type of thyroid cancer is presented in tall columnar cells and occurs in older age showing a higher rate of lymph node metastases. In nearly 80% of these tumors the BRAF (V600E) mutation is found [18]. A new aggressive variant of papillary thyroid carcinoma, which is characterized by cells with hobnail appearance and apically placed nuclei, was described recently. The BRAF (V600E) mutation is found frequently and associated with distant metastases [19]. In children and adults affected by the Chernobyl incident the solid variant of PTC appears predominantly. Mortality within the first 10 years after initial diagnosis and treatment is low (<1%) [20,21]. It is very important to recognize that there are histological differences compared to poorly differentiated carcinomas, because of the very different therapy strategy. In poorly differentiated thyroid cancer the capability to take up (radio) iodine is clearly reduced (e.g., decreased expression of sodium iodine symporter) and therefore not sufficient to achieve a significant therapeutic effect. Another form of PTC is the diffuse sclerosing variant. It is characterized by a higher incidence of lymph node and distant metastases. Nevertheless, overall mortality appears low. The encapsulated follicular variant of papillary carcinoma very rarely shows capsular or vascular invasion. Histologically it is characterized by follicular growth, typical nuclear features of papillary carcinoma and total tumor encapsulation. RAS mutations can be detected frequently. The non-encapsulated follicular variant of papillary cancer shows BRAF (V600E) mutations quite often [22,23]. This tumor is associated with lymph node metastases in about 25–30% and low rates of distant metastases.
PTC presents distant metastases mainly in bones or lungs.
Papillary microcarcinoma is a PTC < 1 cm corresponding to the classification of the World Health Organization (WHO) which is often found incidentally. In some autopsy studies the papillary microcarcinoma was found in 6–35% of the thyroids by incident [10]. Papillary microcarcinoma may also exhibit RET proto-oncogene (RET)/PTC-rearrangements or BRAF (V600E) mutations.
2.2. Follicular Thyroid Cancer
Follicular thyroid carcinoma (FTC) is a malignant tumor, histologically derived from follicular thyroid cells, showing transcapsular or vascular invasion and missing the typical nuclear signs of papillary carcinoma. In the traditional classification of FTC there are two groups: minimally invasive and widely invasive [24,25,26]. The widely invasive FTC shows an extensive vascular invasion, often also associated with extrathyroidal growth.
Oncocytic follicular carcinoma is a special form of FTC with some microscopic differences compared to conventional FTC. One of them is the accumulation of innumerable mitochondria. Due to its histological differences, oncocytic carcinoma shows some different biological behavior with a higher ability to metastasize to lymph nodes and a possibly higher rate of recurrence and tumor-related mortality [27,28,29].
2.3. Familial Tumor Syndromes
Some of the histopathological variants of DTC are associated with familial tumor syndromes. For example, the cribriform-morular form of papillary thyroid cancer is frequently seen in patients with a germline mutation in adenomatous polyposis coli gene [30,31]. About 40% of patients with this special histological form of papillary thyroid carcinoma show simultaneously a familial adenomatous polyposis (FAP) [32]. Due to this high rate of association of cribriform-morular PTC and FAP it is very important to complete the diagnostic work-up with colonoscopy and genetic counseling.
Another type of FTC is associated with the germline mutation of the phosphatase and tensin homolog (PTEN) gene [33,34,35]. The follicular variant of thyroid carcinoma is in this case very characteristic and should be known by pathologists. The syndrome is associated with a high risk of appearance of other tumors, such as colon hamartomas or breast and endometrium tumors. Genetic counseling is recommended.
3. Diagnostic Approach to Thyroid Nodules
The prevalence of sonographically-detected thyroid nodules in the U.S. is described between 19% and 35% [36]. Toxic adenomas are found in up to 4 percent of the population. In Europe the incidence of thyroid nodules is higher in some areas. In Germany, a country with relative iodine deficiency, nodules are found in 33% of the population.
Risk factors for malignancy are exposure to ionizing radiation through radiotherapy or fallout especially in younger years, familial thyroid carcinoma, or syndromes that are associated with thyroid cancer like PTEN, Cowdens disease or multiple endocrine neoplasia type 2 (MEN2). Warning signs in clinical examination are rapid nodule growth, fixation in the surrounding tissue, vocal cord paralysis, possibly accompanied by hoarseness.
The diagnostic cornerstone of thyroid nodules remains the ultrasound examination. It should be performed in any case of known or suspected thyroid nodules or cervical lymphadenopathy to assess if further diagnostic is needed. Sonographic patterns suspicious of malignancy are microcalcifications, irregular margins, solid consistency, hypoechogenity, extrathyroidal extension (ETE) and a tall shape rather than a wide one. Intranodulary vascularization does not seem to have a clear correlation with malignancy [10].
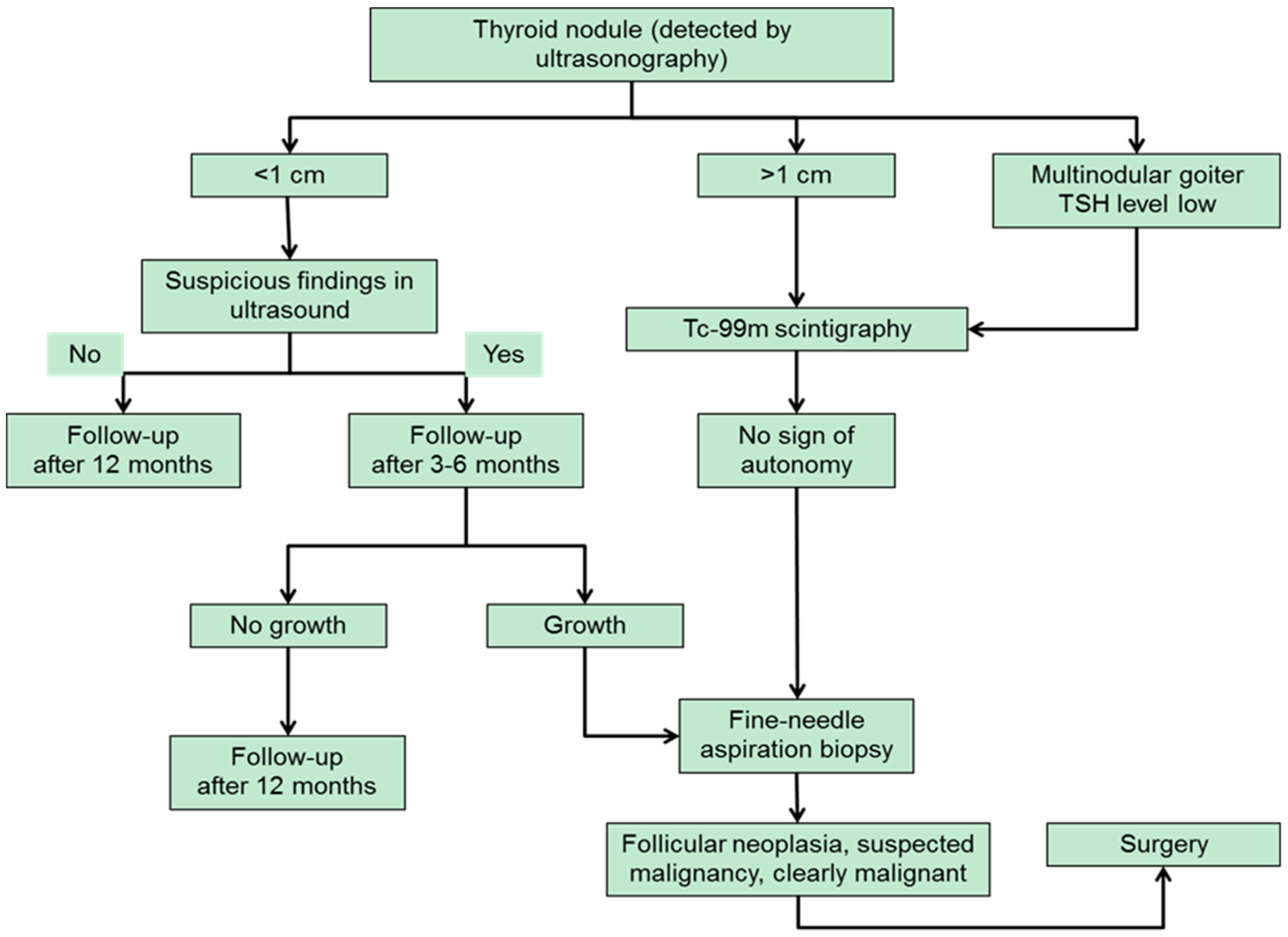
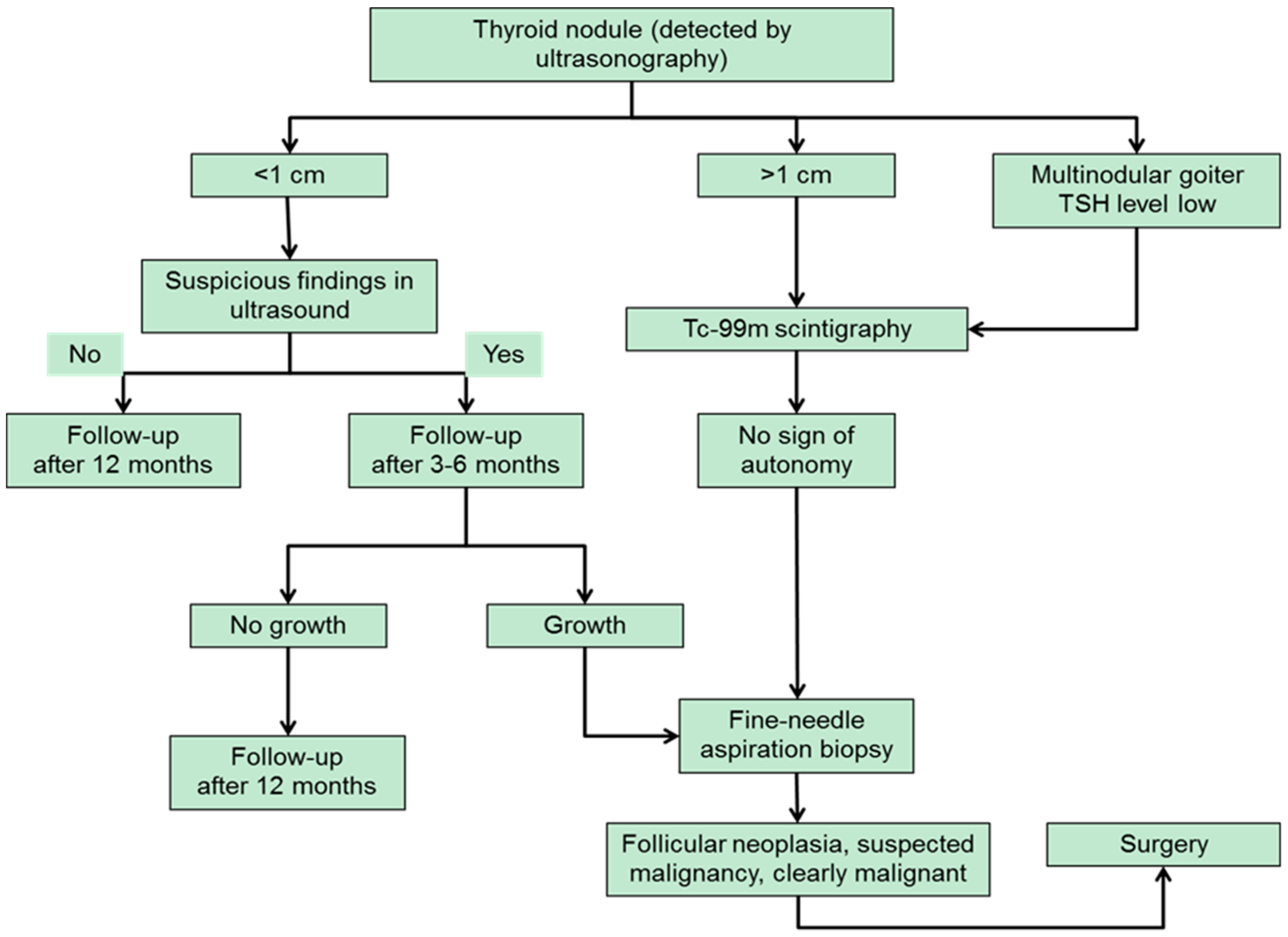
Roughly one third of thyroid nodules are larger than 1 cm and eligible for scintigraphy [37]. The guidelines of the German Society of Nuclear Medicine recommend a scintigraphic examination of every thyroid nodule >1 cm. By routinely performing a Tc-99m thyroid scan autonomous adenomas that have not yet an impact on thyroid-stimulating hormone (TSH) level can be detected without subjecting the patient to the risks and stress of fine-needle aspiration (FNA). This applies especially to groups at increased risk for complications like patients that are treated with coagulation inhibitors. The diagnostic algorithm for evaluation of thyroid nodules according to the German guidelines that was recently published by Feldkamp et al. is shown in Figure 1 [38].
The ATA guidelines recommend measurement of the TSH level if a thyroid nodule is found. A radionuclide scan (Tc-99m, preferable I-123) should be performed only if TSH level is subnormal [10]. Nevertheless, the American guidelines cannot be applied to the rest of the world without adjustment for differences in the patient populations. Except for clearly benign cysts, for every lesion of a certain size ultrasound guided fine-needle aspiration biopsy (FNA) is recommended (Table 4) [10]. Furthermore, the measurement of serum calcitonin is recommended when new thyroid nodules are detected time to rule out medullary thyroid cancer that derives from c-cells and is not added to group of DTC.
Cytological analysis is performed according to the Bethesda System for Reporting Thyroid Cytopathology. The findings are graded into six categories:
- I:
- nondiagnostic/unsatisfactory;
- II:
- benign;
- III:
- atypia of undetermined significance/follicular lesion of undetermined significance;
- IV:
- follicular neoplasm/suspicious for follicular neoplasm;
- V:
- suspicious for malignancy;
- VI:
- malignant.
If the FNA biopsy is graded non-diagnostic/unsatisfactory, biopsy should be repeated. Numerous molecular tests can be applied to distinguish malignant from benign lesions, such as BRAF (V600E), PIK3CA and TERT promoter, AKT1, and TP53, although there is no explicit recommendation in the current guidelines. Accordingly, adjustments are to be expected in the future [15]. For more non-diagnostic biopsies in a row, the decision for close surveillance without intervention or for surgery should be made in dependence of the sonographic pattern [10].
4. Therapy of Differentiated Thyroid Carcinoma
DTC should be treated interdisciplinary in facilities with an appropriate expertise in order to ensure an optimal long-term treatment quality. Specialists in surgery, endocrinology, pathology and nuclear medicine should be available. The therapeutic approach is individualized and risk-adapted.
4.1. Surgery
For widely invasive follicular thyroid carcinomas and FTC with vascular infiltration, thyreoidectomy is recommended. Lymph node dissection is recommended if lymph node metastases can be detected pre- or intraoperatively by sonographic examination and/or palpation. The solitary minimally invasive FTC without vascular invasion does not require a second surgical intervention as completion, if the tumor has been completely removed (R0). Thyreoidectomy and lymph node dissection of the central compartment are recommended for prognostically unfavorable variants.
For all papillary thyroid carcinomas >1 cm and/or for all metastasized or macroscopically invasive PTC irrespective of size, thyreoidectomy is recommended [10,39]. If lymph node metastases have been detected sonographically or intraoperatively, lymph node dissection in the affected compartment should be done to reduce the risk of (local) recurrence. On the other hand, the diagnostic or therapeutic extirpation of only single lymph nodes as a part of the primary intervention is not recommended. Although at present the importance of central lymph dissection with prophylactic intention is still unclear, the high probability of lymph node metastases is a substantial argument to expand the surgical procedure. Furthermore, it is difficult to exclude lymph node metastases pre- or intraoperatively. After all, the increased risk of a local recurrence associated with an increased morbidity due to the surgical intervention in the situation of relapse should be mentioned. On the other hand, the main arguments against a prophylactic dissection are the lack of evidence regarding a better outcome of the patients and the remarkably higher complication rate due to the more extensive intervention (e.g., vocal cord paralysis, parathyreoprival tetany). Specifically, papillary thyroid microcarcinoma that is found incidentally does not require a further surgical treatment.
After all, accurate histopathological examination of the specimen after (hemi)thyroidectomy and lymphadenectomy (if done) is regarded as the gold standard and is indispensable for the management and further diagnostic and therapeutic approach.
4.2. Adjuvant Radioiodine Therapy
Radioiodine therapy (RIT) has been established for more than 60 years. The benefit was demonstrated in DTC patients with a high risk for recurrence. In patients with very low-risk DTC a positive effect of a RIT on tumor-free and overall survival has not been proven by prospective clinical trials.
RIT is defined as the systemic administration of I-131 (radioiodine as sodium iodide or potassium iodide) to irradiate thyroid remnants as well as non-resectable or incompletely resected DTC.
Adjuvant ablative RIT of thyroid remnants or tumor tissue is the optimal precondition for the follow-up including determination of serum thyroglobulin (Tg) and I-131 whole-body scans. The rationale that underlies this approach is to detect a local recurrence or distant metastases in an early and potentially curable stage to minimize mortality. However, regional or distant metastases frequently are only detectable by rising Tg levels after a successful remnant-ablation. It was shown that an ablative RIT decreases the rate of recurrence and mortality over a follow-up period of more than 10 years [40,41,42,43]. RIT is indicated in high-risk DTC (pT3, pT4, each N1, every M1), in low-risk DTC (pT1b, pT2, cN0, pN0, M0) and in small papillary thyroid carcinoma (very low-risk DTC), if there are risk factors (see Section 4.7) [44,45]. Furthermore, RIT can be used for the treatment of radioiodine-positive tumor residues, lymph node and distant metastases with curative or palliative intention. In the case of tumor activity shown by an increasing serum level of thyroglobulin without a macroscopically detectable tumor using morphological and functional imaging RIT can be carried out after carefully weighing risks and benefits [14].
To ensure a high uptake of radioiodine (I-131) in remnant tissue, (suspected) tumor, or metastases, an elevated serum level of TSH is required (>30 mU/L). This level is believed to increase the expression of the sodium iodine symporter (NIS) in benign and malignant follicular cells of the thyroid [46]. According to the guidelines of the ATA and EANM [8,10] this TSH level can be reached by waiting not less than 3 weeks after thyroidectomy or after a withdrawal (4–5 weeks) of levothyroxine (LT4). The subsequent period of hypothyroidism decreases the quality of life significantly in many patients. The physical and psychological symptoms of hypothyroidism include gain of weight, impaired renal function, cardiovascular abnormalities, dyslipidemia (exacerbation), constipation, dry skin, hoarseness, fatigue, sleep disturbance, impaired ability to concentrate and depression [47]. Alternatively, recombinant TSH (rhTSH) can be administered intramuscularly (2 times 0.9 mg rhTSH) to avoid inconvenience and morbidity due to the lack of thyroid hormone. This drug is approved for radioiodine ablation (without known distant metastases) of T1–4 tumors, diagnostic whole-body scan and preparation for testing of serum Tg in adults [48,49,50,51].
Absolute contraindications of RIT are pregnancy and breastfeeding. Relative contraindications include depression of the bone marrow (especially if the administration of high activities of I-131 is planned), a restriction of salivary gland function, pulmonary function restriction (if a high accumulation of I-131 in lung metastases is possible) and symptomatic metastases of the central nervous system, because local edema and inflammation caused by RIT and hypothyroidism can lead to severe compression effects [8].
The activity of I-131 for remnant ablation is still discussed controversially. The HiLo study (Great Britain) and the ESTIMABL study (France) both compared ablative RIT with 1.1 GBq I-131 versus administration of 3.7 GBq (100 mCi) I-131 after thyroid hormone withdrawal or stimulation with rhTSH in patients with low-risk carcinoma [52,53]. Both studies showed that RIT with only 1.1 GBq (30 mCi) I-131 is not inferior compared to the higher activity in regard to the success of ablation. However, the definition of “success of ablation” used in both studies is not accepted by all departments and associations. Several authors report that the rate of a second RIT increases when low therapy activities were used initially [54,55].
In the ESTIMABL study the diagnostic I-131-whole-body scan 8 months after I-131 ablation was limited to patients with elevated Tg antibodies and disturbed Tg recovery. Even in this subgroup this concept was not consistently implemented. Based on an observation study, iodine-accumulating metastases are possible with a measurable Tg level of up to 1 ng/mL [56]. Due to the open question of the “optimal” activity for remnant ablation, the German Society of Nuclear Medicine for example recommends a single administration of 1 to 3.7 GBq (about 30–100 mCi) I-131 [14]. Preablation scanning with Tc-99m pertechnetate on the day of ablation (as used in the HiLo trial [52]) can give very useful information in clinical decision making. In low-risk DTC patients with a large remnant (multiple foci or one large focus) ablation with 3.7 GBq (30 mCi) may be prefered.
Although RIT is generally well tolerated, the procedure has some potential short- and long-term side effects [8]. Short-term risks/side effects are: thyroiditis due to irradiation, swelling of the tumor or metastases (including compression symptoms), gastritis and nausea, sialadenitis and abnormalities of taste and smell, bone marrow depression, and hypospermia.
Long-term risks and side effects include permanent bone marrow depression, second primary malignancy after RIT with a high cumulative activity (leukemia and solid tumors) [57], chronic sialadenitis (including abnormalities of taste and smell, xerostomia,) and pulmonary fibrosis (in patients with diffuse iodine-avid pulmonary metastases). Due to the risk of chronic hypospermia or azoospermia, sperm banking should be considered if high cumulative activities are expected [58]. These risks have to be weighed against the expected benefits of the RIT.
4.3. Metastatic Differentiated Thyroid Carcinoma
Distant metastases occur in patients with differentiated thyroid carcinoma with a prevalence of up to 10%. In particular, they affect lung and bone [59]. If a sufficient uptake of I-131 in metastases is measurable, different therapeutic approaches are to be weighed regarding risk and benefit.
If locoregional lymph node metastases are detectable, surgery should be performed. I-131 is used for iodine-avid metastases for treatment control after surgery or as an alternative therapy if no surgery is possible/planned (e.g., additional detection of distant metastases requiring RIT, previously performed radiotherapy, previous lymph node dissection).
In the case of micronodulary metastases of the lung RIT is carried out as a treatment with curative intent. Macronodulary pulmonary metastases should also be treated with I-131 in a curative intention but a complete remission is unlikely. Alternatively, (or in combination) the resectability can be evaluated.
The complete surgical resection of isolated bone metastases leads to an improved outcome. A combination of different therapeutic approaches like percutaneous radiotherapy, RIT and local interventional therapy could be helpful if symptomatic metastases of the bone cannot be (completely) resected. The same strategy is applied to brain metastases [14].
For the treatment of metastases, standard activities of 4–11 GBq (about 100–300 mCi) I-131 are given depending on individual patient characteristics like age, renal function, bone marrow depression and tumor load.
4.4. Thyroid Hormone Treatment
After thyroidectomy, life-long thyroid hormone therapy is required, usually as monotherapy with levothyroxine (LT4). Since TSH is able to promote the growth of remaining DTC cells, the dosage of LT4 should initially be high enough to achieve a suppression of thyrotropin. The thyroid function should be checked after 6 to 8 weeks. Depending on the result the dosage should be adjusted. An elevated level of triiodothyronine has to be avoided.
A long-term suppression of TSH to values <0.1 mU/L is currently only recommended for high-risk patients and patients with persistent disease indefinitely in the absence of specific contraindications [10]. In these cases, a better prognosis was demonstrated for the suppression of thyrotropin. No evidence-based data are available for optimal duration of TSH suppression.
According to the guidelines of the ATA, serum TSH should be maintained between 0.1 and 0.5 mU/L in patients with high-risk disease but excellent or intermediate response to therapy for up to 5 years and also in patients with a biochemical incomplete response taking into account the initial ATA risk classification published by Haugen et al. [10]. This recommendation is rated as weak with low-quality evidence. If the response to therapy is excellent biochemically and clinically in patients with a low risk for recurrence and there is no evidence of disease in the course of time, the serum level of TSH may be kept in a range of 0.5–2.0 mU/L, because there is no data showing a benefit of TSH suppression for low-risk patients.
Individual patient-related factors such as osteoporosis or osteopenia and cardiac co-morbidities like atrial fibrillation should always be taken into account during thyroid hormone therapy and weighed against the risk of recurrence. Especially in elderly patients >60 years, the use of TSH suppressive therapy should be carefully considered since the risk of such complications is significantly increased [60].
4.5. Follow-Up
Although the cumulative relapse rate is up to 30%, the life expectancy of DTC patients (pT1-3, pN0-1, M0) is not significantly different from the general population after therapy according to the current guidelines. Lifelong follow-up examinations should be carried out because relapses can occur even after decades and may be cured again. Initial checks should be carried out every six months (e.g., for the first 5 years after diagnosis). If there are no pathological findings later on, annual examinations are adequate [61]. The follow-up examination is based on the medical interview, clinical examination, cervical sonography, determination of TSH, triiodothyronine, levothyroxine, and thyroglobulin including Tg antibodies. In the case of postoperative hypoparathyroidism, the substitution therapy (cholecalciferol, calcium) should be checked and adapted (if necessary) to minimize the risk of osteoporosis.
A diagnostic whole-body scan is obligatory 6–12 months after initial RIT, a second scan is only needed in the case of relapse [10,62].
The criteria for a disease-free stage 6–12 months after primary therapy of DTC with total thyroidectomy ± radioiodine therapy are no clinical signs of DTC, no pathological uptake in the I-131 whole-body scan (only after remnant ablation) and a serum Tg below the detection limit (under suppression and after TSH stimulation, with absence of Tg antibodies) [10,62,63]. Under these conditions patients have a very low probability of relapse. If there are signs of relapse (e.g., elevated/rising serum levels of Tg) and no radioiodine-accumulating tumor tissue is detectable, clinical diagnostics should include the search for non-radioiodine-avid tumor tissue using F-18-fluorodeoxy-glucose positron emission tomography (FDG-PET) combined with computed tomography ideally under TSH-stimulation.
4.6. Tyrosine Kinase Inhibitors
For poorly differentiated thyroid carcinoma without relevant iodine metabolism and therefore very low radioiodine uptake, RIT is not a therapeutic option. Radioiodine resistance is currently defined as lesions without iodine uptake under TSH stimulation, progression in size in the year following RIT or persistent metastases after a cumulative dose of 22 GBq (600 mCi) I-131 of radioiodine. In these cases, complimentary diagnostic using FDG-PET/computed tomography (CT) is essential. FDG uptake is typically increased in poorly differentiated lesions that can be overlooked on radioiodine scans. Prognosis for radioiodine resistant thyroid cancer with distant metastases is very poor, with an estimated median survival time of about 2.5 to 3.5 years [64,65].
Chemotherapy comes at high toxicity with disappointing response rates [66]. For these patients a strict LT4 regime with TSH suppression is the best way to go. On showing rapid progression under such a regime, therapy options were few until recently.
Tyrosine kinase inhibitors like vandetanib, sorafenib and lenvatinib are a relatively new approach to systemic therapy in these cases. Tyrosine kinase receptors, the target structure of TKI, are trans-membrane proteins that mediate cell survival and proliferation [67]. If mutated, they can cause uncontrolled cell proliferation, dedifferentiation and apoptosis reduction. A large part of DTC show at least one mutation of RAF, RET or paired box gene 8 (PAX8)/peroxisome proliferator-activated receptor gamma (PPARγ) which makes them targets for TKI therapy. Furthermore, TKIs block receptors of the vascular endothelial growth factor (VEGF), fibroblast growth factor receptors and platelet-derived growth factor and thus inhibit tumor angiogenesis and lymphangiogenesis and cause hypoxia in malignant tissue [68]. TKIs, already approved for the treatment of irresectable liver cancer and renal carcinoma, promise to be an effective new tool for the treatment of poorly differentiated thyroid carcinoma (PDTC) [66].
A recent review on the use of sorafenib, sunitinib and lenvatinib showed a benefit for progression-free survival of up to five months [69]. While initially showing partial response or at least disease stabilization after sorafenib, the first TKI approved for thyroid cancer, patients almost always develop resistance over the course of the following one to two years. Switching to another TKI is possible at this point [70]. A study using lenvatinib was able to indicate prolonged progression-free survival regardless of BRAF or RAS mutation status, suggesting a diminished role of these pathways [71]. However, a benefit in overall survival could not be found.
Therapy with kinase inhibitors may be accompanied by severe side effects. Induced hypertension is one of the most common; the underlying pathophysiology is yet unclear. Vasoconstriction following reduced nitric oxide production via inhibition of the VEGF-PI3K pathway is discussed. A reduction of peripheral arterioles due to antiangiogenic effects resulting in increased peripheral resistance and an activation of the endothelin-1-system causing vasoconstriction have also been suggested [72]. Other side effects may include diarrhea, fatigue, hepatotoxicity, skin changes, nausea, increased LT4 dosage requirement, changes in taste and weight loss and associated with a severe decrease of quality of life [69].
Keeping this in mind kinase inhibitors can certainly not be considered as a standard regime or an alternative to TSH-suppression. For patients with radioiodine-refractory DTC they can be a useful complementation to standard therapy.
While undergoing TKI therapy patients can display somewhat inconclusive lab results. Normally a reliable parameter, thyroglobulin levels can fluctuate under TKI treatment. These changes do not necessarily represent the actual course of the disease as it is monitored in anatomical imaging. Sufficient therapeutic monitoring not only by relying on lab tests but also on CT or PET/CT diagnosis to determine a morphologic or metabolic response is essential [73].
Considering the extensive side effects, this therapy should be reserved for patients with rapid tumor progression and severe to life threatening symptoms. In these cases, the decision for TKI therapy should be made in a interdisciplinary manner, carefully weighed against local strategies like radiotherapy and local surgery [74]. TKI treatment should only be performed by a team of physicians experienced with side effects management.
The European guidelines for treating differentiated thyroid carcinoma are from 2008. Kinase inhibitors are therefore not considered there [8] and a unanimous European recommendation is still awaited.
4.7. Papillary Microcarcinoma
Because of the excellent prognosis of papillary microcarcinoma (PTMC), a hemithyroidectomy without RIT is regarded as sufficient therapy, if there is no sign of local invasion, lymph node and/or distant metastases. The substitution of LT4 should keep the serum level of TSH in a euthyroid metabolic state.
In a meta-analysis, PTMC showed a prevalence of distant metastases of 0.4%, a probability of locoregional relapse of 2.5% but also a prevalence of micrometastases in locoregional lymph nodes of 12–50% [45]. The risk of lymphogenic micrometastases increases with increasing tumor diameter [75]. Using single photon emission computed tomography (SPECT) combined with CT, other studies showed a prevalence of lymph node metastases up to 57% [76,77]. The relapse-free survival in patients with PTMC after 5 years was 78.6% without RIT compared to 95.0% in patients that have had a remnant ablation with RIT [78]. The recommendation for a RIT in PTMC is based on the extent of resection and the individual risk profile. Risk factors are multifocality, infiltration of the thyroid gland, histological variants of papillary thyroid carcinoma, low degree of differentiation, tumor diameter 6–10 mm, molecular markers like BRAF-V600E mutation, infiltrative tumor growth, surrounding desmoplastic fibrosis and previous percutaneous irradiation of the neck [14]. In patients with a residual thyroid gland (e.g., after lobectomy) an ablative RIT is not indicated.
5. Summary and Conclusion
Differentiated thyroid cancer is a rare tumor entity but shows a strongly increasing incidence over the last decades. It derives from the follicular epithelium of the thyroid and shows basic biological characteristics of healthy thyroid tissue. The expression of the sodium iodide symporter is the key feature for specific iodine uptake. Patients with DTC have an excellent prognosis.
The therapeutic approach including surgery and remnant ablation with radioiodine should be risk-adapted to achieve an optimal treatment and to minimize treatment-related morbidity. Overtreatment should be avoided.
With regard to so-called low-risk carcinoma defined by the ATA there are controversial therapeutic approaches. The guidelines of the ATA recommend a lobectomy under certain conditions. Following the guidelines of the EANM a thyreodectomy with RIT should be performed (except PTC pT1a). However, long-term studies are currently not available. These studies are certainly necessary (against the background of the slow growth of the well-differentiated thyroid carcinoma) to decide which approach is appropriate. A risk-stratified follow-up is required since recurrences can occur over years. Furthermore, thyroid hormone substitution must be controlled.
The life span of most DTC patients does not differ from general population when appropriate treatment is given. The prognosis becomes poorer in patients with radioiodine refractory thyroid carcinoma. TKI have shown clinical effectiveness in iodine-refractory DTC with regard to progression free survival. A positive effect on overall survival could not be shown yet and has to be evaluated in further studies. However, therapy should be carried out in centers with special expertise.
In the current guidelines of the ATA and EANM there is no evidence-based treatment concept (or strong recommendation) for every situation. There are still open questions:
- The value of RIT under the condition of increasing serum level of Tg without a detectable correlatation in the morphological or functional imaging (i.e. iodine-negative whole-body scan);
- The benefit of a remnant ablation in patients with papillary microcarcinoma (very low risk of relapse, lymph node metastasis possible);
- Optimal activities of I-131 for safe and effective radioiodine ablation;
- The role of rhTSH as preparation for RIT to treat incomplete or non-resectable local recurrence or metastases;
- The role of a short LT4 withdrawal to reduce blood levels of iodine before RIT or diagnostic whole-body scan.
An analysis by the Cancer Genome Atlas Research Network identifies previously unknown genetic alterations and molecular subtypes of PTC. These alterations may lead to a more accurate diagnosis of tumors and potentially more targeted treatment [79]. Although in the current guidelines no explicit recommendation concerning the determination of molecular markers in the cyto-/histopathological specimen is made, further adjustments are to be expected in the future.
Author Contributions
The manuscript was written by Benedikt Schmidbauer, Karin Menhart and Jirka Grosse, the systematic literature research and corrections were done by Dirk Hellwig and Jirka Grosse, Jirka Grosse concieved the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| AKT1 | RAC-α serine/threonine-protein kinase 1 |
| ATA | American Thyroid Association |
| CT | computed tomography |
| DTC | differentiated thyroid carcinoma |
| EANM | European Association of Nuclear Medicine |
| ETE | extrathyroidal extension |
| ETA | European Thyroid Association |
| FAP | familial adenomatous polyposis |
| FNA | fine-needle aspiration biopsy |
| FTC | follicular thyroid carcinoma |
| FDG-PET | F-18-fluorodeoxy-glucose positron emission tomography |
| LT4 | levothyroxine |
| MEN2 | multiple endocrine neoplasia type 2 |
| PAX8 | paired box gene 8 |
| PDTC | poorly differentiated thyroid carcinoma |
| PIK3CA | phosphatidylinositol 4,5-bisphosphate 3-kinase catalytic subunit α |
| PPARγ | peroxisome proliferator-activated receptor gamma |
| PTC | papillary thyroid carcinoma |
| PTEN | phosphatase and tensin homolog |
| PTMC | papillary microcarcinoma |
| RET | RET proto-oncogene |
| rhTSH | recombinant thyrotropin |
| RIT | radioiodine therapy |
| SPECT | single photon emission computed tomography |
| TERT | telomerase reverse transcriptase |
| Tg | serum thyroglobulin |
| TKI | receptor tyrosine kinase inhibitors |
| TP53 | tumor protein p53 |
| TSH | thyroid-stimulating hormone (also known as thyrotropin) |
| VEGF | vascular endothelial growth factor |
| WHO | World Health Organization |
References
- Hegedüs, L. Clinical practice. The thyroid nodule. N. Engl. J. Med. 2004, 351, 1764–1771. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer statistics, 2014. CA Cancer J. Clin. 2014, 64, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Leenhardt, L.; Bernier, M.O.; Boin-Pineau, M.H.; Conte Devolx, B.; Maréchaud, R.; Niccoli-Sire, P.; Nocaudie, M.; Orgiazzi, J.; Schlumberger, M.; Wémeau, J.L.; et al. Advances in diagnostic practices affect thyroid cancer incidence in France. Eur. J. Endocrinol. 2004, 150, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.I. Thyroid carcinoma. Lancet 2003, 361, 501–511. [Google Scholar] [CrossRef]
- Aschebrook-Kilfoy, B.; Schechter, R.B.; Shih, Y.C.; Kaplan, E.L.; Chiu, B.C.; Angelos, P.; Grogan, R.H. The clinical and economic burden of a sustained increase in thyroid cancer incidence. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1252–1259. [Google Scholar] [CrossRef] [PubMed]
- Leenhardt, L.; Erdogan, M.F.; Hegedus, L.; Mandel, S.J.; Paschke, R.; Rago, T.; Russ, G. 2013 European thyroid association guidelines for cervical ultrasound scan and ultrasound-guided techniques in the postoperative management of patients with thyroid cancer. Eur. Thyroid J. 2013, 2, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, E.B.; Alavi, A.; Balon, H.R.; Clarke, S.E.; Divgi, C.; Gelfand, M.J.; Goldsmith, S.J.; Jadvar, H.; Marcus, C.S.; Martin, W.H.; et al. The SNMMI practice guideline for therapy of thyroid disease with 131I 3.0. J. Nucl. Med. 2012, 53, 1633–1651. [Google Scholar] [CrossRef] [PubMed]
- Luster, M.; Clarke, S.E.; Dietlein, M.; Lassmann, M.; Lind, P.; Oyen, W.J.; Tennvall, J.; Bombardieri, E.; European Association of Nuclear Medicine (EANM). Guidelines for radioiodine therapy of differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1941–1959. [Google Scholar] [CrossRef] [PubMed]
- Takami, H.; Ito, Y.; Okamoto, T.; Onoda, N.; Noguchi, H.; Yoshida, A. Revisiting the guidelines issued by the Japanese Society of Thyroid Surgeons and Japan Association of Endocrine Surgeons: A gradual move towards consensus between Japanese and western practice in the management of thyroid carcinoma. World J. Surg. 2014, 38, 2002–2010. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed]
- Francis, G.L.; Waguespack, S.G.; Bauer, A.J.; Angelos, P.; Benvenga, S.; Cerutti, J.M.; Dinauer, C.A.; Hamilton, J.; Hay, I.D.; Luster, M.; et al. Management guidelines for children with thyroid nodules and differentiated thyroid cancer. Thyroid 2015, 25, 716–759. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Weinheim, Germany, 2017; pp. 69–71. [Google Scholar]
- Armin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017; pp. 1–19. [Google Scholar]
- Dietlein, M.; Eschner, W.; Grünwald, F.; Lassmann, M.; Verburg, F.A.; Luster, M. Procedure guidelines for radioiodine therapy of differentiated thyroid cancer. Version 4. Nuklearmedizin 2016, 55, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Penna, G.C.; Vaisman, F.; Vaisman, M.; Sobrinho-Simões, M.; Soares, P. Molecular Markers Involved in Tumorigenesis of Thyroid Carcinoma: Focus on Aggressive Histotypes. Cytogenet. Genome Res. 2016, 150, 194–207. [Google Scholar] [CrossRef] [PubMed]
- Nikiforov, Y.E.; Ohori, N.P. Papillary Carcinoma. In Diagnostic Pathology and Molecular Genetics of the Thyroid, 1st ed.; Nikiforov, Y.E., Biddinger, P.W., Thompson, L.D.R., Eds.; Lippincott: Philadelphia, PA, USA, 2012; pp. 183–262. [Google Scholar]
- Seethala, R.R.; Asa, S.L.; Carty, S.E.; Hodak, S.P.; McHugh, J.B.; Richardson, M.S.; Shah, J.; Thompson, L.D.R.; Nikiforov, Y.E. For the Members of the Cancer Committee, College of American Pathologists. Protocol for the Examination of Specimens From Patients With Carcinomas of the Thyroid Gland, Based on AJCC/UICC TNM, 7th edition. Version: Thyroid 3.2.0.0. Available online: http://www.cap.org/ShowProperty?nodePath=/UCMCon/Contribution%20Folders/WebContent/pdf/cp-thyroid-16protocol-3200.pdf (accessed on 2 June 2017).
- Nikiforova, M.N.; Kimura, E.T.; Gandhi, M.; Biddinger, P.W.; Knauf, J.A.; Basolo, F.; Zhu, Z.; Giannini, R.; Salvatore, G.; Fusco, A.; et al. BRAF mutations in thyroid tumors are restricted to papillary carcinomas and anaplastic or poorly differentiated carcinomas arising from papillary carcinomas. J. Clin. Endocrinol. Metab. 2003, 88, 5399–5404. [Google Scholar] [CrossRef] [PubMed]
- Asioli, S.; Erickson, L.A.; Sebo, T.J.; Zhang, J.; Jin, L.; Thompson, G.B.; Lloyd, R.V. Papillary thyroid carcinoma with prominent hobnail features: A new aggressive variant of moderately differentiated papillary carcinoma. A clinicopathologic, immunohistochemical, and molecular study of eight cases. Am. J. Surg. Pathol. 2010, 34, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Cardis, E.; Howe, G.; Ron, E.; Bebeshko, V.; Bogdanova, T.; Bouville, A.; Carr, Z.; Chumak, V.; Davis, S.; Demidchik, Y.; et al. Cancer consequences of the Chernobyl accident: 20 years on. J. Radiol. Prot. 2006, 26, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Nikiforov, Y.E. Radiation-induced thyroid cancer: What we have learned from Chernobyl. Endocr. Pathol. 2006, 17, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Howitt, B.E.; Jia, Y.; Sholl, L.M.; Barletta, J.A. Molecular alterations in partially-encapsulated or well-circumscribed follicular variant of papillary thyroid carcinoma. Thyroid 2013, 23, 1256–1262. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Singh, B.; Tallini, G.; Carlson, D.L.; Katabi, N.; Shaha, A.; Tuttle, R.M.; Ghossein, R.A. Follicular variant of papillary thyroid carcinoma: A clinicopathologic study of a problematic entity. Cancer 2006, 107, 1255–1264. [Google Scholar] [CrossRef] [PubMed]
- Brennan, M.D.; Bergstralh, E.J.; van Heerden, J.A.; McConahey, W.M. Follicular thyroid cancer treated at the Mayo Clinic, 1946 through 1970: Initial manifestations, pathologic findings, therapy, and outcome. Mayo Clin. Proc. 1991, 66, 11–22. [Google Scholar] [CrossRef]
- Collini, P.; Sampietro, G.; Pilotti, S. Extensive vascular invasion is a marker of risk of relapse in encapsulated non-Hürthle cell follicular carcinoma of the thyroid gland: A clinicopathological study of 18 consecutive cases from a single institution with a 11-year median follow-up. Histopathology 2004, 44, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Lang, W.; Choritz, H.; Hundeshagen, H. Risk factors in follicular thyroid carcinomas. A retrospective follow-up study covering a 14-year period with emphasis on morphological findings. Am. J. Surg. Pathol. 1986, 10, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Hundahl, S.A.; Fleming, I.D.; Fremgen, A.M.; Menck, H.R. A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985–1995. Cancer 1998, 83, 2638–2648. [Google Scholar] [CrossRef]
- Haigh, P.I.; Urbach, D.R. The treatment and prognosis of Hürthle cell follicular thyroid carcinoma compared with its non-Hürthle cell counterpart. Surgery 2005, 138, 1152–1157. [Google Scholar] [CrossRef] [PubMed]
- Shaha, A.R.; Loree, T.R.; Shah, J.P. Prognostic factors and risk group analysis in follicular carcinoma of the thyroid. Surgery 1995, 118, 1131–1136. [Google Scholar] [CrossRef]
- Cetta, F.; Montalto, G.; Gori, M.; Curia, M.C.; Cama, A.; Olschwang, S. Germline mutations of the APC gene in patients with familial adenomatous polyposis-associated thyroid carcinoma: Results from a European cooperative study. J. Clin. Endocrinol. Metab. 2000, 85, 286–292. [Google Scholar] [PubMed]
- Harach, H.R.; Williams, G.T.; Williams, E.D. Familial adenomatous polyposis associated thyroid carcinoma: A distinct type of follicular cell neoplasm. Histopathology 1994, 25, 549–561. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Miyauchi, A.; Ishikawa, H.; Hirokawa, M.; Kudo, T.; Tomoda, C.; Miya, A. Our experience of treatment of cribriform morular variant of papillary thyroid carcinoma; difference in clinicopathological features of FAP-associated and sporadic patients. Endocr. J. 2011, 58, 685–689. [Google Scholar] [CrossRef] [PubMed]
- Hollander, M.C.; Blumenthal, G.M.; Dennis, P.A. PTEN loss in the continuum of common cancers, rare syndromes and mouse models. Nat. Rev. Cancer 2011, 11, 289–301. [Google Scholar] [CrossRef] [PubMed]
- Laury, A.R.; Bongiovanni, M.; Tille, J.C.; Kozakewich, H.; Nosé, V. Thyroid pathology in PTEN-hamartoma tumor syndrome: Characteristic findings of a distinct entity. Thyroid 2011, 21, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Nosé, V. Familial thyroid cancer: A review. Mod. Pathol. 2011, 24, S19–S33. [Google Scholar] [CrossRef] [PubMed]
- Dean, D.S.; Gharib, H. Epidemiology of thyroid nodules. Best Pract. Res. Clin. Endocrinol. Metab. 2008, 22, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Vanderpump, M.P. The epidemiology of thyroid disease. Br. Med. Bull. 2011, 99, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Feldkamp, J.; Führer, D.; Luster, M.; Musholt, T.J.; Spitzweg, C.; Schott, M. Fine Needle Aspiration in the Investigation of Thyroid Nodules. Dtsch. Arztebl. Int. 2016, 113, 353–359. [Google Scholar] [PubMed]
- Dralle, H.; Musholt, T.J.; Schabram, J.; Steinmüller, T.; Frilling, A.; Simon, D.; Goretzki, P.E.; Niederle, B.; Scheuba, C.; Clerici, T.; et al. German Association of Endocrine Surgeons practice guideline for the surgical management of malignant thyroid tumors. Langenbecks Arch. Surg. 2013, 398, 347–375. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferri, E.L.; Jhiang, S.M. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am. J. Med. 1994, 97, 418–428. [Google Scholar] [CrossRef]
- Samaan, N.A.; Schultz, P.N.; Hickey, R.C.; Goepfert, H.; Haynie, T.P.; Johnston, D.A.; Ordonez, N.G. The results of various modalities of treatment of well differentiated thyroid carcinomas: A retrospective review of 1599 patients. J. Clin. Endocrinol. Metab. 1992, 75, 714–720. [Google Scholar] [PubMed]
- Sawka, A.M.; Thephamongkhol, K.; Brouwers, M.; Thabane, L.; Browman, G.; Gerstein, H.C. Clinical review 170: A systematic review and metaanalysis of the effectiveness of radioactive iodine remnant ablation for well-differentiated thyroid cancer. J. Clin. Endocrinol. Metab. 2004, 89, 3668–3676. [Google Scholar] [CrossRef] [PubMed]
- Sawka, A.M.; Brierley, J.D.; Tsang, R.W.; Thabane, L.; Rotstein, L.; Gafni, A.; Straus, S.; Goldstein, D.P. An updated systematic review and commentary examining the effectiveness of radioactive iodine remnant ablation in well-differentiated thyroid cancer. Endocrinol. Metab. Clin. N. Am. 2008, 37, 457–480. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, H.; Al-Maqbili, T.; Carter, B.; Martin, E.; Campain, N.; Watkinson, J.; McCabe, C.; Boelaert, K.; Franklyn, J.A. Differences in the recurrence and mortality outcomes rates of incidental and nonincidental papillary thyroid microcarcinoma: A systematic review and meta-analysis of 21,329 person-years of follow-up. J. Clin. Endocrinol. Metab. 2014, 99, 2834–2843. [Google Scholar] [CrossRef] [PubMed]
- Perros, P.; Boelaert, K.; Colley, S.; Evans, C.; Evans, R.M.; Gerrard, B.G.; Gilbert, J.; Harrison, B.; Johnson, S.J.; Giles, T.E.; et al. British Thyroid Association. Guidelines for the management of thyroid cancer. Clin. Endocrinol. 2014, 81, 1–122. [Google Scholar] [CrossRef] [PubMed]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Sherman, S.I.; Tuttle, R.M.; et al. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2006, 16, 109–142. [Google Scholar] [CrossRef] [PubMed]
- Luster, M.; Felbinger, R.; Dietlein, M.; Reiners, C. Thyroid hormone withdrawal in patients with differentiated thyroid carcinoma: A one hundred thirty-patient pilot survey on consequences of hypothyroidism and a pharmacoeconomic comparison to recombinant thyrotropin administration. Thyroid 2005, 15, 1147–1155. [Google Scholar] [CrossRef] [PubMed]
- Pacini, F.; Ladenson, P.W.; Schlumberger, M.; Driedger, A.; Luster, M.; Kloos, R.T.; Sherman, S.; Haugen, B.; Corone, C.; Molinaro, E.; et al. Radioiodine ablation of thyroid remnants after preparation with recombinant human thyrotropin in differentiated thyroid carcinoma: Results of an international, randomized, controlled study. J. Clin. Endocrinol. Metab. 2006, 91, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Ladenson, P.W.; Braverman, L.E.; Mazzaferri, E.L.; Brucker-Davis, F.; Cooper, D.S.; Garber, J.R.; Wondisford, F.E.; Davies, T.F.; DeGroot, L.J.; Daniels, G.H.; et al. Comparison of administration of recombinant human thyrotropin with withdrawal of thyroid hormone for radioactive iodine scanning in patients with thyroid carcinoma. N. Engl. J. Med. 1997, 337, 888–896. [Google Scholar] [CrossRef] [PubMed]
- Luster, M. Acta Oncologica Lecture. Present status of the use of recombinant human TSH in thyroid cancer management. Acta Oncol. 2006, 45, 1018–1030. [Google Scholar] [CrossRef] [PubMed]
- Schlumberger, M.; Ricard, M.; De Pouvourville, G.; Pacini, F. How the availability of recombinant human TSH has changed the management of patients who have thyroid cancer. Nat. Clin. Pract. Endocrinol. Metab. 2007, 3, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Mallick, U.; Harmer, C.; Yap, B.; Wadsley, J.; Clarke, S.; Moss, L.; Nicol, A.; Clark, P.M.; Farnell, K.; McCready, R.; et al. Ablation with low-dose radioiodine and thyrotropin alfa in thyroid cancer. N. Engl. J. Med. 2012, 366, 1674–1685. [Google Scholar] [CrossRef] [PubMed]
- Schlumberger, M.; Catargi, B.; Borget, I.; Deandreis, D.; Zerdoud, S.; Bridji, B.; Bardet, S.; Leenhardt, L.; Bastie, D.; Schvartz, C.; et al. Strategies of radioiodine ablation in patients with low-risk thyroid cancer. N. Engl. J. Med. 2012, 366, 1663–1673. [Google Scholar] [CrossRef] [PubMed]
- Kukulska, A.; Krajewska, J.; Gawkowska-Suwińska, M.; Puch, Z.; Paliczka-Cieslik, E.; Roskosz, J.; Handkiewicz-Junak, D.; Jarzab, M.; Gubała, E.; Jarzab, B. Radioiodine thyroid remnant ablation in patients with differentiated thyroid carcinoma (DTC): Prospective comparison of long-term outcomes of treatment with 30, 60 and 100 mCi. Thyroid Res. 2010, 3, 9. [Google Scholar] [CrossRef] [PubMed]
- Fallahi, B.; Beiki, D.; Takavar, A.; Fard-Esfahani, A.; Gilani, K.A.; Saghari, M.; Eftekhari, M. Low versus high radioiodine dose in postoperative ablation of residual thyroid tissue in patients with differentiated thyroid carcinoma: A large randomized clinical trial. Nucl. Med. Commun. 2012, 33, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Robbins, R.J.; Chon, J.T.; Fleisher, M.; Larson, S.M.; Tuttle, R.M. Is the serum thyroglobulin response to recombinant human thyrotropin sufficient, by itself, to monitor for residual thyroid carcinoma? J. Clin. Endocrinol. Metab. 2002, 87, 3242–3247. [Google Scholar] [CrossRef] [PubMed]
- Rubino, C.; de Vathaire, F.; Dottorini, M.E.; Hall, P.; Schvartz, C.; Couette, J.E.; Dondon, M.G.; Abbas, M.T.; Langlois, C.; Schlumberger, M. Second primary malignancies in thyroid cancer patients. Br. J. Cancer 2003, 89, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Wichers, M.; Benz, E.; Palmedo, H.; Biersack, H.J.; Grünwald, F.; Klingmüller, D. Testicular function after radioiodine therapy for thyroid carcinoma. Eur. J. Nucl. Med. 2000, 27, 503–507. [Google Scholar] [CrossRef] [PubMed]
- Benbassat, C.A.; Mechlis-Frish, S.; Hirsch, D. Clinicopathological characteristics and long-term outcome in patients with distant metastases from differentiated thyroid cancer. World J. Surg. 2006, 30, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Abonowara, A.; Quraishi, A.; Sapp, J.L.; Alqambar, M.H.; Saric, A.; O’Connell, C.M.; Rajaraman, M.M.; Hart, R.D.; Imran, S.A. Prevalence of atrial fibrillation in patients taking TSH suppression therapy for management of thyroid cancer. Clin. Investig. Med. 2012, 35, E152–E156. [Google Scholar] [CrossRef] [PubMed]
- Tiedje, V.; Schmid, K.W.; Weber, F.; Bockisch, A.; Führer, D. Differentiated thyroid cancer. Internist 2015, 56, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Pacini, F.; Schlumberger, M.; Dralle, H.; Elisei, R.; Smit, J.W.; Wiersinga, W.; European Thyroid Cancer Taskforce. European consensus for the management of patients with differentiated thyroid carcinoma of the follicular epithelium. Eur. J. Endocrinol. 2006, 154, 787–803. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, R.M.; Tala, H.; Shah, J.; Leboeuf, R.; Ghossein, R.; Gonen, M.; Brokhin, M.; Omry, G.; Fagin, J.A.; Shaha, A. Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: Using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid 2010, 20, 1341–1349. [Google Scholar] [PubMed]
- Durante, C.; Haddy, N.; Baudin, E.; Leboulleux, S.; Hartl, D.; Travagli, J.P.; Caillou, B.; Ricard, M.; Lumbroso, J.D.; De Vathaire, F.; et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: Benefits and limits of radioiodine therapy. J. Clin. Endocrinol. Metab. 2006, 91, 2892–2899. [Google Scholar] [CrossRef] [PubMed]
- Robbins, R.J.; Wan, Q.; Grewal, R.K.; Reibke, R.; Gonen, M.; Strauss, H.W.; Tuttle, R.M.; Drucker, W.; Larson, S.M. Real-time prognosis for metastatic thyroid carcinoma based on 2-[18F]fluoro-2-deoxy-d-glucose-positron emission tomography scanning. J. Clin. Endocrinol. Metab. 2006, 91, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.I. Early clinical studies of novel therapies for thyroid cancers. Endocrinol. Metab. Clin. N. Am. 2008, 37, 511–524. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Kreissl, M.C.; Weismann, D.; Allolio, B. New targets and therapeutic approaches for endocrine malignancies. Pharmacol. Ther. 2009, 123, 117–141. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, L.; Pieruzzi, L.; Biagini, A.; Sabini, E.; Valerio, L.; Giani, C.; Passannanti, P.; Pontillo-Contillo, B.; Battaglia, V.; Mazzeo, S.; et al. Lenvatinib and other tyrosine kinase inhibitors for the treatment of radioiodine refractory, advanced, and progressive thyroid cancer. Onco Targets Ther. 2016, 9, 6467–6477. [Google Scholar] [CrossRef] [PubMed]
- Laursen, R.; Wehland, M.; Kopp, S.; Pietsch, J.; Infanger, M.; Grosse, J.; Grimm, D. Effects and Role of Multikinase Inhibitors in Thyroid Cancer. Curr. Pharm. Des. 2016, 22, 5915–5926. [Google Scholar] [CrossRef] [PubMed]
- Pitoia, F.; Jerkovich, F. Selective use of sorafenib in the treatment of thyroid cancer. Drug Des. Dev. Ther. 2016, 10, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Schlumberger, M.; Tahara, M.; Wirth, L.J.; Robinson, B.; Brose, M.S.; Elisei, R.; Habra, M.A.; Newbold, K.; Shah, M.H.; Hoff, A.O.; et al. Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N. Engl. J. Med. 2015, 372, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Ancker, O.V.; Wehland, M.; Bauer, J.; Infanger, M.; Grimm, D. The Adverse Effect of Hypertension in the Treatment of Thyroid Cancer with Multi-Kinase Inhibitors. Int. J. Mol. Sci. 2017, 18, 625. [Google Scholar] [CrossRef] [PubMed]
- Werner, R.A.; Lückerath, K.; Schmid, J.S.; Higuchi, T.; Kreissl, M.C.; Grelle, I.; Reiners, C.; Buck, A.K.; Lapa, C. Thyroglobulin fluctuations in patients with iodine-refractory differentiated thyroid carcinoma on lenvatinib treatment—initial experience. Sci. Rep. 2016, 6, 28081. [Google Scholar] [CrossRef] [PubMed]
- Kreissl, M.C.; Fassnacht, M.; Mueller, S.P. Systemic treatment of advanced differentiated and medullary thyroid cancer. Overview and practical aspects. Nuklearmedizin 2015, 54, 88–93. [Google Scholar] [PubMed]
- Machens, A.; Holzhausen, H.J.; Dralle, H. The prognostic value of primary tumor size in papillary and follicular thyroid carcinoma. Cancer 2005, 103, 2269–2273. [Google Scholar] [CrossRef] [PubMed]
- Gallicchio, R.; Giacomobono, S.; Capacchione, D.; Nardelli, A.; Barbato, F.; Nappi, A.; Pellegrino, T.; Storto, G. Should patients with remnants from thyroid microcarcinoma really not be treated with iodine-131 ablation? Endocrine 2013, 44, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Avram, A.M.; Fig, L.M.; Frey, K.A.; Gross, M.D.; Wong, K.K. Preablation 131-I scans with SPECT/CT in postoperative thyroid cancer patients: What is the impact on staging? J. Clin. Endocrinol. Metab. 2013, 98, 1163–1171. [Google Scholar] [CrossRef] [PubMed]
- Creach, K.M.; Siegel, B.A.; Nussenbaum, B.; Grigsby, P.W. Radioactive iodine therapy decreases recurrence in thyroid papillary microcarcinoma. ISRN Endocrinol. 2012, 2012, 816386. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Integrated genomic characterization of papillary thyroid carcinoma. Cell 2014, 159, 676–690. [Google Scholar]
Figure 1.
Diagnostic algorithm for the evaluation of thyroid nodules (modified from [38]). TSH: thyroid-stimulating hormone.
Figure 1.
Diagnostic algorithm for the evaluation of thyroid nodules (modified from [38]). TSH: thyroid-stimulating hormone.

{kind=link}
Table 1.
TNM Classification of thyroid cancer, 8th edition (modified from [12]).
Table 1.
TNM Classification of thyroid cancer, 8th edition (modified from [12]).
| TX | Primary Tumor Cannot be Assessed |
| T0 | No evidence of primary tumor |
| T1 | Tumor size maximum 2 cm, limited to the thyroid |
| T1a | Tumor size maximum 1 cm, limited to the thyroid |
| T1b | Tumor size >1 cm up to a maximum of 2 cm, limited to the thyroid |
| T2 | Tumor size >2 cm up to 4 cm, limited to the thyroid |
| T3 | Tumor size >4 cm, limited to the thyroid, or any tumor with macroscopic extrathyroidal extension (Musculus sternohyoideus, Musculus sternothyreoideus, Musculus omohyoideus) |
| T3a | Tumor size >4 cm, limited to the thyroid |
| T3b | Any tumor with macroscopic extrathyroidal extension (M. sternohyoideus, M. sternothyreoideus, M. omohyoideus) |
| T4a | Any tumor size with extrathyroidal extension beyond the thyroid capsule and invasion of subcutaneous soft tissue, larynx, trachea, esophagus and/or recurrent laryngeal nerve |
| T4b | Any tumor size with invasion of prevertebral fascia, mediastinal vessels or carotid artery |
| NX | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastases |
| N1 | Regional lymph node metastases |
| N1a | Lymph node metastases unilateral in level VI or upper mediastinum |
| N1b | Metastases in other unilateral, bilateral or contralateral cervical lymph nodes (level I, II, III, IV and V) or retropharyngeal |
| M0 | No distant metastases |
| M1 | Distant metastases |
Table 2.
Mutations of BRAF and TERTp in follicular-derived thyroid carcinoma and clinicopathological impact (modified from [15]).
Table 2.
Mutations of BRAF and TERTp in follicular-derived thyroid carcinoma and clinicopathological impact (modified from [15]).
| Mutation | Histology | Clinicopathological Associations |
|---|---|---|
| BRAF | papillary thyroid carcinoma (PTC) | recurrence, multifocality, extrathyreoidal extension, lymph nodes metastasis, advanced stage, absence of capsule, vascular invasion, more aggressive histological subtype |
| BRAF | micro PTC | multifocality, extrathyreoidal extension, advanced stage, lymph node metastasis |
| BRAF | thyroid carcinoma derived from follicular cells | no association |
| TERT | papillary thyroid carcinoma | more advanced stage by tall cell variant, higher tumor size, vascular invasion, older age, poor outcome, lymph node and distant metastasis |
| TERT | thyroid carcinoma derived from follicular cells | more aggressive histologic variants, concomitant presence of mutated RAS/BRAF, age > 45, higher tumor size, vascular invasion, persistent or recurrent disease, lymph node metastasis |
Table 3.
WHO classification of papillary and follicular carcinoma of the thyroid (modified from [17]).
Table 3.
WHO classification of papillary and follicular carcinoma of the thyroid (modified from [17]).
| Histology | Histological Variants |
|---|---|
| Papillary carcinoma | Classic (usual) Clear cell variant Columnar cell variant Cribriform-morular variant Diffuse sclerosing variant Follicular variant Macrofollicular variant Microcarcinoma (occult, latent, small, microtumor) Oncocytic or oxyphilic variant (follicular/nonfollicular variant) Solid variant Tall cell variant Warthin-like variant |
| Follicular carcinoma | Clear cell variant Oncocytic (Hürthle cell) variant Mucinous variant With signet-ring cells |
Table 4.
Sonographic patterns and risk of malignancy (modified from [10]).
Table 4.
Sonographic patterns and risk of malignancy (modified from [10]).
| Ultrasound Features | Estimated Risk of Malignancy | Sonographic Pattern | FNA Size Cutoff |
|---|---|---|---|
| Solid hypoechogenic nodule or solid hypoechogenic component of a partially cystic nodule with one or more of the following features: irregular margins, microcalcification, taller rather than wide shape, rim calcifications with small extrusive soft tissue component, evidence of extrathyroidal extension (ETE) | >70–90% | Highly suspicious | >1 cm |
| Solid hypoechogenic nodule with smooth margins without microcalcification, taller rather than wide shape or signs of ETE | 10–20% | Intermediate suspicion | >1 cm |
| Isoechogenic solid nodule or partally cystic nodule with eccentric solid areas without microcalcification, taller rather than wide shape or signs of ETE | 5–10% | Low suspicion | >1.5 cm |
| Spongiform or partially cystic nodule without any of the sonographic features described above | <3% | Very low suspicion | >2 cm, alternative: observation without fine needle aspiration (FNA) |
| Purely cystic nodules without solid components | <1% | Benign | No biopsy |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Schmidbauer, B.; Menhart, K.; Hellwig, D.; Grosse, J. Differentiated Thyroid Cancer—Treatment: State of the Art. Int. J. Mol. Sci. 2017, 18, 1292. https://doi.org/10.3390/ijms18061292
AMA Style
Schmidbauer B, Menhart K, Hellwig D, Grosse J. Differentiated Thyroid Cancer—Treatment: State of the Art. International Journal of Molecular Sciences. 2017; 18(6):1292. https://doi.org/10.3390/ijms18061292
Chicago/Turabian StyleSchmidbauer, Benedikt, Karin Menhart, Dirk Hellwig, and Jirka Grosse. 2017. "Differentiated Thyroid Cancer—Treatment: State of the Art" International Journal of Molecular Sciences 18, no. 6: 1292. https://doi.org/10.3390/ijms18061292
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.