
MALDI Mass Spectrometry Imaging Reveals Decreased CK5 Levels in Vulvar Squamous Cell Carcinomas Compared to the Precursor Lesion Differentiated Vulvar Intraepithelial Neoplasia

 ,
, 
Abstract
:
1. Introduction
2. Results
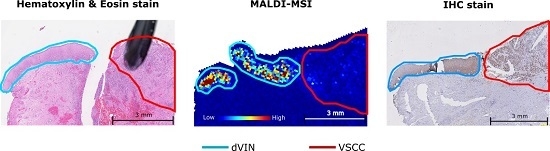
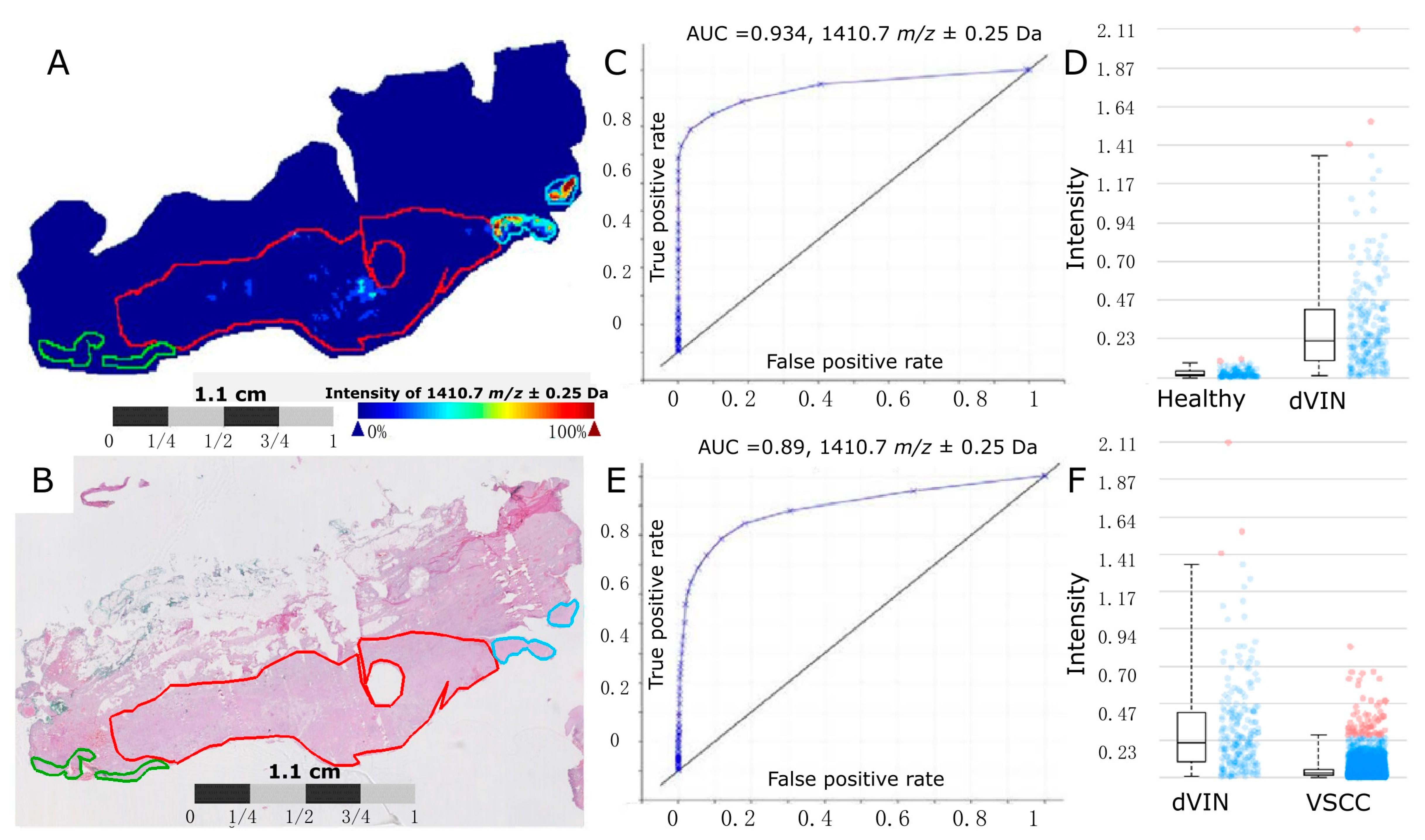
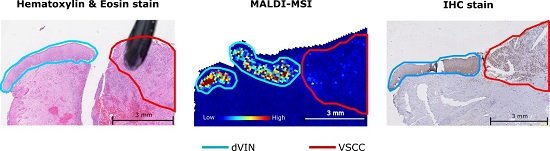
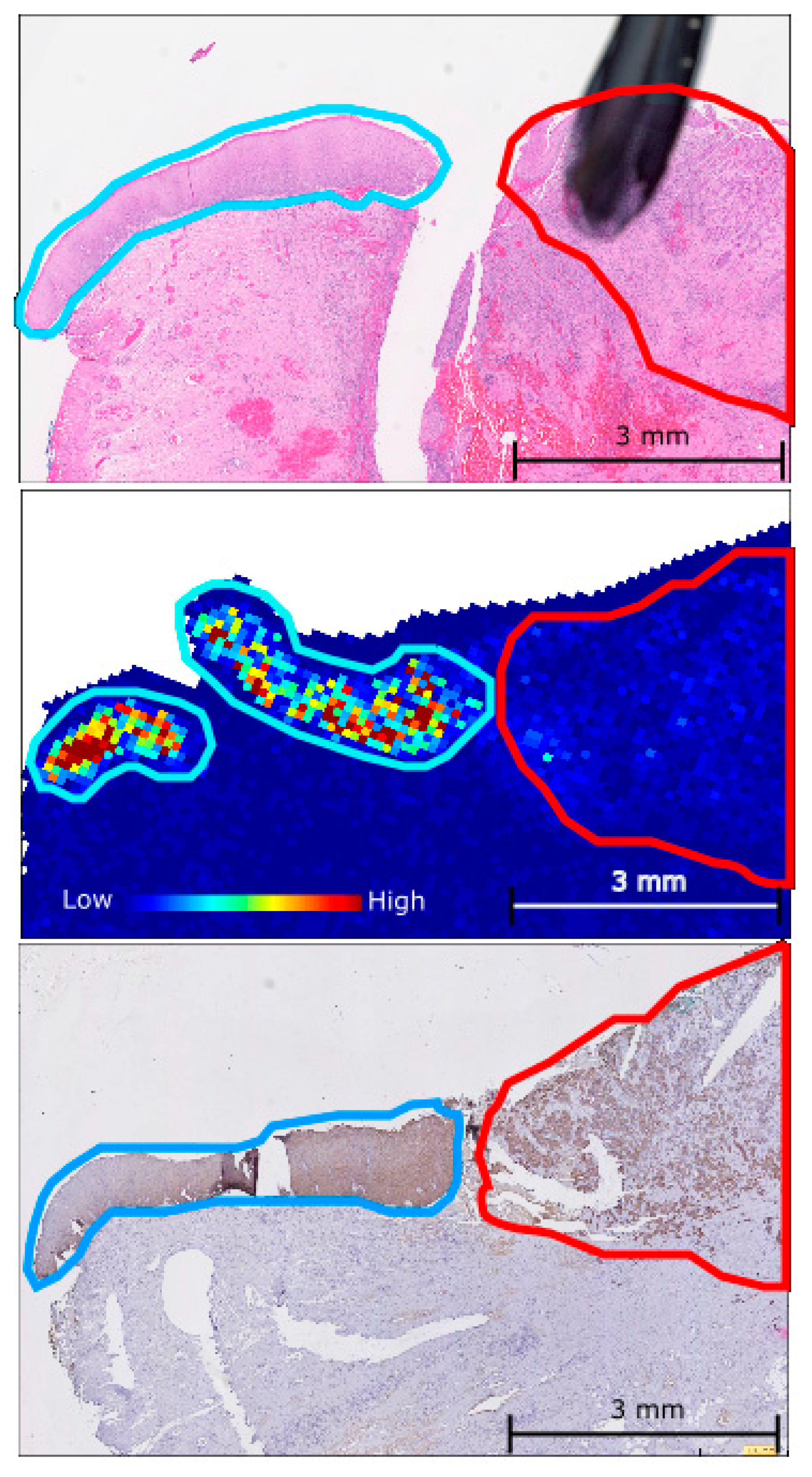
2.1. Matrix-Assisted Laser Desorption/Ionization Mass Spectrometry Imaging (MALDI-MSI)
2.2. Cytokeratin 5 (CK5) Identified as a Protein of Interest
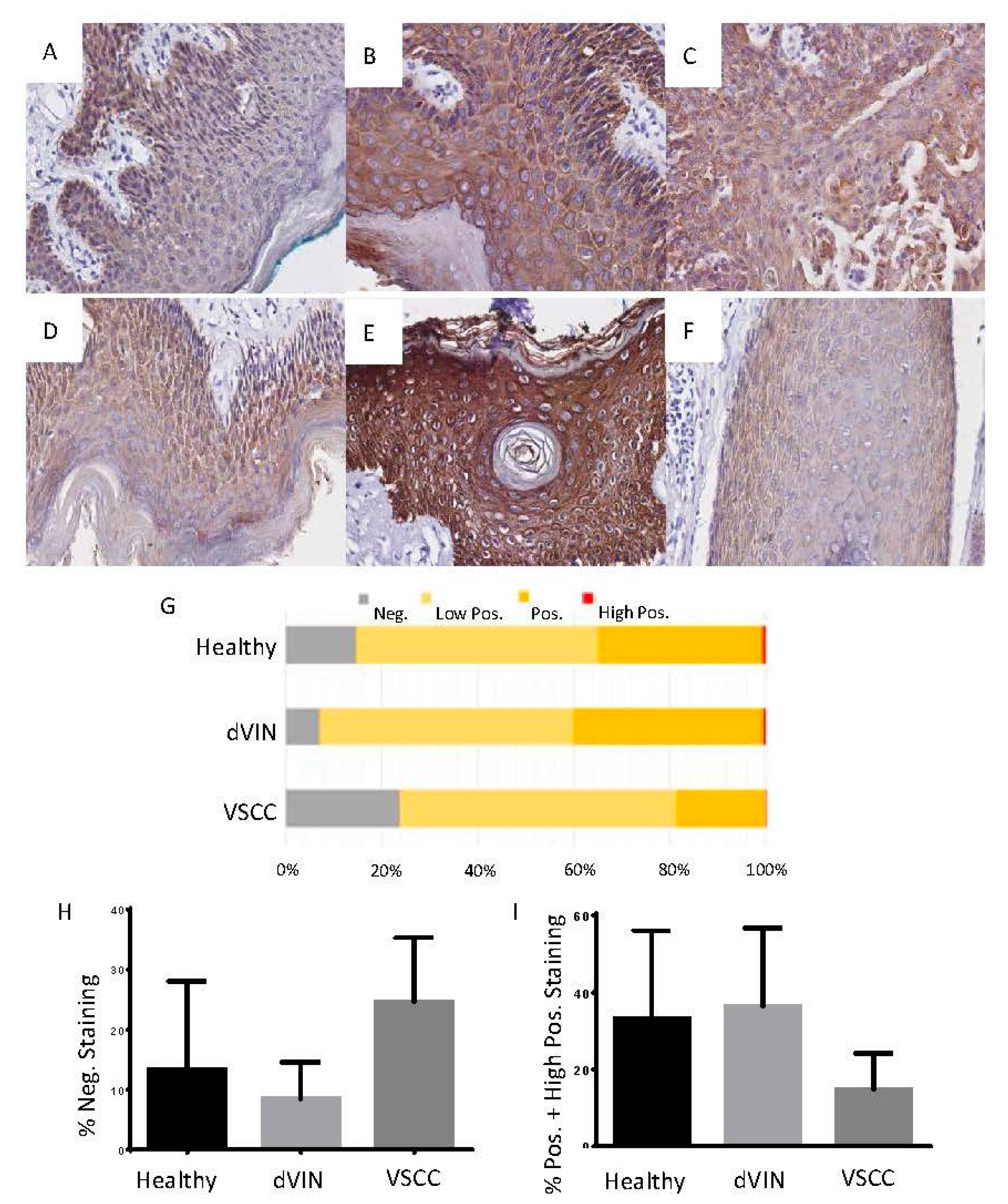
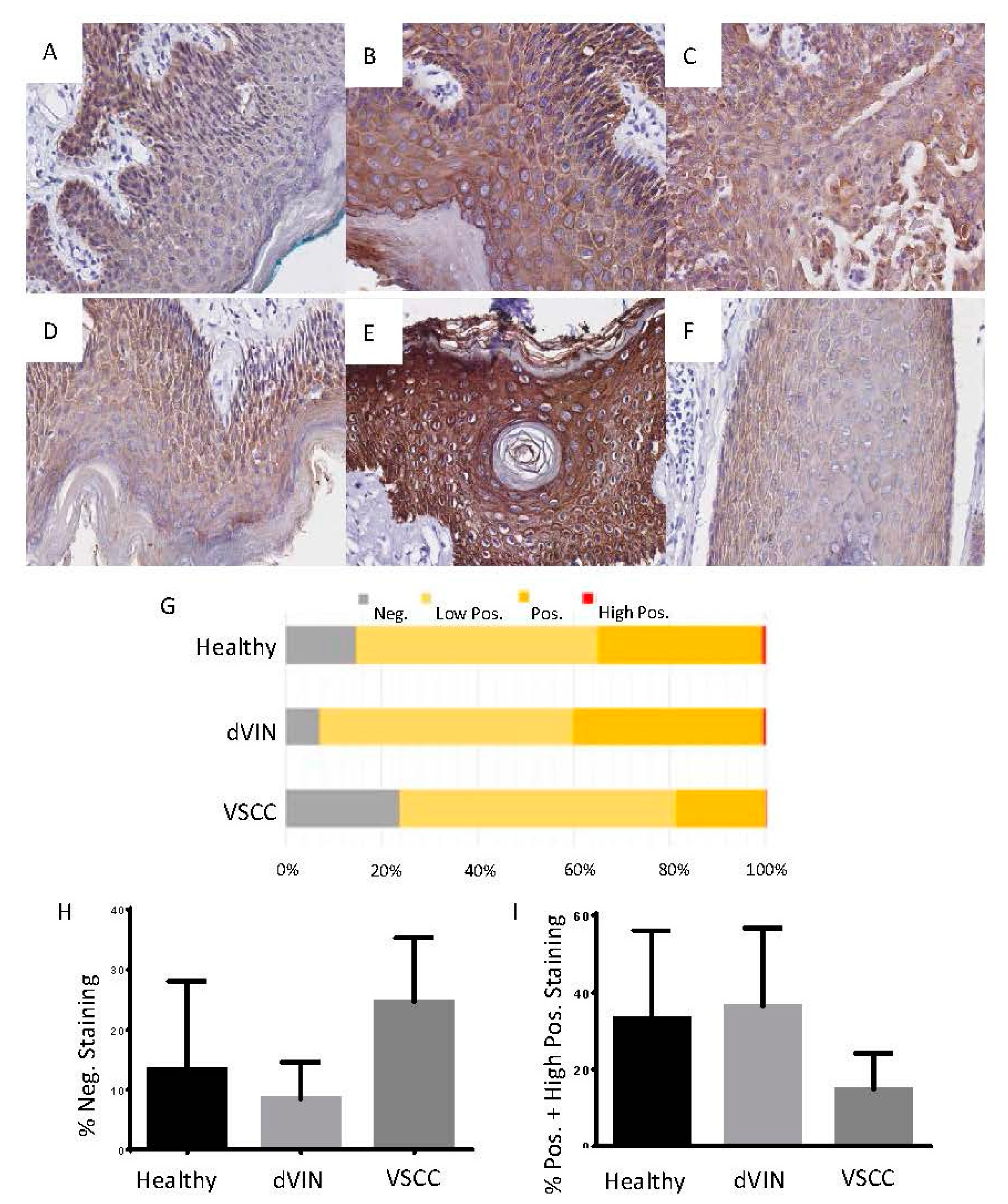
2.3. Immunohistochemistry (IHC) Analysis of CK5 across the Healthy Epithelium, Differentiated Vulvar Intraepithelial Neoplasia and Vulvar Squamous Cell Carcinoma
3. Discussion
4. Materials and Methods
4.1. Sample Cohort
4.2. MALDI-MSI Preparation and Acquisition
4.3. MALDI-MSI Data Analysis
4.4. Peptide Identification by Nanoflow Liquid Chromatography Tandem Mass Spectrometry (nano-LC-MS/MS)
4.5. Matching the MALDI-MSI Peak Groups to the Nanoflow Liquid Chromatography Tandem Mass Spectrometry (Nano-LC-MS/MS) Results
4.6. Immunohistochemistry
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2015. CA Cancer 2015, 65, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Brooks, L.A.; Tidy, J.A.; Gusterson, B.; Hiller, L.; O’Nions, J.; Gasco, M.; Marin, M.C.; Farrell, P.J.; Kaelin, W.G.; Crook, T. Preferential retention of codon 72 arginine p53 in squamous cell carcinomas of the vulva occurs in cancers positive and negative for human papillomavirus. Cancer Res. 2000, 60, 6875–6877. [Google Scholar] [PubMed]
- Condon, J.; Rumbold, A.; Thorn, J.; O’Brien, M.; Davy, M.; Zardawi, I. A cluster of vulvar cancer and vulvar intraepithelial neoplasia in young australian indigenous women. Cancer Causes Control 2009, 20, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Joura, E.A. Epidemiology, diagnosis and treatment of vulvar intraepithelial neoplasia. Curr. Opin. Obstet. Gynecol. 2002, 14, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Liegl, B.; Regauer, S. P53 immunostaining in lichen sclerosus is related to ischaemic stress and is not a marker of differentiated vulvar intraepithelial neoplasia (d-VIN). Histopathology 2006, 48, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Van de Nieuwenhof, H.P.; Massuger, L.F.; van der Avoort, I.A.; Bekkers, R.L.; Casparie, M.; Abma, W.; van Kempen, L.C.; de Hullu, J.A. Vulvar squamous cell carcinoma development after diagnosis of vin increases with age. Eur. J. Cancer 2009, 45, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Van de Nieuwenhof, H.P.; Bulten, J.; Hollema, H.; Dommerholt, R.G.; Massuger, L.F.; van der Zee, A.G.; de Hullu, J.A.; van Kempen, L.C. Differentiated vulvar intraepithelial neoplasia is often found in lesions, previously diagnosed as lichen sclerosus, which have progressed to vulvar squamous cell carcinoma. Mod. Pathol. 2011, 24, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Kokka, F.; Singh, N.; Faruqi, A.; Gibbon, K.; Rosenthal, A.N. Is differentiated vulval intraepithelial neoplasia the precursor lesion of human papillomavirus-negative vulval squamous cell carcinoma? Int. J. Gynecol. Cancer 2011, 21, 1297–1305. [Google Scholar] [CrossRef] [PubMed]
- New Nomenclature for Vulvar Disease. Report of the committee on terminology of the international society for the study of vulvar disease. J. Reprod. Med. 1990, 35, 483–484.
- Ridley, C.M.; Frankman, O.; Jones, I.S.; Pincus, S.H.; Wilkinson, E.J.; Fox, H.; Friedrich, E.G.J.R.; Kaufman, R.H.; Lynch, P.J. New nomenclature for vulvar disease: International society for the study of vulvar disease. Hum. Pathol. 1989, 20, 495–496. [Google Scholar] [CrossRef]
- Pinto, A.P.; Miron, A.; Yassin, Y.; Monte, N.; Woo, T.Y.; Mehra, K.K.; Medeiros, F.; Crum, C.P. Differentiated vulvar intraepithelial neoplasia contains tp53 mutations and is genetically linked to vulvar squamous cell carcinoma. Mod. Pathol. 2010, 23, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Aide, S.; Lattario, F.R.; Almeida, G.; do Val, I.C.; Carvalho Mda, G. Promoter hypermethylation of death-associated protein kinase and p16 genes in vulvar lichen sclerosus. J. Low. Genit. Tract Dis. 2012, 16, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Fox, H.; Wells, M. Recent advances in the pathology of the vulva. Histopathology 2003, 42, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, J.O.R.; Oehler, M.K.; Ruszkiewicz, A.; McColl, S.R.; Hoffmann, P. Maldi imaging mass spectrometry (MALDI-IMS)―Application of spatial proteomics for ovarian cancer classification and diagnosis. Int. J. Mol. Sci. 2011, 12, 773–794. [Google Scholar] [CrossRef] [PubMed]
- Balluff, B.; Rauser, S.; Meding, S.; Elsner, M.; Schöne, C.; Feuchtinger, A.; Schuhmacher, C.; Novotny, A.; Jütting, U.; Maccarrone, G. Maldi imaging identifies prognostic seven-protein signature of novel tissue markers in intestinal-type gastric cancer. Am. J. Pathol. 2011, 179, 2720–2729. [Google Scholar] [CrossRef] [PubMed]
- Marko-Varga, G.; Fehniger, T.E.; Rezeli, M.; Döme, B.; Laurell, T.; Végvári, Á. Drug localization in different lung cancer phenotypes by maldi mass spectrometry imaging. J. Proteom. 2011, 74, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Crecelius, A.C.; Cornett, D.S.; Caprioli, R.M.; Williams, B.; Dawant, B.M.; Bodenheimer, B. Three-dimensional visualization of protein expression in mouse brain structures using imaging mass spectrometry. J. Am. Soc. Mass Spectrom. 2005, 16, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Campello, R.J.; Moulavi, D.; Sander, J. Density-based clustering based on hierarchical density estimates. In Advances in Knowledge Discovery and Data Mining; Springer: Berlin & Heidelberg, Germany, 2013; pp. 160–172. [Google Scholar]
- Reyes, M.C.; Cooper, K. An update on vulvar intraepithelial neoplasia: Terminology and a practical approach to diagnosis. J. Clin. Pathol. 2014, 67, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Trietsch, M.D.; Nooij, L.S.; Gaarenstroom, K.N.; van Poelgeest, M.I. Genetic and epigenetic changes in vulvar squamous cell carcinoma and its precursor lesions: A review of the current literature. Gynecol. Oncol. 2015, 136, 143–157. [Google Scholar] [CrossRef] [PubMed]
- Vasca, V.; Vasca, E.; Freiman, P.; Marian, D.; Luce, A.; Mesolella, M.; Caraglia, M.; Ricciardiello, F.; Duminica, T. Keratin 5 expression in squamocellular carcinoma of the head and neck. Oncol. Lett. 2014, 8, 2501–2504. [Google Scholar] [CrossRef] [PubMed]
- Chu, P.G.; Weiss, L.M. Expression of cytokeratin 5/6 in epithelial neoplasms: An immunohistochemical study of 509 cases. Mod. Pathol. 2002, 15, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Khanna, N.; Rauh, L.A.; Lachiewicz, M.P.; Horowitz, I.R. Margins for cervical and vulvar cancer. J. Surg. Oncol. 2016, 113, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Nofech-Mozes, S.; Khalifa, M.A.; Ismiil, N.; Saad, R.S.; Hanna, W.M.; Covens, A.; Ghorab, Z. Immunophenotyping of serous carcinoma of the female genital tract. Mod. Pathol. 2008, 21, 1147–1155. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, O.J.; Eddes, J.S.; Meding, S.; McColl, S.R.; Oehler, M.K.; Hoffmann, P. Matrix-assisted laser desorption/ionization imaging protocol for in situ characterization of tryptic peptide identity and distribution in formalin-fixed tissue. Rapid Commun. Mass Spectrom. 2013, 27, 655–670. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, J.O.; Oehler, M.K.; McColl, S.R.; Hoffmann, P. Citric acid antigen retrieval (CAAR) for tryptic peptide imaging directly on archived formalin-fixed paraffin-embedded tissue. J. Proteom. Res. 2010, 9, 4315–4328. [Google Scholar] [CrossRef] [PubMed]
- Meding, S.; Martin, K.; Gustafsson, O.J.; Eddes, J.S.; Hack, S.; Oehler, M.K.; Hoffmann, P. Tryptic peptide reference data sets for maldi imaging mass spectrometry on formalin-fixed ovarian cancer tissues. J. Proteom. Res. 2012, 12, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Thiele, H.; Heldmann, S.; Trede, D.; Strehlow, J.; Wirtz, S.; Dreher, W.; Berger, J.; Oetjen, J.; Kobarg, J.H.; Fischer, B. 2D and 3D MALDI-imaging: Conceptual strategies for visualization and data mining. Biochim. Biophys. Acta 2014, 1844, 117–137. [Google Scholar] [CrossRef] [PubMed]
- Lokman, N.A.; Elder, A.S.; Ween, M.P.; Pyragius, C.E.; Hoffmann, P.; Oehler, M.K.; Ricciardelli, C. Annexin a2 is regulated by ovarian cancer-peritoneal cell interactions and promotes metastasis. Oncotarget 2013, 4, 1199–1211. [Google Scholar] [CrossRef] [PubMed]
- Varghese, F.; Bukhari, A.B.; Malhotra, R.; De, A. Ihc profiler: An open source plugin for the quantitative evaluation and automated scoring of immunohistochemistry images of human tissue samples. PLoS ONE 2014, 9, e96801. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Peptide AWM [M + H] of the Peak Group 1 | Da Range of the Peak Group | No. Spectra in Peak Group 2 | Maximum Difference Median Log Intensity 3 |
|---|---|---|---|
| 1198.71 | ±0.62 | 23,099 | 0.75 |
| 1028.62 | ±0.56 | 15,354 | 0.66 |
| 1410.72 * | ±0.82 | 18,784 | 0.58 |
| 1905.95 | ±0.52 | 10,956 | 0.56 |
| 1095.58 | ±0.82 | 21,704 | 0.55 |
| 944.54 | ±0.69 | 19,354 | 0.53 |
| 957.63 | ±0.65 | 10,464 | 0.52 |
| 857.60 | ±0.68 | 14,956 | 0.50 |
| 976.51 | ±0.65 | 15,534 | 0.49 |
| 878.56 | ±0.68 | 11,213 | 0.46 |
| 810.48 * | ±0.76 | 17,095 | 0.45 |
| 958.59 | ±0.69 | 15,432 | 0.42 |
| 943.62 | ±0.82 | 20,030 | 0.41 |
| 865.42 * | ±0.84 | 15,617 | 0.41 |
| 1217.66 | ±0.55 | 10,906 | 0.39 |
| 884.52 * | ±0.66 | 14,337 | 0.37 |
| 856.67 | ±0.74 | 15,483 | 0.36 |
| 1143.65 * | ±0.64 | 17,685 | 0.36 |
| 1045.62 | ±0.65 | 16,370 | 0.35 |
| 2147.19 | ±0.14 | 20,418 | 0.33 |
| 1105.59 | ±0.50 | 11,479 | 0.30 |
| 1296.68 | ±0.10 | 22,823 | 0.29 |
| 870.64 | ±0.85 | 22,749 | 0.29 |
| 842.60 | ±0.90 | 25,210 | 0.22 |
| 1267.65 | ±0.32 | 11,686 | 0.20 |
| 2932.59 | ±0.07 | 15,500 | 0.19 |
| 816.50 | ±0.73 | 10,983 | 0.19 |
| 971.56 * | ±0.65 | 15,998 | 0.18 |
| 1111.58 | ±0.51 | 13,473 | 0.09 |
| 1570.70 | ±0.17 | 12,029 | 0.05 |
| 864.63 | ±0.70 | 11,114 | 0.05 |
| Peptide AWM [M + H] 1 | d 2 | LC-MS/MS m/z 3 | LC-MS/MS MR 4 | Peptide Score 5 | Peptide Significance 6 | Peptide Sequence 7 |
|---|---|---|---|---|---|---|
| 810.48 | 0.45 | 405.7087 | 809.4028 | 21.44 | 0.0072 | QSSVSFR |
| 865.42 | 0.41 | 433.1998 | 864.3851 | 26 | 0.0025 | SGGGGGGGFGR |
| 884.52 | 0.37 | 442.7286 | 883.4427 | 24.74 | 0.0034 | TSFTSVSR |
| 971.56 | 0.18 | 486.2429 | 970.4712 | 25.1 | 0.0031 | FVSTTSSSR |
| 1143.65 | 0.36 | 572.3175 | 1142.6205 | 39.59 | 0.00011 | LAELEEALQK |
| 1410.72 | 0.58 | 705.8674 | 1409.7203 | 115.28 | 3 × 10−12 | SFSTASAITPSVSR |
| 1410.72 | 0.58 | 705.872 | 1409.7295 | 150.55 | 8.8 × 10−16 | TTAENEFVMLKK |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, C.; Arentz, G.; Winderbaum, L.; Lokman, N.A.; Klingler-Hoffmann, M.; Mittal, P.; Carter, C.; Oehler, M.K.; Hoffmann, P. MALDI Mass Spectrometry Imaging Reveals Decreased CK5 Levels in Vulvar Squamous Cell Carcinomas Compared to the Precursor Lesion Differentiated Vulvar Intraepithelial Neoplasia. Int. J. Mol. Sci. 2016, 17, 1088. https://doi.org/10.3390/ijms17071088
Zhang C, Arentz G, Winderbaum L, Lokman NA, Klingler-Hoffmann M, Mittal P, Carter C, Oehler MK, Hoffmann P. MALDI Mass Spectrometry Imaging Reveals Decreased CK5 Levels in Vulvar Squamous Cell Carcinomas Compared to the Precursor Lesion Differentiated Vulvar Intraepithelial Neoplasia. International Journal of Molecular Sciences. 2016; 17(7):1088. https://doi.org/10.3390/ijms17071088
Chicago/Turabian StyleZhang, Chao, Georgia Arentz, Lyron Winderbaum, Noor A. Lokman, Manuela Klingler-Hoffmann, Parul Mittal, Christopher Carter, Martin K. Oehler, and Peter Hoffmann. 2016. "MALDI Mass Spectrometry Imaging Reveals Decreased CK5 Levels in Vulvar Squamous Cell Carcinomas Compared to the Precursor Lesion Differentiated Vulvar Intraepithelial Neoplasia" International Journal of Molecular Sciences 17, no. 7: 1088. https://doi.org/10.3390/ijms17071088
APA StyleZhang, C., Arentz, G., Winderbaum, L., Lokman, N. A., Klingler-Hoffmann, M., Mittal, P., Carter, C., Oehler, M. K., & Hoffmann, P. (2016). MALDI Mass Spectrometry Imaging Reveals Decreased CK5 Levels in Vulvar Squamous Cell Carcinomas Compared to the Precursor Lesion Differentiated Vulvar Intraepithelial Neoplasia. International Journal of Molecular Sciences, 17(7), 1088. https://doi.org/10.3390/ijms17071088