
Oral Supplementation with a Special Additive of Retinyl Palmitate and Alpha Tocopherol Reduces Growth Retardation in Young Pancreatic Duct Ligated Pigs Used as a Model for Children Suffering from Exocrine Pancreatic Insufficiency

 , ,
, ,
Abstract
:1. Introduction
2. Results
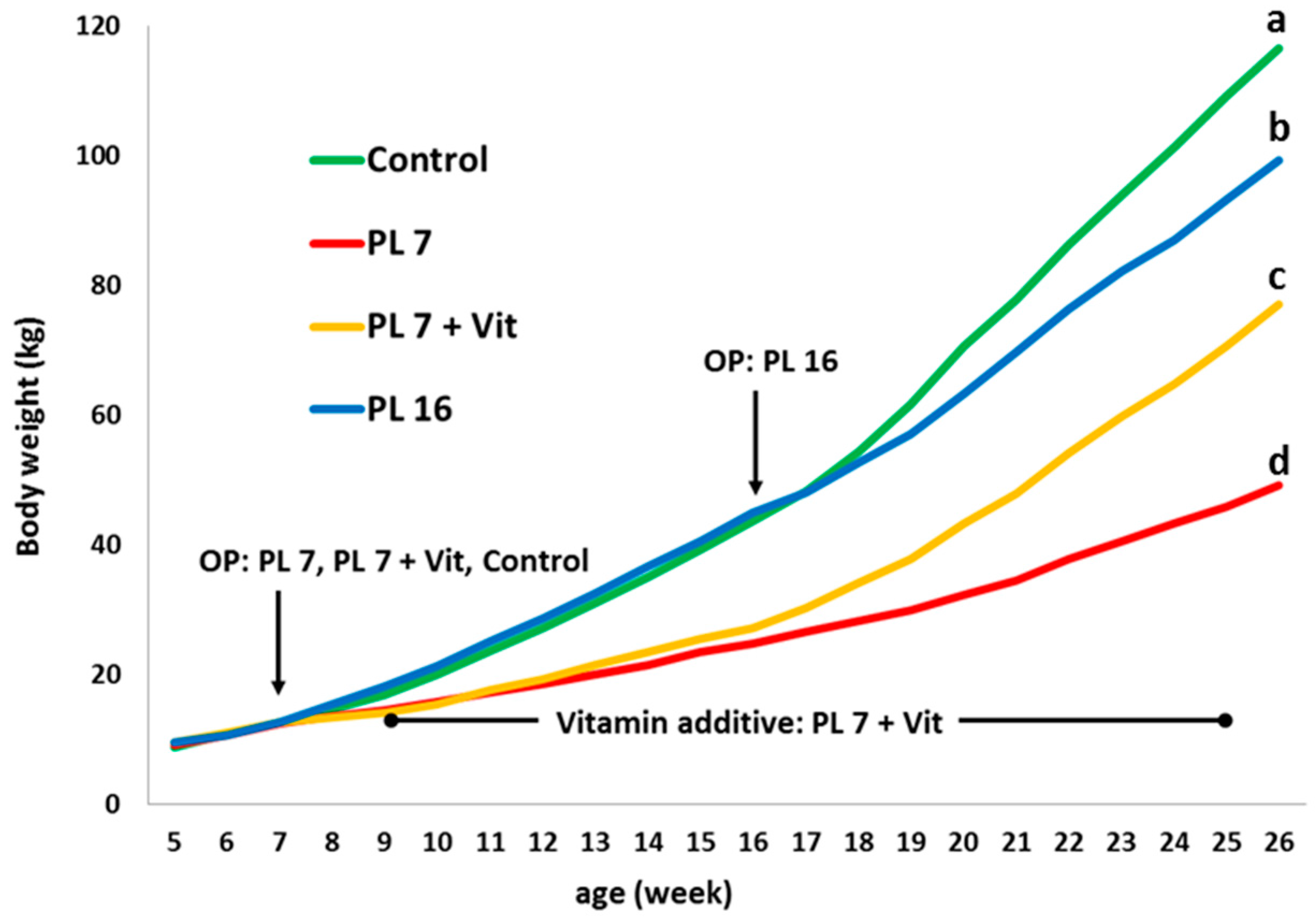
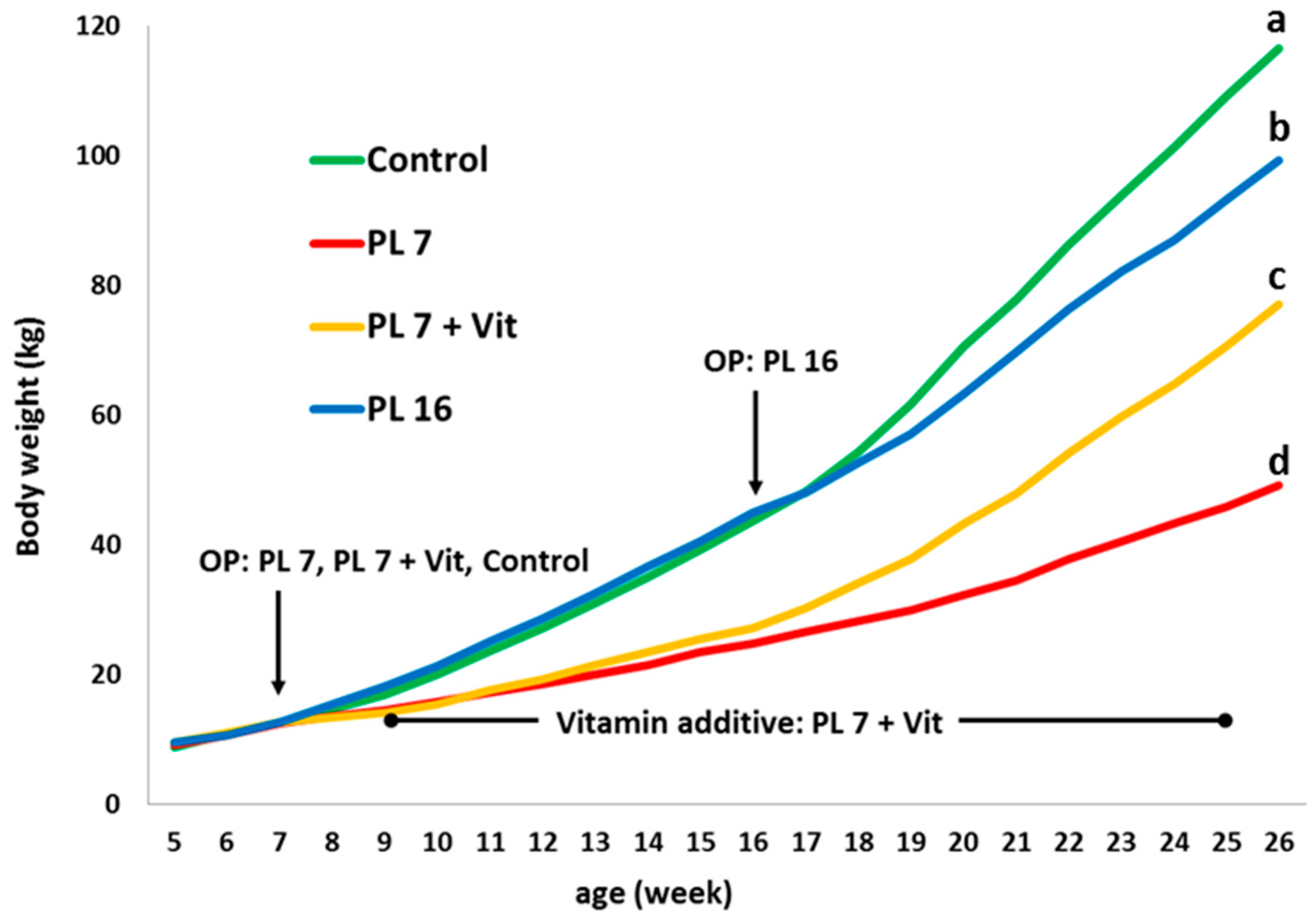
2.1. Body Weight and Body Measurements, Feed Intake, and Body Weight Gain:Feed Ratio
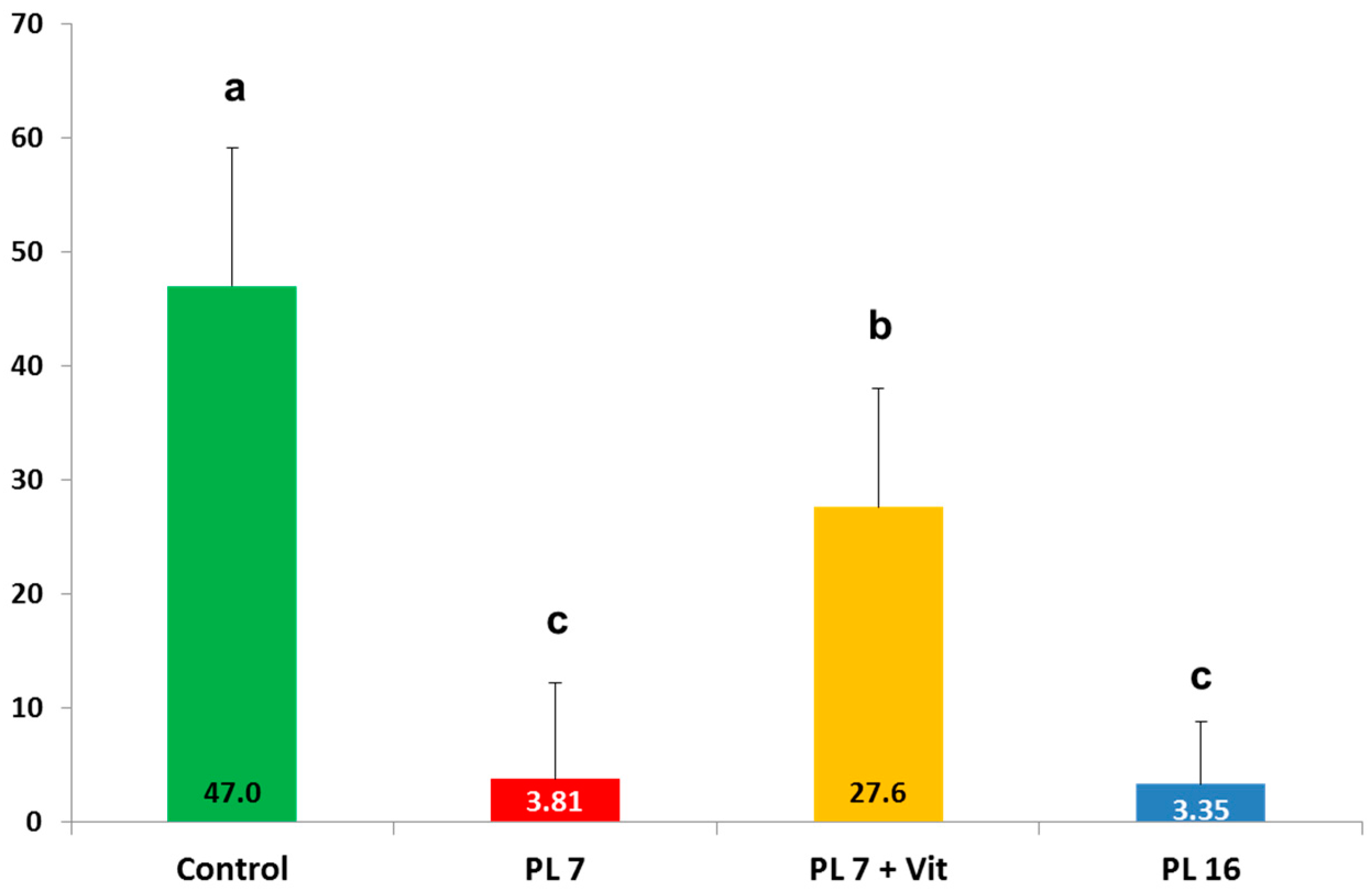
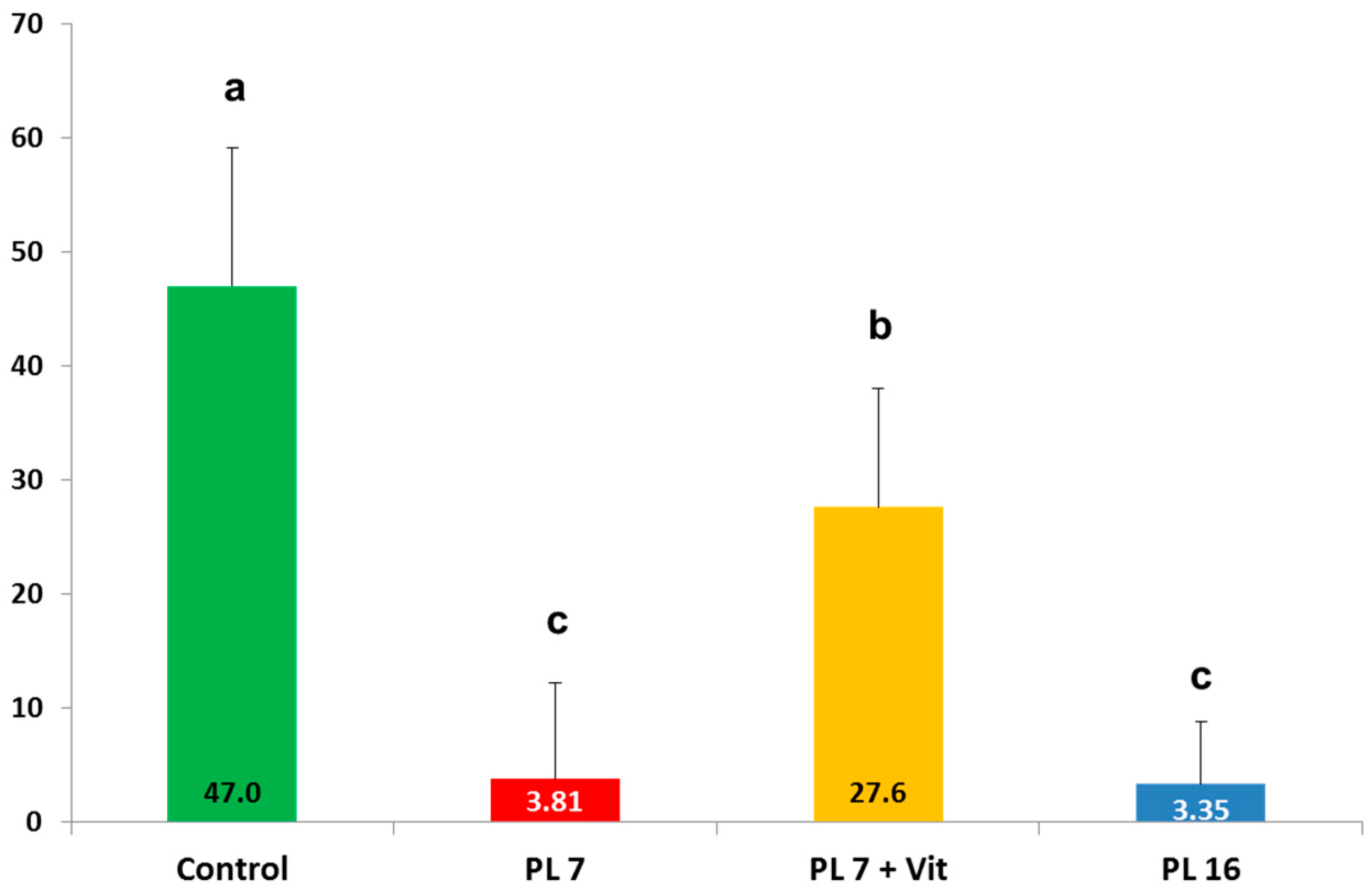
2.2. Faecal Fat Digestibility
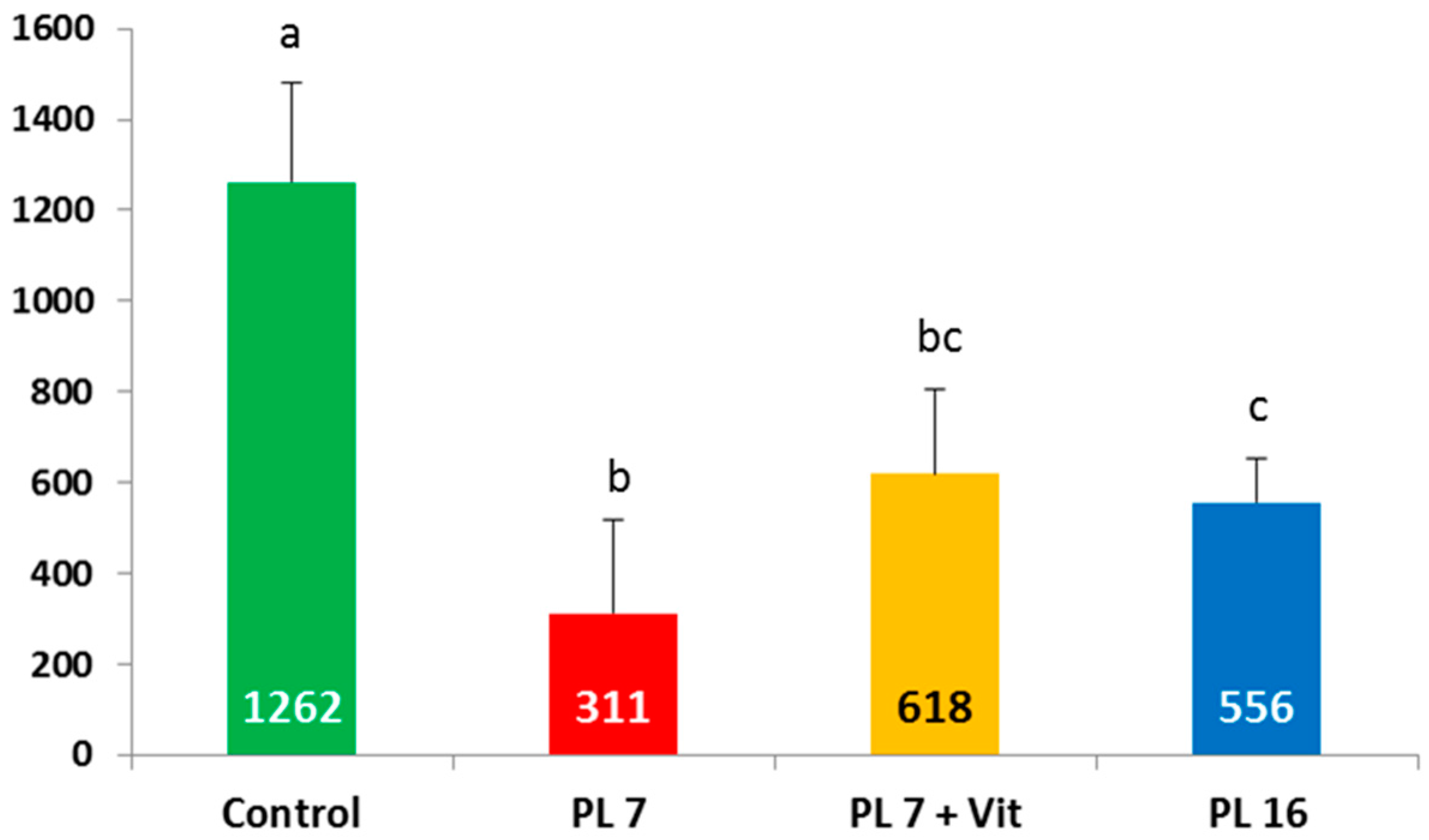
2.3. Leptin Concentration in Serum
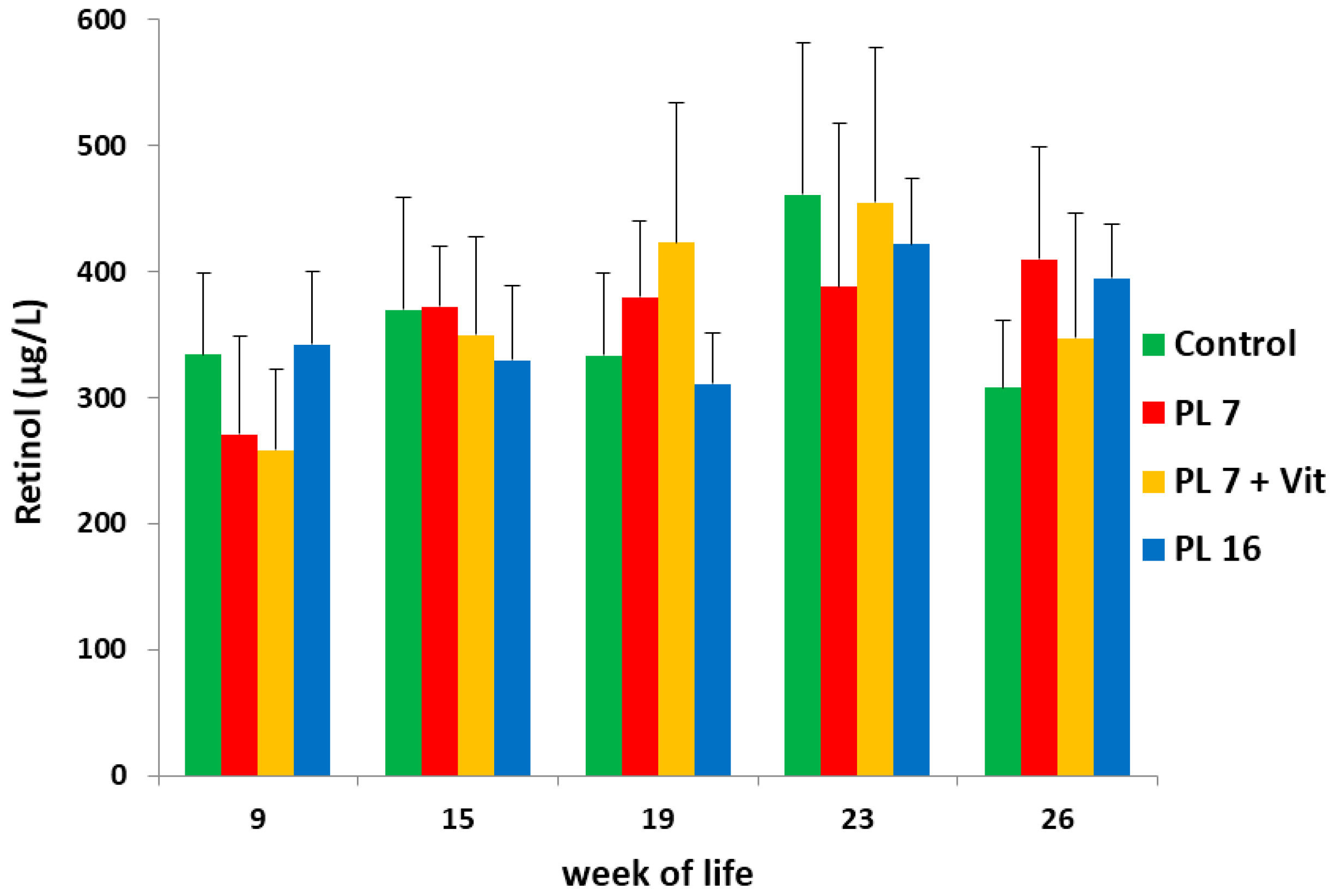
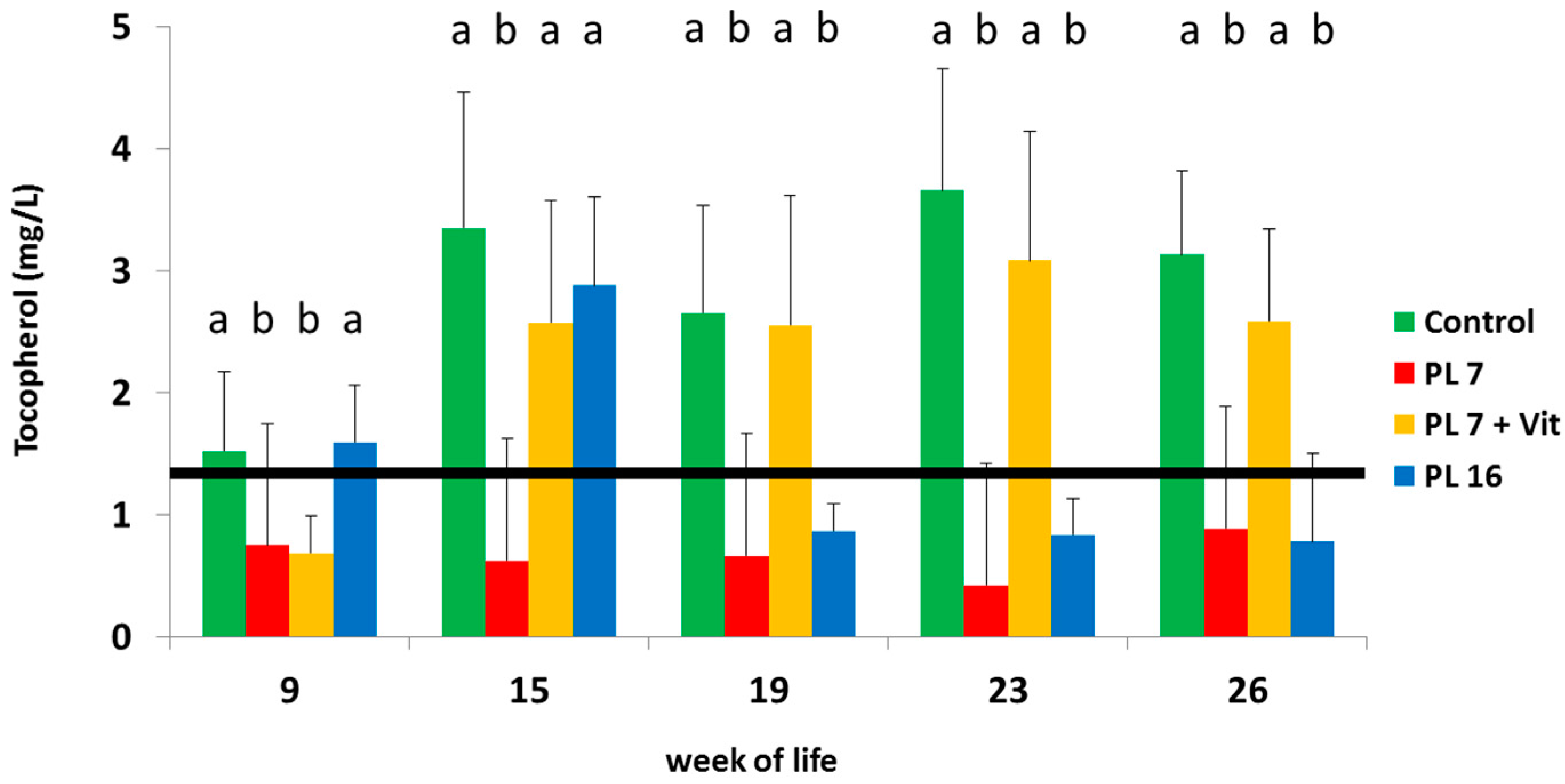
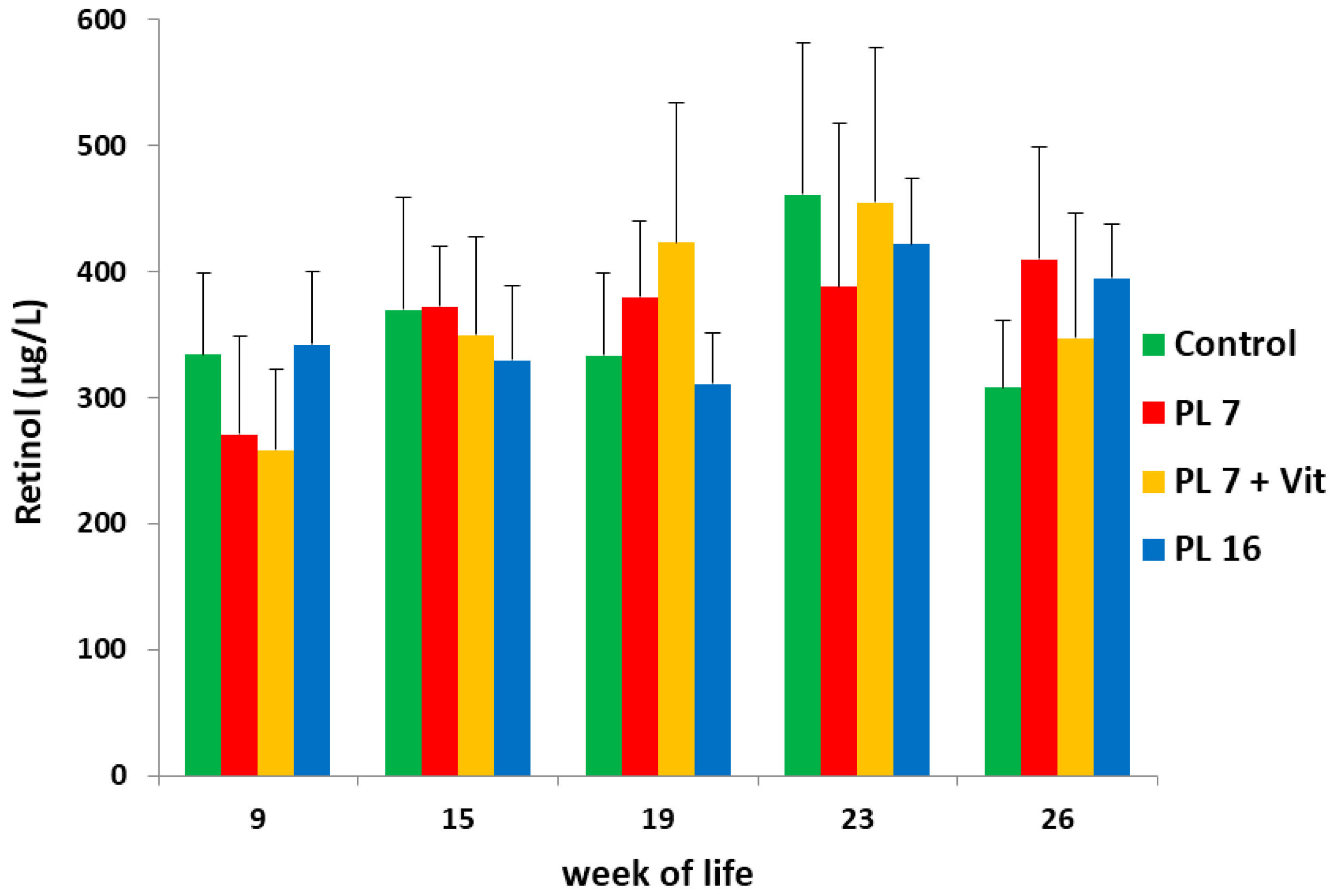
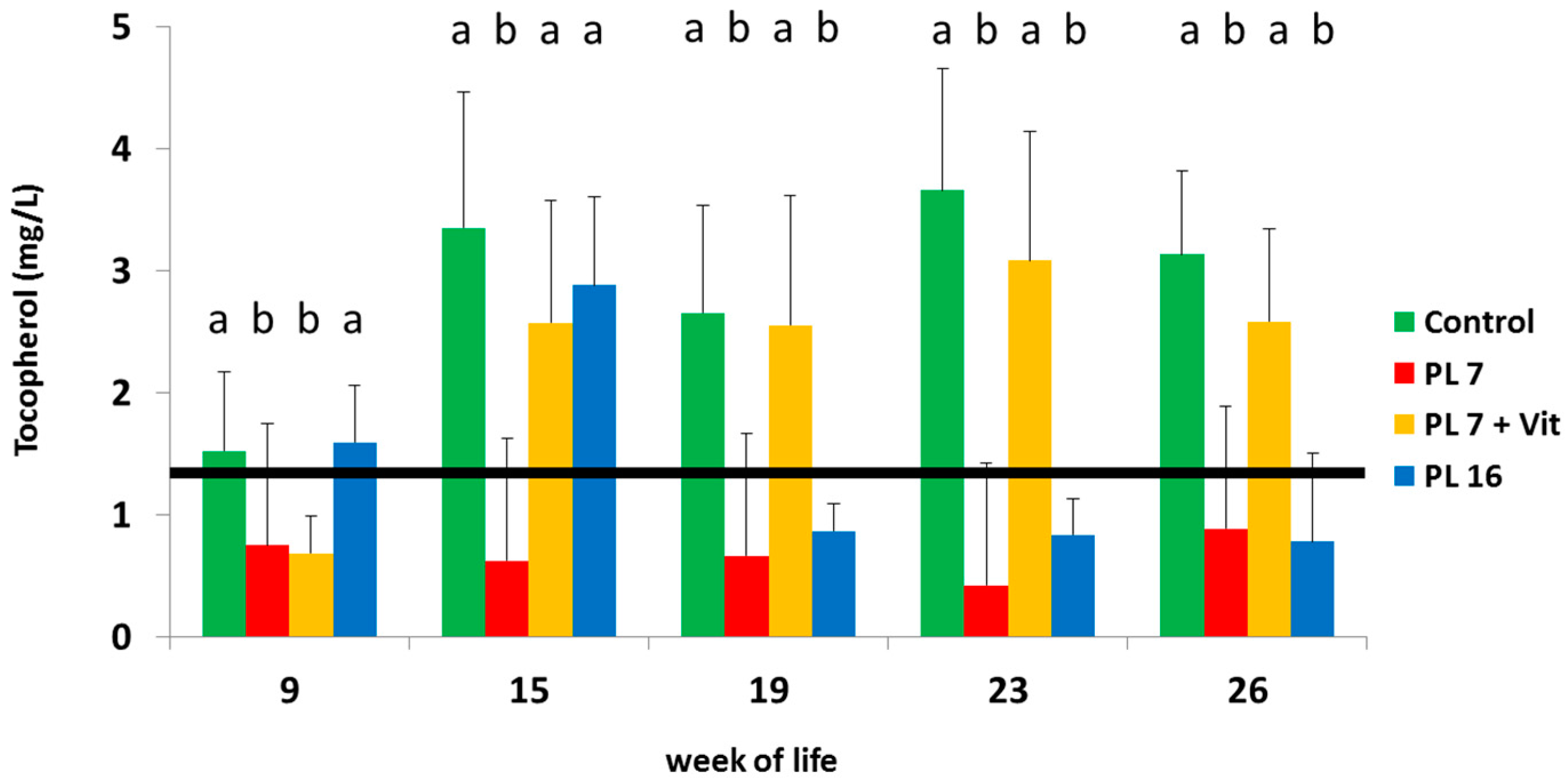
2.4. Serum Levels of Vitamin A (Retinol) and Vitamin E (Tocopherol)
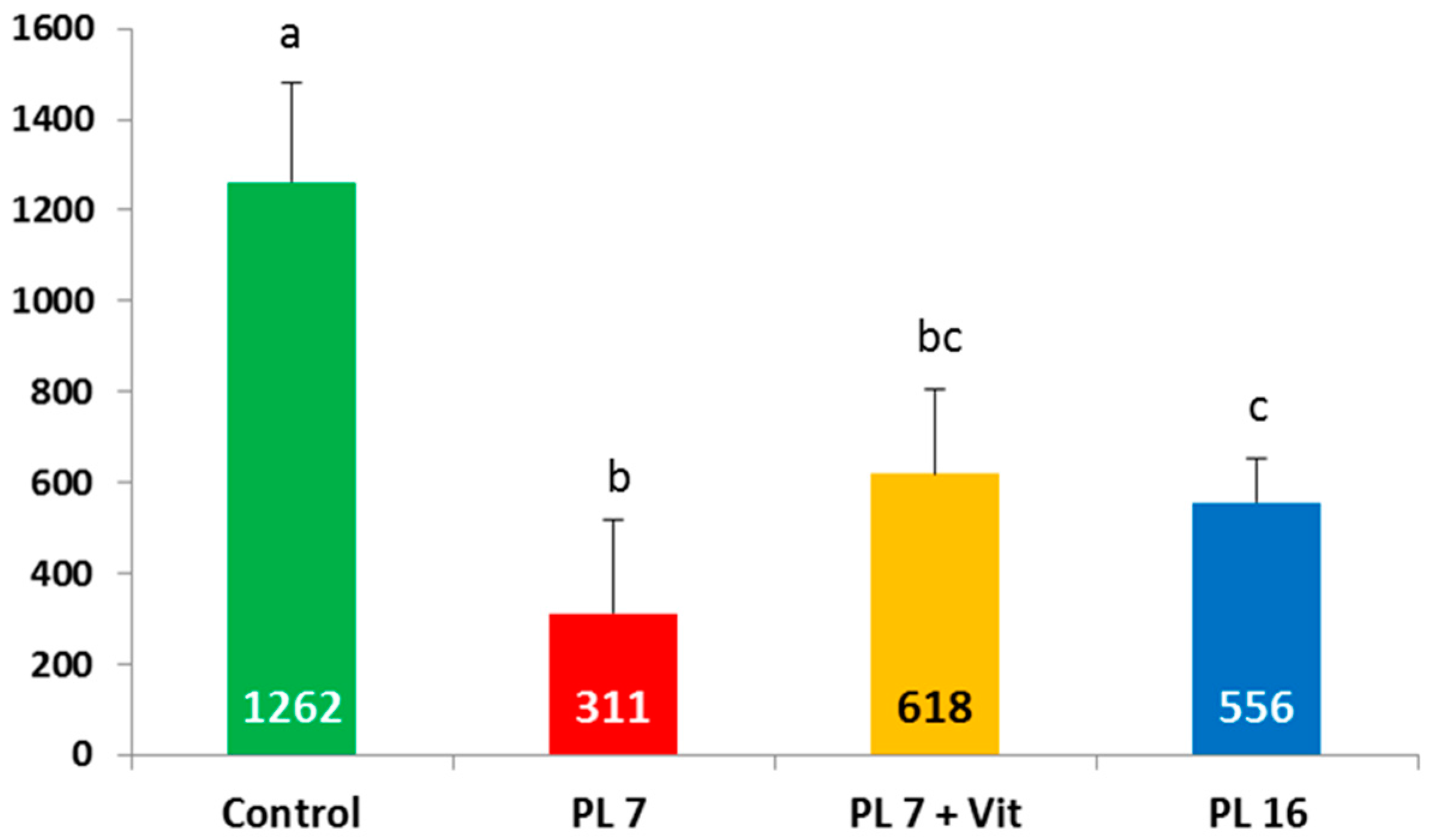
2.5. Concentrations of Vitamin A (Retinol) and Vitamin E (Tocopherol) in Liver Tissue at the End of the Trial
3. Discussion
4. Material and Methods
4.1. Animals
4.2. Housing
4.3. Diet and Feeding
4.4. Vitamin Supplementation
4.5. Parameters and Blood Sampling during the Study Course
4.6. Euthanasia and Dissection
4.7. Analysis
4.8. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BW | Body weight |
| C | Control group |
| CF | Cystic Fibrosis |
| DM | Dry matter |
| G:F | Gain:Feed ratio |
| p | p-Value |
| PEI | Pancreatic exocrine insufficiency |
| PL | Pancreatic duct ligated |
| PL-7 | Pigs that underwent pancreatic duct ligation in week 7 of life |
| PL-7 + Vit | Pigs that underwent pancreatic duct ligation in week 7 of life and received oral vitamin supplement from week 9 of life onwards |
| PL-16 | Pigs that underwent pancreatic duct ligation in week 16 of life |
References
- Layer, P.; Keller, J. Pancreatic enzymes: Secretion and luminal nutrient digestion in health and disease. J. Clin. Gastroenterol. 1999, 28, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Farrell, P.M.; Bieri, J.G.; Fratononi, J.F.; Wood, R.E.; di SantÀgnese, P.A. The occurrence and effects of human vitamin E deficiency—A study in patients with cystic fibrosis. J. Clin. Investig. 1977, 60, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Huet, F.; Semama, D.; Maingueneau, C.; Charavel, A.; Nivelon, J.L. Vitamin A deficiency and nocturnal vision in teenagers with cystic fibrosis. Eur. J. Pediatr. 1997, 156, 949–951. [Google Scholar] [CrossRef] [PubMed]
- Sagel, S.D.; Sontag, M.K.; Anthony, M.M.; Emmett, P.; Papas, K.A. Effect of an antioxidant-rich multivitamin supplement in cystic fibrosis. J. Cyst. Fibros. 2011, 10, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Papas, K.A.; Sontag, M.K.; Pardee, C.; Sokol, R.J.; Sagel, S.D.; Accurso, F.J.; Wagener, J.S. A pilot study on the safety and efficacy of a novel antioxidant rich formulation in patients with cystic fibrosis. J. Cyst. Fibros. 2008, 7, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Cantin, A.M.; White, T.B.; Cross, C.E.; Forman, H.J.; Sokol, R.J.; Borowitz, D. Antioxidants in cystic fibrosis. Conclusions from the CF antioxidant workshop, Bethesda, Maryland, November 11–12, 2003. Free Radic. Biol. Med. 2007, 42, 15–31. [Google Scholar] [CrossRef] [PubMed]
- Sadowska-Woda, I.; Rachel, M.; Pazdan, J.; Bieszczad-Bedrejczuk, E.; Pawliszak, K. Nutritional supplement attenuates selected oxidative stress markers in pediatric patients with cystic fibrosis. Nutr. Res. 2011, 31, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Park, R.W.; Grant, R.J. Gastrointestinal manifestation of cystic fibrosis: A review. Gastroenterology 1981, 81, 1143–1161. [Google Scholar]
- Sinaasappel, M.; Stern, M.; Littlewood, J.; Wolfe, S.; Steinkamp, G.; Heijermann, H.G.M.; Robberecht, E.; Döring, G. Consensus report, nutrition in patients with cystic fibrosis: A European consensus. J. Cyst. Fibros. 2002, 1, 51–75. [Google Scholar] [CrossRef]
- Beckett, K.; Shaw, K.; Sathe, M. Pediatric cystic fibrosis and fat-soluble vitamins. In Diet and Exercise in Cystic Fibrosis; Watson, R.R., Ed.; Elsevier Limited: Oxford, UK, 2015; Chapter 16; pp. 125–130. [Google Scholar]
- Dutta, S.; Bustin, M.P.; Russel, R.M.; Costa, B.S. Deficiency in fat-soluble vitamins in treated patients with pancreatic insufficiency. Ann. Intern. Med. 1982, 97, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Sitrin, M.D.; Liebermann, F.; Jensen, W.E.; Noronha, A.; Milburn, C.; Addington, W. Vitamin E deficiency and neurologic disease in adults with cystic fibrosis. Ann. Intern. Med. 1987, 107, 51–54. [Google Scholar] [CrossRef] [PubMed]
- Feranchak, A.P.; Sontag, M.K.; Wagener, J.S.; Hammond, K.B.; Accurso, F.J.; Sokol, R.J. Prospective, long-term study of fat-soluble vitamin status in children with cystic fibrosis identified by newborn screen. J. Pediatr. 1999, 135, 601–610. [Google Scholar] [CrossRef]
- Back, E.I.; Frindt, C.; Nohr, D.; Frank, J.; Ziebach, R.; Stern, M.; Ranke, M.; Biesalski, H.K. Antioxidant deficiency in cystic fibrosis: When is the right time to take action. Am. J. Clin. Nutr. 2004, 80, 374–384. [Google Scholar] [PubMed]
- Rayner, R.J. Fat-soluble vitamins in cystic fibrosis. Proc. Nutr. Soc. 1992, 51, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Dodge, J.A.; Turck, D. Cystic fibrosis: Nutritional consequences and management. Best Pract. Res. Clin. Gastroenterol. 2006, 20, 531–541. [Google Scholar] [CrossRef] [PubMed]
- Borowitz, D.; Robinson, K.A.; Rosenfeld, M.; Davis, S.D.; Sabadosa, K.A.; Spear, S.L.; Michel, S.H.; Parad, R.B.; White, T.B.; Farrell, P.M.; et al. Cystic fibrosis foundation evidence-based guidelines for management of infants with cystic fibrosis. J. Pediatr. 2009, 155, S73–S93. [Google Scholar] [CrossRef] [PubMed]
- Stern, M.; Ellemunter, H.; Palm, B.; Posselt, H.-G.; Smaczny, C. Mukoviszidose (Cystische Fibrose): Ernährung und Exokrine Pankreasinsuffizienz. S1-Leitlinie der Gesellschaft für Pädiatrische Gastroenterologie und Ernährung (GPGE). Available online: http://www.awmf.org/uploads/tx_szleitlinien/068-020l_S1_Mukoviszidose_Ernährung_exokrine_Pankreasinsuffizienz_2011-05.pdf (accessed on 1 September 2013).
- Offenberger, H.M.; Watson, R.R. Vitamin A Supplementation Therapy for Patients with Cystic Fibrosis. In Diet and Exercise in Cystic Fibrosis; Watson, R.R., Ed.; Elsevier Limited: Oxford, UK, 2015; Chapter 19; pp. 155–158. [Google Scholar]
- Turck, D.; Braegger, C.P.; Colombo, C.; Declercq, D.; Morton, A.; Pancheva, R.; Robberecht, E.; Stern, M.; Strandvik, B.; Wolfe, S.; et al. ESPEN-ESPGHAN-ECFS guidelines on nutrition care for infants, children and adults with cystic fibrosis. Clin. Nutr. 2016. [Google Scholar] [CrossRef] [PubMed]
- Imondi, A.R.; Stradley, R.P.; Wolgemuth, R. Enzyme replacement therapy in the pancreatic duct ligated swine. Proc. Soc. Exp. Biol. Med. 1972, 141, 367–372. [Google Scholar] [CrossRef] [PubMed]
- Abello, J.; Pascaud, X.; Simoes-Nunes, C.; Cuber, J.C.; Junien, J.L.; Rozé, C. Total pancreatic insufficiency in pigs: A model to study intestinal enzymes and plasma levels of digestive hormones after pancreatic supplementation by a whole pancreas preparation. Pancreas 1989, 4, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Gregory, P.C.; Tabeling, R.; Kamphues, J. Growth and digestion in pancreatic duct ligated pigs. Effect of enzyme supplementation. In Biology of the Pancreas in Growing Animals; Pierzynowski, S.G., Zabielski, R., Eds.; Elsevier Science B.V.: North Holland, The Netherlands, 1999; pp. 381–393. [Google Scholar]
- Corring, T.; Bourdon, D. Exclusion of the pancreatic exocrine secretion from intestine in the pig: Existence of a digestive compensation. J. Nutr. 1977, 107, 1216–1221. [Google Scholar] [PubMed]
- Tabeling, R.; Gregory, P.; Kamphues, J. Studies on nutrient digestibilities (praecaecal and total) in pancreatic duct ligated pigs and the effects of enzyme substitution. J. Anim. Physiol. Anim. Nutr. 1999, 82, 251–263. [Google Scholar] [CrossRef]
- Kammlott, E.; Karthoff, J.; Stemme, K.; Gregory, P.; Kamphues, J. Experiments to optimize enzyme substitution therapy in pancreatic duct-ligated pigs. J. Anim. Physiol. Anim. Nutr. 2005, 89, 105–108. [Google Scholar] [CrossRef] [PubMed]
- Mößeler, A.; Tabeling, R.; Gregory, P.C.; Kamphues, J. Compensatory digestion of fat, protein and starch (rates and amounts) in the large intestine of minipigs in case of reduced precaecal digestion due to pancreatic duct ligation—A short review. Livest. Sci. 2007, 109, 50–52. [Google Scholar]
- Fedkiv, O.; Regman, S.; Weström, B.R.; Pierzynowski, S.G. Growth is dependent on the exocrine pancreatic function in young weaners but not in growing-finishing pigs. J. Physiol. Pharmacol. 2009, 60, 55–59. [Google Scholar] [PubMed]
- Prykhodko, O.; Fedkiv, O.; Weström, B.R.; Pierzynowski, S.G. Effects on gut properties in exocrine pancreatic insufficient (EPI) pigs, being growth retarded due to pancreatic duct ligation at 7 weeks but not at 16 weeks of age. Adv. Med. Sci. 2014, 59, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Gonchoarova, K.; Pierzynowski, S.G.; Grujic, D.; Kirko, S.; Szwiec, K.; Wang, J.; Kovalenko, T.; Osadchenko, I.; Ushakova, G.; Shmigel, H.; et al. A piglet with surgically induced exocrine pancreatic insufficiency as an animal model of newborns to study fat digestion. Br. J. Nutr. 2014, 112, 2060–2067. [Google Scholar] [CrossRef] [PubMed]
- Mößeler, A.; Schwarzmaier, T.; Gregory, P.C.; Piechotta, M.; Beyerbach, M.; Kamphues, J. Pancreatic exocrine insufficiency affects not only digestibility of nutrients and growth, but also body composition and endocrinological parameters—Study on piglets used as a model for children. Pancreat. Disord. Ther. 2015. [Google Scholar] [CrossRef]
- Pitkaranta, P.; Kivisaari, L.; Nordling, S.; Saari, A.; Schroder, T. Experimental chronic pancreatitis in the pig. Scand. J. Gastroenterol. 1989, 24, 987–992. [Google Scholar] [CrossRef] [PubMed]
- Rengman, S.; Fedkiv, O.; Boltermans, J.; Svendsen, J.; Weström, B.; Pierzynowski, S. An elemental diet fed, enteral or parenteral, does not support growth in young pigs with exocrine pancreatic insufficiency. Clin. Nutr. 2009, 28, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Saloniemi, H.; Kalima, T.V.; Rahko, T. Pancreatic enzyme supplementation in normal and exocrine pancreatic insufficient pigs. Acta Vet. Scand. 1989, 30, 367–370. [Google Scholar] [PubMed]
- Schwarzmaier, T.E. Studies on the Effects of Substitution of Pancreatic Enzymes as well as Special Supplementation of Vitamin A and E in Growing Pancreatic Duct Ligated Pigs as a Model for Pancreatic Insufficiency in Children. Ph.D. Thesis, University of Veterinary Medicine, Hannover, Germany, 2012. [Google Scholar]
- Mößeler, A.; Schwarzmaier, T.; Grunemann, J.; Gregory, P.C.; Höltershinken, M.; Kamphues, J. The growing pancreatic duct ligated pig as a model for exocrine pancreatic insufficiency in children: Investigations to achieve sufficient vitamin A and vitamin E supply. J. Anim. Sci. 2012, 90, 321–323. [Google Scholar] [CrossRef] [PubMed]
- Mößeler, A.; Schwarzmaier, T.; Höltershinken, M.; Kamphues, J. The pancreatic duct ligated pig as a model for patients suffering from exocrine pancreatic insufficiency—Studies of vitamin A and E status. In Diet and Exercise in Cystic Fibrosis; Watson, R.R., Ed.; Elsevier Limited: Oxford, UK, 2015; Chapter 38; pp. 343–352. [Google Scholar]
- Puls, R. Vitamin Levels in Animal Health; Sherpa Int.: Clearbrook, BC, Canada, 1994. [Google Scholar]
- Mc Donald, P.; Edwards, R.A.; Greenhalgh, J.F.D.; Morgan, C.A. Animal Nutrition, 6th ed.; Pearson Education Limited: Harlow, UK, 2001. [Google Scholar]
- Gat-Yablonski, G.; Ben-Ari, T.; Shtaif, B.; Potievsky, O.; Moran, O.; Eshet, R.; Maor, G.; Segev, Y.; Phillip, M. Leptin reverses the inhibitory effect of caloric restriction on longitudinal growth. Endocrinology 2004, 45, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, J.E.; Dicks, M.W.; Teichmann, R.; Helmboldt, C.F.; Bacon, E.L.; Prouty, R.M.; Dolge, K.L.; Eaton, H.D.; Jungherr, E.L.; Beall, G. Relationships between plasma, liver and dietary α-tocopherol in calves, lambs and pigs. J. Anim. Sci. 1957, 16, 612–622. [Google Scholar]
- Underwood, B.A.; Denning, C.R. Blood and liver concentrations of vitamins A and E in children with cystic fibrosis. Pediatr. Res. 1972, 6, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Myhre, A.M.; Carlsen, M.H.; Bohn, S.K.; Wold, H.L.; Laake, P.; Blomhoff, R. Water-miscible, emulsified, and solid forms of retinol supplements are more toxic than oil-based preparations. Am. J. Clin. Nutr. 2003, 78, 1152–1159. [Google Scholar] [PubMed]
- Penniston, K.L.; Tanumihardjo, S.A. The acute and chronic toxic effects of vitamin A. Am. J. Clin. Nutr. 2006, 83, 137–141. [Google Scholar]
- Bertolaso, C.; Groleau, V.; Schall, J.I.; Maqbool, A.; Mascarenhas, M.; Latham, N.; Dougherty, K.A.; Stallings, V.A. Soluble Vitamins in Cystic Fibrosis and Pancreatic Insufficiency: Efficacy of a Nutrition Intervention. J. Pediatr. Gastroenterol. Nutr. 2014, 58, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Back, E.I.; Frindt, C.; Ocenásková, E.; Nohr, D.; Stern, M.; Biesalski, H.K. Can changes in hydrophobicity increase the bioavailability of α-tocopherol? Eur. J. Nutr. 2015, 45, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Brei, C.; Simon, A.; Krawinkel, M.B.; Naehlich, L. Individualized vitamin A supplementation for patients with cystic fibrosis. Clin. Nutr. 2013, 32, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Colombo, M.L. An update on vitamin E, tocopherol and tocotrienol—Perspectives. Molecules 2010, 15, 2103–2113. [Google Scholar] [CrossRef] [PubMed]
- Tabeling, R. Studies on the Effects of Enzyme Substitution on Nutrient Digestibilities (pre-Caecal/Total) in Pancreatic Duct Ligated Pigs. Ph.D. Thesis, University of Veterinary Medicine, Hannover, Germany, 1988. [Google Scholar]
- GfE (Committee for Requirement Standards of the Society of Nutrition Physiology). Recommendations for the Supply of Energy and Nutrients to Pigs; DLG-Verlag: Frankfurt am Main, Germany, 2008. [Google Scholar]
- Naumann, C.; Bassler, R. Chemical Analysis of Feedstuffs, 3rd ed.; VDLUFA-Verlag: Darmstadt, Germany, 2012. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Control | PL-7 | PL-7 + Vit | PL-16 |
|---|---|---|---|---|
| Body weight (BW), kg | 117 ± 8.07 a | 46.2 ± 22.4 d | 73.5 ± 11.9 c | 96.4 ± 9.89 b |
| Body length, nose to tail, cm | 143 ± 5.59 a | 115 ± 13.4 c | 131 ± 9.58 b | 138 ± 6.41 a,b |
| Metacarpus perimeter, cm | 17.0 ± 0.66 a | 12.6 ± 1.40 c | 14.4 ± 0.79 b | 16.2 ± 0.80 a |
| Feed intake, g as fed/day * | 3001 ± 489 a | 1483 ± 993 b | 2721 ± 824 a | 3093 ± 687 a |
| Feed intake, g as fed/kg BW * | 25.5 ± 3.91 a | 29.5 ± 10.6 a,b | 37.1 ± 9.36 b | 33.1 ± 5.29 a,b |
| BW Gain: Feed # | 0.498 ± 0.026 a | 0.272 ± 0.062 d | 0.337 ± 0.037 c | 0.389 ± 0.029 b |
| Empty body weight, kg | 108 ± 7.11 a | 40.9 ± 19.0 d | 64.7 ± 10.8 c | 82.5 ± 8.61 b |
| Relative mass of GIT, % of BW | 7.95 ± 0.86 a | 17.3 ± 2.00 c | 16.3 ± 2.36 b,c | 14.4 ± 2.75 b |
| Digesta, kg | 5.30 ± 1.11 a | 4.64 ± 1.98 a | 7.41 ± 1.34 b | 8.42 ± 1.61 b |
| Digesta, % of BW | 4.49 ± 0.78 a | 9.53 ± 1.35 b | 9.76 ± 1.88 b | 8.72 ± 1.34 b |
| Chemical Composition (per kg Dry Matter) | |||
|---|---|---|---|
| Crude ash (g) | 55.4 | Cu (mg) | 17.8 |
| Crude protein (g) | 198 | Zn (mg) | 148 |
| Crude fat (g) | 111 | Se (mg) | 0.449 |
| Starch (g) | 400 | Vitamin A (IU) | 13,362 |
| Ca (g) | 11.6 | Vitamin D (IU) | 1850 |
| P (g) | 6.59 | Vitamin E (mg) | 123 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mößeler, A.; Schmicke, M.; Höltershinken, M.; Beyerbach, M.; Kamphues, J. Oral Supplementation with a Special Additive of Retinyl Palmitate and Alpha Tocopherol Reduces Growth Retardation in Young Pancreatic Duct Ligated Pigs Used as a Model for Children Suffering from Exocrine Pancreatic Insufficiency. Int. J. Mol. Sci. 2016, 17, 1642. https://doi.org/10.3390/ijms17101642
Mößeler A, Schmicke M, Höltershinken M, Beyerbach M, Kamphues J. Oral Supplementation with a Special Additive of Retinyl Palmitate and Alpha Tocopherol Reduces Growth Retardation in Young Pancreatic Duct Ligated Pigs Used as a Model for Children Suffering from Exocrine Pancreatic Insufficiency. International Journal of Molecular Sciences. 2016; 17(10):1642. https://doi.org/10.3390/ijms17101642
Chicago/Turabian StyleMößeler, Anne, Marion Schmicke, Martin Höltershinken, Martin Beyerbach, and Josef Kamphues. 2016. "Oral Supplementation with a Special Additive of Retinyl Palmitate and Alpha Tocopherol Reduces Growth Retardation in Young Pancreatic Duct Ligated Pigs Used as a Model for Children Suffering from Exocrine Pancreatic Insufficiency" International Journal of Molecular Sciences 17, no. 10: 1642. https://doi.org/10.3390/ijms17101642