Several Lipid-Related Gene Polymorphisms Interact with Overweight/Obesity to Modulate Blood Pressure Levels

Abstract
:1. Introduction
2. Results
2.1. General Characteristics
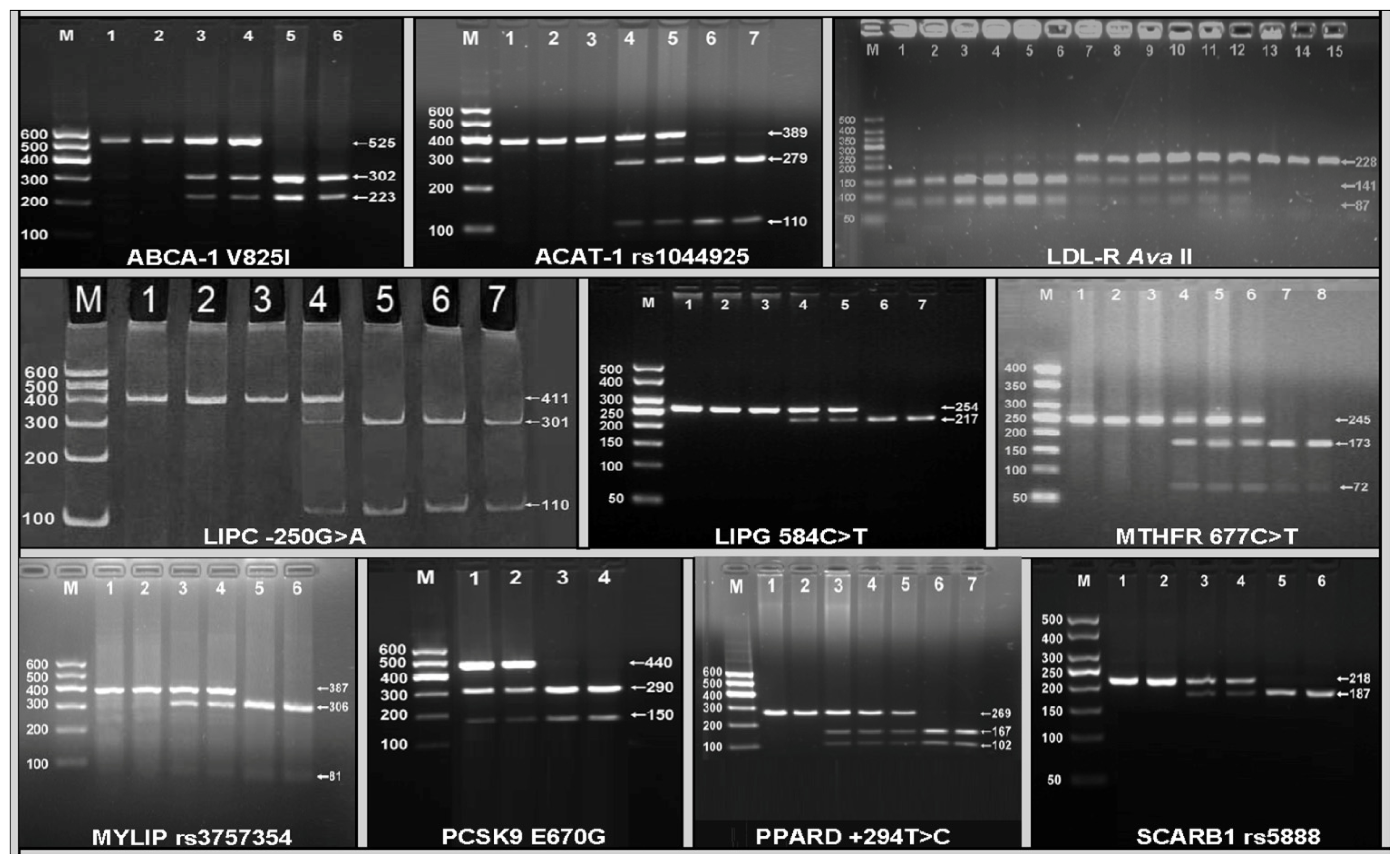
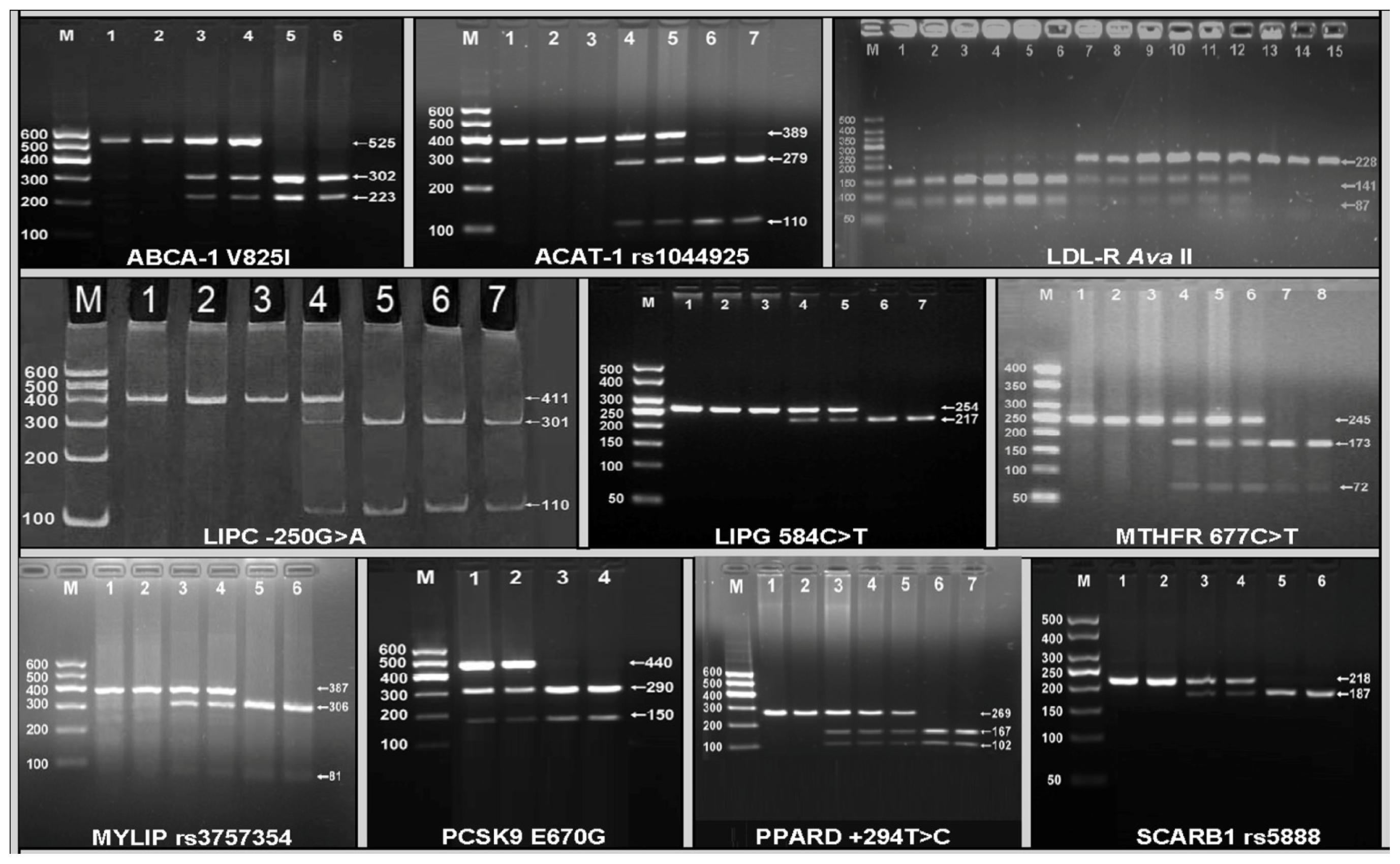
2.2. Electrophoresis and Genotypes
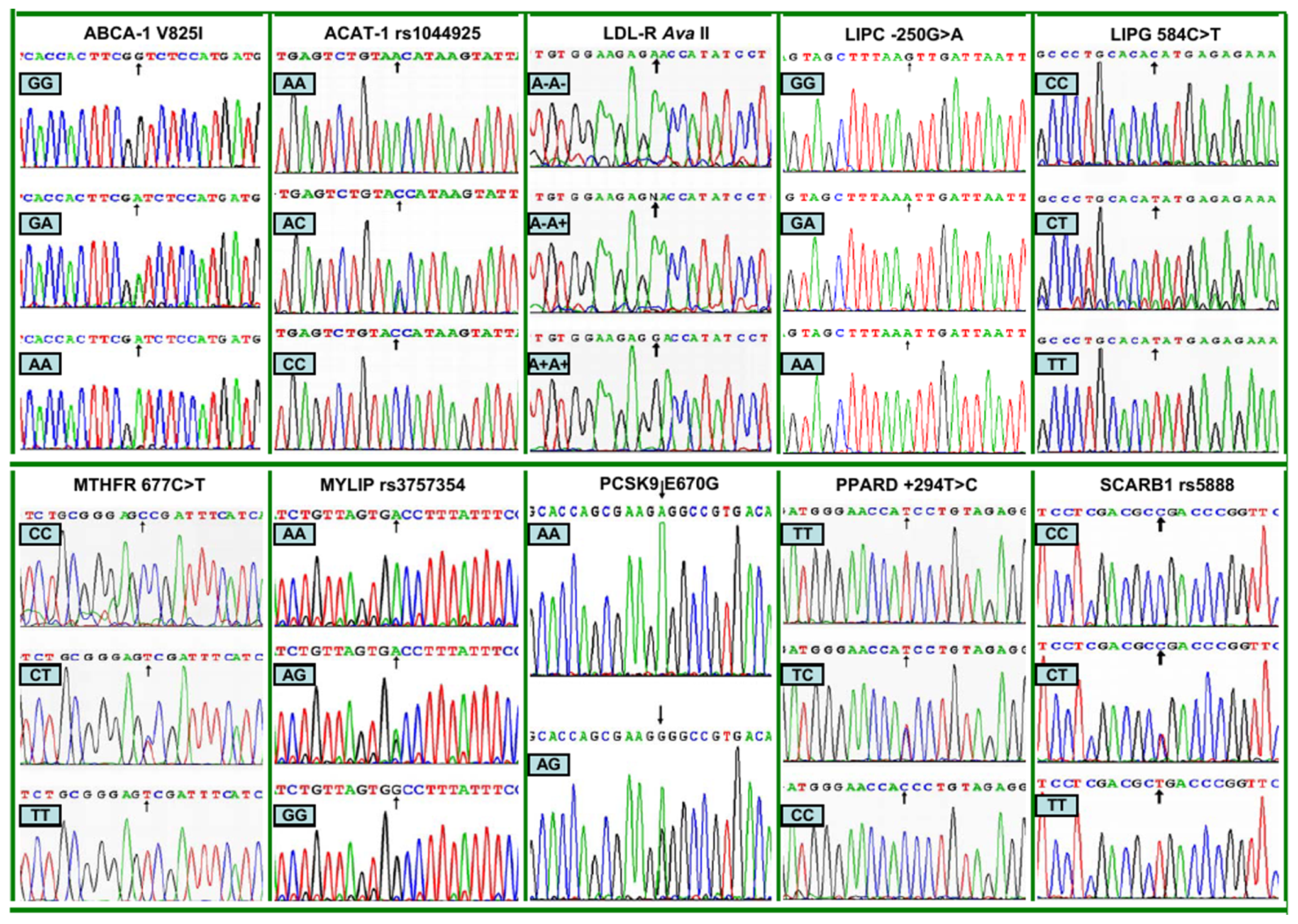
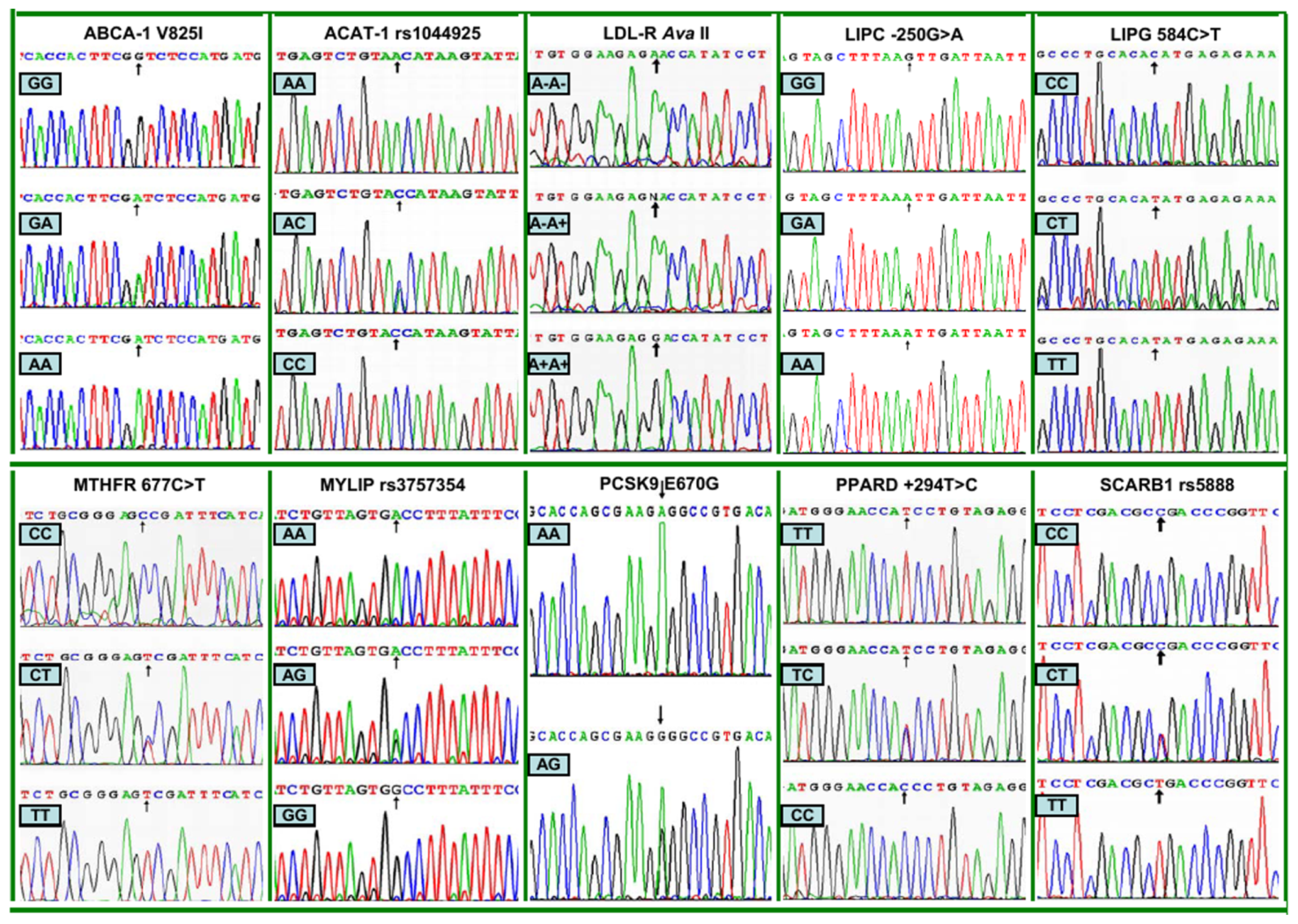
2.3. Nucleotide Sequences
2.4. Genotypic and Allelic Frequencies
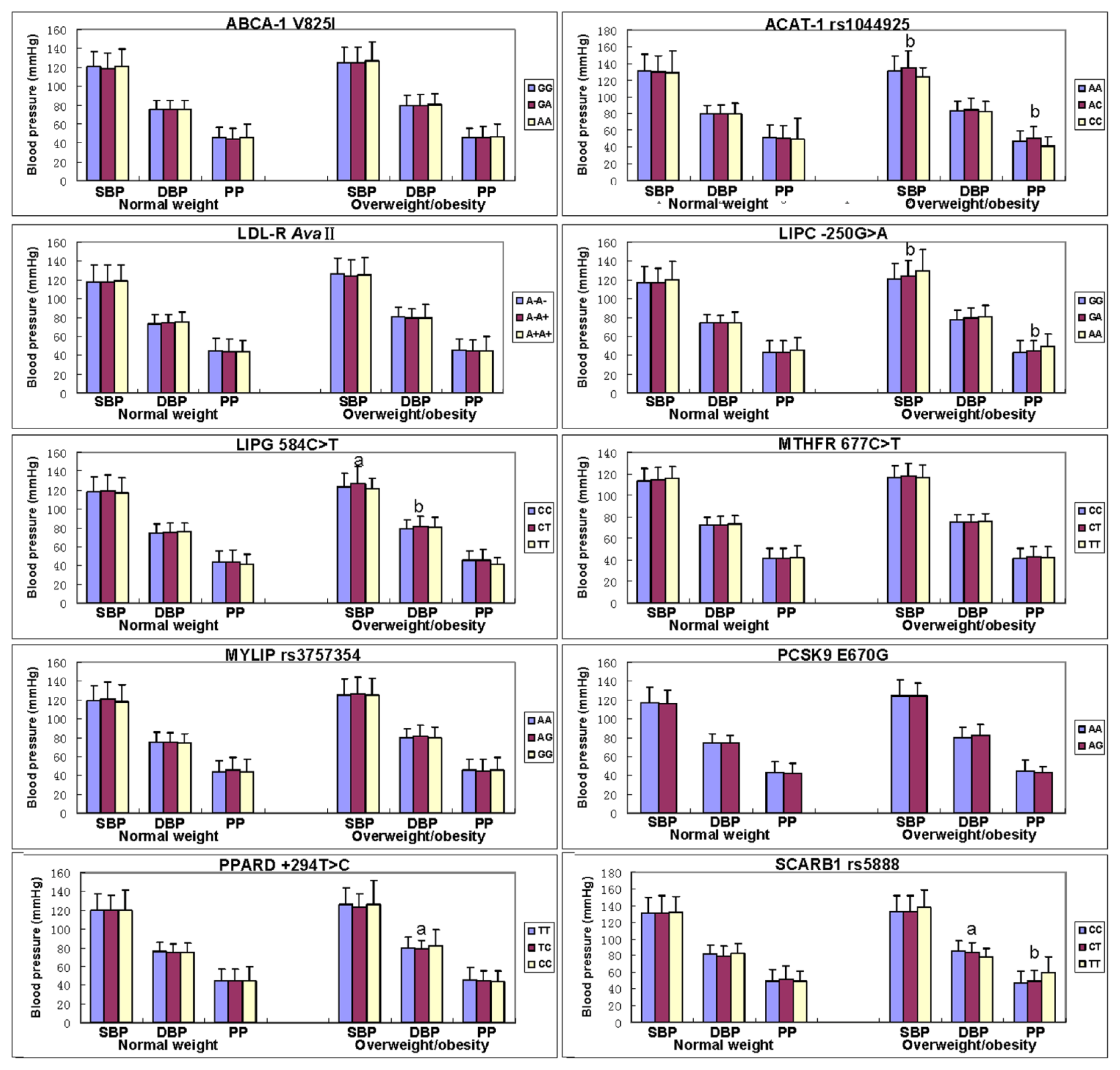
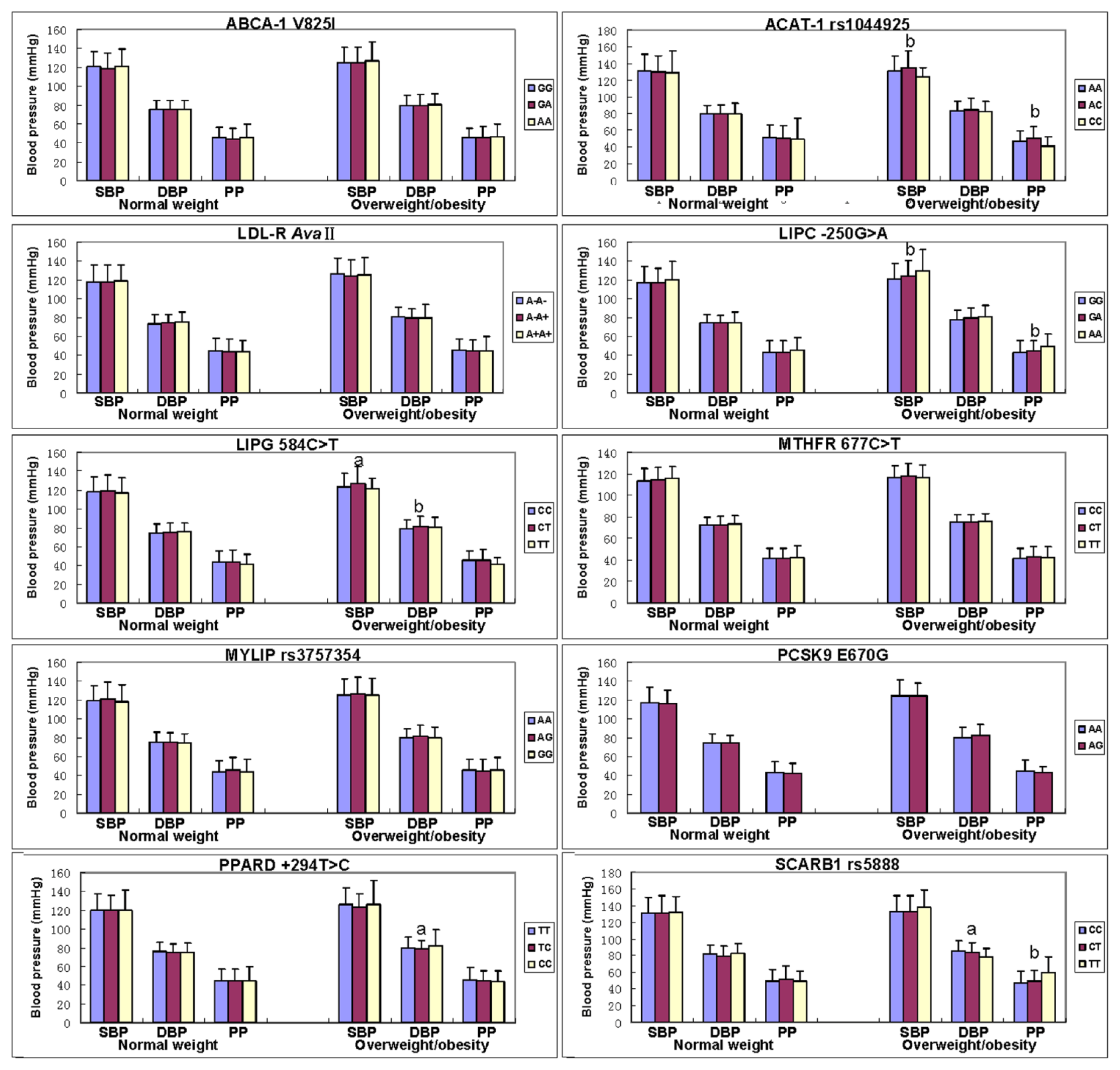
2.5. Genotypes and Blood Pressure Levels
2.6. Interactions of the SNPs and Overweight/Obesity on Blood Pressure Levels
2.7. Correlation between Genotypes or Alleles and Blood Pressure Parameters
3. Experimental Section
3.1. Study Population
3.2. Epidemiological Survey
3.3. Biochemical Measurements
3.4. Genetic Analyses
3.5. DNA Sequencing
3.6. Diagnostic Criteria
3.7. Statistical Analysis
4. Discussion
5. Conclusions
Acknowledgments
References
- Whitworth, J.A. World Health Organization, International Society of Hypertension Writing Group. 2003 World Health Organization (WHO)/International Society of Hypertension (ISH) statement on management of hypertension. J. Hypertens. 2003, 21, 1983–1992. [Google Scholar]
- Hui, P.; Nakayama, T.; Morita, A.; Sato, N.; Hishiki, M.; Saito, K.; Yoshikawa, Y.; Tamura, M.; Sato, I.; Takahashi, T.; et al. Common single nucleotide polymorphisms in Japanese patients with essential hypertension: Aldehyde dehydrogenase 2 gene as a risk factor independent of alcohol consumption. Hypertens. Res 2007, 30, 585–592. [Google Scholar]
- Yin, R.X.; Lin, W.X.; Yang, H.J.; Yang, D.Z.; Li, S.Q.; Pan, S.L.; Feng, Q.M.; Wu, J.Z.; Gan, J.T.; Deng, Y.J. Diet, lifestyle, and blood pressure of the middle-aged and elderly in the Guangxi Bai Ku Yao and Han populations. Am. J. Hypertens 2008, 21, 382–387. [Google Scholar]
- Yin, R.X.; Pan, S.L.; Li, S.Q.; Yang, D.Z.; Lin, W.X.; Feng, Q.M.; Chen, Y.M.; Huang, Y.H.; Zhou, Y.J.; Liao, Q.C. Comparison of hypertension and its risk factors between the Guangxi Bai Ku Yao and Han populations. Blood Press 2008, 17, 306–316. [Google Scholar]
- Yin, R.X.; Wu, D.F.; Wu, J.Z.; Cao, X.L.; Aung, L.H.; Miao, L.; Long, X.J.; Liu, W.Y.; Zhang, L.; Li, M. Interactions of several lipid-related gene polymorphisms and cigarette smoking on blood pressure levels. Int. J. Biol. Sci 2012, 8, 685–696. [Google Scholar]
- Xu, Q.; Wang, Y.H.; Tong, W.J.; Gu, M.L.; Wu, G.; Buren, B.; Liu, Y.Y.; Wang, J.; Li, Y.S.; Feng, H.; et al. Interaction and relationship between angiotensin converting enzyme gene and environmental factors predisposing to essential hypertension in Mongolian population of China. Biomed. Environ. Sci 2004, 17, 177–186. [Google Scholar]
- Levy, D.; Ehret, G.B.; Rice, K.; Verwoert, G.C.; Launer, L.J.; Dehghan, A.; Glazer, N.L.; Morrison, A.C.; Johnson, A.D.; Aspelund, T.; et al. Genome-wide association study of blood pressure and hypertension. Nat. Genet 2009, 41, 677–687. [Google Scholar]
- Newton-Cheh, C.; Johnson, T.; Gateva, V.; Tobin, M.D.; Bochud, M.; Coin, L.; Najjar, S.S.; Zhao, J.H.; Heath, S.C.; Eyheramendy, S.; et al. Genome-wide association study identifies eight loci associated with blood pressure. Nat. Genet 2009, 41, 666–676. [Google Scholar]
- Sõber, S.; Org, E.; Kepp, K.; Juhanson, P.; Eyheramendy, S.; Gieger, C.; Lichtner, P.; Klopp, N.; Veldre, G.; Viigimaa, M.; et al. Targeting 160 candidate genes for blood pressure regulation with a genome-wide genotyping array. PLoS One 2009, 4, e6034. [Google Scholar]
- Ehret, G.B.; Munroe, P.B.; Rice, K.M.; Bochud, M.; Johnson, A.D.; Chasman, D.I.; Smith, A.V.; Tobin, M.D.; Verwoert, G.C.; et al. International Consortium for Blood Pressure Genome-Wide Association Studies. Genetic variants in novel pathways influence blood pressure and cardiovascular disease risk. Nature 2011, 478, 103–109. [Google Scholar] [Green Version]
- Kopelman, P.G. Obesity as a medical problem. Nature 2000, 404, 635–643. [Google Scholar]
- James, P.T. Obesity: The worldwide epidemic. Clin. Dermatol 2004, 22, 276–280. [Google Scholar]
- Cheung, C.Y.; Tso, A.W.; Cheung, B.M.; Xu, A.; Ong, K.L.; Fong, C.H.; Wat, N.M.; Janus, E.D.; Sham, P.C.; Lam, K.S. Obesity susceptibility genetic variants identified from recent genome-wide association studies: Implications in a Chinese population. J. Clin. Endocrinol. Metab 2010, 95, 1395–1403. [Google Scholar]
- Ogden, C.L.; Carroll, M.D.; Curtin, L.R.; McDowell, M.A.; Tabak, C.J.; Flegal, K.M. Prevalence of overweight and obesity in the United States, 1999–2004. J. Am. Med. Assoc 2006, 295, 1549–1555. [Google Scholar]
- Flegal, K.M.; Carroll, M.D.; Ogden, C.L.; Curtin, L.R. Prevalence and trends in obesity among U.S. adults, 1999–2008. J. Am. Med. Assoc 2010, 303, 235–241. [Google Scholar]
- Reynolds, K.; Gu, D.; Whelton, P.K.; Wu, X.; Duan, X.; Mo, J.; He, J. InterASIA Collaborative Group. Prevalence and risk factors of overweight and obesity in China. Obesity (Silver Spring) 2007, 15, 10–18. [Google Scholar]
- Droyvold, W.B.; Midthjell, K.; Nilsen, T.I.; Holmen, J. Change in body mass index and its impact on blood pressure: A prospective population study. Int. J. Obes. Relat. Metab. Disord 2005, 29, 650–655. [Google Scholar]
- Tseng, C.H. Body mass index and blood pressure in adult type 2 diabetic patients in Taiwan. Circ. J 2007, 71, 1749–1754. [Google Scholar]
- Witteman, J.C.; Willett, W.C.; Stampfer, M.J.; Colditz, G.A.; Sacks, F.M.; Speizer, F.E.; Rosner, B.; Hennekens, C.H. A prospective study of nutritional factors and hypertension among US women. Circulation 1989, 80, 1320–1327. [Google Scholar]
- Brock, C.M.; King, D.S.; Wofford, M.R.; Harrell, T.K. Exercise, insulin resistance, and hypertension: A complex relationship. Metab. Syndr. Relat. Disord 2005, 3, 60–65. [Google Scholar]
- Rahmouni, K.; Fath, M.A.; Seo, S.; Thedens, D.R.; Berry, C.J.; Weiss, R.; Nishimura, D.Y.; Sheffield, V.C. Leptin resistance contributes to obesity and hypertension in mouse models of Bardet-Biedl syndrome. J. Clin. Invest 2008, 118, 1458–1467. [Google Scholar]
- Liatis, S.; Tentolouris, N.; Katsilambros, N. Cardiac autonomic nervous system activity in obesity. Pediatr. Endocrinol. Rev 2004, 1, 476–483. [Google Scholar]
- Sarzani, R.; Salvi, F.; Dessì-Fulgheri, P.; Rappelli, A. Renin-angiotensin system, natriuretic peptides, obesity, metabolic syndrome, and hypertension: An integrated view in humans. J. Hypertens 2008, 26, 831–843. [Google Scholar]
- Koenig, W. Haemostatic risk factors for cardiovascular diseases. Eur. Heart J 1998, 19, C39–C43. [Google Scholar]
- Fouillioux, C.; Contreras, F.; Lares, M.; Cano, R.; Leal, E.; Arraiz, N.; Bermúdez, V.; Velasco, M. Metabolic and hemodynamic markers of endothelial dysfunction in patients with hypertension and patients with type 2 diabetes during the cold pressor test. Am. J. Ther 2008, 15, 389–396. [Google Scholar]
- Brocq, M.L.; Leslie, S.J.; Milliken, P.; Megson, I.L. Endothelial dysfunction: From molecular mechanisms to measurement, clinical implications, and therapeutic opportunities. Antioxid. Redox. Signal 2008, 10, 1631–1674. [Google Scholar]
- Li, Q.; Yin, R.X.; Wei, X.L.; Yan, T.T.; Aung, L.H.; Wu, D.F.; Wu, J.Z.; Lin, W.X.; Liu, C.W.; Pan, S.L. ATP-binding cassette transporter G5 and G8 polymorphisms and several environmental factors with serum lipid levels. PLoS One 2012, 7, e37972. [Google Scholar]
- Selby, J.V.; Newman, B.; Quiroga, J.; Christian, J.C.; Austin, M.A.; Fabsitz, R.R. Concordance for dyslipidemic hypertension in male twins. J. Am. Med. Assoc 1991, 265, 2079–2084. [Google Scholar]
- Ruixing, Y.; Jinzhen, W.; Weixiong, L.; Yuming, C.; Dezhai, Y.; Shangling, P. The environmental and genetic evidence for the association of hyperlipidemia and hypertension. J. Hypertens 2009, 27, 251–258. [Google Scholar]
- Hunt, S.C.; Stephenson, S.H.; Hopkins, P.N.; Williams, R.R. Predictors of an increased risk of future hypertension in Utah. A screening analysis. Hypertension 1991, 17, 969–976. [Google Scholar]
- Halperin, R.O.; Sesso, H.D.; Ma, J.; Buring, J.E.; Stampfer, M.J.; Gaziano, J.M. Dyslipidemia and the risk of incident hypertension in men. Hypertension 2006, 47, 45–50. [Google Scholar]
- Shen, B.J.; Todaro, J.F.; Niaura, R.; McCaffery, J.M.; Zhang, J., III; Spiro, A.; Ward, K.D. Are metabolic risk factors one unified syndrome? Modeling the structure of the metabolic syndrome X. Am. J. Epidemiol 2003, 157, 701–711. [Google Scholar]
- Allayee, H.; de Bruin, T.W.; Dominguez, K.M.; Cheng, L.S.; Ipp, E.; Cantor, R.M.; Krass, K.L.; Keulen, E.T.; Aouizerat, B.E.; Lusis, A.J.; et al. Genome scan for blood pressure in Dutch dyslipidemic families reveals linkage to a locus on chromosome 4p. Hypertension 2001, 38, 773–778. [Google Scholar]
- Franceschini, N.; Reiner, A.P.; Heiss, G. Recent findings in the genetics of blood pressure and hypertension traits. Am. J. Hypertens 2011, 24, 392–400. [Google Scholar]
- Liu, A.P.; Zhan, S.Y.; Li, L.M.; Hu, Y.H.; Cao, W.H.; Wu, T.; Li, J.; Guo, X.X. Association between AvaII exon 13 polymorphism at the LDL receptor gene different and serum lipid levels in normotensives and essential hypertensives in Shanghai (In Chinese). Zhonghua Liu Xing Bing Xue Za Zhi 2003, 24, 542–546. [Google Scholar]
- Rodríguez-Esparragón, F.; Hernández-Perera, O.; Rodríguez-Pérez, J.C.; Anábitarte, A.; Díaz-Cremades, J.M.; Losada, A.; Fiuza, D.; Hernández, E.; Yunis, C.; Ferrario, C.M. The effect of methylenetetrahydrofolate reductase C677T common variant on hypertensive risk is not solely explained by increased plasma homocysteine values. Clin. Exp. Hypertens 2003, 25, 209–220. [Google Scholar]
- Kosmas, I.P.; Tatsioni, A.; Ioannidis, J.P. Association of C677T polymorphism in the methylenetetrahydrofolate reductase gene with hypertension in pregnancy and pre-eclampsia: A meta-analysis. J. Hypertens 2004, 22, 1655–1662. [Google Scholar]
- Jiang, S.; Hsu, Y.H.; Xu, X.; Xing, H.; Chen, C.; Niu, T.; Zhang, Y.; Peng, S.; Xu, X. The C677T polymorphism of the methylenetetrahydrofolate reductase gene is associated with the level of decrease on diastolic blood pressure in essential hypertension patients treated by angiotensin-converting enzyme inhibitor. Thromb. Res 2004, 113, 361–369. [Google Scholar]
- Jiang, S.; Hsu, Y.H.; Niu, T.; Xu, X.; Xing, H.; Chen, C.; Wang, X.; Zhang, Y.; Peng, S.; Xu, X. A common haplotype on methylenetetrahydrofolate reductase gene modifies the effect of angiotensin-converting enzyme inhibitor on blood pressure in essential hypertension patients—A family-based association study. Clin. Exp. Hypertens 2005, 27, 509–521. [Google Scholar]
- Qian, X.; Lu, Z.; Tan, M.; Liu, H.; Lu, D. A meta-analysis of association between C677T polymorphism in the methylenetetrahydrofolate reductase gene and hypertension. Eur. J. Hum. Genet 2007, 15, 1239–1245. [Google Scholar]
- Markan, S.; Sachdeva, M.; Sehrawat, B.S.; Kumari, S.; Jain, S.; Khullar, M. MTHFR 677 CT/MTHFR 1298 CC genotypes are associated with increased risk of hypertension in Indians. Mol. Cell. Biochem 2007, 302, 125–131. [Google Scholar]
- Marinho, C.; Alho, I.; Arduíno, D.; Falcão, L.M.; Brás-Nogueira, J.; Bicho, M. GST M1/T1 and MTHFR polymorphisms as risk factors for hypertension. Biochem. Biophys. Res. Commun 2007, 353, 344–350. [Google Scholar]
- Ilhan, N.; Kucuksu, M.; Kaman, D.; Ilhan, N.; Ozbay, Y. The 677 C/T MTHFR polymorphism is associated with essential hypertension, coronary artery disease, and higher homocysteine levels. Arch. Med. Res 2008, 39, 125–130. [Google Scholar]
- Ravera, M.; Viazzi, F.; Berruti, V.; Leoncini, G.; Zagami, P.; Bezante, G.P.; Rosatto, N.; Ravazzolo, R.; Pontremoli, R.; Deferrari, G. 5,10-Methylenetetrahydrofolate reductase polymorphism and early organ damage in primary hypertension. Am. J. Hypertens 2001, 14, 371–376. [Google Scholar]
- Lwin, H.; Yokoyama, T.; Yoshiike, N.; Saito, K.; Yamamoto, A.; Date, C.; Tanaka, H. Polymorphism of methylenetetrahydrofolate reductase gene (C677T MTHFR) is not a confounding factor of the relationship between serum uric acid level and the prevalence of hypertension in Japanese men. Circ. J 2006, 70, 83–87. [Google Scholar]
- Stiefel, P.; Miranda, M.L.; Bellido, L.M.; Luna, J.; Jiménez, L.; Pamies, E.; de Frutos, P.G.; Villar, J. Genotype of the CYBA promoter-930A/G, polymorphism C677T of the MTHFR and APOE genotype in patients with hypertensive disorders of pregnancy: An observational study. Med. Clin (Barc) 2009, 133, 657–661. [Google Scholar]
- Gao, L.; Wang, L.; Yun, H.; Su, L.; Su, X. Association of the PPARgamma2 gene Pro12Ala variant with primary hypertension and metabolic lipid disorders in Han Chinese of Inner Mongolia. Genet. Mol. Res 2010, 9, 1312–1320. [Google Scholar]
- Ostgren, C.J.; Lindblad, U.; Melander, O.; Melander, A.; Groop, L.; Råstam, L. Peroxisome proliferator-activated receptor-gammaPro12Ala polymorphism and the association with blood pressure in type 2 diabetes: Skaraborg hypertension and diabetes project. J. Hypertens 2003, 21, 1657–1662. [Google Scholar]
- Yan, Z.C.; Shen, C.Y.; Zhong, J.; Wang, L.; Ni, Y.X.; Nie, H.; Zhu, Z.M. PPARdelta + 294T/C gene polymorphism related to plasma lipid, obesity and left ventricular hypertrophy in subjects with metabolic syndrome (In Chinese). Zhonghua Xin Xue Guan Bing Za Zhi 2005, 33, 529–533. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Characteristics | Normal weight | Overweight/obesity | t (χ2) | p |
|---|---|---|---|---|
| Number | 978 | 751 | - | - |
| Male/female | 490/488 | 378/373 | 0.009 | 0.924 |
| Age, years | 41.48 ± 16.21 | 41.25 ± 12.50 | 0.332 | 0.740 |
| Education level, years | 3.71 ± 3.89 | 4.71 ± 4.49 | −4.170 | 0.000 |
| Height, cm | 153.73 ± 7.57 | 154.29 ± 8.49 | −1.461 | 0.144 |
| Weight, kg | 50.28 ± 6.20 | 63.19 ± 8.86 | −34.042 | 0.000 |
| Body mass index, kg/m2 | 21.23 ± 1.68 | 26.48 ± 2.59 | −48.285 | 0.000 |
| Waist circumference, cm | 70.58 ± 6.56 | 82.90 ± 7.39 | −30.766 | 0.000 |
| Alcohol consumption, n (%) | 373 (38.1) | 362 (48.2) | 23.034 | 0.000 |
| Cigarette smoking, n (%) | 305 (31.2) | 178 (23.7) | 15.036 | 0.001 |
| Systolic blood pressure, mmHg | 119.69 ± 17.40 | 125.84 ± 17.64 | −7.242 | 0.000 |
| Diastolic blood pressure, mmHg | 75.11 ± 9.98 | 80.57 ± 11.13 | −10.563 | 0.000 |
| Pulse pressure, mmHg | 44.60 ± 12.87 | 45.36 ± 12.11 | −1.251 | 0.211 |
| Total cholesterol, mmol/L | 4.46 ± 0.94 | 5.01 ± 1.05 | −11.325 | 0.000 |
| Triglyceride, mmol/L | 1.21 ± 1.02 | 1.74 ± 1.50 | −8.837 | 0.000 |
| HDL-C, mmol/L | 1.80 ± 0.47 | 1.73 ± 0.41 | 3.099 | 0.002 |
| LDL-C, mmol/L | 2.52 ± 0.73 | 2.96 ± 0.85 | −11.180 | 0.000 |
| Apolipoprotein (Apo) A1, g/L | 1.37 ± 0.31 | 1.40 ± 0.27 | −2.009 | 0.045 |
| ApoB, g/L | 0.84 ± 0.22 | 0.98 ± 0.24 | −12.466 | 0.000 |
| ApoA1/ApoB | 1.75 ± 0.70 | 1.53 ± 0.58 | 7.256 | 0.000 |
| SNP | Genotype (Allele) | Normal weight (n = 978) | Overweight/obesity (n = 751) | χ2 | p |
|---|---|---|---|---|---|
| ABCA-1 V825I (rs2066715) | GG | 326 (33.3) | 269 (35.8) | ||
| GA | 480 (49.1) | 334 (44.5) | |||
| AA | 172 (17.6) | 148 (19.7) | 3.708 | 0.157 | |
| G | 1132 (57.9) | 872 (58.1) | |||
| A | 824 (42.1) | 630 (41.9) | 0.012 | 0.914 | |
| ACAT-1 (rs1044925) | AA | 662 (67.7) | 527 (70.2) | ||
| AC | 279 (28.5) | 205 (27.3) | |||
| CC | 37 (3.8) | 19 (2.5) | 2.671 | 0.263 | |
| A | 1603 (82.0) | 1259 (83.8) | |||
| C | 353 (18.0) | 243 (16.2) | 2.080 | 0.149 | |
| LDL-R AvaII | A−A− | 527 (53.9) | 389 (51.8) | ||
| A−A+ | 371 (37.9) | 295 (39.3) | |||
| A+A+ | 80 (8.2) | 67 (8.9) | 0.824 | 0.662 | |
| A− | 1425 (72.9) | 1073 (71.4) | |||
| A+ | 531 (27.1) | 429 (28.6) | 0.848 | 0.357 | |
| LIPC −250G > A (rs2070895) | GG | 480 (49.1) | 233 (31.0) | ||
| GA | 425 (43.5) | 432 (57.5) | |||
| AA | 73 (7.5) | 86 (11.5) | 57.882 | 0.000 | |
| G | 1385 (70.8) | 898 (59.8) | |||
| A | 571 (29.2) | 604 (40.2) | 45.999 | 0.000 | |
| LIPG 584C > T (rs2000813) | CC | 454 (46.4) | 308 (41.0) | ||
| CT | 477 (48.8) | 412 (54.9) | |||
| TT | 47 (4.8) | 31 (4.1) | 6.314 | 0.043 | |
| C | 1385 (70.8) | 1028 (68.4) | |||
| T | 571 (29.2) | 474 (31.6) | 2.255 | 0.133 | |
| MTHFR 677C > T (rs1801133) | CC | 471 (48.2) | 354 (47.1) | ||
| CT | 441 (45.1) | 341 (45.4) | |||
| TT | 66 (6.7) | 56 (7.5) | 0.404 | 0.817 | |
| C | 1383 (70.7) | 1049 (69.8) | |||
| T | 573 (29.3) | 453 (30.2) | 0.305 | 0.581 | |
| MYLIP (rs3757354) | AA | 230 (23.5) | 148 (19.7) | ||
| AG | 477 (48.8) | 363 (48.3) | |||
| GG | 271 (27.7) | 240 (32.0) | 5.431 | 0.066 | |
| A | 937 (47.9) | 659 (43.9) | |||
| G | 1019 (52.1) | 843 (56.1) | 5.550 | 0.018 | |
| PCSK9 E670G (rs505151) | AA | 916 (93.7) | 721 (96.0) | ||
| AG | 62 (6.3) | 30 (4.0) | |||
| GG | 0 | 0 | 4.636 | 0.031 | |
| A | 1894 (96.8) | 1472 (98.0) | |||
| G | 62 (3.2) | 30 (2.0) | 4.509 | 0.034 | |
| PPARD +294T > C (rs2016520) | TT | 559 (57.2) | 396 (52.7) | ||
| TC | 354 (36.2) | 312 (41.5) | |||
| CC | 65 (6.6) | 43 (5.7) | 5.239 | 0.073 | |
| T | 1472 (75.3) | 1104 (73.5) | |||
| C | 484 (24.7) | 398 (26.5) | 1.375 | 0.241 | |
| SCARB1 (rs5888) | CC | 548 (56.0) | 417 (55.5) | ||
| CT | 390 (39.9) | 311 (41.4) | |||
| TT | 40 (4.1) | 23 (3.1) | 1.497 | 0.473 | |
| C | 1486 (76.0) | 1145 (76.2) | |||
| T | 470 (24.0) | 357 (23.8) | 0.032 | 0.859 | |
| SNP | Genotype | Normal weight | Overweight/obesity | ||||
|---|---|---|---|---|---|---|---|
| SBP | DBP | PP | SBP | DBP | PP | ||
| ABCA-1 V825I (rs2066715) | GG | 120.5 ± 15.9 | 75.4 ± 10.0 | 45.2 ± 11.2 | 125.5 ± 15.4 | 80.0 ± 10.1 | 45.6 ± 10.2 |
| GA | 118.8 ± 16.3 | 75.0 ± 9.6 | 43.8 ± 11.9 | 125.1 ± 16.5 | 79.6 ± 11.3 | 45.5 ± 11.4 | |
| AA | 120.9 ± 18.6 | 75.5 ± 9.2 | 45.5 ± 14.3 | 126.5 ± 20.1 | 80.1 ± 12.2 | 46.4 ± 13.4 | |
| F | 2.127 | 0.262 | 2.309 | 0.199 | 0.079 | 0.724 | |
| p | 0.120 | 0.770 | 0.100 | 0.820 | 0.924 | 0.485 | |
| ACAT-1 (rs1044925) | AA | 130.6 ± 20.2 | 79.4 ± 10.6 | 51.2 ± 15.0 | 130.3 ± 18.3 | 83.5 ± 11.3 | 46.8 ± 12.5↓ |
| AC | 129.6 ± 19.0 | 79.7 ± 11.1 | 49.9 ± 15.3 | 135.1 ± 20.1↑ | 84.9 ± 13.9 | 50.2 ± 13.9 | |
| CC | 129.0 ± 25.5 | 79.8 ± 12.7 | 49.2 ± 24.9 | 123.5 ± 11.5↓ | 82.1 ± 12.7 | 41.5 ± 10.4↓ | |
| F | 0.338 | 0.112 | 1.048 | 5.825 | 1.289 | 5.910 | |
| p | 0.714 | 0.894 | 0.351 | 0.000 c | 0.276 | 0.000 c | |
| LDL-R AvaII | A−A− | 118.0 ± 17.5 | 73.4 ± 9.8 | 44.5 ± 13.2 | 126.3 ± 16.7 | 80.5 ± 10.8↑ | 45.8 ± 11.7 |
| A−A+ | 118.1 ± 18.0 | 74.2 ± 9.3 | 43.9 ± 12.9 | 123.9 ± 17.3 | 79.2 ± 10.0 | 44.7 ± 11.4 | |
| A+A+ | 118.9 ± 17.1 | 74.9 ± 10.5 | 44.0 ± 11.2 | 124.7 ± 18.9 | 79.8 ± 13.7 | 45.0 ± 15.2 | |
| F | 0.142 | 1.420 | 0.340 | 2.249 | 4.276 | 0.538 | |
| p | 0.867 | 0.242 | 0.712 | 0.106 | 0.003 c | 0.548 | |
| LIPC −250G > A (rs2070895) | GG | 117.1 ± 16.9 | 74.2 ± 9.3 | 42.9 ± 12.7 | 120.6 ± 16.9 | 77.8 ± 9.7 | 42.8 ± 13.1 |
| GA | 116.8 ± 15.8 | 73.8 ± 8.9 | 43.0 ± 12.3 | 123.8 ± 16.4↑ | 79.5 ± 10.4↑ | 44.3 ± 10.9 | |
| AA | 119.8 ± 19.2 | 74.3 ± 11.8 | 45.5 ± 13.5 | 129.7 ± 22.0↑ | 80.2 ± 12.6 | 49.5 ± 13.1 | |
| F | 1.347 | 0.299 | 1.685 | 4.233 | 3.125 | 2.367 | |
| p | 0.261 | 0.741 | 0.186 | 0.003c | 0.009 c | 0.094 | |
| LIPG 584C > T (rs2000813) | CC | 117.8 ± 15.8 | 74.4 ± 9.5 | 43.37 ± 12.30 | 123.6 ± 13.9 | 78.2 ± 10.5 | 45.3 ± 10.5 |
| CT | 119.1 ± 17.0 | 75.3 ± 9.6 | 43.81 ± 12.60 | 126.8 ± 18.2 | 81.1 ± 11.0 | 45.7 ± 11.6 | |
| TT | 116.8 ± 16.2 | 76.0 ± 8.8 | 41.07 ± 10.72 | 121.5 ± 11.1 | 80.1 ± 10.9 | 41.4 ± 6.8 | |
| F | 1.214 | 1.452 | 1.261 | 0.920 | 2.408 | 0.087 | |
| p | 0.297 | 0.235 | 0.284 | 0.399 | 0.090 | 0.917 | |
| MTHFR 677C > T (rs1801133) | CC | 113.7 ± 11.7 | 72.6 ± 7.5 | 41.1 ± 9.7 | 116.4 ± 10.9 | 74.8 ± 7.5 | 41.7 ± 9.3 |
| CT | 114.1 ± 11.9 | 73.0 ± 7.3 | 41.1 ± 9.5 | 118.1 ± 11.7 | 75.2 ± 6.6 | 43.0 ± 9.6 | |
| TT | 115.8 ± 10.5 | 73.4 ± 7.6 | 42.5 ± 10.4 | 116.8 ± 11.7 | 75.7 ± 7.6 | 42.6 ± 10.2 | |
| F | 1.057 | 0.604 | 0.660 | 1.312 | 0.005 | 1.186 | |
| p | 0.348 | 0.547 | 0.517 | 0.270 | 0.995 | 0.306 | |
| MYLIP (rs3757354) | AA | 118.9 ± 16.3 | 75.5 ± 9.9 | 43.5 ± 11.8 | 125.5 ± 16.5 | 79.5 ± 9.9 | 46.0 ± 11.2 |
| AG | 120.8 ± 17.7 | 75.4 ± 10.0 | 45.4 ± 13.3 | 126.3 ± 17.9 | 81.5 ± 11.2 | 44.8 ± 12.0 | |
| GG | 118.4 ± 17.6 | 74.4 ± 10.0 | 44.1 ± 12.9 | 125.4 ± 18.0 | 79.9 ± 11.6 | 45.8 ± 12.8 | |
| F | 2.122 | 1.194 | 2.224 | 0.293 | 1.648 | 2.565 | |
| p | 0.120 | 0.303 | 0.109 | 0.746 | 0.193 | 0.077 | |
| PCSK9 E670G (rs505151) | AA | 117.2 ± 16.3 | 74.2 ± 9.6 | 42.9 ± 12.0 | 124.2 ± 16.9 | 79.8 ± 11.0 | 44.4 ± 12.1 |
| AG | 116.0 ± 15.0 | 74.1 ± 8.1 | 41.8 ± 11.3 | 124.7 ± 13.1 | 82.2 ± 11.9 | 42.5 ± 6.4 | |
| F | 0.418 | 0.006 | 0.620 | 0.457 | 1.868 | 0.085 | |
| p | 0.518 | 0.938 | 0.431 | 0.499 | 0.172 | 0.770 | |
| PPARD +294T > C (rs2016520) | TT | 120.0 ± 17.5 | 75.7 ± 10.1 | 44.4 ± 12.8 | 125.8 ± 18.3 | 79.9 ± 11.1 | 45.9 ± 13.3 |
| TC | 119.4 ± 16.6 | 74.6 ± 9.2 | 44.7 ± 12.1 | 123.5 ± 14.6 | 78.4 ± 8.9 | 45.1 ± 10.7 | |
| CC | 120.0 ± 21.3 | 75.5 ± 9.8 | 44.5 ± 15.5 | 125.9 ± 25.7 | 82.0 ± 17.4 | 43.9 ± 11.2 | |
| F | 0.207 | 1.301 | 0.088 | 0.629 | 0.858 | 0.703 | |
| p | 0.813 | 0.273 | 0.916 | 0.533 | 0.424 | 0.495 | |
| SCARB1 (rs5888) | CC | 130.3 ± 19.3 | 81.2 ± 11.7 | 49.1 ± 14.7 | 132.4 ± 19.9 | 85.1 ± 12.0 | 47.3 ± 14.2 |
| CT | 131.1 ± 20.6 | 79.7 ± 11.5 | 51.4 ± 16.4 | 132.6 ± 19.1 | 83.6 ± 11.5 | 48.9 ± 13.8 | |
| TT | 131.7 ± 19.5 | 82.1 ± 12.6 | 49.6 ± 11.4 | 137.6 ± 21.2 | 78.6 ± 10.3 | 59.1 ± 19.8↑ | |
| F | 0.227 | 2.190 | 2.615 | 0.357 | 2.920 | 4.830 | |
| p | 0.797 | 0.112 | 0.074 | 0.700 | 0.054 | 0.002 c | |
| Blood pressure | Genotype/allele | Unstandardized coefficient | Std. error | Standardized coefficient | t | p |
|---|---|---|---|---|---|---|
| Total population | ||||||
| SBP | LIPC −250G > A genotype | 2.211 | 0.587 | 0.081 | 3.764 | 0.000 |
| LIPC −250G > A allele | 1.887 | 0.760 | 0.054 | 2.482 | 0.013 | |
| LIPG 584C > T allele | 1.799 | 0.737 | 0.053 | 2.414 | 0.016 | |
| DBP | LIPG 584C > T genotype | 1.396 | 0.403 | 0.077 | 3.460 | 0.001 |
| LIPG 584C > T allele | 1.734 | 0.466 | 0.083 | 3.718 | 0.000 | |
| PPARD +294T > C allele | −0.964 | 0.469 | −0.046 | −2.054 | 0.040 | |
| SCARB1 rs5888 genotype | −1.298 | 0.494 | −0.062 | −2.627 | 0.009 | |
| SCARB1 rs5888 allele | −1.530 | 0.564 | −0.064 | −2.711 | 0.007 | |
| PP | SCARB1 rs5888 genotype | 1.945 | 0.606 | 0.074 | 3.208 | 0.001 |
| SCARB1 rs5888 allele | 2.095 | 0.694 | 0.070 | 3.016 | 0.003 | |
| Overweight/obesity | ||||||
| SBP | ACAT-1 rs1044925 genotype | 2.884 | 1.277 | 0.079 | 2.259 | 0.024 |
| ACAT-1 rs1044925 allele | 4.816 | 1.443 | 0.116 | 3.338 | 0.001 | |
| LIPC −250G > A genotype | 4.317 | 0.933 | 0.154 | 4.629 | 0.000 | |
| LIPC −250G > A allele | 4.415 | 1.267 | 0.117 | 3.484 | 0.001 | |
| LIPG 584C > T allele | 2.850 | 1.166 | 0.085 | 2.444 | 0.015 | |
| DBP | LIPC −250G > A genotype | 1.444 | 0.579 | 0.086 | 2.493 | 0.013 |
| LIPC −250G > A allele | 1.938 | 0.782 | 0.085 | 2.478 | 0.013 | |
| LIPG 584C > T genotype | 2.167 | 0.671 | 0.112 | 3.232 | 0.001 | |
| LIPG 584C > T allele | 2.783 | 0.764 | 0.126 | 3.644 | 0.000 | |
| SCARB1 rs5888 genotype | −1.979 | 0.762 | −0.093 | −2.597 | 0.010 | |
| SCARB1 rs5888 allele | −1.788 | 0.856 | −0.075 | −2.089 | 0.037 | |
| PP | ACAT-1 rs1044925 allele | 2.651 | 0.941 | 0.093 | 2.816 | 0.005 |
| LIPC −250G > A genotype | 2.862 | 0.650 | 0.148 | 4.405 | 0.000 | |
| LIPC −250G > A allele | 2.414 | 0.882 | 0.093 | 2.736 | 0.006 | |
| SCARB1 rs5888 genotype | 2.989 | 0.884 | 0.117 | 3.383 | 0.001 | |
| SCARB1 rs5888 allele | 2.384 | 0.994 | 0.083 | 2.397 | 0.017 | |
© 2012 by the authors; licensee Molecular Diversity Preservation International, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Yin, R.-X.; Wu, D.-F.; Aung, L.H.H.; Yan, T.-T.; Cao, X.-L.; Long, X.-J.; Miao, L.; Liu, W.-Y.; Zhang, L.; Li, M. Several Lipid-Related Gene Polymorphisms Interact with Overweight/Obesity to Modulate Blood Pressure Levels. Int. J. Mol. Sci. 2012, 13, 12062-12081. https://doi.org/10.3390/ijms130912062
Yin R-X, Wu D-F, Aung LHH, Yan T-T, Cao X-L, Long X-J, Miao L, Liu W-Y, Zhang L, Li M. Several Lipid-Related Gene Polymorphisms Interact with Overweight/Obesity to Modulate Blood Pressure Levels. International Journal of Molecular Sciences. 2012; 13(9):12062-12081. https://doi.org/10.3390/ijms130912062
Chicago/Turabian StyleYin, Rui-Xing, Dong-Feng Wu, Lynn Htet Htet Aung, Ting-Ting Yan, Xiao-Li Cao, Xing-Jiang Long, Lin Miao, Wan-Ying Liu, Lin Zhang, and Meng Li. 2012. "Several Lipid-Related Gene Polymorphisms Interact with Overweight/Obesity to Modulate Blood Pressure Levels" International Journal of Molecular Sciences 13, no. 9: 12062-12081. https://doi.org/10.3390/ijms130912062