
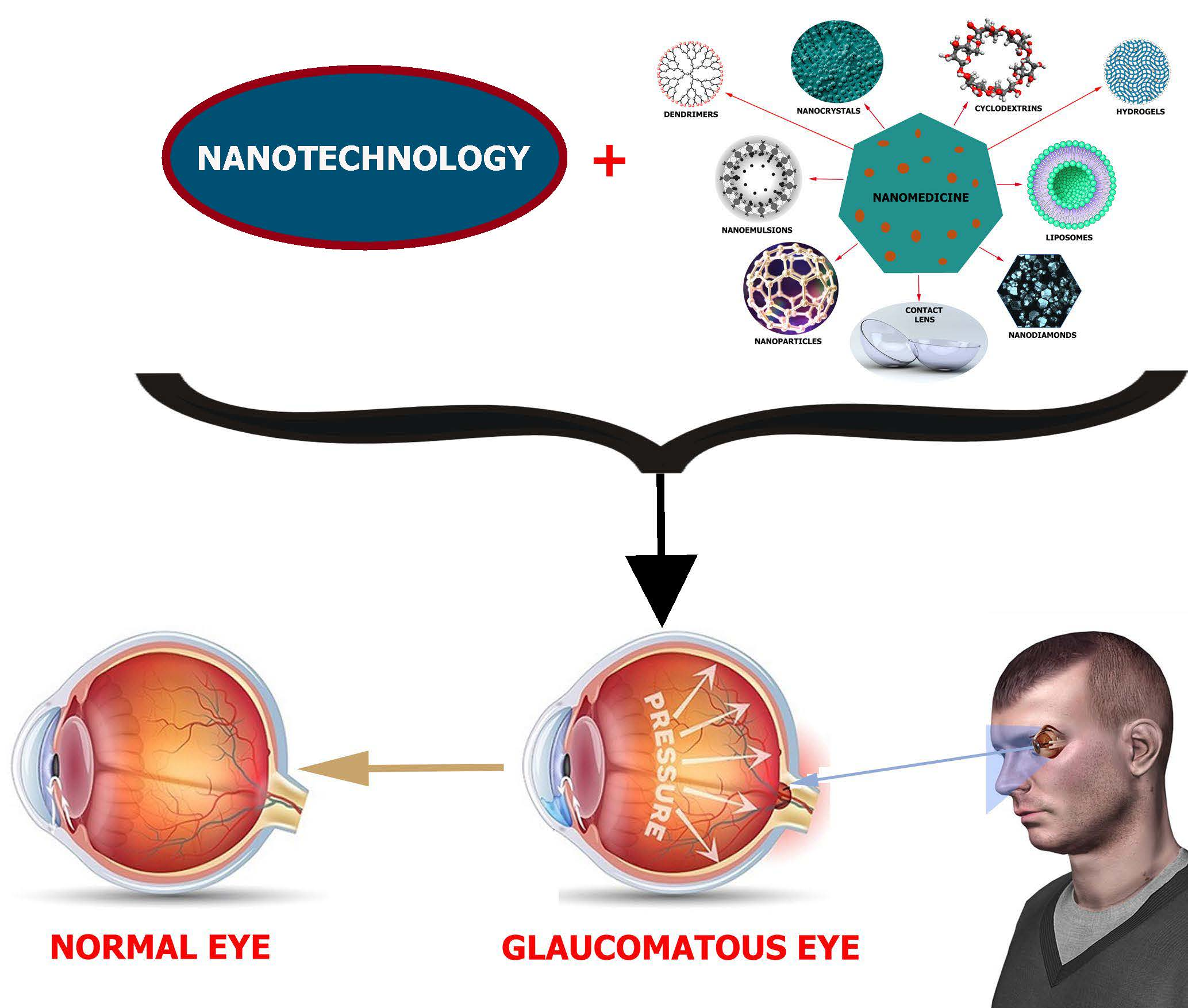
Promising Approach in the Treatment of Glaucoma Using Nanotechnology and Nanomedicine-Based Systems

 ,
,
Abstract
:
1. Introduction
2. Anatomy of the Human Eye and its Constraints
3. Advancements of Nanomedicine in Glaucoma
Triggered, Controlled and Sustained Drug Release in Glaucoma
4. Nanosystems for Posterior and Anterior Glaucoma Therapy
5. Diagnostic and Therapeutic Glaucoma Nanodevices
5.1. Therapeutic Nanodevices
5.2. Measurement of Intraocular Pressure
5.3. Imaging
5.4. Surgical Implants
Refined Surgical Implants
6. Replacement and Regeneration of the Trabecular Meshwork (TM)
7. Major Challenges, Expected Breakthrough, and Conclusions
7.1. Major Challenges
7.2. Expected Breakthrough
7.3. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Initiative, U.S.N.N. What It Iis and How It Works. Available online: https://www.nano.gov/nanotech-101/what (accessed on 1 May 2019).
- Li, X.; Chen, H.; Dang, Y.; Lin, Y.; Larson, C.A.; Roco, M.C. A longitudinal analysis of nanotechnology literature: 1976–2004. J. Nanoparticle Res. 2008, 10, 3–22. [Google Scholar] [CrossRef]
- Gao, W.; Chan, J.M.; Farokhzad, O.C. pH-responsive nanoparticles for drug delivery. Mol. Pharm. 2010, 7, 1913–1920. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Tang, Y.; Oh, Y.; Lamb, N.W.; Xia, S.; Ding, Z.; Chen, B.; Suarez, M.J.; Meng, T.; Kulkarni, V. Controlled release of dexamethasone sodium phosphate with biodegradable nanoparticles for preventing experimental corneal neovascularization. Nanomed. Nanotechnol. Biol. Med. 2019, 17, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Wagner, V.; Dullaart, A.; Bock, A.-K.; Zweck, A. The emerging nanomedicine landscape. Nat. Biotechnol. 2006, 24, 1211. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.J.; Harris, A.; Gerber, A.; Tobe, L.A.; Amireskandari, A.; Huck, A.; Siesky, B. Nanotechnology and glaucoma: A review of the potential implications of glaucoma nanomedicine. Br. J. Ophthalmol. 2014, 98, 427–431. [Google Scholar] [CrossRef]
- Bucolo, C.; Drago, F.; Salomone, S. Ocular drug delivery: A clue from nanotechnology. Front. Pharmacol. 2012, 3, 188. [Google Scholar] [CrossRef]
- Zarbin, M.A.; Montemagno, C.; Leary, J.F.; Ritch, R. Nanomedicine in ophthalmology: The new frontier. Am. J. Ophthalmol. 2010, 150, 144–162.e142. [Google Scholar] [CrossRef]
- Initiative, U.S.N.N. What’s So Special about the Nanoscale? Available online: https://www.nano.gov/nanotech-101/special (accessed on 1 May 2019).
- Ibrahim, M.M.; Jablonski, M.M. The Impact of R-801 Nanoparticles as a Long Acting Topical Glaucoma Therapy. J. Biomed. Nanotechnol. 2019, 15, 1968–1981. [Google Scholar] [CrossRef]
- Tham, Y.-C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef]
- Gross, R.L.; McMillian, B. Current medical management of glaucoma. In Ophthalmol., 5th ed.; Elsevier: Philadelphia, PA, USA, 2019. [Google Scholar]
- Braunger, B.M.; Fuchshofer, R.; Tamm, E.R. The aqueous humor outflow pathways in glaucoma: A unifying concept of disease mechanisms and causative treatment. Eur. J. Pharm. Biopharm. 2015, 95, 173–181. [Google Scholar] [CrossRef]
- Overby, D.R.; Stamer, W.D.; Johnson, M. The changing paradigm of outflow resistance generation: Towards synergistic models of the JCT and inner wall endothelium. Exp. Eye Res. 2009, 88, 656–670. [Google Scholar] [CrossRef] [Green Version]
- Tamm, E.R. The trabecular meshwork outflow pathways: Structural and functional aspects. Exp. Eye Res. 2009, 88, 648–655. [Google Scholar] [CrossRef]
- Dillinger, A.E.; Guter, M.; Froemel, F.; Weber, G.R.; Perkumas, K.; Stamer, W.D.; Ohlmann, A.; Fuchshofer, R.; Breunig, M. Intracameral Delivery of Layer-by-Layer Coated siRNA Nanoparticles for Glaucoma Therapy. Small 2018, 14, 1803239. [Google Scholar] [CrossRef]
- Pascolini, D.; Mariotti, S.P. Global estimates of visual impairment: 2010. Br. J. Ophthalmol. 2012, 96, 614–618. [Google Scholar] [CrossRef] [PubMed]
- Baughman, R.; Lower, E.; Ingledue, R. Management of ocular sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2012, 29, 26–33. [Google Scholar]
- Weng, Y.; Liu, J.; Jin, S.; Guo, W.; Liang, X.; Hu, Z. Nanotechnology-based strategies for treatment of ocular disease. Acta Pharm. Sin. B 2017, 7, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Xue, C.; Rosen, R.; Jordan, A.; Hu, D.-N. Management of ocular diseases using Lutein and Zeaxanthin: What have we learned from experimental animal studies? J. Ophthalmol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Sacchetti, M.; Lambiase, A. Diagnosis and management of neurotrophic keratitis. Clin. Ophthalmol. (Auckl. Nz) 2014, 8, 571. [Google Scholar]
- Schoenfeld, E.R.; Greene, J.M.; Wu, S.Y.; Leske, M.C. Patterns of adherence to diabetes vision care guidelines: Baseline findings from the Diabetic Retinopathy Awareness Program. Ophthalmology 2001, 108, 563–571. [Google Scholar] [CrossRef]
- Atchison, D.A.; Smith, G.; Smith, G. Optics of the Human Eye; Butterworth-Heinemann Oxford: Oxford, UK, 2000. [Google Scholar]
- Deane, B.; Wyszecki, G. Color in Business, Science and Industry; Wiley: Hoboken, NJ, USA, 1963. [Google Scholar]
- Palczewska, G.; Vinberg, F.; Stremplewski, P.; Bircher, M.P.; Salom, D.; Komar, K.; Zhang, J.; Cascella, M.; Wojtkowski, M.; Kefalov, V.J. Human infrared vision is triggered by two-photon chromophore isomerization. Proc. Natl. Acad. Sci. 2014, 111, E5445–E5454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmer, C. Our strange, important, subconscious light detectors. Discov. Mag.. Retrieved 2012, 02–18. [Google Scholar]
- Mann, I. The Development of the Human Eye; CUP Archive: Cambridge, UK, 1949. [Google Scholar]
- Treuting, P.M.; Wong, R.; Tu, D.C.; Phan, I. Special senses: Eye. In Comparative Anatomy and Histology; Elsevier: Amsterdam, The Netherlands, 2012; pp. 395–418. [Google Scholar]
- Yi, X.-j.; Wang, Y.; Fu-Shin, X.Y. Corneal epithelial tight junctions and their response to lipopolysaccharide challenge. Investig. Ophthalmol. Vis. Sci. 2000, 41, 4093–4100. [Google Scholar]
- Cunha-Vaz, J.; Bernardes, R.; Lobo, C. Blood-retinal barrier. Eur. J. Ophthalmol. 2011, 21, 3–9. [Google Scholar] [CrossRef]
- Furuichi, M.; Chiba, T.; Abe, K.; Kogure, S.; Iijima, H.; Tsukahara, S.; Kashiwagi, K. Cystoid macular edema associated with topical latanoprost in glaucomatous eyes with a normally functioning blood–ocular barrier. J. Glaucoma 2001, 10, 233–236. [Google Scholar] [CrossRef]
- Cunha-Vaz, J.G. The blood-ocular barriers: Past, present, and future. Doc. Ophthalmol. 1997, 93, 149–157. [Google Scholar] [CrossRef]
- Gipson, I.K.; Argueso, P. Role of mucins in the function of the corneal and conjunctival epithelia. Int Rev Cytol 2003, 231, 1–49. [Google Scholar]
- Gaudana, R.; Jwala, J.; Boddu, S.H.; Mitra, A.K. Recent perspectives in ocular drug delivery. Pharm. Res. 2009, 26, 1197. [Google Scholar] [CrossRef]
- Barar, J.; Javadzadeh, A.R.; Omidi, Y. Ocular novel drug delivery: Impacts of membranes and barriers. Expert Opin. Drug Deliv. 2008, 5, 567–581. [Google Scholar] [CrossRef]
- Schwartz, G.F.; Hollander, D.A.; Williams, J.M. Evaluation of eye drop administration technique in patients with glaucoma or ocular hypertension. Curr. Med Res. Opin. 2013, 29, 1515–1522. [Google Scholar] [CrossRef]
- Stamper, R.L. Primary drug treatment for glaucoma: Beta-blockers versus other medications. Surv. Ophthalmol. 2002, 47, 63–67. [Google Scholar] [CrossRef]
- Masini, E.; Carta, F.; Scozzafava, A.; Supuran, C.T. Antiglaucoma carbonic anhydrase inhibitors: A patent review. Expert Opin. Ther. Pat. 2013, 23, 705–716. [Google Scholar] [CrossRef] [PubMed]
- Burke, J.A. Combinations of selective alpha-adrenergic agonists and antagonists useful in lowering intraocular pressure. US Patent 5,281,591, 1994. [Google Scholar]
- Medeiros, F.A.; Weinreb, R.N. Medical backgrounders: Glaucoma. Drugs Today (Barc) 2002, 38, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Goyal, G.; Garg, T.; Rath, G.; Goyal, A.K. Current nanotechnological strategies for treating glaucoma. Crit. Rev. ™ Ther. Drug Carr. Syst. 2014, 31. [Google Scholar] [CrossRef]
- Pita-Thomas, D.W.; Goldberg, J.L. Nanotechnology and glaucoma: Little particles for a big disease. Curr. Opin. Ophthalmol. 2013, 24, 130–135. [Google Scholar] [CrossRef]
- Salama, H.A.; Ghorab, M.; Mahmoud, A.A.; Hady, M.A. PLGA nanoparticles as subconjunctival injection for management of glaucoma. Aaps Pharmscitech 2017, 18, 2517–2528. [Google Scholar] [CrossRef]
- Morsi, N.; Ibrahim, M.; Refai, H.; El Sorogy, H. Nanoemulsion-based electrolyte triggered in situ gel for ocular delivery of acetazolamide. Eur. J. Pharm. Sci. 2017, 104, 302–314. [Google Scholar] [CrossRef]
- Kim, H.-J.; Zhang, K.; Moore, L.; Ho, D. Diamond nanogel-embedded contact lenses mediate lysozyme-dependent therapeutic release. Acs Nano 2014, 8, 2998–3005. [Google Scholar] [CrossRef]
- Tuomela, A.; Liu, P.; Puranen, J.; Rönkkö, S.; Laaksonen, T.; Kalesnykas, G.; Oksala, O.; Ilkka, J.; Laru, J.; Järvinen, K. Brinzolamide nanocrystal formulations for ophthalmic delivery: Reduction of elevated intraocular pressure in vivo. Int. J. Pharm. 2014, 467, 34–41. [Google Scholar] [CrossRef]
- Natarajan, J.V.; Darwitan, A.; Barathi, V.A.; Ang, M.; Htoon, H.M.; Boey, F.; Tam, K.C.; Wong, T.T.; Venkatraman, S.S. Sustained drug release in nanomedicine: A long-acting nanocarrier-based formulation for glaucoma. Acs Nano 2014, 8, 419–429. [Google Scholar] [CrossRef]
- Kambhampati, S.P.; Kannan, R.M. Dendrimer nanoparticles for ocular drug delivery. J. Ocul. Pharmacol. Ther. 2013, 29, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Aller, M.; Guinchard, S.; Guillarme, D.; Pupier, M.; Jeannerat, D.; Rivara-Minten, E.; Veuthey, J.-L.; Gurny, R. New prostaglandin analog formulation for glaucoma treatment containing cyclodextrins for improved stability, solubility and ocular tolerance. Eur. J. Pharm. Biopharm. 2015, 95, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Cardigos, J.; Ferreira, Q.; Crisóstomo, S.; Moura-Coelho, N.; Cunha, J.P.; Pinto, L.A.; Ferreira, J.T. Nanotechnology-Ocular Devices for Glaucoma Treatment: A Literature Review. Curr. Eye Res. 2019, 44, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Jones, L.; Gu, F.X. Nanomaterials for ocular drug delivery. Macromol. Biosci. 2012, 12, 608–620. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.; Li, H.; Jin, Z.; Huang, L.; Wang, F.; Zhou, Y.; Liu, Y.; Jiang, C.; Oswald, J.; Wu, J. TPGS modified nanoliposomes as an effective ocular delivery system to treat glaucoma. Int. J. Pharm. 2018, 553, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Wadhwa, S.; Paliwal, R.; Paliwal, S.R.; Vyas, S. Hyaluronic acid modified chitosan nanoparticles for effective management of glaucoma: Development, characterization, and evaluation. J. Drug Target. 2010, 18, 292–302. [Google Scholar] [CrossRef]
- Fedorchak, M.V.; Conner, I.P.; Medina, C.A.; Wingard, J.B.; Schuman, J.S.; Little, S.R. 28-day intraocular pressure reduction with a single dose of brimonidine tartrate-loaded microspheres. Exp. Eye Res. 2014, 125, 210–216. [Google Scholar] [CrossRef]
- Liu, H.; Wan, J.; Hughes, P.M. Microsphere drug delivery system for sustained intraocular release. US Patent 9,504,653, 2016. [Google Scholar]
- Bertram, J.P.; Saluja, S.S.; McKain, J.; Lavik, E.B. Sustained delivery of timolol maleate from poly (lactic-co-glycolic acid)/poly (lactic acid) microspheres for over 3 months. J. Microencapsul. 2009, 26, 18–26. [Google Scholar] [CrossRef]
- Jung, H.J.; Abou-Jaoude, M.; Carbia, B.E.; Plummer, C.; Chauhan, A. Glaucoma therapy by extended release of timolol from nanoparticle loaded silicone-hydrogel contact lenses. J. Control. Release 2013, 165, 82–89. [Google Scholar] [CrossRef]
- Peng, C.-C.; Burke, M.T.; Carbia, B.E.; Plummer, C.; Chauhan, A. Extended drug delivery by contact lenses for glaucoma therapy. J. Control. Release 2012, 162, 152–158. [Google Scholar] [CrossRef]
- Garg, T.; Malik, B.; Rath, G.; Goyal, A.K. Development and characterization of nano-fiber patch for the treatment of glaucoma. Eur. J. Pharm. Sci. 2014, 53, 10–16. [Google Scholar]
- Natarajan, J.V.; Ang, M.; Darwitan, A.; Chattopadhyay, S.; Wong, T.T.; Venkatraman, S.S. Nanomedicine for glaucoma: Liposomes provide sustained release of latanoprost in the eye. Int. J. Nanomed. 2012, 7, 123. [Google Scholar]
- Wong, T.T.; Novack, G.D.; Natarajan, J.V.; Ho, C.L.; Htoon, H.M.; Venkatraman, S.S. Nanomedicine for glaucoma: Sustained release latanoprost offers a new therapeutic option with substantial benefits over eyedrops. Drug Deliv. Transl. Res. 2014, 4, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Vold, S.; Ahmed, I.I.K.; Craven, E.R.; Mattox, C.; Stamper, R.; Packer, M.; Brown, R.H.; Ianchulev, T.; Group, C.S. Two-year COMPASS trial results: Supraciliary microstenting with phacoemulsification in patients with open-angle glaucoma and cataracts. Ophthalmology 2016, 123, 2103–2112. [Google Scholar] [CrossRef] [PubMed]
- Sheybani, A.; Dick, H.B.; Ahmed, I.I. Early clinical results of a novel ab interno gel stent for the surgical treatment of open-angle glaucoma. J. Glaucoma 2016, 25, e691–e696. [Google Scholar] [CrossRef] [PubMed]
- Loewen, R.T.; Roy, P.; Parikh, H.A.; Dang, Y.; Schuman, J.S.; Loewen, N.A. Impact of a glaucoma severity index on results of trabectome surgery: Larger pressure reduction in more severe glaucoma. Plos One 2016, 11, e0151926. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Li, J.; Wu, L.; Wang, B.; Wang, Z.; Xu, Q.; Xin, H. Ophthalmic delivery of brinzolamide by liquid crystalline nanoparticles: In vitro and in vivo evaluation. Aaps Pharmscitech 2013, 14, 1063–1071. [Google Scholar] [CrossRef]
- Han, Q.; Wang, Y.; Li, X.; Peng, R.; Li, A.; Qian, Z.; Yu, L. Effects of bevacizumab loaded PEG-PCL-PEG hydrogel intracameral application on intraocular pressure after glaucoma filtration surgery. J. Mater. Sci. Mater. Med. 2015, 26, 225. [Google Scholar] [CrossRef]
- Liao, Y.-T.; Lee, C.-H.; Chen, S.-T.; Lai, J.-Y.; Wu, K.C.-W. Gelatin-functionalized mesoporous silica nanoparticles with sustained release properties for intracameral pharmacotherapy of glaucoma. J. Mater. Chem. B 2017, 5, 7008–7013. [Google Scholar] [CrossRef]
- Hassan, D.; Abdelmonem, R.; Abdellatif, M. Formulation and Characterization of Carvedilol Leciplex for Glaucoma Treatment: In-Vitro, Ex-Vivo and In-Vivo Study. Pharmaceutics 2018, 10, 197. [Google Scholar] [CrossRef]
- Szumny, D.; Szeląg, A. The influence of new beta-adrenolytics nebivolol and carvedilol on intraocular pressure and iris blood flow in rabbits. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 252, 917–923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodward, D.F.; Gil, D.W. The inflow and outflow of anti-glaucoma drugs. Trends Pharmacol. Sci. 2004, 25, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Tian, S.; Tao, Q.; Zhao, Y.; Gui, R.; Yang, F.; Zang, L.; Chen, Y.; Ping, Q.; Hou, D. Montmorillonite/chitosan nanoparticles as a novel controlled-release topical ophthalmic delivery system for the treatment of glaucoma. Int. J. Nanomed. 2018, 13, 3975. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Gan, L.; Zhu, C.; Dong, Y.; Liu, J.; Gan, Y. Cationic core–shell liponanoparticles for ocular gene delivery. Biomaterials 2012, 33, 7621–7630. [Google Scholar] [CrossRef] [PubMed]
- Yuan, X.; Marcano, D.C.; Shin, C.S.; Hua, X.; Isenhart, L.C.; Pflugfelder, S.C.; Acharya, G. Ocular drug delivery nanowafer with enhanced therapeutic efficacy. Acs Nano 2015, 9, 1749–1758. [Google Scholar] [CrossRef]
- Shi, S.; Zhang, Z.; Luo, Z.; Yu, J.; Liang, R.; Li, X.; Chen, H. Chitosan grafted methoxy poly (ethylene glycol)-poly (ε-caprolactone) nanosuspension for ocular delivery of hydrophobic diclofenac. Sci. Rep. 2015, 5, 11337. [Google Scholar] [CrossRef]
- Colin, J. Ganciclovir ophthalmic gel, 0.15%: A valuable tool for treating ocular herpes. Clin. Ophthalmol. (Auckl. Nz) 2007, 1, 441. [Google Scholar]
- Foster, C.S. Ganciclovir gel—a new topical treatment for herpetic keratitis. Ganciclovir Gel—A New Top. Treat. Herpetic Keratitis 2013. [Google Scholar] [CrossRef]
- Kaufman, H.E.; Haw, W.H. Ganciclovir ophthalmic gel 0.15%: Safety and efficacy of a new treatment for herpes simplex keratitis. Curr. Eye Res. 2012, 37, 654–660. [Google Scholar] [CrossRef]
- Chou, T.Y.; Hong, B.Y. Ganciclovir ophthalmic gel 0.15% for the treatment of acute herpetic keratitis: Background, effectiveness, tolerability, safety, and future applications. Ther. Clin. Risk Manag. 2014, 10, 665. [Google Scholar] [CrossRef]
- Vega, E.; Egea, M.; Valls, O.; Espina, M.; Garcia, M. Flurbiprofen loaded biodegradable nanoparticles for ophtalmic administration. J. Pharm. Sci. 2006, 95, 2393–2405. [Google Scholar] [CrossRef]
- Pan, Q.; Xu, Q.; Boylan, N.J.; Lamb, N.W.; Emmert, D.G.; Yang, J.-C.; Tang, L.; Heflin, T.; Alwadani, S.; Eberhart, C.G. Corticosteroid-loaded biodegradable nanoparticles for prevention of corneal allograft rejection in rats. J. Control. Release 2015, 201, 32–40. [Google Scholar] [CrossRef]
- Zhang, W.; Wang, Y.; Lee, B.T.K.; Liu, C.; Wei, G.; Lu, W. A novel nanoscale-dispersed eye ointment for the treatment of dry eye disease. Nanotechnology 2014, 25, 125101. [Google Scholar] [CrossRef]
- Pignatello, R.; Bucolo, C.; Spedalieri, G.; Maltese, A.; Puglisi, G. Flurbiprofen-loaded acrylate polymer nanosuspensions for ophthalmic application. Biomaterials 2002, 23, 3247–3255. [Google Scholar] [CrossRef]
- Zhang, Z.; He, Z.; Liang, R.; Ma, Y.; Huang, W.; Jiang, R.; Shi, S.; Chen, H.; Li, X. Fabrication of a micellar supramolecular hydrogel for ocular drug delivery. Biomacromolecules 2016, 17, 798–807. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, S. Topical use of Coenzyme Q10-loaded liposomes coated with trimethyl chitosan: Tolerance, precorneal retention and anti-cataract effect. Int. J. Pharm. 2009, 372, 66–75. [Google Scholar] [CrossRef]
- Kao, H.J.; Lo, Y.L.; Lin, H.R.; Yu, S.P. Characterization of pilocarpine-loaded chitosan/Carbopol nanoparticles. J. Pharm. Pharmacol. 2006, 58, 179–186. [Google Scholar] [CrossRef]
- Tyagi, P.; Barros, M.; Stansbury, J.W.; Kompella, U.B. Light-activated, in situ forming gel for sustained suprachoroidal delivery of bevacizumab. Mol. Pharm. 2013, 10, 2858–2867. [Google Scholar] [CrossRef]
- Shedden, A.H.; Laurence, J.; Barrish, A.; Olah, T.V. Plasma timolol concentrations of timolol maleate: Timolol gel-forming solution (TIMOPTIC-XE®) once daily versus timolol maleate ophthalmic solution twice daily. Doc. Ophthalmol. 2001, 103, 73–79. [Google Scholar] [CrossRef]
- ElShaer, A.; Mustafa, S.; Kasar, M.; Thapa, S.; Ghatora, B.; Alany, R. Nanoparticle-laden contact lens for controlled ocular delivery of prednisolone: Formulation optimization using statistical experimental design. Pharmaceutics 2016, 8, 14. [Google Scholar] [CrossRef]
- Chen, C.-W.; Yeh, M.-K.; Shiau, C.-Y.; Chiang, C.-H.; Lu, D.-W. Efficient downregulation of VEGF in retinal pigment epithelial cells by integrin ligand-labeled liposome-mediated siRNA delivery. Int. J. Nanomed. 2013, 8, 2613. [Google Scholar]
- Chen, C.-W.; Lu, D.-W.; Yeh, M.-K.; Shiau, C.-Y.; Chiang, C.-H. Novel RGD-lipid conjugate-modified liposomes for enhancing siRNA delivery in human retinal pigment epithelial cells. Int. J. Nanomed. 2011, 6, 2567. [Google Scholar] [CrossRef]
- Mastorakos, P.; Kambhampati, S.P.; Mishra, M.K.; Wu, T.; Song, E.; Hanes, J.; Kannan, R.M. Hydroxyl PAMAM dendrimer-based gene vectors for transgene delivery to human retinal pigment epithelial cells. Nanoscale 2015, 7, 3845–3856. [Google Scholar] [CrossRef]
- Read, S.P.; Cashman, S.M.; Kumar-Singh, R. POD nanoparticles expressing GDNF provide structural and functional rescue of light-induced retinal degeneration in an adult mouse. Mol. Ther. 2010, 18, 1917–1926. [Google Scholar] [CrossRef]
- Rajala, A.; Wang, Y.; Zhu, Y.; Ranjo-Bishop, M.; Ma, J.-X.; Mao, C.; Rajala, R.V. Nanoparticle-assisted targeted delivery of eye-specific genes to eyes significantly improves the vision of blind mice in vivo. Nano Lett. 2014, 14, 5257–5263. [Google Scholar] [CrossRef]
- Mitrev, P. Glaucoma drainage device implant. US Patent 6,589,203, 2003. [Google Scholar]
- Coleman, A.L.; Hill, R.; Wilson, M.R.; Choplin, N.; Kotas-Neumann, R.; Tam, M.; Bacharach, J.; Panek, W.C. Initial clinical experience with the Ahmed glaucoma valve implant. Am. J. Ophthalmol. 1995, 120, 23–31. [Google Scholar] [CrossRef]
- Syed, H.M.; Law, S.K.; Nam, S.H.; Li, G.; Caprioli, J.; Coleman, A. Baerveldt-350 implant versus Ahmed valve for refractory glaucoma: A case-controlled comparison. J. Glaucoma 2004, 13, 38–45. [Google Scholar] [CrossRef]
- Yalvac, I.; Eksioglu, U.; Satana, B.; Duman, S. Long-term results of Ahmed glaucoma valve and Molteno implant in neovascular glaucoma. Eye 2007, 21, 65. [Google Scholar] [CrossRef]
- Hong, C.-H.; Arosemena, A.; Zurakowski, D.; Ayyala, R.S. Glaucoma drainage devices: A systematic literature review and current controversies. Surv. Ophthalmol. 2005, 50, 48–60. [Google Scholar] [CrossRef]
- Alvarado, J.A.; Hollander, D.A.; Juster, R.P.; Lee, L.C. Ahmed valve implantation with adjunctive mitomycin C and 5-fluorouracil: Long-term outcomes. Am. J. Ophthalmol. 2008, 146, 276–284.e272. [Google Scholar] [CrossRef]
- Ponnusamy, T.; Yu, H.; John, V.T.; Ayyala, R.S.; Blake, D.A. A novel antiproliferative drug coating for glaucoma drainage devices. J. Glaucoma 2014, 23, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Pan, T.; Brown, J.D.; Ziaie, B. An artificial nano-drainage implant (ANDI) for glaucoma treatment. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 3174–3177. [Google Scholar]
- Paschalis, E.I.; Chodosh, J.; Sperling, R.A.; Salvador-Culla, B.; Dohlman, C. A novel implantable glaucoma valve using ferrofluid. Plos One 2013, 8, e67404. [Google Scholar] [CrossRef] [PubMed]
- Maleki, T.; Chitnis, G.; Park, J.H.; Cantor, L.B.; Ziaie, B. Biodegradable microfabricated plug-filters for glaucoma drainage devices. Ieee Trans. Biomed. Eng. 2012, 59, 1507–1513. [Google Scholar] [CrossRef]
- Harake, R.S.; Ding, Y.; Brown, J.D.; Pan, T. Design, fabrication, and in vitro testing of an anti-biofouling glaucoma micro-shunt. Ann. Biomed. Eng. 2015, 43, 2394–2405. [Google Scholar] [CrossRef]
- Abegão Pinto, L.; Willekens, K.; Van Keer, K.; Shibesh, A.; Molenberghs, G.; Vandewalle, E.; Stalmans, I. Ocular blood flow in glaucoma–the Leuven Eye Study. Acta Ophthalmol. 2016, 94, 592–598. [Google Scholar] [CrossRef]
- Leonardi, M.; Pitchon, E.M.; Bertsch, A.; Renaud, P.; Mermoud, A. Wireless contact lens sensor for intraocular pressure monitoring: Assessment on enucleated pig eyes. Acta Ophthalmol. 2009, 87, 433–437. [Google Scholar] [CrossRef]
- Faschinger, C.; Mossböck, G. Continuous 24 h monitoring of changes in intraocular pressure with the wireless contact lens sensor Triggerfish™. First results in patients. Der Ophthalmol. Z. Der Dtsch. Ophthalmol. Ges. 2010, 107, 918–922. [Google Scholar] [CrossRef]
- Lee, G.A.; Khaw, P.T.; Ficker, L.A.; Shah, P. The corneal thickness and intraocular pressure story: Where are we now? Clin. Exp. Ophthalmol. 2002, 30, 334–337. [Google Scholar] [CrossRef]
- Graham, S.; Drance, S. Nocturnal hypotension: Role in glaucoma progression. Surv. Ophthalmol. 1999, 43, S10–S16. [Google Scholar] [CrossRef]
- Irazoqui, P.P.; Chow, E.Y.; Chappell, W.J.; Yang, C.-l.; Ziaie, B. Intra-occular pressure sensor. U.S. Patent 5,281,591, 2013. [Google Scholar]
- Tanihara, H.; Inoue, T.; Yamamoto, T.; Kuwayama, Y.; Abe, H.; Suganami, H.; Araie, M.; Group, K.C.S. Intra-ocular pressure-lowering effects of a Rho kinase inhibitor, ripasudil (K-115), over 24 hours in primary open-angle glaucoma and ocular hypertension: A randomized, open-label, crossover study. Acta Ophthalmol. 2015, 93, e254–e260. [Google Scholar] [CrossRef]
- Chen, G.-Z.; Chan, I.-S.; Leung, L.K.; Lam, D.C. Soft wearable contact lens sensor for continuous intraocular pressure monitoring. Med Eng. Phys. 2014, 36, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- Rizq, R.N.; Choi, W.-H.; Eilers, D.; Wright, M.M.; Ziaie, B. Intraocular pressure measurement at the choroid surface: A feasibility study with implications for implantable microsystems. Br. J. Ophthalmol. 2001, 85, 868–871. [Google Scholar] [CrossRef] [PubMed]
- Dresher, R.P.; Irazoqui, P.P. A compact nanopower low output impedance CMOS operational amplifier for wireless intraocular pressure recordings. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 22–26 August 2007, Lyon, France; pp. 6055–6058.
- Chen, P.-J.; Rodger, D.C.; Saati, S.; Humayun, M.S.; Tai, Y.-C. Microfabricated implantable parylene-based wireless passive intraocular pressure sensors. J. Microelectromechanical Syst. 2008, 17, 1342–1351. [Google Scholar] [CrossRef]
- Chen, P.-J.; Rodger, D.C.; Humayun, M.S.; Tai, Y.-C. Unpowered spiral-tube parylene pressure sensor for intraocular pressure sensing. Sens. Actuators A Phys. 2006, 127, 276–282. [Google Scholar] [CrossRef]
- Chen, P.-J.; Rodger, D.C.; Agrawal, R.; Saati, S.; Meng, E.; Varma, R.; Humayun, M.S.; Tai, Y.-C. Implantable micromechanical parylene-based pressure sensors for unpowered intraocular pressure sensing. J. Micromechanics Microengineering 2007, 17, 1931. [Google Scholar] [CrossRef]
- Phan, A.; Truong, P.; Camp, A.; Stewart, K.; Suen, B.; Weinreb, R.N.; Talke, F.E. A Wireless Handheld Pressure Measurement System for in vivo Monitoring of Intraocular Pressure in Rabbits. Ieee Trans. Biomed. Eng. 2019. [Google Scholar] [CrossRef]
- Zilly, J.; Buhmann, J.M.; Mahapatra, D. Glaucoma detection using entropy sampling and ensemble learning for automatic optic cup and disc segmentation. Comput. Med Imaging Graph. 2017, 55, 28–41. [Google Scholar] [CrossRef]
- Morgan, J.E.; Sheen, N.J.L.; North, R.V.; Choong, Y.; Ansari, E. Digital imaging of the optic nerve head: Monoscopic and stereoscopic analysis. Br. J. Ophthalmol. 2005, 89, 879–884. [Google Scholar] [CrossRef]
- Fallon, M.; Valero, O.; Pazos, M.; Anton, A. Diagnostic accuracy of imaging devices in glaucoma: A meta-analysis. Surv. Ophthalmol. 2017, 62, 446–461. [Google Scholar] [CrossRef] [Green Version]
- Jia, Y.; Wei, E.; Wang, X.; Zhang, X.; Morrison, J.C.; Parikh, M.; Lombardi, L.H.; Gattey, D.M.; Armour, R.L.; Edmunds, B. Optical coherence tomography angiography of optic disc perfusion in glaucoma. Ophthalmology 2014, 121, 1322–1332. [Google Scholar] [CrossRef]
- Liu, L.; Jia, Y.; Takusagawa, H.L.; Pechauer, A.D.; Edmunds, B.; Lombardi, L.; Davis, E.; Morrison, J.C.; Huang, D. Optical coherence tomography angiography of the peripapillary retina in glaucoma. Jama Ophthalmol. 2015, 133, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Jiang, C.; Ko, T.; Kong, X.; Yu, X.; Min, W.; Shi, G.; Sun, X. Correlation between optic disc perfusion and glaucomatous severity in patients with open-angle glaucoma: An optical coherence tomography angiography study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- Bussel, I.I.; Wollstein, G.; Schuman, J.S. OCT for glaucoma diagnosis, screening and detection of glaucoma progression. Br. J. Ophthalmol. 2014, 98, ii15–ii19. [Google Scholar] [CrossRef] [PubMed]
- Strouthidis, N.G.; Scott, A.; Peter, N.M.; Garway-Heath, D.F. Optic disc and visual field progression in ocular hypertensive subjects: Detection rates, specificity, and agreement. Investig. Ophthalmol. Vis. Sci. 2006, 47, 2904–2910. [Google Scholar] [CrossRef]
- Chiang, B.; Kim, Y.; Doty, A.; Grossniklaus, H.; Schwendeman, S.; Prausnitz, M. Sustained reduction of intraocular pressure by supraciliary delivery of brimonidine-loaded poly (lactic acid) microspheres for the treatment of glaucoma. J. Control. Release 2016, 228, 48–57. [Google Scholar] [CrossRef]
- Chandrawati, R.; Chang, J.Y.; Reina-Torres, E.; Jumeaux, C.; Sherwood, J.M.; Stamer, W.D.; Zelikin, A.N.; Overby, D.R.; Stevens, M.M. Localized and controlled delivery of nitric oxide to the conventional outflow pathway via enzyme biocatalysis: Toward therapy for glaucoma. Adv. Mater. 2017, 29, 1604932. [Google Scholar] [CrossRef]
- Tam, A.L.; Gupta, N.; Zhang, Z.; Yücel, Y.H. Quantum dots trace lymphatic drainage from the mouse eye. Nanotechnology 2011, 22, 425101. [Google Scholar] [CrossRef]
- Roubeix, C.; Godefroy, D.; Mias, C.; Sapienza, A.; Riancho, L.; Degardin, J.; Fradot, V.; Ivkovic, I.; Picaud, S.; Sennlaub, F. Intraocular pressure reduction and neuroprotection conferred by bone marrow-derived mesenchymal stem cells in an animal model of glaucoma. Stem Cell Res. Ther. 2015, 6, 177. [Google Scholar] [CrossRef]
- Arcinue, C.A.; Cerón, O.M.; Foster, C.S. A comparison between the fluocinolone acetonide (Retisert) and dexamethasone (Ozurdex) intravitreal implants in uveitis. J. Ocul. Pharmacol. Ther. 2013, 29, 501–507. [Google Scholar] [CrossRef]
- G Schwartz, S.; W Flynn, H. Fluocinolone acetonide implantable device for diabetic retinopathy. Curr. Pharm. Biotechnol. 2011, 12, 347–351. [Google Scholar] [CrossRef]
- Haller, J.A.; Bandello, F.; Belfort, R., Jr.; Blumenkranz, M.S.; Gillies, M.; Heier, J.; Loewenstein, A.; Yoon, Y.-H.; Jacques, M.-L.; Jiao, J. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology 2010, 117, 1134–1146.e1133. [Google Scholar] [CrossRef] [PubMed]
- Zahid, S.; Musch, D.C.; Niziol, L.M.; Lichter, P.R.; Group, C.I.G.T.S. Risk of endophthalmitis and other long-term complications of trabeculectomy in the Collaborative Initial Glaucoma Treatment Study (CIGTS). Am. J. Ophthalmol. 2013, 155, 674–680.e671. [Google Scholar] [CrossRef] [PubMed]
- Kauper, K.; McGovern, C.; Sherman, S.; Heatherton, P.; Rapoza, R.; Stabila, P.; Dean, B.; Lee, A.; Borges, S.; Bouchard, B. Two-year intraocular delivery of ciliary neurotrophic factor by encapsulated cell technology implants in patients with chronic retinal degenerative diseases. Investig. Ophthalmol. Vis. Sci. 2012, 53, 7484–7491. [Google Scholar] [CrossRef] [PubMed]
- Thanos, C.G.; Bell, W.J.; O’Rourke, P.; Kauper, K.; Sherman, S.; Stabila, P.; Tao, W. Sustained secretion of ciliary neurotrophic factor to the vitreous, using the encapsulated cell therapy-based NT-501 intraocular device. Tissue Eng. 2004, 10, 1617–1622. [Google Scholar] [CrossRef]
- Birch, D.G.; Weleber, R.G.; Duncan, J.L.; Jaffe, G.J.; Tao, W.; Groups, C.N.F.R.P.S. Randomized trial of ciliary neurotrophic factor delivered by encapsulated cell intraocular implants for retinitis pigmentosa. Am. J. Ophthalmol. 2013, 156, 283–292.e281. [Google Scholar] [CrossRef]
- Lavik, E.; Kuehn, M.; Kwon, Y. Novel drug delivery systems for glaucoma. Eye 2011, 25, 578. [Google Scholar] [CrossRef]
- Norell, S.E.; Granström, P. Self-medication with pilocarpine among outpatients in a glaucoma clinic. Br. J. Ophthalmol. 1980, 64, 137–141. [Google Scholar] [CrossRef]
- Saati, S.; Lo, R.; Li, P.-Y.; Meng, E.; Varma, R.; Humayun, M.S. Mini drug pump for ophthalmic use. Curr. Eye Res. 2010, 35, 192–201. [Google Scholar] [CrossRef]
- Lo, R.; Li, P.-Y.; Saati, S.; Agrawal, R.N.; Humayun, M.S.; Meng, E. A passive MEMS drug delivery pump for treatment of ocular diseases. Biomed. Microdevices 2009, 11, 959. [Google Scholar] [CrossRef]
- Saati, S.; Lo, R.; Li, P.-Y.; Meng, E.; Varma, R.; Humayun, M.S. Mini drug pump for ophthalmic use. Trans. Am. Ophthalmol. Soc. 2009, 107, 60. [Google Scholar] [CrossRef]
- Staples, M.; Daniel, K.; Cima, M.J.; Langer, R. Application of micro-and nano-electromechanical devices to drug delivery. Pharm. Res. 2006, 23, 847–863. [Google Scholar] [CrossRef] [PubMed]
- de Juan, E., Jr.; Boyd, S.; Deem, M.E.; Gifford III, H.S.; Rosenman, D. Glaucoma treatment device. US Patent 2014. [Google Scholar]
- Chow, E.Y.; Chlebowski, A.L.; Irazoqui, P.P. A miniature-implantable RF-wireless active glaucoma intraocular pressure monitor. Ieee Trans. Biomed. Circuits Syst. 2010, 4, 340–349. [Google Scholar] [CrossRef] [PubMed]
- Molaei, A.; Karamzadeh, V.; Safi, S.; Esfandiari, H.; Dargahi, J.; Khosravi, M.A. Upcoming methods and specifications of continuous intraocular pressure monitoring systems for glaucoma. J. Ophthalmic Vis. Res. 2018, 13, 66. [Google Scholar] [CrossRef]
- Davis, B.M.; Crawley, L.; Pahlitzsch, M.; Javaid, F.; Cordeiro, M.F. Glaucoma: The retina and beyond. Acta Neuropathol. 2016, 132, 807–826. [Google Scholar] [CrossRef]
- Roizenblatt, R.; Weiland, J.D.; Carcieri, S.; Qiu, G.; Behrend, M.; Humayun, M.S.; Chow, R.H. Nanobiolistic delivery of indicators to the living mouse retina. J. Neurosci. Methods 2006, 153, 154–161. [Google Scholar] [CrossRef]
- Anderson, S.A.; Rader, R.K.; Westlin, W.F.; Null, C.; Jackson, D.; Lanza, G.M.; Wickline, S.A.; Kotyk, J.J. Magnetic resonance contrast enhancement of neovasculature with αvβ3-targeted nanoparticles. Magn. Reson. Med. Off. J. Int. Soc. Magn. Reson. Med. 2000, 44, 433–439. [Google Scholar] [CrossRef]
- Cang, H.; Sun, T.; Li, Z.-Y.; Chen, J.; Wiley, B.J.; Xia, Y.; Li, X. Gold nanocages as contrast agents for spectroscopic optical coherence tomography. Opt. Lett. 2005, 30, 3048–3050. [Google Scholar] [CrossRef]
- Akerman, M.; Chan, W.; Laakkonen, P.; Bhatia, S.; Ruoslahti, E. Nanocrystal targeting in vivo Proc Natl Acad Sci USA 99: 12617–12621. Find This Artic. Online 2002. [Google Scholar]
- Schachar, R.A.; Chen, W.; Woo, B.K.; Pierscionek, B.K.; Zhang, X.; Ma, L. Diffusion of nanoparticles into the capsule and cortex of a crystalline lens. Nanotechnology 2007, 19, 025102. [Google Scholar] [CrossRef]
- Saccà, S.C.; Pascotto, A.; Camicione, P.; Capris, P.; Izzotti, A. Oxidative DNA damage in the human trabecular meshwork: Clinical correlation in patients with primary open-angle glaucoma. Arch. Ophthalmol. 2005, 123, 458–463. [Google Scholar] [CrossRef] [PubMed]
- Acott, T.S.; Kelley, M.J. Extracellular matrix in the trabecular meshwork. Exp. Eye Res. 2008, 86, 543–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vranka, J.A.; Kelley, M.J.; Acott, T.S.; Keller, K.E. Extracellular matrix in the trabecular meshwork: Intraocular pressure regulation and dysregulation in glaucoma. Exp. Eye Res. 2015, 133, 112–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borrás, T. Advances in glaucoma treatment and management: Gene therapy. Investig. Ophthalmol. Vis. Sci. 2012, 53, 2506–2510. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, E.; Nakajima, T.; Minagawa, Y.; Shearer, T.R.; Azuma, M. Contribution of ROCK in contraction of trabecular meshwork: Proposed mechanism for regulating aqueous outflow in monkey and human eyes. J. Pharm. Sci. 2005, 94, 701–708. [Google Scholar] [CrossRef] [PubMed]
- De Groef, L.; Van Hove, I.; Dekeyster, E.; Stalmans, I.; Moons, L. MMPs in the trabecular meshwork: Promising targets for future glaucoma therapies? Investig. Ophthalmol. Vis. Sci. 2013, 54, 7756–7763. [Google Scholar] [CrossRef] [PubMed]
- Gerometta, R.; Spiga, M.-G.; Borrás, T.; Candia, O.A. Treatment of sheep steroid–induced ocular hypertension with a glucocorticoid-inducible MMP1 gene therapy virus. Investig. Ophthalmol. Vis. Sci. 2010, 51, 3042–3048. [Google Scholar] [CrossRef]
- Du, Y.; Yun, H.; Yang, E.; Schuman, J.S. Stem cells from trabecular meshwork home to TM tissue in vivo. Investig. Ophthalmol. Vis. Sci. 2013, 54, 1450–1459. [Google Scholar] [CrossRef]
- Dautriche, C.N.; Szymanski, D.; Kerr, M.; Torrejon, K.Y.; Bergkvist, M.; Xie, Y.; Danias, J.; Stamer, W.; Sharfstein, S.T. A biomimetic Schlemm’s canal inner wall: A model to study outflow physiology, glaucoma pathology and high-throughput drug screening. Biomaterials 2015, 65, 86–92. [Google Scholar] [CrossRef]
- Torrejon, K.Y.; Pu, D.; Bergkvist, M.; Danias, J.; Sharfstein, S.T.; Xie, Y. Recreating a human trabecular meshwork outflow system on microfabricated porous structures. Biotechnol. Bioeng. 2013, 110, 3205–3218. [Google Scholar] [CrossRef]
- Bergkvist, M.; Brenner, S.; Danias, I.; Sharfstein, S.; Xie, Y.; Gracias, A.; Torrejon, K.Y. Bioengineered human trabecular meshwork for biological applications. U.S. Patent 9,506,907, 2016. [Google Scholar]
- Xie, Y.; Torrejon, K.; Sharfstein, S.; Bergkvist, M.; Danias, J.; Dautriche, C.N. Use of vascular cells to create the conventional outflow tract. US Patent 16/044,806, 2019. [Google Scholar]
- Snider, E.; Kubelick, K.; Tweed, K.; Kim, R.; Li, Y.; Gao, K.; Read, A.; Emelianov, S.; Ethier, C. Improving Stem Cell Delivery to the Trabecular Meshwork Using Magnetic Nanoparticles. Sci. Rep. 2018, 8, 12251. [Google Scholar] [CrossRef] [PubMed]
- Ikuta, Y.; Aoyagi, S.; Tanaka, Y.; Sato, K.; Inada, S.; Koseki, Y.; Onodera, T.; Oikawa, H.; Kasai, H. Creation of nano eye-drops and effective drug delivery to the interior of the eye. Sci. Rep. 2017, 7, 44229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alqawlaq, S.; Huzil, J.T.; Ivanova, M.V.; Foldvari, M. Challenges in neuroprotective nanomedicine development: Progress towards noninvasive gene therapy of glaucoma. Nanomedicine 2012, 7, 1067–1083. [Google Scholar] [CrossRef] [PubMed]
- Yadav, K.S.; Rajpurohit, R.; Sharma, S. Glaucoma: Current treatment and impact of advanced drug delivery systems. Life Sci. 2019. [Google Scholar] [CrossRef] [PubMed]
- Prow, T.W. Toxicity of nanomaterials to the eye. Wiley Interdisciplinary Rev. Nanomed. Nanobiotechnol. 2010, 2, 317–333. [Google Scholar] [CrossRef] [PubMed]
- Sutariya, V.B.; Groshev, A.; Dave, V.S.; Saluja, H.; Bhatia, D.; Sadana, P.; Pathak, Y. Nanoparticles and human health: A review of epidemiological studies. Biointeractions Nanomater. 2014, 175–208. [Google Scholar]
- Albanese, A.; Tang, P.S.; Chan, W.C. The effect of nanoparticle size, shape, and surface chemistry on biological systems. Annu. Rev. Biomed. Eng. 2012, 14, 1–16. [Google Scholar] [CrossRef]
- del Pozo-Rodriguez, A.; Delgado, D.; Solinis, M.; Gascon, A.; Pedraz, J. Solid lipid nanoparticles for retinal gene therapy: Transfection and intracellular trafficking in RPE cells. Int. J. Pharm. 2008, 360, 177–183. [Google Scholar] [CrossRef]
- Calvo, P.; Vila-Jato, J.L.; Alonso, M.J. Comparative in vitro evaluation of several colloidal systems, nanoparticles, nanocapsules, and nanoemulsions, as ocular drug carriers. J. Pharm. Sci. 1996, 85, 530–536. [Google Scholar] [CrossRef]
- Vadlapudi, A.D.; Mitra, A.K. Nanomicelles: An emerging platform for drug delivery to the eye. Ther. Deliv. 2013, 4, 1–3. [Google Scholar] [CrossRef]
- Araújo, J.; Gonzalez, E.; Egea, M.A.; Garcia, M.L.; Souto, E.B. Nanomedicines for ocular NSAIDs: Safety on drug delivery. Nanomed. Nanotechnol. Biol. Med. 2009, 5, 394–401. [Google Scholar]
- Marmor, M.F.; Negi, A.; Maurice, D.M. Kinetics of macromolecules injected into the subretinal space. Exp. Eye Res. 1985, 40, 687–696. [Google Scholar] [CrossRef]
- Amrite, A.C.; Kompella, U.B. Size-dependent disposition of nanoparticles and microparticles following subconjunctival administration. J. Pharm. Pharmacol. 2005, 57, 1555–1563. [Google Scholar] [CrossRef] [PubMed]
- Cheruvu, N.P.; Amrite, A.C.; Kompella, U.B. Effect of eye pigmentation on transscleral drug delivery. Investig. Ophthalmol. Vis. Sci. 2008, 49, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Tezel, G. A proteomics view of the molecular mechanisms and biomarkers of glaucomatous neurodegeneration. Prog. Retin. Eye Res. 2013, 35, 18–43. [Google Scholar] [CrossRef] [Green Version]
- Sanvicens, N.; Marco, M.P. Multifunctional nanoparticles–properties and prospects for their use in human medicine. Trends Biotechnol. 2008, 26, 425–433. [Google Scholar] [CrossRef]
- Sahoo, S.K.; Misra, R.; Parveen, S. Nanoparticles: A boon to drug delivery, therapeutics, diagnostics and imaging. In Nanomedicine in Cancer; Pan Stanford: Stanford, CA, USA, 2017; pp. 73–124. [Google Scholar]
- Crommelin, D.J.; Florence, A.T. Towards more effective advanced drug delivery systems. Int. J. Pharm. 2013, 454, 496–511. [Google Scholar] [CrossRef]
- Smith, B.R.; Gambhir, S.S. Nanomaterials for in vivo imaging. Chem. Rev. 2017, 117, 901–986. [Google Scholar] [CrossRef]
- Osborne, N.N. Recent clinical findings with memantine should not mean that the idea of neuroprotection in glaucoma is abandoned. Acta Ophthalmol. 2009, 87, 450–454. [Google Scholar] [CrossRef]
- Moroi, S.E.; Raoof, D.A.; Reed, D.M.; Zöllner, S.; Qin, Z.; Richards, J.E. Progress toward personalized medicine for glaucoma. Expert Rev. Ophthalmol. 2009, 4, 145–161. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulation | Role/Function | Cargo | Material Type | Size (nm) | Stage | Ref. |
|---|---|---|---|---|---|---|
| Nanoparticle | Exhibition of superior transfection potency at the anterior region of the eye. | Gene | Chitosan | ~200 | Preclinical stage | [72] |
| Nanowafer | High level of nontoxicity with a low dose and ability to efficiently treat corneal neovascularization as compared with eye drops. | Axitinib | Polymer | 500 | Preclinical stage | [73] |
| Nanosuspension | Increasing retention time and penetration in corneal tissues. | Diclofenac | Polymer | 105 | Preclinical stage | [74] |
| Hydrogel (Virgan) | Treatment of herpes simplex infection in the eye. | Ganciclovir | Polymer | Data not found | On the market | [75,76,77,78] |
| Nanoparticle | Increased anti-inflammatory effect via the topical route. | Flurbiprofen | Polymer | 200–300 | Preclinical stage | [79] |
| Nanoparticle | Improved the efficacy of the drug to aid in corneal graft rejection. | Dexamethasone sodium phosphate | Polymer | 100–500 | Preclinical stage | [80] |
| Nanoscale dispersed ointment | Improved efficacy of corneal surface restoration and tear film repairing. | Data not found | Polymer | 100 | Preclinical Stage | [81] |
| Nanoparticle | Inhibitory effect in rabbit models with a mild response using a low drug concentration. A higher volume of the drug penetrated the aqueous humor in comparison with eye drops. | Flurbiprofen | Polymer | 100 | Preclinical stage | [82] |
| Hydrogel | Improvement of drug bioavailability in the eye as well as retention time on the surface of the cornea. | Diclofenac | Polymer | Data not found | Preclinical stage | [83] |
| Liposome | High anti-cataract effect with enhanced superoxide dismutase activity and glutathione reduction. | Coenzyme-Q10 | Polymer | 100–200 | Preclinical stage | [84] |
| Nanoparticle | Increase miotic response to 40%. | Pilocarpine | Polymer | 83 | Preclinical stage | [85] |
| Formulation | Role/Function | Cargo | Material Type | Size (nm) | Stage | Ref. |
|---|---|---|---|---|---|---|
| Nanoparticle | Provide sustained drug release via the subconjunctival route. | Latanoprost acid | Polymer | 80 | Preclinical stage | [47] |
| Hydrogel | Sustained drug release of Bevacizumab in SD rats for a period of four months. | Bevacizumab | Polymer | Data not found | Preclinical stage | [86] |
| Hydrogel (Timoptic-XE) | Treatment of glaucoma. | Timolol maleate | Polymer | Data not found | On the market | [87] |
| Liposome | Ability to pass through biological barriers after topical administration via annexin-A5 mediated endocytosis | Bevacizumab | Polymer | 100–200 | Preclinical stage | [73] |
| Hydrogel | Sustained drug release and decrease intraocular pressure as well as good compatibility with polymer. | Mitomycin C | Polymer | Data not found | Preclinical stage | [88] |
| Liposome | Entrapment of RPE cells and increased siRNA delivery by four-fold. | Gene | Polymer | 130–230 | Preclinical stage | [89,90] |
| Micelle | Sustain drug release for a period of one year after intravitreal injection in rat eyes. | Triamcinolone acetonide | Polymer | 200–350 | Preclinical stage | [72] |
| Dendrimer | Effective gene transfection in RPE cell lines. | Gene | Polymer | ~50 | Preclinical stage | [91] |
| Nanoparticle | Ability to prevent retinal degeneration and increase histological properties. | Gene | Peptide/ polymer | ~180 | Preclinical stage | [92] |
| Nanoparticle | Promotion of gene expression in RPE cells. | Gene | Polymer | ~250 | Preclinical stage | [93] |
| Formulation | Role/Functions | Target | Material Type | Size (nm) | Stage | Ref. |
|---|---|---|---|---|---|---|
| Nanoparticle | Nanoparticles coated with calcium elicit slight damage and can be used in retina imaging. | Retina | Silver | 80 | Preclinical stage | [148] |
| Nanoparticle | Improvement of angiogenic vessels in a rabbit corneal neovasculature model. | Corneal neovascularization | Gold | ~260 | Preclinical stage | [149] |
| Nano-cage | Good optical resonance | Retina | Gold | 35 | Preclinical stage | [150] |
| Nanoparticle | Enhanced and clear fluorophores in eye imaging. | Intraocular cancer | Quantum dots | 3–6 | Preclinical stage | [129,151] |
| Nanoparticle | Diffusion of nanoparticles present in in vitro model of human vitreous humor. | Retinal detachment | Magnetic Nanoparticles (Fe3O4) | 10 | Preclinical stage | [152] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juliana, F.R.; Kesse, S.; Boakye-Yiadom, K.O.; Veroniaina, H.; Wang, H.; Sun, M. Promising Approach in the Treatment of Glaucoma Using Nanotechnology and Nanomedicine-Based Systems. Molecules 2019, 24, 3805. https://doi.org/10.3390/molecules24203805
Juliana FR, Kesse S, Boakye-Yiadom KO, Veroniaina H, Wang H, Sun M. Promising Approach in the Treatment of Glaucoma Using Nanotechnology and Nanomedicine-Based Systems. Molecules. 2019; 24(20):3805. https://doi.org/10.3390/molecules24203805
Chicago/Turabian StyleJuliana, Fidiniaina Rina, Samuel Kesse, Kofi Oti Boakye-Yiadom, Hanitrarimalala Veroniaina, Huihui Wang, and Meihao Sun. 2019. "Promising Approach in the Treatment of Glaucoma Using Nanotechnology and Nanomedicine-Based Systems" Molecules 24, no. 20: 3805. https://doi.org/10.3390/molecules24203805