A Rapid Chemiluminescence Assay for Measurement of Folate in Small Volumes of Breast Milk


Abstract
:1. Introduction
2. Results
2.1. Sample Pre-Treatment for Recovery and Measurement Optimization
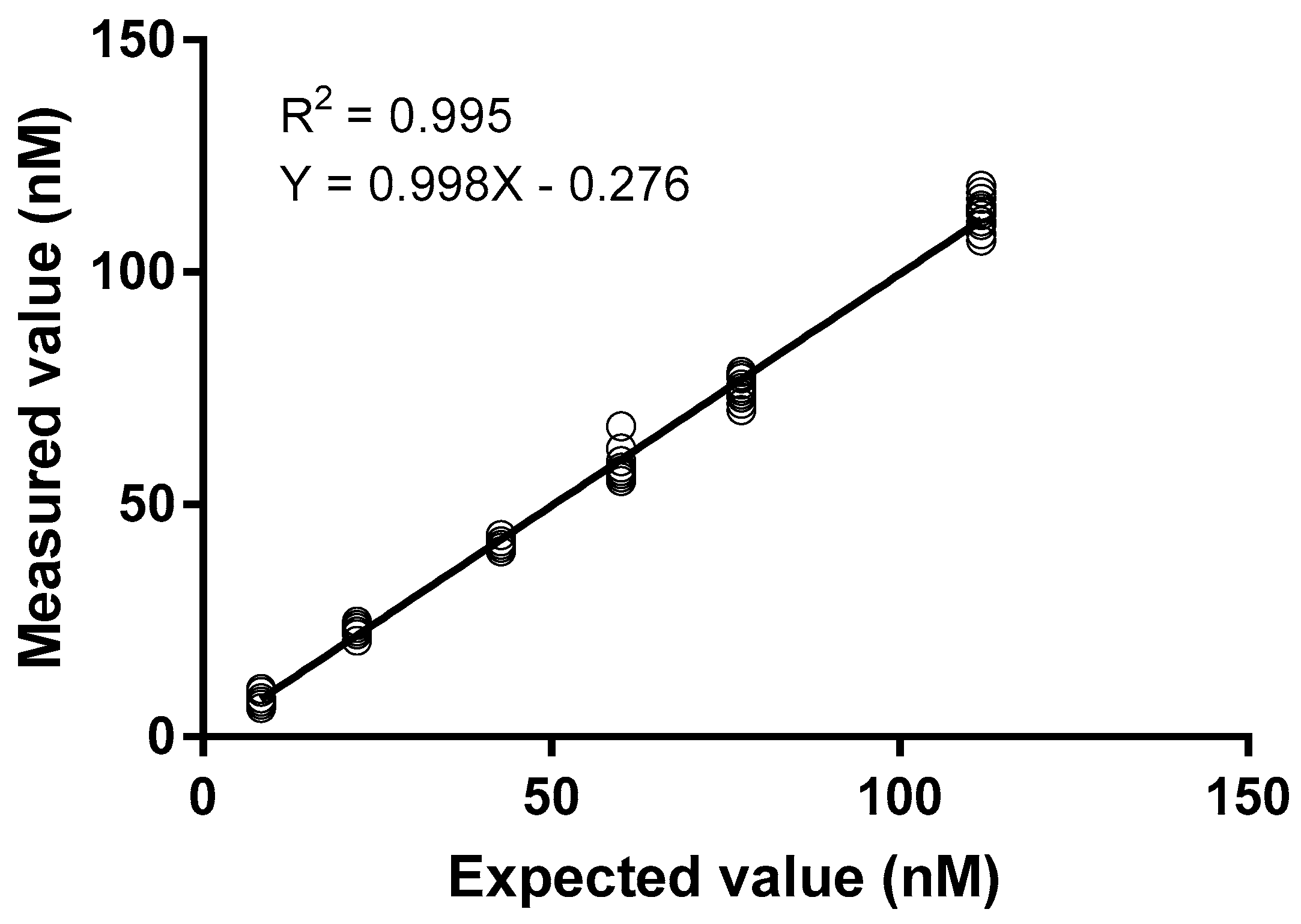
2.2. Analytical Range and Method Performance
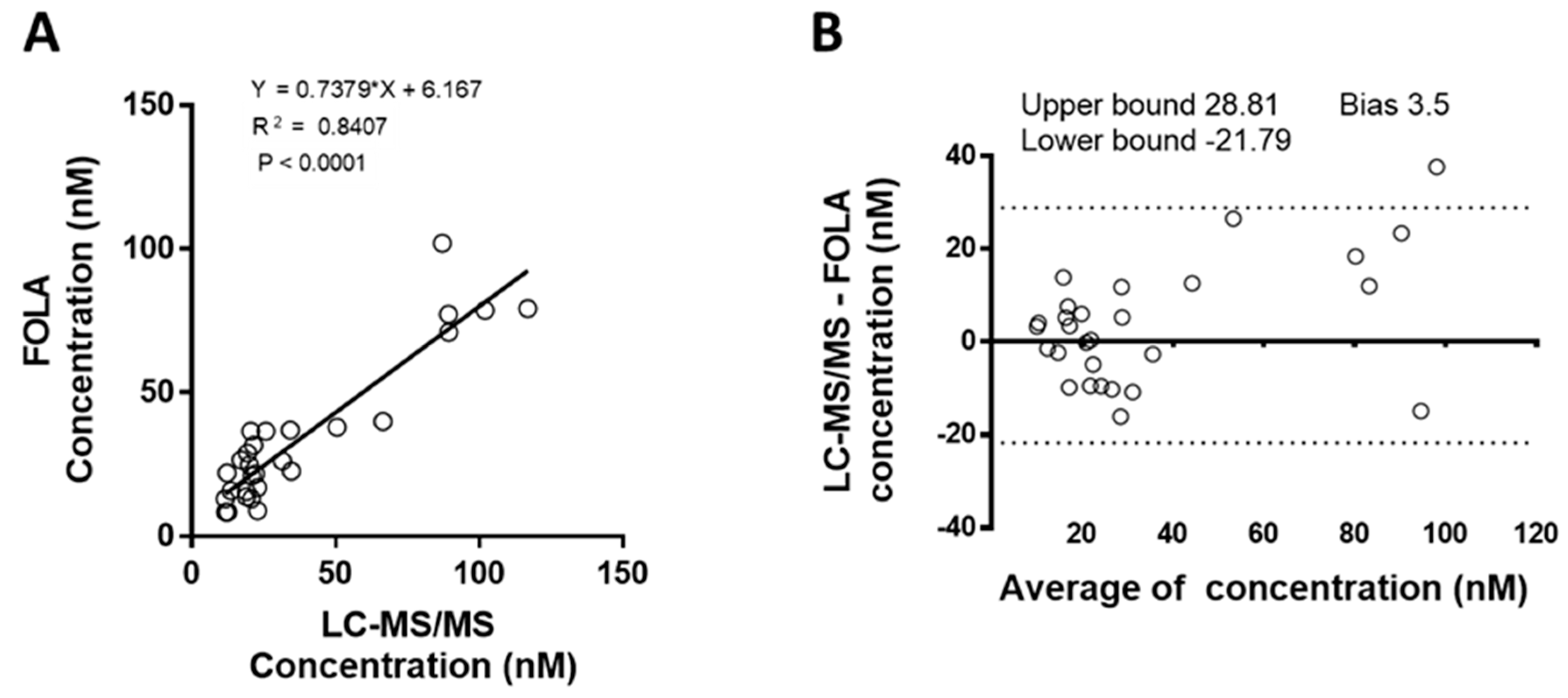
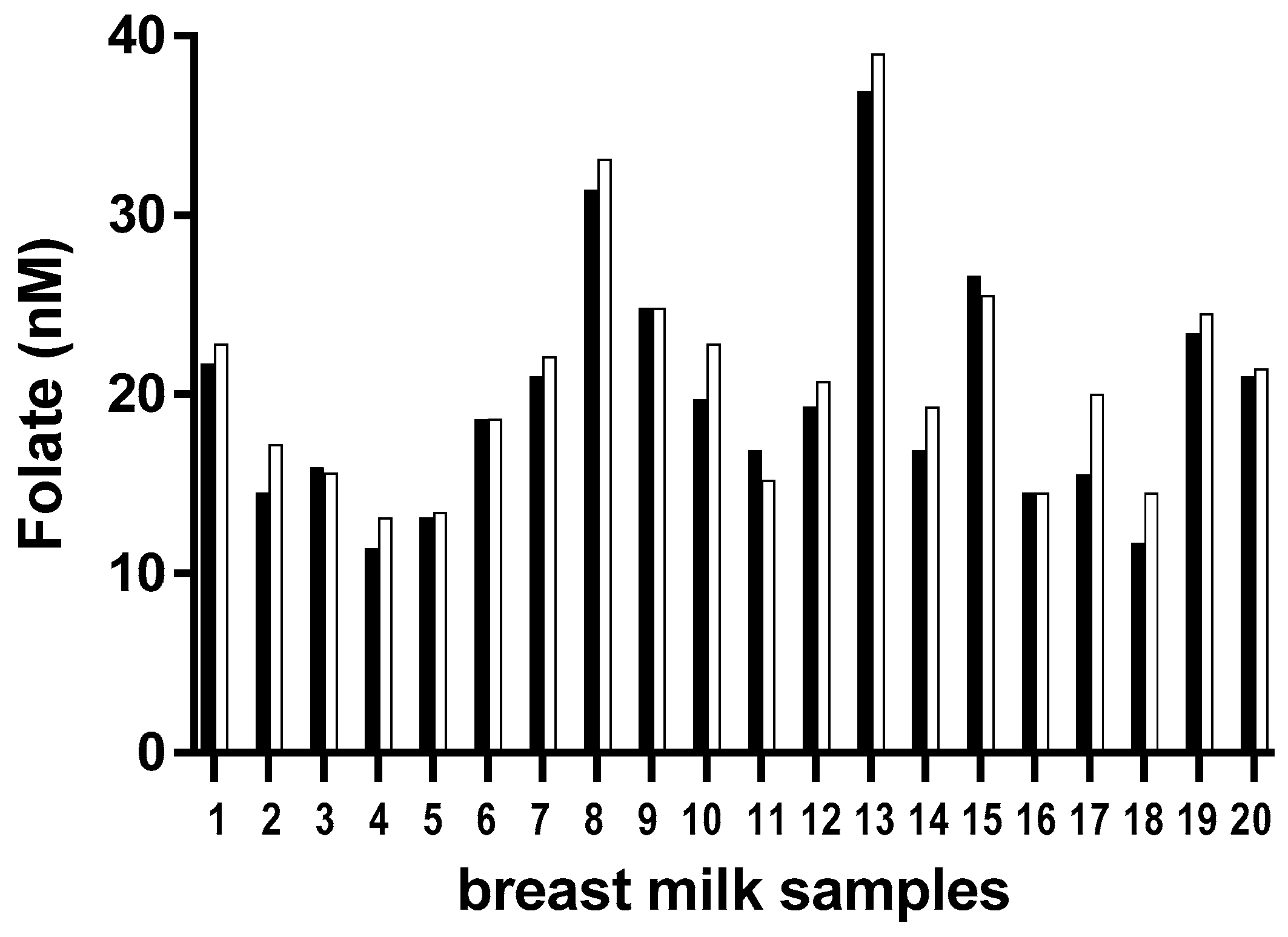
2.3. Comparison of Results with a LC-MS/MS Method
2.4. Folate Stability in Breast Milk Samples
2.5. Folate Levels in Milk Samples from the Life Cohort
3. Discussion
4. Materials and Methods
4.1. Standards and Controls
4.2. Breast Milk Samples
4.3. Sample Pre-Treatment
4.4. FOLA Method
4.5. Method Validation
4.6. LC-MS/MS Measurement
4.7. Statistical Analyses
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zheng, Y.; Cantley, L.C. Toward a better understanding of folate metabolism in health and disease. J. Exp. Med. 2019, 216, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, M.; Treiman, K.A.; Kish-Doto, J.; Middleton, J.C.; Coker-Schwimmer, E.J.L.; Nicholson, W.K. Folic Acid Supplementation for the Prevention of Neural Tube Defects: An Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2017, 317, 190–203. [Google Scholar] [CrossRef] [PubMed]
- Cantarella, C.D.; Ragusa, D.; Giammanco, M.; Tosi, S. Folate deficiency as predisposing factor for childhood leukaemia: A review of the literature. Genes Nutr. 2017, 12, 14. [Google Scholar] [CrossRef] [PubMed]
- Houghton, L.A.; Yang, J.; O’connor, D.L. Unmetabolized folic acid and total folate concentrations in breast milk are unaffected by low-dose folate supplements. Am. J. Clin. Nutr. 2009, 89, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H. B vitamins in breast milk: Relative importance of maternal status and intake, and effects on infant status and function. Adv. Nutr. 2012, 3, 362–369. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes and its Panel on Folate, Other B Vitamins, and Choline. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academies Press: Washington, DC, USA, 1998. [Google Scholar] [CrossRef]
- Tamura, T.; Picciano, M.F. Folate determination in human milk. J. Nutr. Sci. Vitaminol. 2006, 52, 161. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.-S.; Mackey, A.D.; Tamura, T.; Wong, S.C.; Picciano, M.F. Measurable human milk folate is increased by treatment with α-amylase and protease in addition to folate conjugase. Food Chem. 1998, 63, 401–407. [Google Scholar] [CrossRef]
- Pfeiffer, C.M.; Zhang, M.; Lacher, D.A.; Molloy, A.M.; Tamura, T.; Yetley, E.A.; Picciano, M.F.; Johnson, C.L. Comparison of serum and red blood cell folate microbiologic assays for national population surveys. J. Nutr. 2011, 141, 1402–1409. [Google Scholar] [CrossRef]
- Redeuil, K.; Benet, S.; Affolter, M.; Thakkar, K.S.; Campos Gimenez, E. A Novel Methodology for the Quantification of B-Vitamers in Breast Milk. J. Anal. Bioanal. Tech. 2017, 8. [Google Scholar] [CrossRef] [Green Version]
- West, A.A.; Yan, J.; Perry, C.A.; Jiang, X.; Malysheva, O.V.; Caudill, M.A. Folate-status response to a controlled folate intake in nonpregnant, pregnant, and lactating women. Am. J. Clin. Nutr. 2012, 96, 789–800. [Google Scholar] [CrossRef] [Green Version]
- Sakurai, T.; Furukawa, M.; Asoh, M.; Kanno, T.; Kojima, T.; Yonekubo, A. Fat-soluble and water-soluble vitamin contents of breast milk from Japanese women. J. Nutr. Sci. Vitaminol. 2005, 51, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Büttner, B.E.; Witthöft, C.M.; Domellöf, M.; Hernell, O.; Öhlund, I. Effect of type of heat treatment of breastmilk on folate content and pattern. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2014, 9, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Poulain, T.; Baber, R.; Vogel, M.; Pietzner, D.; Kirsten, T.; Jurkutat, A.; Hiemisch, A.; Hilbert, A.; Kratzsch, J.; Thiery, J.; et al. The LIFE Child study: A population-based perinatal and pediatric cohort in Germany. Eur. J. Epidemiol. 2017, 32, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Nygren-Babol, L.; Jagerstad, M. Folate-binding protein in milk: A review of biochemistry, physiology, and analytical methods. Crit Rev. Food Sci. Nutr. 2012, 52, 410–425. [Google Scholar] [CrossRef] [PubMed]
- Osifo, B.O.; Onifade, A. Effect of folate supplementation and malaria on the folate content of human milk. Nutr. Metab. 1980, 24, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Tamura, T.; Yoshimura, Y.; Arakawa, T. Human milk folate and folate status in lactating mothers and their infants. Am. J. Clin. Nutr. 1980, 33, 193–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, M.R.; Sneed, S.M.; Wei, C.; Nail, P.A.; Wilson, M.; Sprinkle, E.E. The effects of vitamin C, vitamin B6, vitamin B12, folic acid, riboflavin, and thiamin on the breast milk and maternal status of well-nourished women at 6 months postpartum. Am. J. Clin. Nutr. 1980, 33, 2151–2156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sneed, S.M.; Zane, C.; Thomas, M.R. The effects of ascorbic acid, vitamin B6, vitamin B12, and folic acid supplementation on the breast milk and maternal nutritional status of low socioeconomic lactating women. Am. J. Clin. Nutr. 1981, 34, 1338–1346. [Google Scholar] [CrossRef] [Green Version]
- Ford, J.E.; Zechalko, A.; Murphy, J.; Brooke, O.G. Comparison of the B vitamin composition of milk from mothers of preterm and term babies. Arch. Dis. Child. 1983, 58, 367–372. [Google Scholar] [CrossRef]
- Karra, M.V.; Udipi, S.A.; Kirksey, A.; Roepke, J.L. Changes in specific nutrients in breast milk during extended lactation. Am. J. Clin. Nutr. 1986, 43, 495–503. [Google Scholar] [CrossRef] [Green Version]
- Keizer, S.E.; Gibson, R.S.; O’Connor, D.L. Postpartum folic acid supplementation of adolescents: Impact on maternal folate and zinc status and milk composition. Am. J. Clin. Nutr. 1995, 62, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Mackey, A.D.; Picciano, M.F. Maternal folate status during extended lactation and the effect of supplemental folic acid. Am. J. Clin. Nutr. 1999, 69, 285–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khambalia, A.; Latulippe, M.E.; Campos, C.; Merlos, C.; Villalpando, S.; Picciano, M.F.; O’connor, D.L. Milk folate secretion is not impaired during iron deficiency in humans. J. Nutr. 2006, 136, 2617–2624. [Google Scholar] [CrossRef] [PubMed]
- Barwick, V.J.; Ellison, S.L.R.; Rafferty, M.J.Q.; Gill, R.S. The evaluation of measurement uncertainty from method validation studies. Accredit. Qual. Assur. 2000, 5, 104–113. [Google Scholar] [CrossRef]
- Rousseeuw, P.J.; Croux, C. Alternatives to the Median Absolute Deviation. J. Am. Stat. Assoc. 1993, 88, 1273–1283. [Google Scholar] [CrossRef]
Sample Availability: Samples are available from the authors. |




{kind=link}
{kind=link}
{kind=link}
| Spike Level (nM) | Median Measured Value (nM) | Repeatability | Intermediate Reproducibility | Recovery [%] | Uncertainty | Relative Uncertainty [%] |
|---|---|---|---|---|---|---|
| CV [%] | CV [%] | |||||
| 0 | 8.5 | 12.1 | 10.3 | - | - | - |
| 13.8 | 23.2 | 3.8 | 5.1 | 107 | 3.01 | 13 |
| 34.5 | 41.8 | 2.3 | 2.0 | 97 | 2.36 | 6 |
| 51.7 | 58.3 | 3.3 | 4.4 | 96 | 5.64 | 10 |
| 68.9 | 76.1 | 1.7 | 2.0 | 98 | 3.40 | 4 |
| 103.4 | 113.5 | 1.3 | 4.8 | 102 | 11.80 | 10 |
| a | Folate (nM) | ||||||
| Lactation Week | n | Average | SD | Median | Min | Max | |
| 12 | 243 | 27.2 | 15.8 | 23.4 | 6.2 | 89.6 | |
| 24 | 240 | 34.7 | 17.4 | 30.3 | 10.3 | 100.7 | |
| 52 | 66 | 29.5 | 19.2 | 24.1 | 9.0 | 97.9 | |
| b | Maternal / infant parameters | n | Average (SD) | ||||
| Maternal age at birth (years) | 333 | 31.17 (4.55) | |||||
| Gestational age (weeks) | 298 | 39.69 (1.67) | |||||
| n | Percentage of Infants | ||||||
| Exclusive breastfeeding at 3 months | 298 | 89% | |||||
| n | Male/Female | ||||||
| Gender | 333 | 175/158 | |||||
| C-section births | 324 | 57 (17.6%) | |||||
| Country, Year | n | Folate (nM) | Lactation Week | Method | Reference |
|---|---|---|---|---|---|
| Nigeria, 1980 | 30 | 11.3, 16.1 | 1, 2 | Microbiology (Lactobacillus casei 6375), No pretreatment | [16] |
| Japan, 1980 | 31 | 320.4 | 3–25 | Microbiology (L. casei), Conjugase pretreatment | [17] |
| USA, 1980 | 12 | 113.5 | 42 | Microbiology (L. casei), Pretreatment unclear | [18] |
| USA, 1981 | 16 | 94.3, 97.0 | 1, 6–7 | Microbiology (L. casei ATCC 7469), No pretreatment | [19] |
| UK, 1983 | 26–35 | 38.5, 70.2, 95.2 | 1, 2, 3–34 | Microbiology (L. casei), Pretreatment unspecified | [20] |
| USA, 1986 | 55 | 97.4, 63.4, 90.6, 49.8 | 49, 84, 126, 168 | Microbiology (L. casei ATCC 7469), No pretreatment | [21] |
| Canada, 1995 | 29 | 114.9, 124.6, 83.8 | 4, 8, 12 | Microbiology (L. casei), Conjugase pretreatment | [22] |
| USA, 1998 | 84 | 205.3, 184.7 | 12, 24 | Microbiology (L. casei), Trienzyme pretreatment. | [8] |
| USA, 1999 | 42 | 224.4, 187 | 12, 24 | Microbiology (L. casei), Trienzyme pretreatment | [23] |
| Japan, 2005 | 4000 | 339.9, 231.1, 117.8, 131.4, 53.0 | 1, 2, 3–13, 14–25, 26- 52 | HPLC | [12] |
| Mexico, 2006 | 71 | 103.1, 154.2, 143.3 | 3, 12, 20 | Microbiology (L. casei), Trienzyme pretreatment | [24] |
| Canada, 2009 | 69 (3 groups) | 181 | 16 | Microbiology (L. rhamnosus ATCC 7649), Trienzyme pretreatment | [4] |
| USA, 2012 | 28 | 142.0 (microbiological), 86.1 (HPLC) | 5–15 | HPLC and Microbiology (L. casei ATCC 7469), Conjugase pretreatment. | [11] |
| Sweden, 2014 | 38 | 150 | Unknown | HPLC | [13] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guignard, L.; Nembrini, C.; Moulin, J.; Meisser, K.; Silva-Zolezzi, I.; Kratzsch, J.; Vogel, M.; Kiess, W.; Eckhardt, E. A Rapid Chemiluminescence Assay for Measurement of Folate in Small Volumes of Breast Milk. Molecules 2019, 24, 2730. https://doi.org/10.3390/molecules24152730
Guignard L, Nembrini C, Moulin J, Meisser K, Silva-Zolezzi I, Kratzsch J, Vogel M, Kiess W, Eckhardt E. A Rapid Chemiluminescence Assay for Measurement of Folate in Small Volumes of Breast Milk. Molecules. 2019; 24(15):2730. https://doi.org/10.3390/molecules24152730
Chicago/Turabian StyleGuignard, Laurence, Chiara Nembrini, Julie Moulin, Karine Meisser, Irma Silva-Zolezzi, Jürgen Kratzsch, Mandy Vogel, Wieland Kiess, and Erik Eckhardt. 2019. "A Rapid Chemiluminescence Assay for Measurement of Folate in Small Volumes of Breast Milk" Molecules 24, no. 15: 2730. https://doi.org/10.3390/molecules24152730