Splenectomy in Lymphoproliferative Disorders: A Single Eastern European Center Experience

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
- Response to first-line treatment (mostly chemotherapy-61.5%) was generally partial (57.7% cases). As expected, chemotherapy as a single treatment was not associated with complete response in these patients. Thus, 76.9% (20/26) needed second line therapy, which was splenectomy in 80% of cases. The benefit of this therapeutic option was very good, because there was a 60% complete response (CR) rate.
- Splenectomy represented the first line treatment for only 34.6% of cases.
- 38.5% of patients presented different side effects after splenectomy (n = 26). Most of these were thrombotic complications in the abdominal area (four cases), followed by infections (approximately 30%), mechanical complications (eventration, hernia), and very rarely bleeding (accounting for 10% of all complications after splenectomy, respectively 3.8% of splenectomized patients).
4. Discussion
- The number of enrolled patients was low;
- We selected a control group of patients with NHL (non-splenectomized) to match the splenectomized ones as close as possible, before splenectomy took place. There might be a selection bias, as the discussed pathology is rare, and the study comprises only one center, which is located in a large emergency hospital in the capital city, receiving all types of hematological disorders; furthermore, splenectomy is not a frequently used procedure in malignant hematology.
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mavrodin, C.I.; Pariza, G.; Ion, D.; Antoniac, V.I. Abdominal compartment syndrome—a major complication of large incisional hernia surgery. Chirurgia 2013, 108, 414–417. [Google Scholar]
- Antoniac, I.; Negrusoiu, M.; Mardare, M.; Socoliuc, C.; Zazgyva, A.; Niculescu, M. Adverse local tissue reaction after 2 revision hip replacements for ceramic liner fracture: A case report. Medicine 2017, 96, e6687. [Google Scholar] [CrossRef] [PubMed]
- Earar, K.; Gradinaru, S.; Pariza, G.; Miculescu, F.; Antoniac, A.; Cojocaru, V.D.; Mohan, A.; Pintilie, G.; Grigorescu, D.O. Effect of the Sterilization Procedures of Different Surgical Meshes for Abdominal Surgery. Rev. Chim. 2017, 68, 1868–1873. [Google Scholar]
- Neagu, S.; Zarnescu, N.O.; Costea, R.; Stamatoiu, A.; Badea, V.; Dumitrescu, C.; Grădinaru, S.; Sajin, M.; Ardeleanu, C.; Pelmuş, M. Gastric stromal tumors-Clinical and histopathological analysis of four cases. Chirurgia 2003, 98, 443–451. [Google Scholar] [PubMed]
- Dumitrescu, D.; Savlovschi, C.; Borcan, R.; Pantu, H.; Serban, D.; Gradinaru, S.; Smarandache, G.; Trotea, T.; Branescu, C.; Musat, L.; et al. Clinical case-voluminous diaphragmatic hernia-surgically acute abdomen: diagnostic and therapeutical challenges. Chirurgia 2011, 106, 657–660. [Google Scholar]
- Vilcioiu, J.D.; Zamfirescu, D.G.; Cristescu, I.; Ursache, A.; Popescu, S.A.; Creanga, C.A.; Lascar, I. The interdisciplinary approach of an aggressive giant cell tumor of bone complicated with a fracture of the distal femur. Rom. J. Morphol. Embryo. 2016, 57, 567–572. [Google Scholar]
- Moldovan, H.; Popescu, D.; Buliga, T.; Filip, A.; Antoniac, I.; Gheorghita, D.; Molnar, A. Gastric Adenocarcinoma Associated with Acute Endocarditis of the Aortic Valve and Coronary Artery Disease in a 61-Year-Old Male with Multiple Comorbidities-Combined Surgical Management-Case Report. Medicina (Lithuania) 2019, 55, 242. [Google Scholar] [CrossRef] [Green Version]
- Chacón, J.I.; Mollejo, M.; Muñoz, E.; Algara, P.; Mateo, M.; Lopez, L.; Andrade, J.; Carbonero, I.G.; Martínez, B.; Piris, M.A.; et al. Splenic marginal zone lymphoma: clinical characteristics and prognostic factors in a series of 60 patients. Blood 2002, 100, 1648. [Google Scholar] [CrossRef] [Green Version]
- Perrone, S.; D’Elia, G.M.; Annechini, G.; Ferretti, A.; Tosti, M.E.; Foà, R.; Pulsoni, A. Splenic marginal zone lymphoma: Prognostic factors, role of watch and wait policy, and other therapeutic approaches in the rituximab era. Leuk. Res. 2016, 44, 53–60. [Google Scholar] [CrossRef]
- Olszewski, A.J.; Castillo, J.J. Survival of patients with marginal zone lymphoma: analysis of the Surveillance, Epidemiology, and End Results database. Cancer 2013, 119, 629–638. [Google Scholar] [CrossRef]
- Joshi, M.; Sheikh, H.; Abbi, K.; Long, L. Marginal zone lymphoma: old, new, targeted, and epigenetic therapies. Therap. Adv. Hematol. Oct. 2012, 3, 275–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franco, V.; Florena, A.M.; Iannitto, E. Splenic marginal zone lymphoma. Blood 2003, 101, 2464–2472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Comprehensive Cancer Network. Available online: https://www.nccn.org/store/login/login.aspx?ReturnURL=https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf (accessed on 1 September 2017).
- Baccarani, U.; Terrosu, G.; Donini, A.; Zaja, F.; Bresadola, F.; Baccarani, M. Splenectomy in hematology: Current practice and new perspectives. Haematologica 1999, 84, 431–436. [Google Scholar]
- Thieblemont, C.; Felman, P.; Callet-Bauchu, E.; Traverse-Glehen, A.; Salles, G.; Berger, F.; Coiffier, B. Splenic marginal-zone lymphoma: a distinct clinical and pathological entity. Lancet Oncol. 2003, 4, 95. [Google Scholar] [CrossRef]
- Montalbán, C.; Abraira, V.; Arcaini, L.; Domingo-Domenech, E.; Guisado-Vasco, P.; Iannitto, E.; Mollejo, M.; Matutes, E.; Ferreri, A.; Salar, A.; et al. Risk stratification for Splenic Marginal Zone Lymphoma based on haemoglobin concentration, platelet count, high lactate dehydrogenase level and extrahilar lymphadenopathy: development and validation on 593 cases. Br. J. Haematol. 2012, 159, 164. [Google Scholar] [CrossRef]
- Parry-Jones, N.; Matutes, E.; Gruszka-Westwood, A.M.; Swansbury, G.J.; Wotherspoon, A.C.; Catovsky, D. Prognostic features of splenic lymphoma with villous lymphocytes: a report on 129 patients. Br. J. Haematol. 2003, 120, 759. [Google Scholar] [CrossRef]
- Iannitto, E.; Ambrosetti, A.; Ammatuna, E.; Colosio, M.; Florena, A.M.; Tripodo, C.; Minardi, V.; Calvaruso, G.; Mitra, M.E.; Pizzolo, G.; et al. Splenic marginal zone lymphoma with or without villous lymphocytes. Hematologic findings and outcomes in a series of 57 patients. Cancer 2004, 101, 2050. [Google Scholar] [CrossRef] [Green Version]
- Thieblemont, C. Clinical presentation and management of marginal zone lymphomas. Hematol. Am. Soc. Hematol. Educ. Program 2005, 307–313. [Google Scholar] [CrossRef] [Green Version]
- Hammer, R.D.; Glick, A.D.; Greer, J.P.; Collins, R.D.; Cousar, J.B. Splenic marginal zone lymphoma: A distinct B-cell neoplasm. Am. J. Surg. Pathol. 1996, 20, 613–626. [Google Scholar] [CrossRef]
- Pawade, J.; Wilkins, B.S.; Wright, D.H. Low-grade B-cell lymphomas of the splenic marginal zone: A clinicopathological and immunohistochemical study of 14 cases. Histopathology 1995, 27, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Hermine, O.; Lefrere, F.; Bronowicki, J.; Mariette, X.; Jondeau, K.; Eclache-Saudreau, V.; Delmas, B.; Valensi, F.; Cacoub, P.; Brechot, C.; et al. Regression of splenic lymphoma with villous lymphocytes after treatment of hepatitis C virus infection. N. Engl. J. Med. 2002, 11, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Saadoun, D.; Suarez, F.; Lefrere, F.; Valensi, F.; Mariette, X.; Aouba, A.; Besson, C.; Varet, B.; Troussard, X.; Cacoub, P.; et al. Splenic lymphoma with villous lymphocytes, associated with type II cryoglobulinemia and HCV infection: a new entity? Blood 2005, 105, 74–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodgers, G. Thrombocytopenia: Pathophysiology and classification. In Wintrobe’s Clinical Haematology, 12th ed.; Greer, J., Foerster, J., Lukens, J., Rodgers, G., Paraskevas, F., Glader, B., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2009; pp. 1289–1291. [Google Scholar]
- Arcaini, L.; Paulli, M.; Boveri, E.; Magrini, U.; Lazzarino, M. Marginal zone-related neoplasms of splenic and nodal origin. J. Hematol. 2003, 88, 80–93. [Google Scholar]
- Van Huyen, J.P.; Molina, T.; Delmer, A.; Audouin, J.; Le Tourneau, A.; Zittoun, R.; Bernadou, A.; Diebold, J. Splenic marginal zone lymphoma with or without plasmacytic differentiation. Am. J. Surg. Pathol. 2000, 24, 1581–1592. [Google Scholar] [CrossRef]
- Murakami, H.; Irisawa, H.; Saitoh, T.; Matsushima, T.; Tamura, J.; Sawamura, M.; Karasawa, M.; Hosomura, Y.; Kojima, M. Immunological abnormalities in splenic marginal zone cell lymphoma. Am. J. Hematol. 1997, 56, 173–178. [Google Scholar] [CrossRef]
- Roumier, M.; Loustau, V.; Guillaud, C.; Languille, L.; Mahevas, M.; Khellaf, M.; Limal, N.; Noizat-Pirenne, F.; Godeau, B.; Michel, M. Characteristics and outcome of warm autoimmune hemolytic anemia in adults: New insights based on a singlecenter experience with 60 patients. Am. J. Hematol. 2014, 89, E15. [Google Scholar] [CrossRef]
- Lenglet, J.; Traullé, C.; Mounier, N.; Benet, C.; Munoz-Bongrand, N.; Amorin, S.; Noguera, M.E.; Traverse-Glehen, A.; Ffrench, M.; Baseggio, L.; et al. Long-term follow-up analysis of 100 patients with splenic marginal zone lymphoma treated with splenectomy as first-line treatment. Leuk. Lymphoma. 2014, 55, 1854–1860. [Google Scholar] [CrossRef] [PubMed]
- Iannitto, E.; Tripodo, C. How I diagnose and treat splenic lymphomas. Blood 2011, 117, 2585–2595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, K.H.; Kahlon, A.; Skinnider, B.F.; Connors, J.M.; Gascoyne, R.D.; Sehn, L.H.; Savage, K.J.; Slack, G.W.; Shenkier, T.N.; Klasa, R.; et al. Outcomes in splenic marginal zone lymphoma: analysis of 107 patients treated in British Columbia. Br. J. Haematol. 2015, 169, 520–527. [Google Scholar] [CrossRef]
- Grahn, S.W.; Alvarez, J., 3rd; Kirkwood, K. Trends in laparoscopic splenectomy for massive splenomegaly. Arch. Surg. 2006, 141, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Klingersmith, M.E. The Washington Manual of Surgery; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2008; pp. 290–291. [Google Scholar]
- Romano, F.; Garancini, M. The implications for patients undergoing splenectomy: postsurgery risk management. Dovepress 2011, 2011, 23–34. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Lot | Value | p |
|---|---|---|---|
| Age (years) | SMZL Indolent NHL | 59.5 ± 9.7 61.5 ± 10.4 | NS |
| Splenectomized Non-splenectomized | 59.0 ± 9.5 55.1 ± 17.6 | NS | |
| Hemoglobin (g/dL) | SMZL Indolent NHL | 9.5 ± 2.1 11.2 ± 1.9 | 0.049 |
| Splenectomized Non-splenectomized | 10.3 ± 2.2 10.5 ± 2.6 | NS | |
| Leucocytes (× 103/mmc) | SMZL Indolent NHL | 18.3 ± 16.8 9.3 ± 4.2 | NS |
| Splenectomized Non-splenectomized | 16.9 ± 15.5 8.6+ ± 4.1 | 0.050 | |
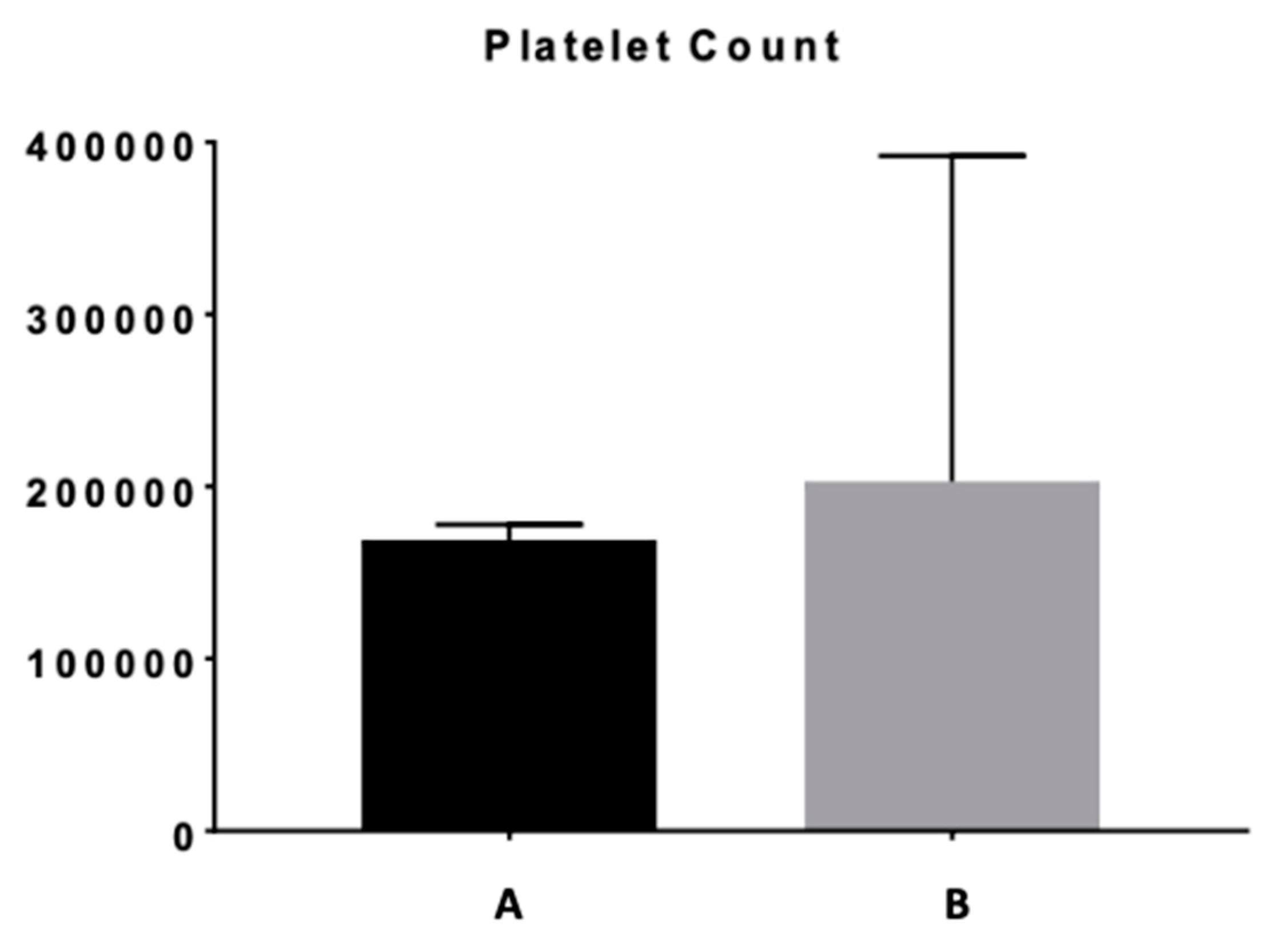
| Thrombocytes (× 103/mmc) | SMZL Indolent NHL | 172.2 ± −97.0 270.7 ± 133.0 | 0.019 |
| Risk rates (OR) | |||
| Lymphocytosis | SMZL Indolent NHL | 6.00 | 0.018 |
| Splenectomized Non-splenectomized | 9.15 | 0.0004 | |
| Low albumin | SMZL Indolent NHL | 1.73 | NS |
| Splenectomized Non-splenectomized | 3.15 | 0.040 | |
| Autoimmune anemia | SMZL Indolent NHL | 3.78 | NS |
| Splenectomized Non-splenectomized | 6.84 | 0.027 | |
| Advanced vs. early stage (Ann-Arbor) | SMZL Indolent NHL | NS | NS |
| Splenectomized Non-splenectomized | 2.58 | NS |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onisâi, M.; Vlădăreanu, A.-M.; Nica, A.; Spînu, A.; Găman, M.; Bumbea, H.; Voican, I.; Iordan, I.; Alexandru, A.; Zdrenghea, M.; et al. Splenectomy in Lymphoproliferative Disorders: A Single Eastern European Center Experience. Medicina 2020, 56, 12. https://doi.org/10.3390/medicina56010012
Onisâi M, Vlădăreanu A-M, Nica A, Spînu A, Găman M, Bumbea H, Voican I, Iordan I, Alexandru A, Zdrenghea M, et al. Splenectomy in Lymphoproliferative Disorders: A Single Eastern European Center Experience. Medicina. 2020; 56(1):12. https://doi.org/10.3390/medicina56010012
Chicago/Turabian StyleOnisâi, Minodora, Ana-Maria Vlădăreanu, Adriana Nica, Andreea Spînu, Mihaela Găman, Horia Bumbea, Irina Voican, Iuliana Iordan, Adrian Alexandru, Mihnea Zdrenghea, and et al. 2020. "Splenectomy in Lymphoproliferative Disorders: A Single Eastern European Center Experience" Medicina 56, no. 1: 12. https://doi.org/10.3390/medicina56010012