Lumboperitoneal Shunt: A New Modified Surgical Technique and a Comparison of the Complications with Ventriculoperitoneal Shunt in a Single Center



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Surgery Procedure
2.2.1. Pre-Operative Assessment for LP Shunt Group
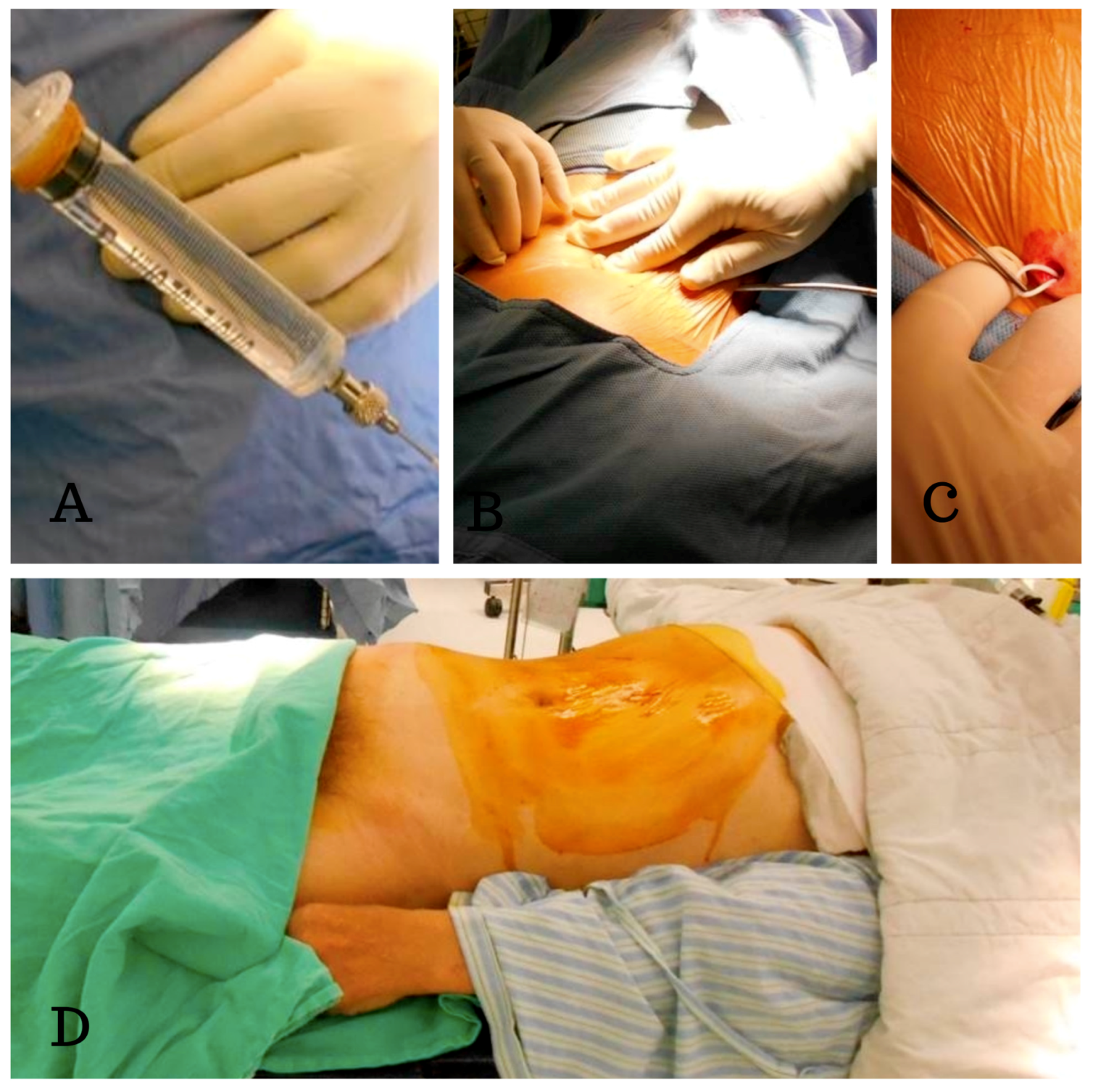
2.2.2. Procedure of the New Two-Stage Procedure for LP Shunts Insertion
2.2.3. Procedure of the VP Shunt Insertion
2.3. Statistical Analysis
3. Results
4. Discussion
- (1)
- It allowed us to easily perform lumbar tapping and insertion of the spinal catheter under fluoroscopic guidance. Sabah et al. revealed that insertion of an LP shunt without fluoroscopy guidance has a 15.8% chance of false positioning of the proximal end of the spinal catheter [11]. We designed the two-stage surgery with the patient in a prone then a supine position. In the first stage, the prone position simplified checking the true lateral view of the spine X-ray so that we could actually place the catheter in the correct position.
- (2)
- It ensured one lumbar tapping into intrathecal sac. This decreased the trauma rate during the puncture, as trauma might cause severe complications. Basaran et al. showed a case report of a spinal intradural hematoma and permanent paraparesis after an LP shunt insertion, while other studies have also reported the induction of epidural hematomas by spinal puncture [12,13,14].
- (3)
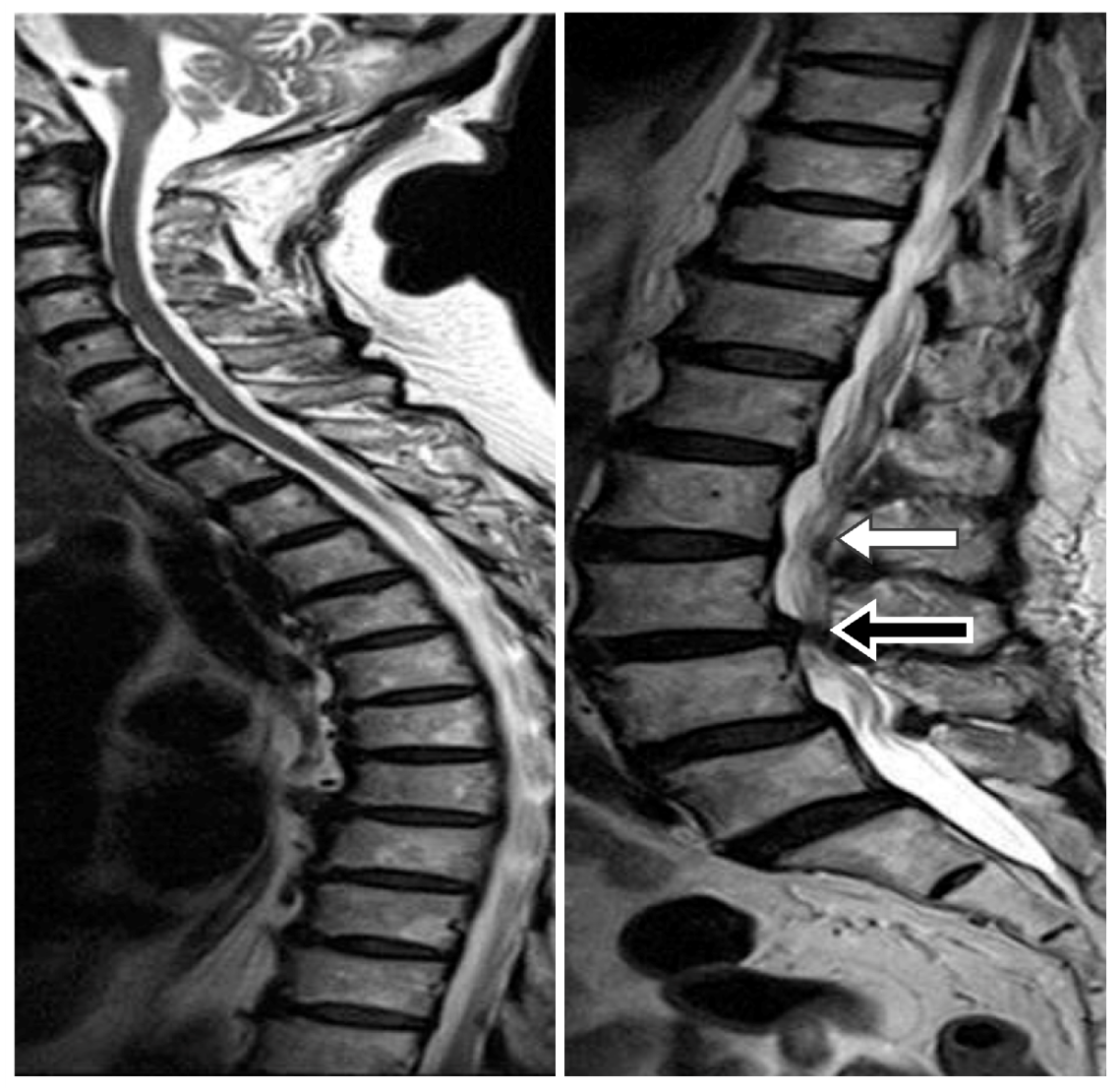
- It avoided the kinking of the lumbar spinal catheter in the thecal sac. In our experience, spinal catheter entanglement or twisting occurred in about 10%–15% cases, but we were able to correct it immediately under fluoroscopic guidance (Figure 5).
- (4)
- It ensured the level of the lumbar catheter tip placement. We placed the spinal catheter tip at the T8–10 level, which helped to avoid extraction of the spinal catheter from thecal sac when the patient performs strenuous exercise. Matsubara et al. revealed a case report of CSF leakage into the epidural space through a side hole, due to placement of a length of the spinal catheter into the dural sac. Shortly after the operation, the side hole was opened up when the patient moved his body [15].
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Savitz, M.H.; Bobroff, L.M. Low incidence of delayed intracerebral hemorrhage secondary to ventriculoperitoneal shunt insertion. J. Neurosurg. 1999, 91, 32–34. [Google Scholar] [CrossRef] [PubMed]
- Chumas, P.D.; Armstrong, D.C.; Drake, J.M.; Kulkarni, A.V.; Hoffman, H.J.; Humphreys, R.P.; Rutka, J.T.; Hendrick, E.B. Tonsillar herniation: The rule rather than the exception after lumboperitoneal shunting in the pediatric population. J. Neurosurg. 1993, 78, 568–573. [Google Scholar] [CrossRef] [PubMed]
- Ishiwata, Y.; Yamashita, T.; Ide, K.; Gondo, G.; Kuwana, N.; Kuwabara, T. A new technique for percutaneous study of lumboperitoneal shunt patency. Technical note. J. Neurosurg. 1988, 681, 52–54. [Google Scholar]
- Spetzler, R.; Wilson, C.B.; Schulte, R. Simplified percutaneous lumboperitoneal shunting. Surg. Neurol. 1977, 7, 25–29. [Google Scholar] [PubMed]
- Aoki, N. Lumboperitoneal shunt: Clinical applications, complications, and comparison with ventriculoperitoneal shunt. Neurosurgery 1990, 26, 998–1004. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Vajpeyi, I.N. Comparative study of lumboperitoneal shunt versus ventriculoperitoneal shunt in post meningitis communicating hydrocephalus in children. Neurol. India 2013, 61, 513–516. [Google Scholar] [CrossRef]
- Duthel, R.; Nuti, C.; Motuo-Fotso, M.J.; Beauchesne, P.; Brunon, J. Complications of lumboperitoneal shunts. A retrospective study of a series of 195 patients (214 procedures). Neuro-Chirurgie 1996, 42, 83–89. [Google Scholar]
- Wu, Y.; Green, N.L.; Wrensch, M.R.; Zhao, S.; Gupta, N. Ventriculoperitoneal shunt complications in California: 1990 to 2000. Neurosurgery 2007, 61, 557–562. [Google Scholar] [CrossRef]
- Reddy, G.K.; Bollam, P.; Caldito, G. Ventriculoperitoneal shunt surgery and the risk of shunt infection in patients with hydrocephalus: Long-term single institution experience. World Neurosurg. 2012, 78, 155–163. [Google Scholar] [CrossRef]
- Chumas, P.D.; Kulkarni, A.V.; Drake, J.M.; Hoffman, H.J.; Humphreys, R.P.; Rutka, J.T. Lumboperitoneal shunting: A retrospective study in the pediatric population. Neurosurgery 1993, 32, 376–383. [Google Scholar] [CrossRef]
- Al-Rashed, S.; Kareem, H.; Kalra, N.; D’Antona, L.; Obeidat, M.; Patel, B.; Toma, A. Lumboperitoneal shunt insertion without fluoroscopy guidance: Accuracy of placement in a series of 107 procedures. F1000Research 2017, 6, 565. [Google Scholar] [CrossRef] [PubMed]
- Basaran, R.; Efendioglu, M.; Bolukbasi, F.H.; Aslan, S.; Isik, N.; Kaner, T. Spinal intradural hematoma and permanent paraparesis after a lumboperitoneal shunt operation: An unusual complication. Asian Spine J. 2014, 8, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Kou, J.; Fischgrund, J.; Biddinger, A.; Herkowitz, H. Risk factors for spinal epidural hematoma after spinal surgery. Spine 2002, 27, 1670–1673. [Google Scholar] [CrossRef] [PubMed]
- Gurkanlar, D.; Acikbas, C.; Cengiz, G.K.; Tuncer, R. Lumbar epidural hematoma following lumbar puncture: The role of high dose LMWH and late surgery. A case report. Neurocirugia 2007, 18, 52–55. [Google Scholar] [CrossRef]
- Matsubara, T.; Ishikawa, E.; Hirata, K.; Matsuda, M.; Akutsu, H.; Masumoto, T.; Zaboronok, A.; Matsumura, A. A new mechanism of cerebrospinal fluid leakage after lumboperitoneal shunt: A theory of shunt side hole—Case report. Neurol. Medico-Chirurgica 2014, 54, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Wang, V.Y.; Barbaro, N.M.; Lawton, M.T.; Pitts, L.; Kunwar, S.; Parsa, A.T.; Gupta, N.; McDermott, M.W. Complications of lumboperitoneal shunts. Neurosurgery 2007, 60, 1045–1048. [Google Scholar] [CrossRef] [PubMed]
- Yadav, Y.R.; Parihar, V.; Sinha, M. Lumbar peritoneal shunt. Neurol. India 2010, 58, 179–184. [Google Scholar] [CrossRef]
- Yadav, Y.R.; Pande, S.; Raina, V.K.; Singh, M. Lumboperitoneal shunts: Review of 409 cases. Neurol. India 2004, 52, 188–190. [Google Scholar]
- Bloch, O.; McDermott, M.W. Lumboperitoneal shunts for the treatment of normal pressure hydrocephalus. J. Clin. Neurosci. 2012, 19, 1107–1111. [Google Scholar] [CrossRef]
- Kazui, H.; Miyajima, M.; Mori, E.; Ishikawa, M.; Investigators, S. Lumboperitoneal shunt surgery for idiopathic normal pressure hydrocephalus (SINPHONI-2): An open-label randomised trial. Lancet Neurol. 2015, 14, 585–594. [Google Scholar] [CrossRef]
- El-Saadany, W.F.; Farhoud, A.; Zidan, I. Lumboperitoneal shunt for idiopathic intracranial hypertension: Patients’ selection and outcome. Neurosurg. Rev. 2012, 35, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Alkherayf, F.; Abou Al-Shaar, H.; Awad, M. Management of idiopathic intracranial hypertension with a programmable lumboperitoneal shunt: Early experience. Clin. Neurol. Neurosurg. 2015, 136, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, M.; Miyajima, M.; Akiba, C.; Ogino, I.; Kawamura, K.; Sugano, H.; Hara, T.; Tange, Y.; Fusegi, K.; Karagiozov, K.; et al. Lumboperitoneal shunts for the treatment of idiopathic normal pressure hydrocephalus: A comparison of small-lumen abdominal catheters to gravitational add-on valves in a single center. Oper. Neurosurg. 2018, 15, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Miyajima, M.; Kazui, H.; Mori, E.; Ishikawa, M. Sinphoni-Investigators obot. One-year outcome in patients with idiopathic normal-pressure hydrocephalus: Comparison of lumboperitoneal shunt to ventriculoperitoneal shunt. J. Neurosurg. 2016, 125, 1483–1492. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LP Versus VP | LP Group | VP Group | p Value †† |
|---|---|---|---|
| Total surgery number | 96 | 192 | |
| Revision * | 1 (1.0%) | 26 (13.5%) | 0.001 |
| Shunt malfunction † | 0 (0.0%) | 14 (7.3%) | N/A |
| Shunt infection | 1 (1.0%) | 11 (5.7%) | 0.061 |
| Subdural hematoma | 1 (1.0%) | 5 (2.6%) | 0.766 |
| LP Versus VP | LPS Group Our Study (n = 137) | VPS Group Yvonne (n = 14,455) | p Value | VPS Group Reddy (n = 1015) | p Value † |
|---|---|---|---|---|---|
| Total surgery number | 138 | N/D | 2239 | ||
| Revision | 1 (0.7%) | 1224 (21.6%) | <0.001 | 1224 (50.2%) | <0.001 |
| Any shunt complication | 4 (2.9%) | 4192 (29.0%) | <0.001 | N/D | N/A |
| Shunt infection | 1 (0.7%) | N/D | N/A | 162 (7.2%) | <0.001 |
| LP Versus LP | Ours (n = 137) | Aoki (n = 204) | p Value †† | Duthel (n = 195) | p Value †† | Yadav (n = 409) | p Value †† | Bloch (n = 33) | p Value †† |
|---|---|---|---|---|---|---|---|---|---|
| Revision | 1 (0.7%) | 33 (16.2%) | <0.001 | N/D | N/D | 44 (11%) | <0.001 | 9 (17%) | <0.001 |
| Malfunction | 0 | 29 (14%) | N/A | 28 (4%) | N/A | 32 (7.8%) | N/A | 5 (15%) | N/A |
| Infection | 1 (0.7%) | 2 (1%) | 0.813 | 10 (5%) | 0.028 | 14 (3.4%) | 0.097 | 2 (6%) | 0.038 |
| CSF leakage * | 0 | 0 | N/A | 0 | N/A | 12 (2.9%) | N/A | 2(6%) | N/A |
| ACM | 0 | 4 (2%) | N/A | 1 (0.5%) | N/A | 2 (0.5%) | N/A | 0 | N/A |
| Radicular pain | 0 | 10 (5%) | N/A | 0 | N/A | 2 (0.5%) | N/A | 0 | N/A |
| Subdural hematoma † | 3 (2.2%) | 6 (2.9%) | 0.679 | 8 (4%) | 0.343 | 0 | N/A | 2 (6%) | 0.241 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, T.-H.; Chang, C.-S.; Sung, W.-W.; Liu, J.-T. Lumboperitoneal Shunt: A New Modified Surgical Technique and a Comparison of the Complications with Ventriculoperitoneal Shunt in a Single Center. Medicina 2019, 55, 643. https://doi.org/10.3390/medicina55100643
Yang T-H, Chang C-S, Sung W-W, Liu J-T. Lumboperitoneal Shunt: A New Modified Surgical Technique and a Comparison of the Complications with Ventriculoperitoneal Shunt in a Single Center. Medicina. 2019; 55(10):643. https://doi.org/10.3390/medicina55100643
Chicago/Turabian StyleYang, Tsung-Hsi, Cheng-Siu Chang, Wen-Wei Sung, and Jung-Tung Liu. 2019. "Lumboperitoneal Shunt: A New Modified Surgical Technique and a Comparison of the Complications with Ventriculoperitoneal Shunt in a Single Center" Medicina 55, no. 10: 643. https://doi.org/10.3390/medicina55100643