Effectiveness of Low-Level Laser Therapy with a 915 Nm Wavelength Diode Laser on the Healing of Intraoral Mucosal Wound: An Animal Study and a Double-Blind Randomized Clinical Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal Study
2.2. Surgical Procedures
2.3. Clinical Study Participants
2.4. Inclusion/Exclusion Criteria
2.5. Clinical Study Procedures
2.6. Statistical Analysis
3. Results
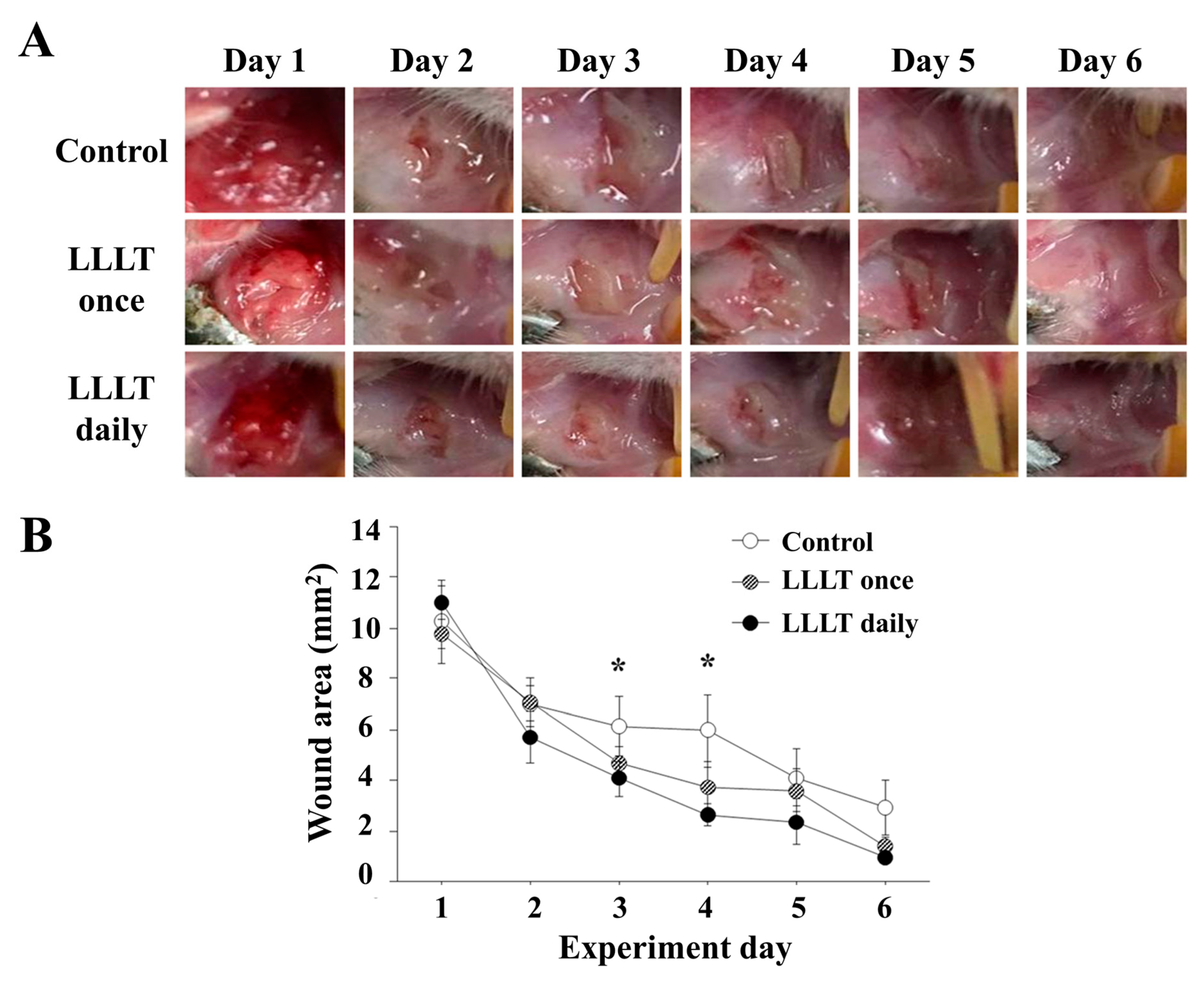
3.1. Animal Study
3.2. Clinical Study
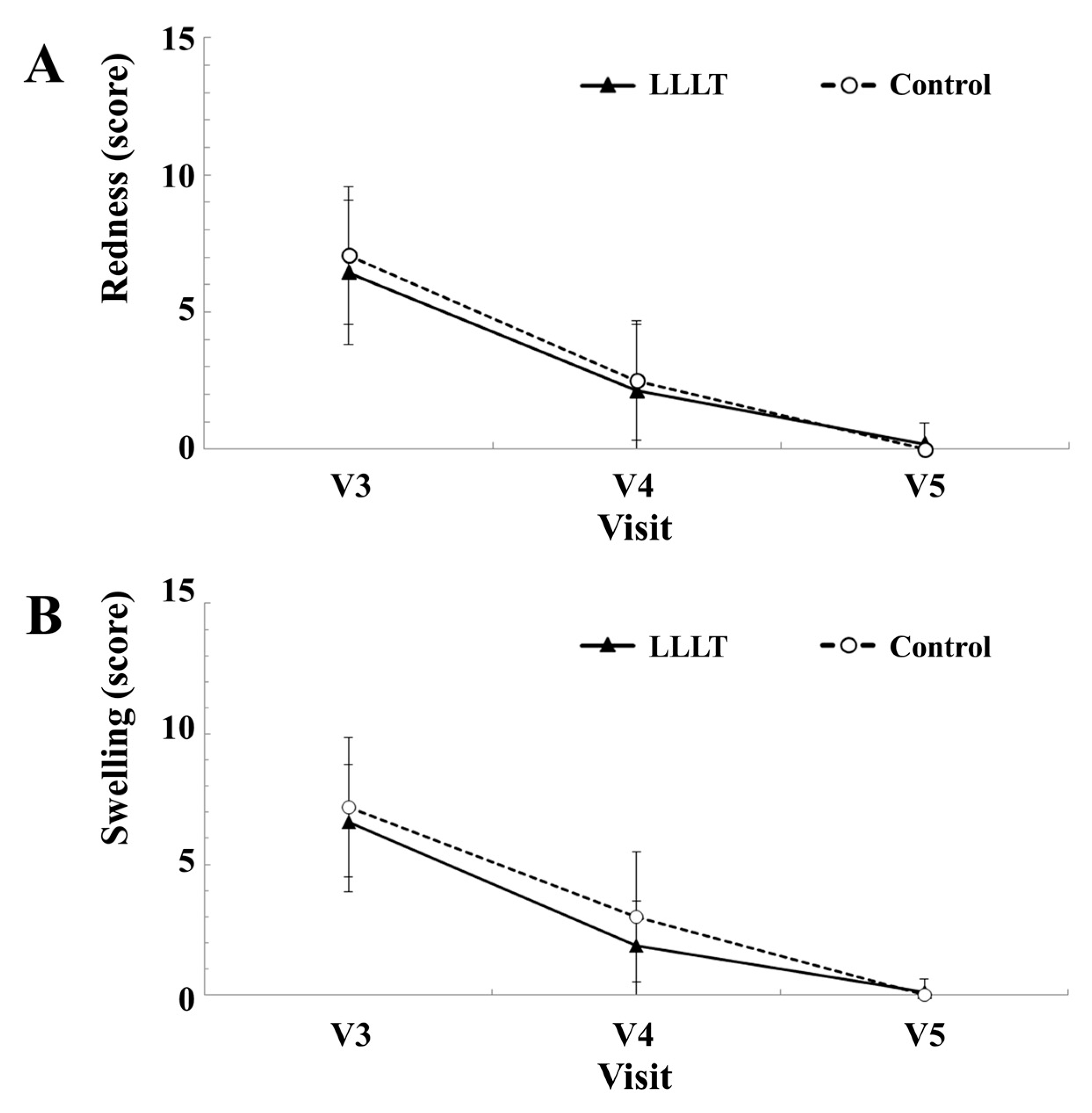
3.2.1. Redness and Swelling Intensities
3.2.2. Pain Intensity and Dehiscence of the Wound
3.2.3. Overall Efficacy Evaluation
3.2.4. Safety Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Sato, F.R.L.; Asprino, L.; De Araújo, D.E.S.; De Moraes, M. Short-Term Outcome of Postoperative Patient Recovery Perception After Surgical Removal of Third Molars. J. Oral Maxillofac. Surg. 2009, 67, 1083–1091. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Brar, P.; Jakubowski, J.; Kaltman, S.; Lopez, E. The use of corticosteroids and nonsteroidal antiinflammatory medication for the management of pain and inflammation after third molar surgery: A review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, 630–640. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.D.; Milward, M.R.; Cooper, P.R.; Hadis, M.; Palin, W.M. Developments in low level light therapy (LLLT) for dentistry. Dent. Mater. 2014, 30, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Qadri, T.; Miranda, L.; Tunér, J.; Gustafsson, A. The short-term effects of low-level lasers as adjunct therapy in the treatment of periodontal inflammation. J. Clin. Periodontol. 2005, 32, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Coluzzi, D.J.; Convissar, R.A. Lasers in clinical dentistry. Dent. Clin. N. Am. 2004, 48, xi–xii. [Google Scholar] [CrossRef] [PubMed]
- Boschi, E.S.; Leite, C.E.; Saciura, V.C.; Caberlon, E.; Lunardelli, A.; Bitencourt, S.; Melo, D.A.; Oliveira, J.R. Anti-Inflammatory effects of low-level laser therapy (660 nm) in the early phase in carrageenan-induced pleurisy in rat. Lasers Surg. Med. 2008, 40, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Aras, M.H.; Güngörmüş, M. The Effect of Low-Level Laser Therapy on Trismus and Facial Swelling Following Surgical Extraction of a Lower Third Molar. Photomed. Laser Surg. 2009, 27, 21–24. [Google Scholar] [CrossRef]
- Almeida-Lopes, L.; Rigau, J.; Zângaro, R.A.; Guidugli-Neto, J.; Jaeger, M.M.M. Comparison of the low level laser therapy effects on cultured human gingival fibroblasts proliferation using different irradiance and same fluence. Lasers Surg. Med. 2001, 29, 179–184. [Google Scholar] [CrossRef]
- Nomura, K.; Yamaguchi, M.; Abiko, Y. Inhibition of interleukin-1beta production and gene expression in human gingival fibroblasts by low-energy laser irradiation. Lasers Med. Sci. 2001, 16, 218–223. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R.; Carrasco-Labra, A.; Araya, I.; Yanine, N.; Beyene, J.; Shah, P.S. Is Adjuvant Laser Therapy Effective for Preventing Pain, Swelling, and Trismus After Surgical Removal of Impacted Mandibular Third Molars? A Systematic Review and Meta-Analysis. J. Oral Maxillofac. Surg. 2012, 70, 1789–1801. [Google Scholar] [CrossRef]
- Batinjan, G.; Zore, I.F.; Rupić, I.; Jurič, I.B.; Zore, Z.; Pandurić, D.G. Assessing Health-Related Quality of Life with Antimicrobial Photodynamic Therapy (APDT) and Low Level Laser Therapy (LLLT) after Third Molar Removal. J. Lasers Med. Sci. 2013, 4, 120–126. [Google Scholar] [PubMed]
- Aoki, A.; Sasaki, K.M.; Watanabe, H.; Ishikawa, I. Lasers in nonsurgical periodontal therapy. Periodontology 2000 2004, 36, 59–97. [Google Scholar] [CrossRef]
- Mileto, T.N.; Azambuja, F.G. Low-intensity laser efficacy in postoperative extraction of third molars. RGO-Revista Gaúcha de Odontologia 2017, 65, 13–19. [Google Scholar] [CrossRef] [Green Version]
- He, W.L.; Yu, F.Y.; Li, C.J.; Pan, J.; Zhuang, R.; Duan, P.J. A systematic review and meta-analysis on the efficacy of low-level laser therapy in the management of complication after mandibular third molar surgery. Lasers Med. Sci. 2015, 30, 1779–1788. [Google Scholar] [CrossRef] [PubMed]
- Eroglu, C.N.; Tunc, S.K. Effectiveness of Single Session of Low-Level Laser Therapy with a 940 nm Wavelength Diode Laser on Pain, Swelling, and Trismus After Impacted Third Molar Surgery. Photomed. Laser Surg. 2016, 34, 406–410. [Google Scholar] [CrossRef]
- Petrini, M.; Ferrante, M.; Trentini, P.; Perfetti, G.; Spoto, G. Effect of pre-operatory low-level laser therapy on pain, swelling, and trismus associated with third-molar surgery. Medicina Oral Patología Oral y Cirugia Bucal 2017, 22, e467–e472. [Google Scholar] [CrossRef]
- Ferrante, M.; Petrini, M.; Trentini, P.; Perfetti, G.; Spoto, G. Effect of low-level laser therapy after extraction of impacted lower third molars. Lasers Med. Sci. 2013, 28, 845–849. [Google Scholar] [CrossRef]
- Lobo, T.M.; Pol, D.G. Evaluation of the use of a 940 nm diode laser as an adjunct in flap surgery for treatment of chronic periodontitis. J. Indian Soc. Periodontol. 2015, 19, 43–48. [Google Scholar] [CrossRef]
- Simunovic, Z.; Ivankovich, A.D.; Depolo, A. Wound Healing of Animal and Human Body Sport and Traffic Accident Injuries Using Low-Level Laser Therapy Treatment: A Randomized Clinical Study of Seventy-Four Patients with Control Group. J. Clin. Laser Med. Surg. 2000, 18, 67–73. [Google Scholar] [CrossRef] [Green Version]
- Farhadi, F.; Eslami, H.; Majidi, A.; Fakhrzadeh, V.; Ghanizadeh, M.; KhademNeghad, S. Evaluation of adjunctive effect of low-level laser Therapy on pain, swelling and trismus after surgical removal of impacted lower third molar: A double blind randomized clinical trial. Laser Ther. 2017, 26, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Aimbire, F.; Albertini, R.; Pacheco, M.T.; Castro-Faria-Neto, H.C.; Leonardo, P.S.; Iversen, V.V.; Lopes-Martins, R.A.; Bjordal, J.M. Low-level laser therapy induces dose-dependent reduction of TNFalpha levels in acute inflammation. Photomed. Laser Surg. 2006, 24, 33–37. [Google Scholar] [CrossRef] [PubMed]
- De Matos Brunelli Braghin, R.; Libardi, E.C.; Junqueira, C.; Rodrigues, N.C.; Nogueira-Barbosa, M.H.; Renno, A.C.M.; De Abreu, D.C.C. The effect of low-level laser therapy and physical exercise on pain, stiffness, function, and spatiotemporal gait variables in subjects with bilateral knee osteoarthritis: A blind randomized clinical trial. Disabil. Rehabil. 2018, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Wanitphakdeedecha, R.; Iamphonrat, T.; Phothong, W.; Eimpunth, S.; Manuskiatti, W. Local and systemic effects of low-level light therapy with light-emitting diodes to improve erythema after fractional ablative skin resurfacing: A controlled study. Lasers Med. Sci. 2019, 34, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Fan, S.M.-Y.; Cheng, Y.-P.; Lee, M.-Y.; Lin, S.-J.; Chiu, H.-Y. Efficacy and Safety of a Low-Level Light Therapy for Androgenetic Alopecia: A 24-Week, Randomized, Double-Blind, Self-Comparison, Sham Device-Controlled Trial. Dermatol. Surg. 2018, 44, 1411–1420. [Google Scholar] [CrossRef] [PubMed]
- Neves, C.R.; Buskermolen, J.; Roffel, S.; Waaijman, T.; Thon, M.; Veerman, E.; Gibbs, S. Human saliva stimulates skin and oral wound healing in vitro. J. Tissue Eng. Regen. Med. 2019, 13, 1079–1092. [Google Scholar] [Green Version]
- Politis, C.; Schoenaers, J.; Jacobs, R.; Agbaje, J.O. Wound Healing Problems in the Mouth. Front. Physiol. 2016, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Menon, R.; Gopinath, D.; Li, K.; Leung, Y.; Botelho, M. Does the use of amoxicillin/amoxicillin–clavulanic acid in third molar surgery reduce the risk of postoperative infection? A systematic review with meta-analysis. Int. J. Oral Maxillofac. Surg. 2019, 48, 263–273. [Google Scholar] [CrossRef] [PubMed]
- De Souza, T.O.F.; Martins, M.A.T.; Bussadori, S.K.; Fernandes, K.P.S.; Tanji, E.Y.; Mesquita-Ferrari, R.A.; Martins, M.D. Clinical Evaluation of Low-Level Laser Treatment for Recurring Aphthous Stomatitis. Photomed. Laser Surg. 2010, 28, S-85. [Google Scholar] [CrossRef] [PubMed]
- Cafaro, A.; Albanese, G.; Arduino, P.G.; Mario, C.; Massolini, G.; Mozzati, M.; Broccoletti, R. Effect of Low-Level Laser Irradiation on Unresponsive Oral Lichen Planus: Early Preliminary Results in 13 Patients. Photomed. Laser Surg. 2010, 28, S-99. [Google Scholar] [CrossRef] [PubMed]
- Mozzati, M.; Martinasso, G.; Cocero, N.; Pol, R.; Maggiora, M.; Muzio, G.; Canuto, R.A. Influence of Superpulsed Laser Therapy on Healing Processes Following Tooth Extraction. Photomed. Laser Surg. 2011, 29, 565–571. [Google Scholar] [CrossRef]
- Calderin, S.; Garcia-Nunez, J.A.; Gomez, C. Short-term clinical and osteoimmunological effects of scaling and root planing complemented by simple or repeated laser phototherapy in chronic periodontitis. Lasers Med. Sci. 2013, 28, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Amorim, J.C.F.; De Sousa, G.R.; Silveira, L.D.B.; Prates, R.A.; Pinotti, M.; Ribeiro, M.S. Clinical Study of the Gingiva Healing after Gingivectomy and Low-Level Laser Therapy. Photomed. Laser Surg. 2006, 24, 588–594. [Google Scholar] [CrossRef] [Green Version]
- Ozcelik, O.; Haytac, M.C.; Kunin, A.; Seydaoglu, G. Improved wound healing by low-level laser irradiation after gingivectomy operations: A controlled clinical pilot study. J. Clin. Periodontol. 2008, 35, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Weber, J.B.B.; Camilotti, R.S.; Ponte, M.E. Efficacy of laser therapy in the management of bisphosphonate-related osteonecrosis of the jaw (BRONJ): A systematic review. Lasers Med. Sci. 2016, 31, 1261–1272. [Google Scholar] [CrossRef] [PubMed]
- Aras, M.H.; Gungormus, M. Placebo-controlled randomized clinical trial of the effect two different low-level laser therapies (LLLT)-intraoral and extraoral-on trismus and facial swelling following surgical extraction of the lower third molar. Lasers Med. Sci. 2010, 25, 641–645. [Google Scholar] [CrossRef] [PubMed]
- Chaves, M.E.D.A.; De Araújo, A.R.; Piancastelli, A.C.C.; Pinotti, M. Effects of low-power light therapy on wound healing: LASER x LED. An. Bras. Dermatol. 2014, 89, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Karu, T.I.; Pyatibrat, L.V.; Ryabykh, T.P. Nonmonotonic behavior of the dose dependence of the radiation effect on cells in vitro exposed to pulsed laser radiation at lambda 820 nm. Lasers Surg. Med. 1997, 21, 485–492. [Google Scholar] [CrossRef]
- Zare, D.; Haerian, A.; Molla, R.; Vaziri, F. Evaluation of the Effects of Diode (980 Nm) Laser on Gingival Inflammation after Nonsurgical Periodontal Therapy. J. Lasers Med. Sci. 2014, 5, 27–31. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Control (n = 36) | LLLT Once (n = 36) | LLLT Daily (n = 36) |
|---|---|---|---|
| 1 day | 6 | 6 | 6 |
| 2 day | 6 | 6 | 6 |
| 3 day | 6 | 6 | 6 |
| 4 day | 6 | 6 | 6 |
| 5 day | 6 | 6 | 6 |
| 6 day | 6 | 6 | 6 |
| Parameters of Local Clinical Symptoms | Scoring Points |
|---|---|
| Redness | 0: Complete absence of symptom |
| Swelling | 5: Mild |
| Pain | 10: Moderate |
| Incision wound closure | 15: Severe |
| Adverse Event | Control (n = 16) N (%) | LLLT (n = 16) N (%) | p-Value 1) |
|---|---|---|---|
| Yes | 3 (18.75) | 1 (6.25) | 0.5996 |
| No | 13 (81.25) | 15 (93.75) |
| System Organ Class * | Preferred Term | Control (n = 16) N (%) | LLLT (n = 16) N (%) |
|---|---|---|---|
| Gastrointestinal disorders | postoperative pain and swelling | 2 (12.50) | 1 (6.25) |
| Infections and infestations | postoperative infection | 1 (6.25) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choung, H.-W.; Lee, S.-H.; Ham, A.R.; Lee, N.R.; Kim, B.; Pang, K.-M.; Jahng, J.W.; Lee, J.-H. Effectiveness of Low-Level Laser Therapy with a 915 Nm Wavelength Diode Laser on the Healing of Intraoral Mucosal Wound: An Animal Study and a Double-Blind Randomized Clinical Trial. Medicina 2019, 55, 405. https://doi.org/10.3390/medicina55080405
Choung H-W, Lee S-H, Ham AR, Lee NR, Kim B, Pang K-M, Jahng JW, Lee J-H. Effectiveness of Low-Level Laser Therapy with a 915 Nm Wavelength Diode Laser on the Healing of Intraoral Mucosal Wound: An Animal Study and a Double-Blind Randomized Clinical Trial. Medicina. 2019; 55(8):405. https://doi.org/10.3390/medicina55080405
Chicago/Turabian StyleChoung, Han-Wool, Sung-Ho Lee, Ahe Reum Ham, Na Ra Lee, Bongju Kim, Kang-Mi Pang, Jeong Won Jahng, and Jong-Ho Lee. 2019. "Effectiveness of Low-Level Laser Therapy with a 915 Nm Wavelength Diode Laser on the Healing of Intraoral Mucosal Wound: An Animal Study and a Double-Blind Randomized Clinical Trial" Medicina 55, no. 8: 405. https://doi.org/10.3390/medicina55080405