1. Introduction
Dry eye disease (DED) is arguably the most common ocular disease presenting to the eye care professional, affecting approximately one of every four patients in an ophthalmologist’s office. As a progressive condition, and if left without treatment, it can lead to vision loss, ocular surface damage, discomfort, and overall reduction in quality of life [
1,
2,
3]. DED is treated primarily by topical lubricants, immunomodulation with cyclosporine, lifitegrast and corticosteroids, oral nutrition with omega-3s, antibiotics, lid hygiene, and a variety of punctal and canalicular plugs (occluders) [
1,
2,
3]. Punctal occluders are particularly effective in patients with aqueous insufficiency and DED, because they prevent outflow of tears through the punctum and preserve the natural tear lake [
4]. Punctal occluders can be permanent, with an exposed flange that rests on the surface of the punctum, or temporary and dissolvable when placed within the punctum [
5].
Biofilm formation has been reported in the literature as an ongoing problem with the clinical use of occluders, leading to infection, inflammation, and intolerance [
6]. First coined by William J. Costerson in 1978, the term “biofilm” describes “surface-attached microbial agglomerations”, or a capsular polysaccharide enabling bacteria to attach to a device [
7] Within the biofilm, bacteria produce extracellular polymeric substances (EPS) that include extracellular polysaccharides, proteins, lipids, and DNA. One of these proteins is adhesin, which facilitates the adhesion of the biofilm to a surface, which, in turn, prevents the colony from being dislodged into the environment [
8]. The scaffold of the biofilm not only insulates bacteria from anti-infectives, disinfectant systems, and even our own white cells, but also facilitates further bacterial adhesion and colonization [
7,
8,
9,
10].
S. aureus is an excellent example that demonstrates this [
11]. Our study examined the formation of biofilms in vitro on three popular silicone-based punctal occluders using
S. aureus. This strain was chosen because
S. aureus is the most common bacteria found on punctal occluders [
12], and also because it is known for biofilm formation on ophthalmic devices [
13]. In addition,
S. aureus can also cause corneal ulceration [
14]. Dynamic microbial cultures, histological staining, and SEM were all used to investigate the bacterial colonization and biofilm formation on the three types of occluders.
2. Materials and Methods
2.1. Bacteria Strains
The bacterial strain, Staphylococcus aureus (#10390), was purchased from American Tissue Culture Collection (ATCC, Manassas, VA, USA). Bacteria were streaked on nutrient broth agar plates and incubated overnight at 37 °C. A single colony was selected and grown in 3 mL of nutrient broth overnight in a shaking 37 °C incubator to establish the liquid cultures.
2.2. Punctal Occluders
Three different types of punctal occluders were used in this study from the following manufacturers: Delta Life Sciences
R (Comfortear
R), Odyssey Medical
R (Parasol
R), and Alphamed
R (Quintess
R). All were hydrophobic silicone-based and measuring 0.9 mm in greatest diameter (
Figure 1) [
5]. The length of each occluder was approximately 2 mm. Light microscopy was performed on all three punctal occluders and all three have a flat head, a thin neck, a thick cone-shaped base, and a central lumen (
Figure 1).
2.3. Occluder Exposure to Bacteria
Each occluder type (n = 4 for each type) was placed individually in 5 mL of nutrient broth containing growing S. aureus cells. The culture were placed in a shaking 37 °C incubator. Every morning, for the next seven days, 5 mL of the growing bacteria were removed and replaced with an equal amount of fresh nutrient broth so that the existing bacteria would continue to grow. The total time that all occluders were exposed to the bacteria was seven days.
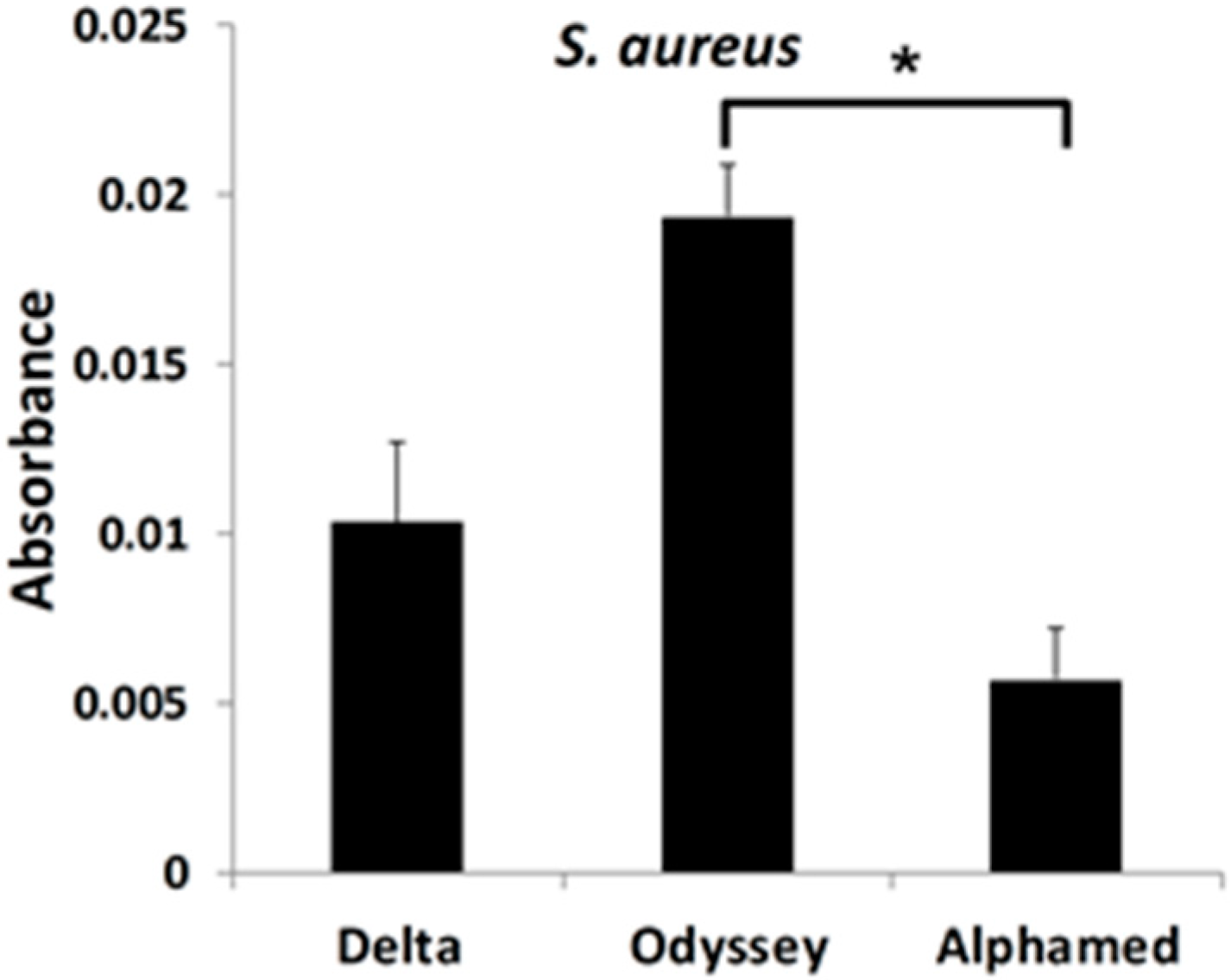
2.4. Bacteria Biofilm Quantitation
Following seven days of continued exposure to the dynamically growing bacterial cells, the occluders (n = 3 for each type; another one was used for SEM, see below) were removed from the cultures and placed in a microcentrifuge tube. Following three washes with distilled water (300 μL each time), 50 μL of 0.1% crystal violet was added, and then incubated overnight at Room Temperature (RT). The same procedure was done with unused (n = 3 for each type). Following staining, the crystal violet was eluted by rinsing the stained occluders three times with distilled water (300 μL each time), followed by the addition of 95% ethanol (20 μL) and incubation for 15 min at RT. Finally, the eluted crystal violet from each occluder (both experimental and unused control) was measured in a spectrophotometer at an OD (Optical Density) of 600 nm. The OD from the control samples was subtracted from the experimental values before the data was plotted.
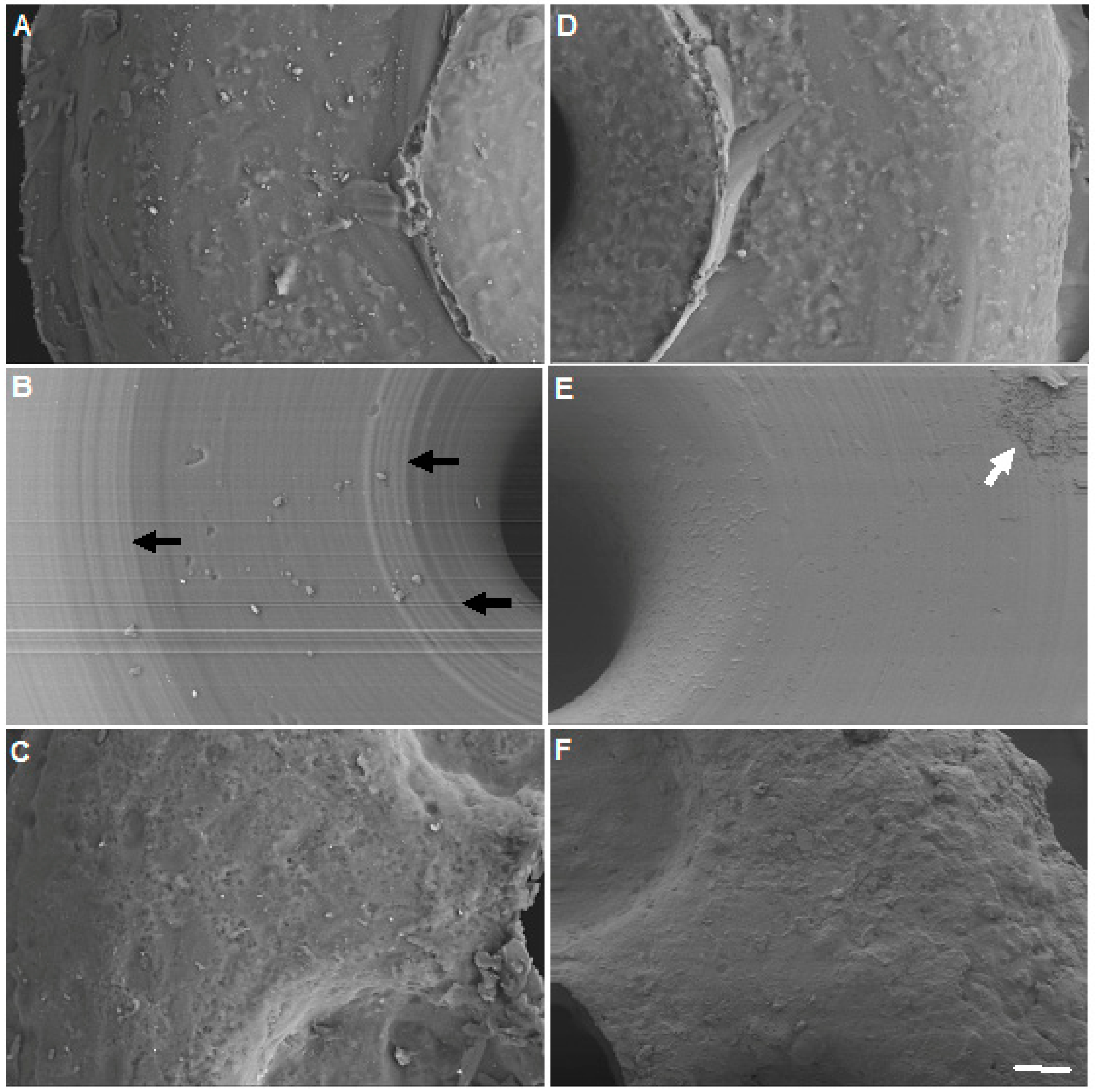
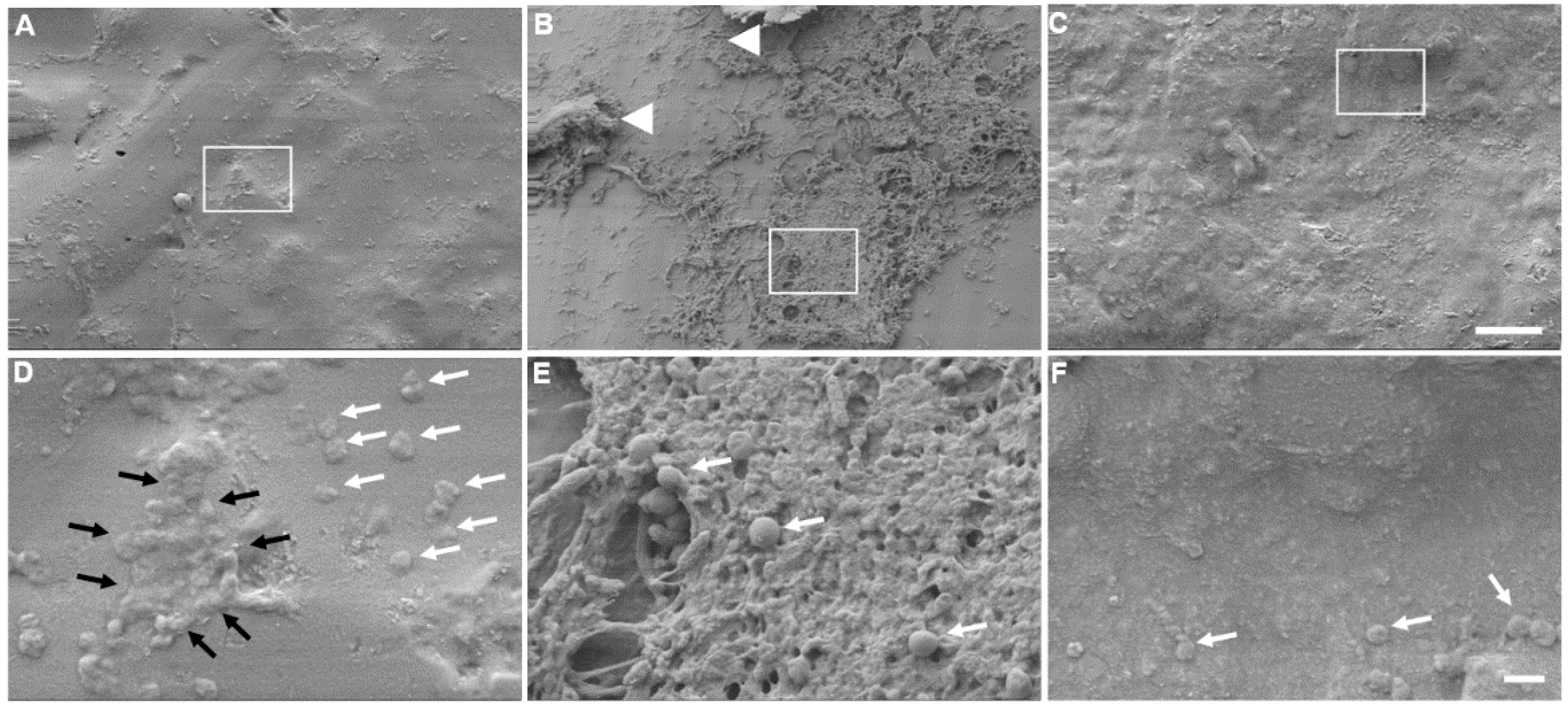
2.5. Scanning Electron Microscopy (SEM)
The presence of bacteria and overall biofilm formation on each of the three different types of occluders was evaluated by SEM. Prior to SEM, each occluder was washed three times (5 min each time) in 1× Phosphate Buffer Saline (PBS). The occluders were then dehydrated serially in alcohol washes, as follows: 70%, 80%, 90% (15 min at RT) and 100% (three times for 15 min at RT). Images were obtained on a LEO 1550 Field Emission Scanning Electron Microscope (Carl Zeiss AG, Oberkochen, Germany), with a Schottky Field Emission Gun, at an acceleration voltage of 20 kV and a Robinson Back Scatter Detector. Occluders were gold coated to prevent charging effects.
2.6. Statistical Analysis
For the spectrophotometric data of bacterial colonization/quantification, each type of occluder was tested in triplicate and the results are presented as group mean +/− standard deviation (SD). The significance of the results was determined using the Kruskal–Wallis nonparametric ANOVA for multiple comparisons. The significance for all tests was p < 0.05. The statistical software package SPSS 22 for Windows (version 22, SPSS, Chicago, IL, USA) was used for data analysis.
4. Discussion
The primary defense of most bacteria is the formation of a biofilm. Staphylococcal bacteria characteristically are found in biofilms. Because biofilms are found on any surface with moisture and nutrients present, ranging from freezing glaciers to boiling hot springs, it should not be surprising that they are found growing on occluders. In this study, we demonstrated the growth of S. aureus on all three occluder types. As bacterial infection is a rare but serious complication of punctal plug insertion, these findings lend credence to the possibility of occluders being the source for recurrent conjunctival and canalicular infections due to biofilm adhesion, and, in addition, may allow for a faster re-accumulation of biofilm on eyelids that have undergone a mechanical or electromechanical therapeutic lid scrub. In essence, the occluders would act as a nidus for biofilm reformation with cloistered colonies of S. aureus.
Previous studies demonstrated a strong causal relationship between
S. aureus nasal colonization and increased risk of infection [
11]. As the lacrimal duct connects to the nares, it is likely that this increased risk of infection extends to the tear duct. In a retrospective study evaluating the microbiologic spectrum of dacryocystitis,
S. aureus was the most commonly cultured species, followed by
S. epidermitis and
S. viridans. Gram negative bacteria, such as
P. aeruginosa, were far less common [
13].
S. aureus and
S. epidermidis are also the most frequent causes of nosocomial infection on indwelling medical devices [
15]. Sugita et al. evaluated punctal occluders with SEM and cultured material extracted from plugs in 21 patients, finding positive culture results in 44%, isolating
S. epidermidis in 75% of these and
S. aureus in 25% [
12]. Earlier, Yokoi et al. also found widespread bacterial colonization of
S. haemolyticus and
C. tropicalis on a removed punctal plug from a 63-year-old woman diagnosed as having tear-deficient type dry eye and treated with a punctal plug for several months [
16]. Similarly,
P. aeruginosa is notorious for causing chronic infection, particularly as the chief cause of corneal ulcer in contact lens wearers [
17,
18,
19].
It is not clear why a statistically significant difference was found in the quantity of bacterial growth on the Odyssey
R occluder when compared with the Alphamed
R. All of the occluders are made of silicone, and none were treated with any additional coatings. However, as the largest amount of bacteria was found on the Odyssey
R, its smoother (al be it with grooves) texture does not appear to have affected biofilm formation. When comparing occluder shapes, the Odyssey
R has a collapsible nose that was designed to open inside the puncta, fitting the shape of the tear duct much like an umbrella unfolds (likely giving rise to its name, “Parasol”) [
5]. It is possible that pooling of material within this umbrella-like cavity lead to a statistically significant difference in the quantity of bacteria when compared with the other two occluders. Further, all three punctal occluders were made of 100% silicone, but there was no documentation of their relative hydrophobicity or surface charge. Collectively, these factors are all known to play a role in bacteria-surface interactions.
Texture was considered as a differentiating factor and explored by SEM, revealing, at least qualitatively, the Odyssey
R as the smoothest but with circular grooves. The surprising evidence that the smoother surface occluder seemed to potentiate biofilm development might be explained by the mechanism of biofilm migration, which occurs via detachment, dispersal, rolling, and rippling. While one would not expect the detachment and dispersal to be affected by the roughness of the surface, rolling and rippling could indeed be affected and impeded by a rougher surface, similar to a hiker having more difficulty with a rough or mountainous terrain vs. a smooth flat terrain. Moreover, it is well established that bacterial adhesion is greater in grooved and braided materials as compared to flat ones due to increased surface area [
20,
21,
22]. However, Katsikogianni and Missirlis [
23] suggested that bacteria adhere preferentially to surface irregularities that resemble those of their size, since this maximizes bacteria-surface area. According to the authors, grooves or scratches that are on order of bacterial size increase the contact area and hence the binding potential [
23]. It is conceivable then, that the Odyssey
R occluder with the visible regular grooves may serve as a desirable surface for
S. aureus biofilm formation. Clearly, additional research is needed to further probe the exact size of the grooves that were observed on the Odyssey
R occluder.
There is new evidence that biofilm may play a significant role in dry eye disease with a unified theory that was proposed by Rynerson and Perry [
2]. They suggest that bacterial biofilm coats the lid margin, creating inflammation that affects not only the Meibomian glands but also the lacrimal gland as well. This theory, known as DEBS (Dry Eye Blepharitis Syndrome), may lead to both evaporative and aqueous insufficiency, as the natural sequelae of decades of chronic blepharitis. Dry eye may be, in part, a late form and late manifestation of blepharitis. It is well known that bacteria colonize the lid margin with biofilm. The biofilm allows for population densities that initiate quorum-sensing gene activation. These newly activated gene products consist of inflammatory virulence factors, such as exotoxins, cytolytic toxins, and super-antigens. It may also be possible that punctal occluders may play a role in increasing inflammation to the lid margin by being a potent source of biofilm formation.
In conclusion, bacterial growth and biofilm is found on punctal occluders. The role of biofilm formation on these punctal occluders is not known but it may play a role in ocular surface inflammation. Unfortunately, there are not sufficient case reports or studies to prove a clinical difference between these three occluders. In addition, there is no evidence, case reports or studies to prove a differential exists clinically between these three occluders. As this was only an in vitro study, further evaluation of punctal occluders in relation to bacterial adherence, biofilm formation, as well as DED in vivo is warranted.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




