Osteopontin in the Cerebrospinal Fluid of Patients with Severe Aneurysmal Subarachnoid Hemorrhage

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting and Patients
2.2. Experimental Analysis
2.3. Statistical Analysis
3. Results
3.1. Patients
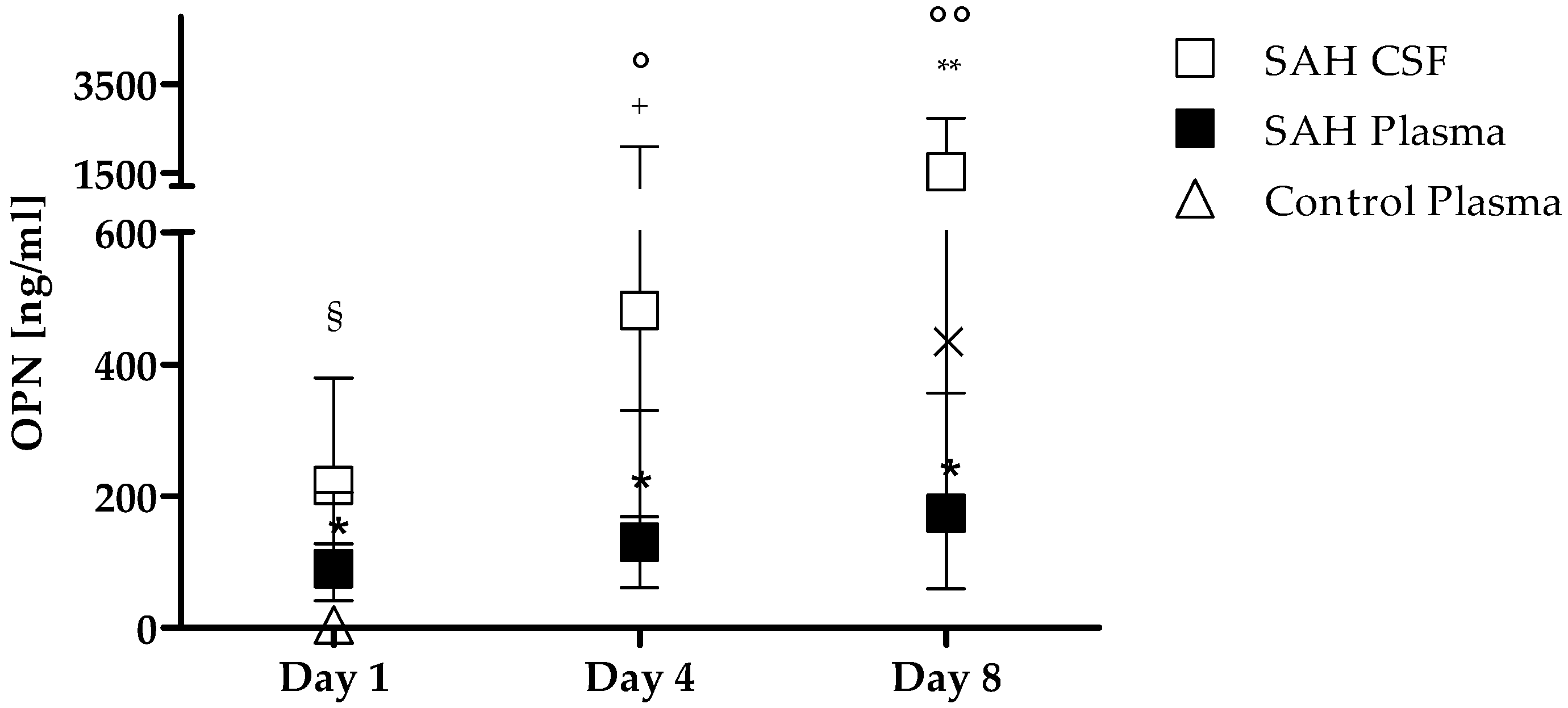
3.2. OPN Levels in Plasma and CSF
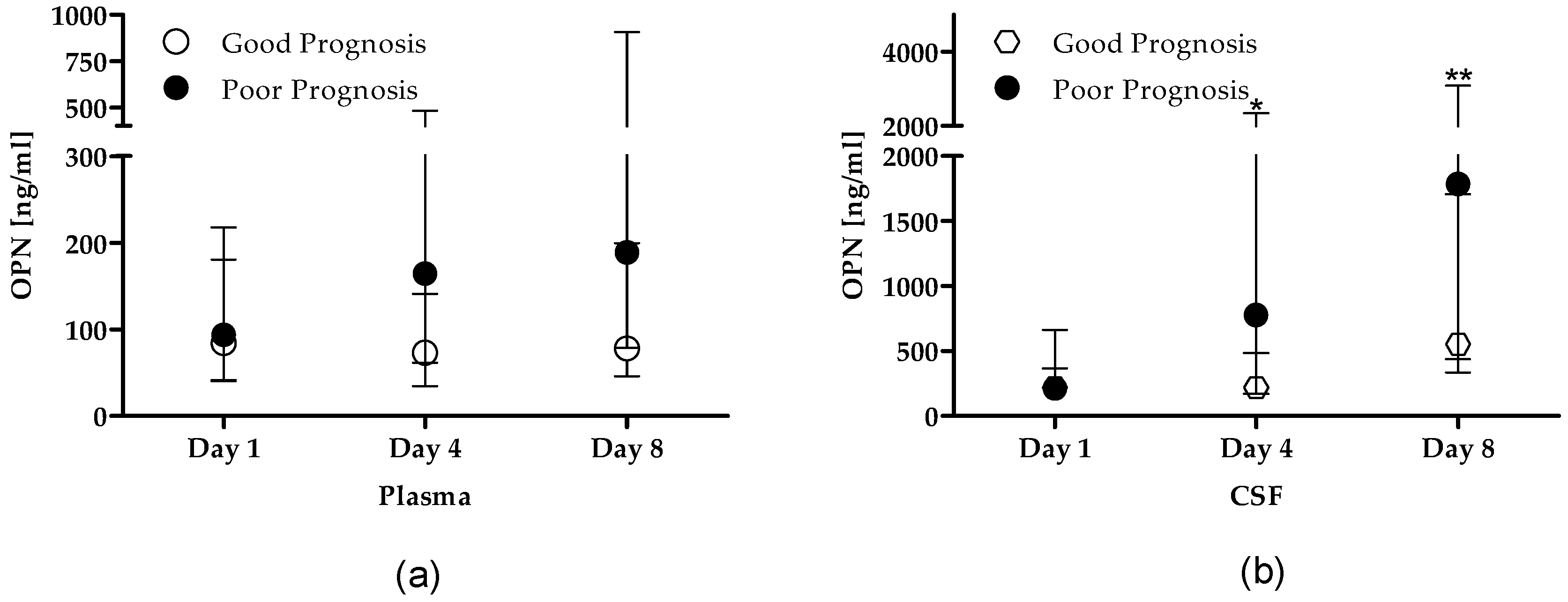
3.3. OPN Levels Stratified by Prognosis
3.4. OPN Levels as Independent Predictors of Poor Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Suarez, J.I.; Tarr, R.W.; Selman, W.R. Aneurysmal subarachnoid hemorrhage. N. Engl. J. Med. 2006, 354, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Ostrowski, R.P.; Colohan, A.R.; Zhang, J.H. Molecular mechanisms of early brain injury after subarachnoid hemorrhage. Neurol. Res. 2006, 28, 399–414. [Google Scholar] [CrossRef] [PubMed]
- Caner, B.; Hou, J.; Altay, O.; Fujii, M.; Zhang, J.H. Transition of research focus from vasospasm to early brain injury after subarachnoid hemorrhage. J. Neurochem. 2012, 123 (Suppl. 2), 12–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucke-Wold, B.P.; Logsdon, A.F.; Manoranjan, B.; Turner, R.C.; McConnell, E.; Vates, G.E.; Huber, J.D.; Rosen, C.L.; Simard, J.M. Aneurysmal Subarachnoid Hemorrhage and Neuroinflammation: A Comprehensive Review. Int. J. Mol. Sci. 2016, 17, 497. [Google Scholar] [CrossRef] [PubMed]
- Ross, F.P.; Chappel, J.; Alvarez, J.I.; Sander, D.; Butler, W.T.; Farach-Carson, M.C.; Mintz, K.A.; Robey, P.G.; Teitelbaum, S.L.; Cheresh, D.A. Interactions between the bone matrix proteins osteopontin and bone sialoprotein and the osteoclast integrin alpha v beta 3 potentiate bone resorption. J. Biol. Chem. 1993, 268, 9901–9907. [Google Scholar] [PubMed]
- Patarca, R.; Freeman, G.J.; Singh, R.P.; Wei, F.Y.; Durfee, T.; Blattner, F.; Regnier, D.C.; Kozak, C.A.; Mock, B.A.; Morse, H.C., III; et al. Structural and functional studies of the early T lymphocyte activation 1 (Eta-1) gene. Definition of a novel T cell-dependent response associated with genetic resistance to bacterial infection. J. Exp. Med. 1989, 170, 145–161. [Google Scholar] [CrossRef] [PubMed]
- Clemente, N.; Raineri, D.; Cappellano, G.; Boggio, E.; Favero, F.; Soluri, M.F.; Dianzani, C.; Comi, C.; Dianzani, U.; Chiocchetti, A. Osteopontin Bridging Innate and Adaptive Immunity in Autoimmune Diseases. J. Immunol. Res. 2016, 2016, 7675437. [Google Scholar] [CrossRef] [PubMed]
- Marcondes, M.C.; Poling, M.; Watry, D.D.; Hall, D.; Fox, H.S. In vivo osteopontin-induced macrophage accumulation is dependent on CD44 expression. Cell. Immunol. 2008, 254, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castello, L.M.; Raineri, D.; Salmi, L.; Clemente, N.; Vaschetto, R.; Quaglia, M.; Garzaro, M.; Gentilli, S.; Navalesi, P.; Cantaluppi, V.; et al. Osteopontin at the Crossroads of Inflammation and Tumor Progression. Mediat. Inflamm. 2017, 2017, 4049098. [Google Scholar] [CrossRef] [PubMed]
- Wolak, T. Osteopontin—A multi-modal marker and mediator in atherosclerotic vascular disease. Atherosclerosis 2014, 236, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Castello, L.M.; Baldrighi, M.; Molinari, L.; Salmi, L.; Cantaluppi, V.; Vaschetto, R.; Zunino, G.; Quaglia, M.; Bellan, M.; Gavelli, F.; et al. The Role of Osteopontin as a Diagnostic and Prognostic Biomarker in Sepsis and Septic Shock. Cells 2019, 8, 174. [Google Scholar] [CrossRef] [PubMed]
- Vaschetto, R.; Nicola, S.; Olivieri, C.; Boggio, E.; Piccolella, F.; Mesturini, R.; Damnotti, F.; Colombo, D.; Navalesi, P.; Della, C.F.; et al. Serum levels of osteopontin are increased in SIRS and sepsis. Intensive Care Med. 2008, 34, 2176–2184. [Google Scholar] [CrossRef] [PubMed]
- Vaschetto, R.; Navalesi, P.; Clemente, N.; Boggio, E.; Valsecchi, S.; Olivieri, C.; Soluri, M.F.; Kroumova, V.; Fonio, P.; Dinatale, C.; et al. Osteopontin induces soluble urokinase-type plasminogen activator receptor production and release. Minerva Anestesiol. 2015, 81, 157–165. [Google Scholar] [PubMed]
- Bandopadhyay, M.; Bulbule, A.; Butti, R.; Chakraborty, G.; Ghorpade, P.; Ghosh, P.; Gorain, M.; Kale, S.; Kumar, D.; Kumar, S.; et al. Osteopontin as a therapeutic target for cancer. Expert Opin. Ther. Targets 2014, 18, 883–895. [Google Scholar] [CrossRef] [PubMed]
- Chabas, D.; Baranzini, S.E.; Mitchell, D.; Bernard, C.C.; Rittling, S.R.; Denhardt, D.T.; Sobel, R.A.; Lock, C.; Karpuj, M.; Pedotti, R.; et al. The influence of the proinflammatory cytokine, osteopontin, on autoimmune demyelinating disease. Science 2001, 294, 1731–1735. [Google Scholar] [CrossRef] [PubMed]
- Shin, Y.J.; Kim, H.L.; Choi, J.S.; Choi, J.Y.; Cha, J.H.; Lee, M.Y. Osteopontin: Correlation with phagocytosis by brain macrophages in a rat model of stroke. Glia 2011, 59, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Hasegawa, Y.; Kanamaru, K.; Zhang, J.H. Mechanisms of osteopontin-induced stabilization of blood–brain barrier disruption after subarachnoid hemorrhage in rats. Stroke 2010, 41, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Hasegawa, Y.; Chen, W.; Kanamaru, K.; Zhang, J.H. Recombinant osteopontin in cerebral vasospasm after subarachnoid hemorrhage. Ann. Neurol. 2010, 68, 650–660. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, H.; Ayer, R.; Sugawara, T.; Chen, W.; Sozen, T.; Hasegawa, Y.; Kanamaru, K.; Zhang, J.H. Protective effects of recombinant osteopontin on early brain injury after subarachnoid hemorrhage in rats. Crit. Care Med. 2010, 38, 612–618. [Google Scholar] [CrossRef] [PubMed]
- Topkoru, B.C.; Altay, O.; Duris, K.; Krafft, P.R.; Yan, J.; Zhang, J.H. Nasal administration of recombinant osteopontin attenuates early brain injury after subarachnoid hemorrhage. Stroke 2013, 44, 3189–3194. [Google Scholar] [CrossRef]
- Nakatsuka, Y.; Shiba, M.; Nishikawa, H.; Terashima, M.; Kawakita, F.; Fujimoto, M.; Suzuki, H. Acute-Phase Plasma Osteopontin as an Independent Predictor for Poor Outcome After Aneurysmal Subarachnoid Hemorrhage. Mol. Neurobiol. 2018, 55, 6841–6849. [Google Scholar] [CrossRef] [PubMed]
- Carbone, F.; Vuilleumier, N.; Burger, F.; Roversi, G.; Tamborino, C.; Casetta, I.; Seraceni, S.; Trentini, A.; Padroni, M.; Dallegri, F.; et al. Serum osteopontin levels are upregulated and predict disability after an ischaemic stroke. Eur. J. Clin. Investig. 2015, 45, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Mendioroz, M.; Fernandez-Cadenas, I.; Rosell, A.; Delgado, P.; Domingues-Montanari, S.; Ribo, M.; Penalba, A.; Quintana, M.; Alvarez-Sabin, J.; Montaner, J. Osteopontin predicts long-term functional outcome among ischemic stroke patients. J. Neurol. 2011, 258, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Tambuyzer, B.R.; Casteleyn, C.; Vergauwen, H.; Van, C.S.; Van, G.C. Osteopontin alters the functional profile of porcine microglia in vitro. Cell Biol. Int. 2012, 36, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Zohar, R.; Suzuki, N.; Suzuki, K.; Arora, P.; Glogauer, M.; McCulloch, C.A.; Sodek, J. Intracellular osteopontin is an integral component of the CD44-ERM complex involved in cell migration. J. Cell. Physiol. 2000, 184, 118–130. [Google Scholar] [CrossRef]
- Iczkiewicz, J.; Rose, S.; Jenner, P. Increased osteopontin expression following intranigral lipopolysaccharide injection in the rat. Eur. J. Neurosci. 2005, 21, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Liu, X.; Zhong, Y. The Effect of Osteopontin on Microglia. BioMed Res. Int. 2017, 2017, 1879437. [Google Scholar] [CrossRef] [PubMed]
- Vlachogiannis, P.; Hillered, L.; Khalil, F.; Enblad, P.; Ronne-Engstrom, E. Interleukin-6 Levels in Cerebrospinal Fluid and Plasma in Patients with Severe Spontaneous Subarachnoid Hemorrhage. World Neurosurg. 2019, 122, e612–e618. [Google Scholar] [CrossRef]
- Hopkins, S.J.; McMahon, C.J.; Singh, N.; Galea, J.; Hoadley, M.; Scarth, S.; Patel, H.; Vail, A.; Hulme, S.; Rothwell, N.J.; et al. Cerebrospinal fluid and plasma cytokines after subarachnoid haemorrhage: CSF interleukin-6 may be an early marker of infection. J. Neuroinflamm. 2012, 9, 255. [Google Scholar] [CrossRef]
- Tarkowski, E.; Rosengren, L.; Blomstrand, C.; Wikkelso, C.; Jensen, C.; Ekholm, S.; Tarkowski, A. Early intrathecal production of interleukin-6 predicts the size of brain lesion in stroke. Stroke 1995, 26, 1393–1398. [Google Scholar] [CrossRef]
- Niwa, A.; Osuka, K.; Nakura, T.; Matsuo, N.; Watabe, T.; Takayasu, M. Interleukin-6, MCP-1, IP-10, and MIG are sequentially expressed in cerebrospinal fluid after subarachnoid hemorrhage. J. Neuroinflamm. 2016, 13, 217. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.H.; Kellner, C.P.; Hahn, D.K.; Desantis, B.M.; Musabbir, M.; Starke, R.M.; Rynkowski, M.; Komotar, R.J.; Otten, M.L.; Sciacca, R.; et al. Monocyte chemoattractant protein-1 predicts outcome and vasospasm following aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2008, 109, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Rodriguez, A.; Egea-Guerrero, J.J.; Ruiz, D.A.-L.; Murillo-Cabezas, F. Biomarkers of vasospasm development and outcome in aneurysmal subarachnoid hemorrhage. J. Neurol. Sci. 2014, 341, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.K.; Dong, X.Q.; Du, Q.; Wang, H.; Yang, D.B.; Zhu, Q.; Che, Z.H.; Shen, Y.F.; Jiang, L.; Hu, W.; et al. Comparison of plasma copeptin and multiple biomarkers for assessing prognosis of patients with aneurysmal subarachnoid hemorrhage. Clin. Chim. Acta 2017, 475, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, K.L.; Czosnyka, M.; Jalloh, I.; Newcombe, V.F.; Helmy, A.; Shannon, R.J.; Budohoski, K.P.; Kolias, A.G.; Kirkpatrick, P.J.; Carpenter, T.A.; et al. Systemic, local, and imaging biomarkers of brain injury: More needed, and better use of those already established? Front. Neurol. 2015, 6, 26. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Good Prognosis mRS 0–2 n = 7 | Poor Prognosis mRS 3–6 n = 37 | All n = 44 | p Value |
|---|---|---|---|---|
| Age, median (IQ) | 52 (46–68) | 60 (51–70) | 60 (50–69) | 0.480 |
| Gender, Female | 5 (71%) | 23 (62%) | 28 (64%) | 1.000 |
| Ruptured aneurysm location | 1.000 | |||
| Anterior communicating artery and Anterior cerebral artery | 2 (29%) | 11 (30%) | 13 (30%) | |
| Internal carotid artery | 1 (14%) | 7 (19%) | 8 (18%) | |
| Middle cerebral artery | 2 (29%) | 10 (27%) | 12 (27%) | |
| Posterior circulation | 2 (29%) | 9 (24%) | 11 (25%) | |
| Coiling, n (%) | 7 (100%) | 27 (73%) | 34 (77%) | 0.177 |
| Preoperative WFNS grades 4 –5, n (%) | 4 (57%) | 32 (86%) | 36 (82%) | 0.100 |
| Fisher grade 4, n (%) | 5 (71%) | 26 (70%) | 31 (70%) | 1.000 |
| GCS | 11 (11–14) | 6 (4–8) | 6 (4–11) | 0.005 |
| ICU-LOS | 15 (13–21) | 20 (9–30) | 16 (11–28) | 0.656 |
| Hospital-LOS | 20 (14–21) | 26 (10–32) | 23 (11–30) | 0.610 |
| Vasospasm at day 4 (yes/no) | 1/6 | 5/26 | 6/32 | 0.514 |
| Vasospasm at day 8 (yes/no) | 2/5 | 12/18 | 14/23 | 0.477 |
| Vasospasm after day 8 (yes/no) | 2/5 | 8/22 | 10/27 | 0.612 |
| ICU mortality | 0 | 15 (40%) | 15 (34%) | 0.077 |
| Parameters | OR | 95%CI | p Value |
|---|---|---|---|
| Gender (Male vs. Female) | 2.07 | 0–16963.21 | 0.87 |
| Plasma OPN at day 1 | 1.03 | 1.01–1.04 | <0.001 |
| Plasma OPN at day 4 | 1.12 | 1.11–1.14 | <0.001 |
| Plasma OPN at day 8 | 1.00 | 0.99–1.02 | 0.56 |
| Gender (Male vs. Female) | 1.35 | 0–48895.24 | 0.95 |
| CSF OPN at day 1 | 0.99 | 0.99–1.01 | 0.99 |
| CSF OPN at day 4 | 1.00 | 1.00–1.00 | 0.97 |
| CSF OPN at day 8 | 1.00 | 1.00–1.00 | 0.99 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abate, M.G.; Moretto, L.; Licari, I.; Esposito, T.; Capuano, L.; Olivieri, C.; Benech, A.; Brucoli, M.; Avanzi, G.C.; Cammarota, G.; et al. Osteopontin in the Cerebrospinal Fluid of Patients with Severe Aneurysmal Subarachnoid Hemorrhage. Cells 2019, 8, 695. https://doi.org/10.3390/cells8070695
Abate MG, Moretto L, Licari I, Esposito T, Capuano L, Olivieri C, Benech A, Brucoli M, Avanzi GC, Cammarota G, et al. Osteopontin in the Cerebrospinal Fluid of Patients with Severe Aneurysmal Subarachnoid Hemorrhage. Cells. 2019; 8(7):695. https://doi.org/10.3390/cells8070695
Chicago/Turabian StyleAbate, Maria Giulia, Lorenza Moretto, Ilaria Licari, Teresa Esposito, Lorenzo Capuano, Carlo Olivieri, Arnaldo Benech, Matteo Brucoli, Gian Carlo Avanzi, Gianmaria Cammarota, and et al. 2019. "Osteopontin in the Cerebrospinal Fluid of Patients with Severe Aneurysmal Subarachnoid Hemorrhage" Cells 8, no. 7: 695. https://doi.org/10.3390/cells8070695