
COVID-19 Vaccine Acceptance: A Case Study from Nepal


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Study Design, Population, and Sampling
2.3. Measures
2.4. Data Analysis and Vaccine Acceptance
3. Results
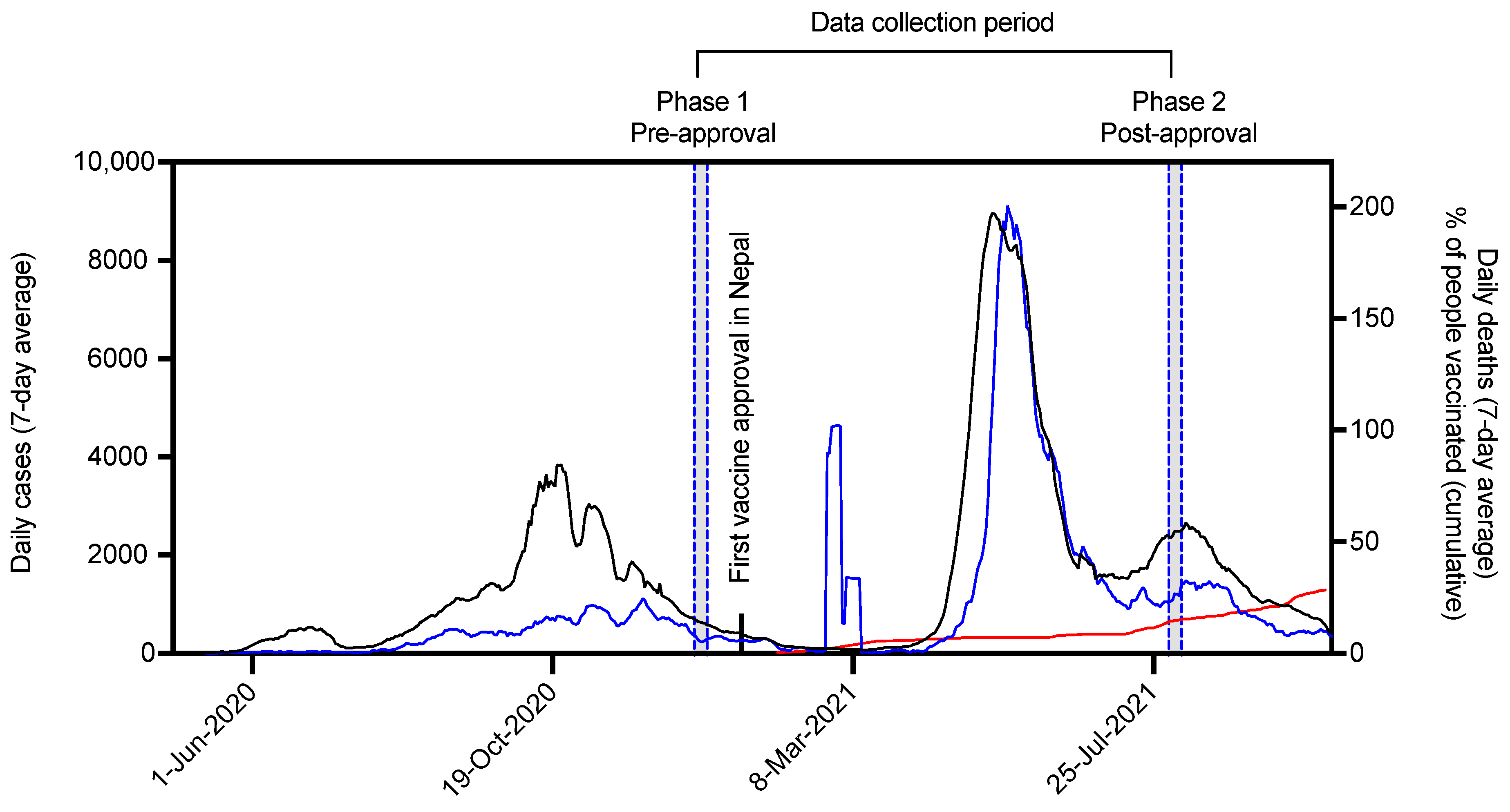
3.1. Current Scenario of COVID-19 Cases, Deaths, Vaccination, and Vaccine Approval in Nepal
3.2. Study Sample Characteristics and Perceived Impact of COVID-19
3.3. COVID-19 Vaccine Acceptance and Attitudes towards the Vaccine
3.4. Factors Associated with Accepting a COVID-19 Vaccine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, M.; Zhang, X.; Qu, J. Coronavirus disease 2019 (COVID-19): A clinical update. Front. Med. 2020, 14, 126–135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pun, S.B.; Mandal, S.; Bhandari, L.; Jha, S.; Rajbhandari, S.; Mishra, A.K.; Sharma Chalise, B.; Shah, R. Understanding COVID-19 in Nepal. J. Nepal Health Res. Counc. 2020, 18, 126–127. [Google Scholar] [CrossRef] [PubMed]
- Panthee, B.; Dhungana, S.; Panthee, N.; Paudel, A.; Gyawali, S.; Panthee, S. COVID-19: The current situation in Nepal. New Microbes New Infect. 2020, 37, 100737. [Google Scholar] [CrossRef]
- Panthee, B.; Dhungana, S.; Panthee, N.; Gyawali, S.; Paudel, A.; Panthee, S. Clinical and epidemiological features of COVID-19 deaths in Nepal. New Microbes New Infect. 2020, 38, 100797. [Google Scholar] [CrossRef] [PubMed]
- GC, S.; Khanal, A.; Paudel, A.; GC, V.S.; Khanal, A.; Panthee, S. Comparative analysis of COVID-19 case fatality rate between two waves in Nepal. Influenza Other Respir. Viruses 2022, 16, :186–189. [Google Scholar] [CrossRef]
- Ministry of Health and Population. COVID-19 Dashboard. 2021. Available online: https://covid19.mohp.gov.np/ (accessed on 1 July 2022).
- Sharma, O.; Sultan, A.A.; Ding, H.; Triggle, C.R. A Review of the Progress and Challenges of Developing a Vaccine for COVID-19. Front. Immunol. 2020, 11, 585354. [Google Scholar] [CrossRef]
- Ball, P. The lightning-fast quest for COVID vaccines - and what it means for other diseases. Nature 2021, 589, 16–18. [Google Scholar] [CrossRef]
- Goodman, J.L.; Grabenstein, J.D.; Braun, M.M. Answering Key Questions About COVID-19 Vaccines. JAMA 2020, 324, 2027–2028. [Google Scholar] [CrossRef]
- Solis Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Nichter, M. Vaccinations in the Third World: A consideration of community demand. Soc. Sci. Med. 1995, 41, 617–632. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Hasell, J.; Mathieu, E.; Beltekian, D.; Macdonald, B.; Giattino, C.; Ortiz-Ospina, E.; Roser, M.; Ritchie, H. A cross-country database of COVID-19 testing. Sci. Data 2020, 7, 345. [Google Scholar] [CrossRef] [PubMed]
- Malik, A.; Malik, J.; Ishaq, U. Acceptance of COVID-19 vaccine in Pakistan among health care workers. PLoS ONE 2021, 16, e0257237. [Google Scholar] [CrossRef] [PubMed]
- Zawahrah, H.J.; Saca-Hazboun, H.; Melhem, S.S.; Adwan, R.; Sabateen, A.; Abu-Rmeileh, N.M.E. Acceptance of COVID-19 vaccines in Palestine: A cross-sectional online study. BMJ Open 2021, 11, e053681. [Google Scholar] [CrossRef]
- Wong, L.P.; Alias, H.; Danaee, M.; Ahmed, J.; Lachyan, A.; Cai, C.Z.; Lin, Y.; Hu, Z.; Tan, S.Y.; Lu, Y.; et al. COVID-19 vaccination intention and vaccine characteristics influencing vaccination acceptance: A global survey of 17 countries. Infect. Dis. Poverty 2021, 10, 122. [Google Scholar] [CrossRef]
- Jones, D.L.; Salazar, A.S.; Rodriguez, V.J.; Balise, R.R.; Starita, C.U.; Morgan, K.; Raccamarich, P.D.; Montgomerie, E.; Nogueira, N.F.; Barreto Ojeda, I.; et al. Severe Acute Respiratory Syndrome Coronavirus 2: Vaccine Hesitancy Among Underrepresented Racial and Ethnic Groups With HIV in Miami, Florida. Open Forum Infect. Dis. 2021, 8, ofab154. [Google Scholar] [CrossRef]
- Hawlader, M.D.H.; Rahman, M.L.; Nazir, A.; Ara, T.; Haque, M.M.A.; Saha, S.; Barsha, S.Y.; Hossian, M.; Matin, K.F.; Siddiquea, S.R.; et al. Belief, Attitude, and Intention to take COVID-19 Vaccine among South Asian Population: A Multi-country Study. Int. J. Infect. Dis. 2021, 114, 1–10. [Google Scholar] [CrossRef]
- Ripabelli, G.; Tamburro, M.; Buccieri, N.; Adesso, C.; Caggiano, V.; Cannizzaro, F.; Di Palma, M.A.; Mantuano, G.; Montemitro, V.G.; Natale, A.; et al. Active Surveillance of Adverse Events in Healthcare Workers Recipients After Vaccination with COVID-19 BNT162b2 Vaccine (Pfizer-BioNTech, Comirnaty): A Cross-Sectional Study. J. Community Health 2022, 47, 211–225. [Google Scholar] [CrossRef]
- Kennedy, J. Vaccine Hesitancy: A Growing Concern. Paediatr. Drugs 2020, 22, 105–111. [Google Scholar] [CrossRef]
- Wake, A.D. The Willingness to Receive COVID-19 Vaccine and Its Associated Factors: “Vaccination Refusal Could Prolong the War of This Pandemic”—A Systematic Review. Risk Manag. Healthc. Policy 2021, 14, 2609–2623. [Google Scholar] [CrossRef] [PubMed]
- Gidengil, C.; Lieu, T.A.; Payne, K.; Rusinak, D.; Messonnier, M.; Prosser, L.A. Parental and societal values for the risks and benefits of childhood combination vaccines. Vaccine 2012, 30, 3445–3452. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Wagner, A.L.; Ji, J.; Huang, Z.; Zikmund-Fisher, B.J.; Boulton, M.L.; Ren, J.; Prosser, L.A. A conjoint analysis of stated vaccine preferences in Shanghai, China. Vaccine 2020, 38, 1520–1525. [Google Scholar] [CrossRef] [PubMed]
- Kerekes, S.; Ji, M.; Shih, S.F.; Chang, H.Y.; Harapan, H.; Rajamoorthy, Y.; Singh, A.; Kanwar, S.; Wagner, A.L. Differential Effect of Vaccine Effectiveness and Safety on COVID-19 Vaccine Acceptance across Socioeconomic Groups in an International Sample. Vaccines 2021, 9, 1010. [Google Scholar] [CrossRef]
- Hatmal, M.M.; Al-Hatamleh, M.A.I.; Olaimat, A.N.; Hatmal, M.; Alhaj-Qasem, D.M.; Olaimat, T.M.; Mohamud, R. Side Effects and Perceptions Following COVID-19 Vaccination in Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for Predicting Severity of Side Effects. Vaccines 2021, 9, 556. [Google Scholar] [CrossRef]


{kind=link}
| SN | Vaccine Platform | Type of Candidate Vaccine | Doses and Schedule | Developers | Phase | Approved in Nepal |
|---|---|---|---|---|---|---|
| 1 | Viral vector (Non-replicating) | ChAdOx1-S -(AZD1222) Vaxzevria Covishield | 1–2 Day 0 + 28 | AstraZeneca + University of Oxford | 4 | 15 January 2021 |
| 2 | Inactivated virus | Inactivated SARS-CoV-2 vaccine (Vero cell), vaccine name BBIBP-CorV | 2 Day 0 + 21 | Sinopharm + China National Biotec Group Co + Beijing Institute of Biological Products | 4 | 16 February 2021 |
| 3 | Inactivated virus | Whole-Virion Inactivated SARS-CoV-2 Vaccine (BBV152); Covaxin | 2 Day 0 + 14 | Bharat Biotech International Limited | 3 | 19 March 2021 |
| 4 | Viral vector (Non-replicating) | Gam-COVID-Vac Adeno-based (rAd26-S+rAd5-S) Sputnik V | 2 Day 0 + 21 | Gamaleya Research Institute; Health Ministry of the Russian Federation | 3 | 20 April 2021 |
| 5 | Inactivated virus | CoronaVac; inactivated SARS-CoV-2 vaccine (vero cell) | 2 Day 0 + 14 | Sinovac Research and Development Co., Ltd. | 4 | 4 June 2021 |
| 6 | Viral vector (Non-replicating) | Ad26.COV2.S | 1–2 Day 0 or Day 0 + 56 | Janssen PharmaceuticalJohnson & Johnson | 4 | 30 June 2021 |
| 7 | RNA-based | BNT162b2 (3 LNP-mRNAs) “Comirnaty” | 2 Day 0 + 21 | Pfizer/BioNTech + Fosun Pharma | 4 | 8 September 2021 |
| 8 | RNA-based | mRNA-1273 | 2 Day 0 + 28 | Moderna + National Institute of Allergy and Infectious Diseases (NIAID) | 4 | 15 September 2021 |
| Variables | Phase 1 (Pre-Approval) | Phase 2 (Post-Approval) | χ2 | p | ||
|---|---|---|---|---|---|---|
| Frequency | % | Frequency | % | |||
| Age | ||||||
| 18–30 | 418 | 72.6 | 171 | 71.0 | 0.97 | 0.61 |
| 31–40 | 99 | 17.2 | 48 | 19.9 | ||
| >40 | 59 | 10.2 | 22 | 9.1 | ||
| Gender | ||||||
| Female | 274 | 47.6 | 108 | 44.8 | 0.51 | 0.47 |
| Male | 302 | 52.4 | 133 | 55.2 | ||
| Religion | ||||||
| Hindu | 558 | 96.9 | 235 | 97.5 | 0.24 | 0.40 |
| Others (Muslim, Buddhist, Kirat, Christian) | 18 | 3.1 | 6 | 2.5 | ||
| Ethnicity | ||||||
| Brahmin/Chhetri | 374 | 64.9 | 156 | 64.7 | 0.12 | 0.93 |
| Madhesi | 102 | 17.7 | 41 | 17.0 | ||
| Janjati and Dalit | 100 | 17.4 | 44 | 18.3 | ||
| Marital status | ||||||
| Married | 184 | 31.9 | 92 | 38.2 | 2.94 | 0.08 |
| Unmarried | 392 | 68.1 | 149 | 61.8 | ||
| Highest level of education | ||||||
| Basic and secondary | 61 | 10.6 | 41 | 17 | 10.37 | 0.00 |
| Higher secondary | 160 | 27.8 | 78 | 32.4 | ||
| Undergraduate and above | 355 | 61.6 | 122 | 50.6 | ||
| Health status | ||||||
| Fair, poor, very poor | 66 | 11.5 | 38 | 15.8 | 2.84 | 0.09 |
| Good, very good | 510 | 88.5 | 203 | 84.2 | ||
| Main occupation | ||||||
| Agriculture | 64 | 11.1 | 35 | 14.5 | 7.34 | 0.11 |
| Business | 62 | 10.8 | 33 | 13.7 | ||
| Health care students and staff | 239 | 41.5 | 94 | 39 | ||
| Non-medical students | 143 | 24.8 | 44 | 18.3 | ||
| Office worker | 68 | 11.8 | 35 | 14.5 | ||
| Current area of residence | ||||||
| Province 1 | 68 | 11.8 | 34 | 14.1 | 41.2 | 0.00 |
| Province 2 | 45 | 7.8 | 31 | 12.9 | ||
| Bagmati | 169 | 29.3 | 45 | 18.7 | ||
| Gandaki | 42 | 7.3 | 36 | 14.9 | ||
| Lumbini | 181 | 31.4 | 45 | 18.7 | ||
| Karnali | 38 | 6.6 | 27 | 11.2 | ||
| Sudurpaschim | 33 | 5.7 | 23 | 9.5 | ||
| Monthly income (NPR) | ||||||
| <10,000 | 65 | 11.3 | 13 | 5.4 | 33.2 | 0.00 |
| 10,000–20,000 | 114 | 19.8 | 27 | 11.2 | ||
| 21,000–30,000 | 151 | 26.2 | 46 | 19.1 | ||
| 31,000–40,000 | 113 | 19.6 | 70 | 29 | ||
| >40,000 | 133 | 23.1 | 85 | 35.3 | ||
| Perceived risk | ||||||
| Less or very less | 100 | 17.4 | 28 | 11.6 | 17.24 | 0.00 |
| Fair | 320 | 55.6 | 113 | 46.9 | ||
| Large or very large | 156 | 27.1 | 100 | 41.5 | ||
| Pandemic impact on daily life | ||||||
| Small or very small | 72 | 12.5 | 16 | 6.7 | 7.8 | 0.02 |
| Fair | 345 | 59.9 | 143 | 59.3 | ||
| Large or very large | 159 | 27.6 | 82 | 34 | ||
| Pandemic impact on Work | ||||||
| Small or very small | 72 | 12.5 | 19 | 7.9 | 4.41 | 0.11 |
| Fair | 255 | 44.3 | 120 | 49.8 | ||
| Large or very large | 249 | 43.2 | 102 | 42.3 | ||
| Pandemic impact on Income | ||||||
| Small or very small | 94 | 16.3 | 34 | 14.1 | 1.52 | 0.46 |
| Fair | 263 | 45.7 | 121 | 50.2 | ||
| Large or very large | 219 | 38 | 86 | 35.7 | ||
| Total | 576 | 100 | 241 | 100 | ||
| Variables | Phase 1 (Pre-Approval) | Phase 2 (Post-Approval) | χ2 | p | ||
|---|---|---|---|---|---|---|
| Frequency | % | Frequency | % | |||
| Vaccine acceptance | ||||||
| Yes | 540 | 93.8 | 237 | 98.3 | 7.69 | 0.00 |
| No | 36 | 6.3 | 4 | 1.7 | ||
| If yes, when? | ||||||
| As soon as possible | 232 | 43 | 208 | 86.3 | 127.26 | 0.00 |
| Later | 308 | 57 | 33 | 13.7 | ||
| Vaccination is an effective way | ||||||
| Agree | 506 | 87.8 | 231 | 95.9 | 12.32 | 0.00 |
| Disagree | 70 | 12.2 | 33 | 13.7 | ||
| Convenience is an important factor | ||||||
| Yes | 544 | 94.4 | 233 | 96.7 | 1.82 | 0.17 |
| No | 32 | 5.6 | 8 | 3.3 | ||
| Price is an important factor | ||||||
| Agree | 454 | 78.8 | 192 | 79.7 | 0.07 | 0.78 |
| Disagree | 122 | 21.2 | 49 | 20.3 | ||
| COVID-19 vaccine might have mild side effects | ||||||
| Agree | 441 | 76.6 | 231 | 95.9 | 43.30 | 0.00 |
| Disagree | 135 | 23.4 | 10 | 4.1 | ||
| Participation in vaccine clinical trial | ||||||
| Agree | 184 | 31.9 | 66 | 27.4 | 1.66 | 0.19 |
| Disagree | 392 | 68.1 | 175 | 72.6 | ||
| Willing to get vaccine if it was free | ||||||
| Willing (probably and definitely) | 565 | 98.1 | - | - | - | - |
| Not sure/ not willing | 11 | 1.9 | ||||
| Agree to pay for the vaccine | ||||||
| Yes | 334 | 58 | 88 | 36.5 | 31.37 | 0.00 |
| No | 242 | 42 | 153 | 63.5 | ||
| If yes, how much (NPR)? | ||||||
| Less than 100 | 30 | 9 | 28 | 31.8 | 31.89 | 0.00 |
| 100–1999 | 237 | 71 | 51 | 58 | ||
| Greater than 2000 | 67 | 20.1 | 9 | 10.2 | ||
| Variables | Vaccine Acceptance | χ2 | p | |
|---|---|---|---|---|
| Yes n(%) | No n(%) | |||
| Age | ||||
| 18–30 | 400(95.7) | 18(4.3) | 13.24 | 0.00 |
| 31–40 | 85 (85.9) | 14 (14.1) | ||
| >40 | 55 (93.2) | 4 (6.8) | ||
| Gender | ||||
| Female | 253 (92.3) | 21 (7.7) | 1.78 | 0.18 |
| Male | 287 (95) | 15 (5) | ||
| Marital status | ||||
| Married | 161 (87.5) | 23 (12.5) | 18.02 | 0.00 |
| Unmarried | 379 (96.7) | 13 (3.3) | ||
| Highest level of education | ||||
| Basic and secondary | 50 (82) | 11 (18) | 29.35 | 0.00 |
| Higher secondary | 143 (89.4) | 17 (10.6) | ||
| Undergraduate and above | 347 (97.7) | 8 (2.3) | ||
| Health status | ||||
| Fair, poor, very poor | 63 (95.5) | 3 (4.5) | 0.40 | 0.52 |
| Good, very good | 477 (93.5) | 33 (6.5) | ||
| Main occupation | ||||
| Agriculture | 60 (93.8) | 4 (6.2) | 25.5 | 0.00 |
| Business | 50 (80.6) | 12 (19.4) | ||
| Health care students and staff | 234 (97.9) | 5 (2.1) | ||
| Non-medical students | 133 (93) | 10 (7) | ||
| Office worker | 63 (92.6) | 5 (7.4) | ||
| Current area of residence | ||||
| Province 1 | 68(100) | 0(0) | 76.66 | 0.00 |
| Province 2 | 44 (97.8) | 1 (2.2) | ||
| Bagmati | 166 (98.2) | 3 (1.8) | ||
| Gandaki | 38 (90.5) | 4 (9.5) | ||
| Lumbini | 173 (95.6) | 8 (4.4) | ||
| Karnali | 25 (65.8) | 13 (34.2) | ||
| Sudurpaschim | 26 (78.8) | 7 (21.2) | ||
| Monthly income (NPR) | ||||
| <10,000 | 59 (90.8) | 6 (9.2) | 3.32 | 0.50 |
| 10,000–20,000 | 104 (91.2) | 10 (8.8) | ||
| 21,000–30,000 | 143 (94.7) | 8 (5.3) | ||
| 31,000–40,000 | 108 (95.6) | 5 (4.4) | ||
| >40,000 | 126 (94.7) | 7 (5.3) | ||
| Perceived risk | ||||
| Less or very less | 89 (89) | 11 (11) | 4.66 | 0.09 |
| Fair | 303 (94.7) | 17 (5.3) | ||
| Large or very large | 148 (94.9) | 8 (5.1) | ||
| Pandemic impact on daily life | ||||
| Small or very small | 64 (88.9) | 8 (11.1) | 4.89 | 0.08 |
| Fair | 329 (57.1) | 16 (4.6) | ||
| Large or very large | 147 (92.5) | 12 (7.5) | ||
| Pandemic impact on Work | ||||
| Small or very small | 61 (84.7) | 11 (15.3) | 11.50 | 0.00 |
| Fair | 243 (95.3) | 12 (4.7) | ||
| Large or very large | 236 (94.8) | 13 (5.2) | ||
| Pandemic impact on Income | ||||
| Small or very small | 88 (93.6) | 6 (6.4) | 5.79 | 0.059 |
| Fair | 253 (96.2) | 10 (3.8) | ||
| Large or very large | 199 (90.9) | 20 (9.1) | ||
| COVID-19 vaccination is an effective way to prevent and control COVID-19 | ||||
| Agree | 483 (95.5) | 23 (4.5) | 20.64 | 0.00 |
| Disagree | 57 (81.4) | 13 (18.6) | ||
| Vaccine Convenience is an important factor | ||||
| Yes | 518 (95.2) | 26 (4.8) | 36.14 | 0.00 |
| No | 22 (68.8) | 10 (31.3) | ||
| The COVID-19 vaccine might have side effects such as fever or soreness in the arm | ||||
| Agree | 419 (95) | 22 (5) | 5.10 | 0.02 |
| Disagree | 121 (89.6) | 14 (10.4) | ||
| I would be willing to participate in a clinical trial for the coronavirus (COVID-19) vaccine | ||||
| Agree | 181 (98.4) | 3 (1.6) | 9.84 | 0.00 |
| Disagree | 359 (91.6) | 33 (8.4) | ||
| Do you agree to pay for the COVID-19 vaccine? | ||||
| Agree | 327 (97.9) | 7 (2.1) | 23.41 | 0.00 |
| Disagree | 213 (88.0) | 29 (12) | ||
| If yes, how much (NPR)? | ||||
| Less than 100 | 23 (76.7) | 7 (23.3) | 72.45 | 0.00 |
| 100–1999 | 237 (100) | 0 (0) | ||
| Greater than 2000 | 67 (100) | 0 (0) | ||
| Total | 540(93.8) | 36(6.2) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaire, A.; Panthee, B.; Basyal, D.; Paudel, A.; Panthee, S. COVID-19 Vaccine Acceptance: A Case Study from Nepal. COVID 2022, 2, 1014-1025. https://doi.org/10.3390/covid2080075
Gaire A, Panthee B, Basyal D, Paudel A, Panthee S. COVID-19 Vaccine Acceptance: A Case Study from Nepal. COVID. 2022; 2(8):1014-1025. https://doi.org/10.3390/covid2080075
Chicago/Turabian StyleGaire, Amrit, Bimala Panthee, Deepak Basyal, Atmika Paudel, and Suresh Panthee. 2022. "COVID-19 Vaccine Acceptance: A Case Study from Nepal" COVID 2, no. 8: 1014-1025. https://doi.org/10.3390/covid2080075
APA StyleGaire, A., Panthee, B., Basyal, D., Paudel, A., & Panthee, S. (2022). COVID-19 Vaccine Acceptance: A Case Study from Nepal. COVID, 2(8), 1014-1025. https://doi.org/10.3390/covid2080075