1. Introduction
The control of blood pressure (BP) is crucial, making regular BP monitoring a significant concern. According to the World Health Organization (WHO) [
1], 17.9 million people die each year from cardiovascular illnesses. The American Society of Anesthesiologists (ASA) has outlined basic anesthetic monitoring criteria [
2], recommending blood pressure checks every 5 min to ensure the patient’s circulatory system functions properly.
According to the ASA, blood pressure should be taken every 5 min to ensure the proper functioning of the patient’s circulatory system. Typically, BP is represented through three essential readings, including systolic, diastolic, and mean pressure, which are defined as follows: the pressure imposed on the walls of blood arteries by blood at the conclusion of systolic ventricular contraction is known as systolic blood pressure (SBP); the pressure imposed on the blood vessel walls at the conclusion of diastole, or relaxation, is known as diastolic blood pressure (DBP); and the pressure that determines the average rate of blood flow through systemic arteries is known as mean pressure.
Continuous arterial blood pressure (ABP) represents the gold standard of BP monitoring; however, it is difficult to measure in routine clinical practice because it is performed via arterial cannulation by a trained operator. Auscultatory, oscillometry, tonometry, and volume clamping methods are commonly used in traditional BP monitoring.
Traditional blood pressure monitoring techniques have two main drawbacks. Firstly, they require special instruments that may not be available to everyone. Secondly, these methods are not always suitable for babies and elderly individuals. As a result, using existing technologies is challenging, as they are unsafe for high-rate usage. Frequent use of cuff-based BP monitoring at a high rate can cause a measurement error due to the deterioration of the mechanical parts. Hence, continuous BP monitoring cannot be effectively carried out through traditional non-invasive approaches.
Recently, photoplethysmography (PPG) signals have been leveraged for continuous BP monitoring through simple wearable devices [
3,
4,
5] through simple wearable devices [
6]. PPG signal represents changes in blood volume in the skin blood vessels by tracking fine variations in the absorbed/reflected infrared light intensity due to blood pulsation. These changes not only explain blood volume but also provide information on blood flow and red blood cell orientation.
Thanks to the publicly available MIMIC II dataset (Multi-parameter Intelligent Monitoring in Intensive Care) [
7], which provides joint PPG–ABP data along with electrocardiogram (ECG) signals. Numerous research efforts have been dedicated to inferring the relationship between PPG and BP based on these available datasets through machine learning [
8,
9,
10,
11,
12,
13] and deep-learning techniques [
14,
15,
16,
17,
18,
19].
In this paper, we propose an efficient approach for beat-by-beat BP estimation from PPG signals utilizing different feature extraction methods and deep learning techniques. Different learning scenarios are carried out in this study: (1) estimation of ABP beats from the corresponding PPG beats, and (2) estimation of BP values (SBP and DBP) from the corresponding PPG beats.
Section 2 discusses recently published BP estimation methods, the motivation, and challenges of BP estimation, and finally it presents the contributions of our study.
Section 3 presents the datasets and preprocessing techniques used in the study.
Section 4 explains the proposed method.
Section 5 presents the results of the proposed method.
Section 6 summarizes the study and highlights some lines of our future work.
2. Related Works
Recently, several BP estimation methods have been proposed in the literature, leveraging machine and deep learning techniques. Literature in the field of BP monitoring can be categorized into two main groups: BP estimation and ABP waveform reconstruction. These clusters are based on both PPG and ECG signals.
For example, the authors in the work presented in [
13] extracted features from contact PPG to train a neural network for BP determination. This system has undergone experimentation on patients. In [
14], deep learning networks have been evaluated for BP estimation based on both contact PPG and camera-based remote PPG (rPPG) signals. A spectro-temporal deep neural network is employed to estimate BP in [
15]. The authors used the MIMIC III database to train the network after many prepossessing operations. The authors used the MIMIC II database [
7] to train the network after many prepossessing operations. The experimental results showed that the mean absolute errors were 9.43 and 6.88 for SBP and DBP, respectively.
Instead of using a single PPG sensor approach, two sensors were employed to estimate BP in [
17,
20,
21,
22,
23,
24]. In the work presented in [
23], the authors suggested using the pulse transit time (PTT) and pulse arrival time (PAT) with the PPG signal that is collected using the contact method to find the blood pressure. The time it takes for a pressure wave to transition between two artery sites is known as the PTT. Authors in the work presented in [
23] investigated the relationship between BP and PTT in various scenarios. The pulse arrival time is the amount of time that elapses between when the heart is electrically stimulated and when the pulse wave reaches a certain location on the body (PAT). To rephrase, PAT is the combination of the PTT plus the isovolumic contraction duration and ventricular electromechanical delay, collectively termed as the pre-ejection period (PEP) delay. PAT is still employed in the literature because of its simplicity even though it has been discovered that it can lower diastolic pressure accuracy.
In addition to using a cuffless method, pulse wave velocity (PWV) can be used to estimate blood pressure as well. This strategy is based on the hypothesis that BP may be roughly estimated from the speed of the heartbeat pulse. In the work presented in [
21], the authors confirmed the relationship between PWV and SBP by experiments applied to 63 volunteers. Jointly using two kinds of signals, ECG and PPG signals, this method is not recommended because it needs signals from two different sensors. Also, the estimated signals in this scheme need more refinements to be clearer. In the work presented in [
25], a scheme to convert the PPG signal to the ABP signal has been introduced using the federated learning approach. The simulation results explained that the mean absolute error was improved to reach 2.54 mmHg. In contrast, the standard deviation was 23.7 mmHg for the mean arterial blood pressure.
In the work presented in [
26], a unique blood pressure estimation technique based on the feature of PPG signals using LSTM and PCA was presented. The raw PPG signals were employed to extract 12 time-domain features. Moreover, ten features were extracted from the raw PPG signals using principal component analysis (PCA). By using the long short-term memory network (LSTM) model, all sets of features were merged to produce 22 features for blood pressure estimation. The LSTM model was adopted to implement a waveform-based technique for continuous BP measurement from ECG and PPG waveforms [
27]. The model had two layers: one artificial neural network (ANN) that trained the features from signal sound waves and another LSTM that created the temporal correlation between the relatively low hierarchy’s extracted features with output SBP and DBP values. This model’s performance is highly dependent on the ECG and PPG cycles. A hybrid CNN-RNN model is adopted as well to estimate BP from PPG signals. In [
28], a phase network is proposed for BP estimation. The first phase preferred two CNNs to extract features from PPG segments before estimating the systolic and diastolic blood pressures independently. The second phase applied LSTM to capture temporal dependencies. In this model CNN network is used as a feature extractor and LSTM is used as the BP estimator.
On the other hand, the ABP waveform is approximated using two deep learning models [
17]. An approximation network, which is a one-dimensional U-Net network fed with PPG and ECG signals, was first used to estimate the waveform. Then, an iterative network to resolve the estimated BP waveforms is employed. Then, ABP is used to calculate SBP and DBP by finding the maximum and minimum values of the ABP signal, respectively. In another research [
29], a 1D V-Net deep learning algorithm for BP waveform prediction is used. The model is fed with two signals (ECG and PPG). The main problem is that the model necessitates a large amount of input variables as well as noninvasive blood pressure indicators.
Furthermore, the work presented in [
30] explored the use of a cycle generative adversarial network (Cycle GAN) to assess BP waveforms employing PPG data. The authors estimated the waveforms using a transformer and a convolutional network, using data from the same subject for training and testing, which may impact the realism of the results.
5. Experimental Results and Discussion
In this section, the results of BP from PPG are reported according to two learning scenarios: (1) Per-beat continuous PPG-to-ABP learning, and (2) Per-beat discrete PPG-to-SBP/DBP learning scheme. These scenarios are shown in
Figure 6, while the detailed network configurations are described in
Table 1 and
Table 2. Based on these two learning scenarios, we are interested in studying the impact of the feature extraction stage on the overall performance. So, different feature extractors are used besides WST.
The dataset which is cleaned in the work presented in [
32] is used. It is the same as that in MIMIC II [
31] after cleaning using the cleaning criteria. It was split into training, validation, and test sets on a beat basis to prevent contamination of the validation and test set by training data.
The total number of beats in the training phase is 175,660 beats; 90% of these beats (158,094 beats) are used for training and 10% of these beats (17,566 beats) are used for validation. In the testing phase, 17,566 beats are used for testing.
We used the mean absolute error (MAE) metric to assess the performance of all methods. We determined the prediction errors for the full dataset.
The segmented PPG beats are normalized to be in the range [0–1] by using the following equation.
where S
n is the normalized signal and S is the un-normalized beat. The normalized beats are then normalized in time to be with a fixed length of 120. The time interval is used as a feature besides the normalized beats. The corresponding ABP signals are also divided into beats, however, the ABP beats are only normalized in terms of time and not amplitude. The complete ABP beat represents the label for the first scenario, while only its maxima (SBP) and minima (DBP) points are utilized for labeling in the second scenario.
For the two tested scenarios, beat-by-beat is used in training, validation, and testing rather than signals, the input to the LSTM network is a beat (or corresponding feature domain representation) with a length of 120 in addition to BI (in the case of time domain features) as tabulated in
Table 2. In the first scenario, ABP estimation, the output is a sequence with a size equal to 120 × 1 for all feature domains. On the other hand, in the second BP estimation scenario, the output is two values that are the SBP and the DBP, for all feature domains.
Author Contributions
Conceptualization, O.A.O., M.S., A.M.H., N.S. and Y.S.; Methodology, O.A.O., M.S., A.M.H., N.S. and Y.S.; Software, O.A.O. and M.S.; Validation, O.A.O., M.S., A.M.H., N.S. and Y.S.; Formal analysis, O.A.O., M.S., A.M.H. and N.S.; Investigation, O.A.O., M.S., A.M.H. and N.S.; Resources, O.A.O. and M.A.-N.; Data curation, O.A.O. and M.S.; Writing—original draft, O.A.O. and M.S.; Writing—review & editing, O.A.O., M.S., M.A.-N., N.S. and Y.S.; Visualization, O.A.O.; Supervision, M.A.-N. and O.A.O.; Project administration, M.A.-N. and O.A.O.; Funding acquisition, M.A.-N. and O.A.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The authors declare that the manuscript consists of the public dataset for PPG signals and does not include any human or animal studies. Our cleaned dataset will be made available to those concerned upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab (accessed on 5 March 2022).
- American Society of Anesthesiologists. Standards of the American Society of Anesthesiologists: Standards for Basic Anesthetic Monitoring. 2020. Available online: https://www.asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring (accessed on 1 October 2023).
- Martínez, G.; Howard, N.; Abbott, D.; Lim, K.; Ward, R.; Elgendi, M. Can photoplethysmography replace arterial blood pressure in the assessment of blood pressure? J. Clin. Med. 2018, 7, 316. [Google Scholar] [CrossRef]
- Panula, T.; Sirkia, J.-P.; Wong, D.; Kaisti, M. Advances in non-invasive blood pressure measurement techniques. IEEE Rev. Biomed. Eng. 2022, 16, 424–438. [Google Scholar] [CrossRef]
- Moraes, J.; Rocha, M.; Vasconcelos, G.; Filho, J.V.; De Albuquerque, V.; Alexandria, A. Advances in photopletysmography signal analysis for biomedical applications. Sensors 2018, 18, 1894. [Google Scholar] [CrossRef] [PubMed]
- Le, T.; Ellington, F.; Lee, T.Y.; Vo, K.; Khine, M.; Krishnan, S.K.; Dutt, N.; Cao, H. Continuous non-invasive blood pressure monitoring: A methodological review on measurement techniques. IEEE Access 2020, 8, 212478–212498. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2020, 101, e215–e220. [Google Scholar]
- Slapničar, G.; Luštrek, M.; Marinko, M. Continuous blood pressure estimation from PPG signal. Informatica 2018, 42, 33–42. [Google Scholar]
- Haddad, S.; Boukhayma, A.; Caizzone, A. Continuous ppg-based blood pressure monitoring using multi-linear regression. IEEE J. Biomed. Health Inform. 2021, 26, 2096–2105. [Google Scholar]
- Yan, W.-R.; Peng, R.-C.; Zhang, Y.-T.; Ho, D. Cuffless continuous blood pressure estimation from pulse morphology of photoplethysmograms. IEEE Access 2019, 7, 141970–141977. [Google Scholar] [CrossRef]
- Khalid, S.; Zhang, J.; Chen, F.; Zheng, D. Blood pressure estimation using photoplethysmography only: Comparison between different machine learning approaches. J. Healthc. Eng. 2018, 2018, 1548647. [Google Scholar] [CrossRef] [PubMed]
- Maqsood, S.; Xu, S.; Tran, S.; Garg, S.; Springer, M.; Karunanithi, M.; Mohawesh, R. A survey: From shallow to deep machine learning approaches for blood pressure estimation using biosensors. Expert Syst. Appl. 2022, 197, 116788. [Google Scholar]
- Xing, X.; Sun, M. Optical blood pressure estimation with photoplethysmography and FFT-based neural networks. Biomed. Opt. Express 2016, 7, 3007–3020. [Google Scholar] [CrossRef]
- Schrumpf, F.; Frenzel, P.; Aust, C.; Osterhoff, G.; Fuchs, M. Assessment of deep learning based blood pressure prediction from PPG and rPPG signals. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Nashville, TN, USA, 20–25 June 2021; pp. 3820–3830. [Google Scholar]
- Slapničar, G.; Mlakar, N.; Luštrek, M. Blood pressure estimation from photoplethysmogram using a spectro-temporal deep neural network. Sensors 2019, 19, 3420. [Google Scholar] [CrossRef] [PubMed]
- Harfiya, L.; Chang, C.-C.; Li, Y.-H. Continuous blood pressure estimation using exclusively photopletysmography by LSTM-based signal-to-signal translation. Sensors 2021, 21, 2952. [Google Scholar] [CrossRef] [PubMed]
- Ibtehaz, N.; Mahmud, S.; Chowdhury, M.E.H.; Khandakar, A.; Salman Khan, M.; Ayari, M.A.; Tahir, A.M.; Rahman, M.S. PPG2ABP: Translating Photoplethysmogram (PPG) Signals to Arterial Blood Pressure (ABP) Waveforms. Bioengineering 2022, 9, 692. [Google Scholar] [CrossRef]
- Hsu, Y.-C.; Li, Y.-H.; Chang, C.-C.; Harfiya, L.N. Generalized deep neural network model for cuffless blood pressure estimation with photoplethysmogram signal only. Sensors 2020, 20, 5668. [Google Scholar] [CrossRef]
- Schrumpf, F.; Frenzel, P.; Aust, C.; Osterhoff, G.; Fuchs, M. Assessment of Non-Invasive Blood Pressure Prediction from PPG and rPPG Signals Using Deep Learning. Sensors 2021, 21, 6022. [Google Scholar] [CrossRef]
- McCombie, D.B.; Reisner, A.T.; Asada, H.H. Adaptive blood pressure estimation from wearable PPG sensors using peripheral artery pulse wave velocity measurements and multi-channel blind identification of local arterial dynamics. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August 2006–3 September 2006; pp. 3521–3524. [Google Scholar]
- Gesche, H.; Grosskurth, D.; Küchler, G.; Patzak, A. Continuous blood pressure measurement by using the pulse transit time: Comparison to a cuff-based method. Eur. J. Appl. Physiol. 2012, 112, 309–315. [Google Scholar] [CrossRef]
- Kachuee, M.; Kiani, M.M.; Mohammadzade, H.; Shabany, M. Cuff-less high-accuracy calibration-free blood pressure estimation using pulse transit time. In Proceedings of the 2015 IEEE International Symposium on Circuits and Systems (ISCAS), Lisbon, Portugal, 24–27 May 2015; pp. 1006–1009. [Google Scholar]
- Chen, T.; Ng, S.H.; Teo, J.T.; Yang, X. Method and System for Optical Blood Pressure Monitoring. U.S. Patent 10,251,568, 2019. [Google Scholar]
- Mahmud, S.; Ibtehaz, N.; Khandakar, A.; Tahir, A.M.; Rahman, T.; Islam, K.R.; Hossain, M.S.; Rahman, M.S.; Musharavati, F.; Ayari, M.A.; et al. A Shallow U-Net Architecture for Reliably Predicting Blood Pressure (BP) from Photoplethysmogram (PPG) and Electrocardiogram (ECG) Signals. Sensors 2022, 22, 919. [Google Scholar] [CrossRef] [PubMed]
- Brophy, E.; De Vos, M.; Boylan, G.; Ward, T. Estimation of continuous blood pressure from ppg via a federated learning approach. Sensors 2021, 21, 6311. [Google Scholar] [CrossRef]
- Senturk, U.; Polat, K.; Yucedag, I. A Novel Blood Pressure Estimation Method with the Combination of Long Short Term Memory Neural Network and Principal Component Analysis Based on PPG Signals; Springer: Berlin/Heidelberg, Germany, 2019; pp. 868–876. [Google Scholar]
- Tanveer, M.S.; Hasan, M.K. Cuffless blood pressure estimation from electrocardiogram and photoplethysmogram using waveform based ANN-LSTM network. Biomed. Signal Process. Control 2019, 51, 382–392. [Google Scholar] [CrossRef]
- Esmaelpoor, J.; Moradi, M.H.; Kadkhodamohammadi, A. A multistage deep neural network model for blood pressure estimation using photoplethysmogram signals. Comput. Biol. Med. 2020, 120, 103719. [Google Scholar] [CrossRef] [PubMed]
- Hill, B.L.; Rakocz, N.; Rudas, Á.; Chiang, J.N.; Wang, S.; Hofer, I.; Cannesson, M.; Halperin, E. Imputation of the Continuous Arterial Line Blood Pressure Waveform from Non-Invasive Measurements Using Deep Learning. Sci. Rep. 2021, 11, 15755. [Google Scholar] [CrossRef] [PubMed]
- Mehrabadi, M.A.; Aqajari, S.A.H.; Zargari, A.H.A.; Dutt, N.; Rahmani, A.M. Novel Blood Pressure Waveform Reconstruction from Photoplethysmography Using Cycle Generative Adversarial Networks. arXiv 2022, arXiv:2201.09976. [Google Scholar]
- Saeed, M.; Lieu, C.; Raber, G.; Mark, R.G. MIMIC II: A massive temporal ICU patient database to support research in intelligent patient monitoring. Comput. Cardiol. 2002, 29, 641–644. [Google Scholar]
- Salah, M.; Omer, O.A.; Hassan, L.; Ragab, M.; Hassan, A.M.; Abdelreheem, A. Beat-Based PPG-ABP Cleaning Technique for Blood Pressure Estimation. IEEE Access 2022, 10, 55616–55626. [Google Scholar] [CrossRef]
- Oyallon, E.; Mallat, S.; Sifre, L. Generic deep networks with wavelet scattering. arXiv 2013, arXiv:1312.5940. [Google Scholar]
- Oyallon, E.; Belilovsky, E.; Zagoruyko, S. Scaling the scattering transform: Deep hybrid networks. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 5618–5627. [Google Scholar]
- Cotter, F.; Kingsbury, N. Visualizing and improving scattering networks. In Proceedings of the 2017 IEEE 27th International Workshop on Machine Learning for Signal Processing (MLSP), Tokyo, Japan, 25–28 September 2017; pp. 1–6. [Google Scholar]
- Oyallon, E.; Zagoruyko, S.; Huang, G.; Komodakis, N.; Lacoste-Julien, S.; Blaschko, M.; Belilovsky, E. Scattering networks for hybrid representation learning. IEEE Trans. Pattern Anal. Mach. Intell. 2018, 41, 2208–2221. [Google Scholar] [CrossRef] [PubMed]
- Salah, M.; Hassan, L.; Abdel-khier, S.; Hassan, A.M.; Omer, O.A. Robust Facial-Based Inter-Beat Interval Estimation through Spectral Signature Tracking and Periodic Filtering. In Intelligent Sustainable Systems; Springer: Berlin/Heidelberg, Germany, 2022; pp. 161–171. [Google Scholar]
- Sifre, L.; Mallat, S. Rotation, scaling and deformation invariant scattering for texture discrimination. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Portland, OR, USA, 23 June 2013–28 June 2013; pp. 1233–1240. [Google Scholar]
- Liu, Z.; Yao, G.; Zhang, Q.; Zhang, J.; Zeng, X. Wavelet scattering transform for ECG beat classification. Comput. Math. Methods Med. 2020, 2020, 3215681. [Google Scholar] [CrossRef]
- Bruna, J.; Mallat, S. Invariant scattering convolution networks. IEEE Trans. Pattern Anal. Mach. Intell. 2013, 35, 1872–1886. [Google Scholar] [CrossRef] [PubMed]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
Figure 1.
An example dataset sample includes the PPG signal and the corresponding ABP signal.
Figure 2.
Proposed blood pressure monitoring system (testing phase). In the Raw Signal block, the red, green, and blue colors stand for the three channels of RGB images.
Figure 3.
Beat segmentation based on local minimum detection. The red symbols stand for the end of each beat.
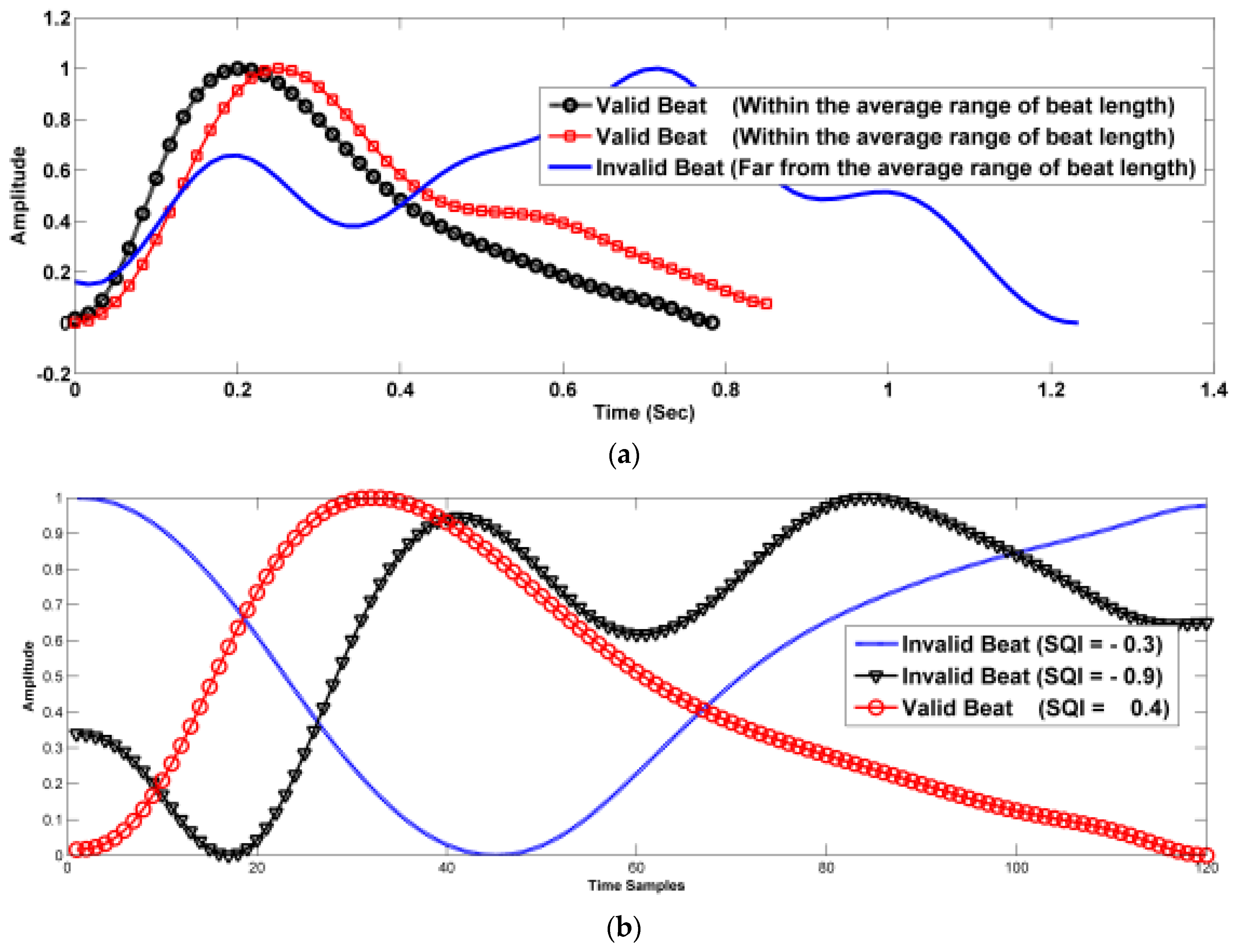
Figure 4.
Segmented beats (including noisy beats), (a) the effect of noise on the beat length, (b) the effect of noise on the beat correlation, and (c) the effect of noise on the beat skewness.
Figure 5.
Selected beats (according to common selection criteria).
Figure 6.
The block diagram of the proposed per-beat BP estimation system (training stage).
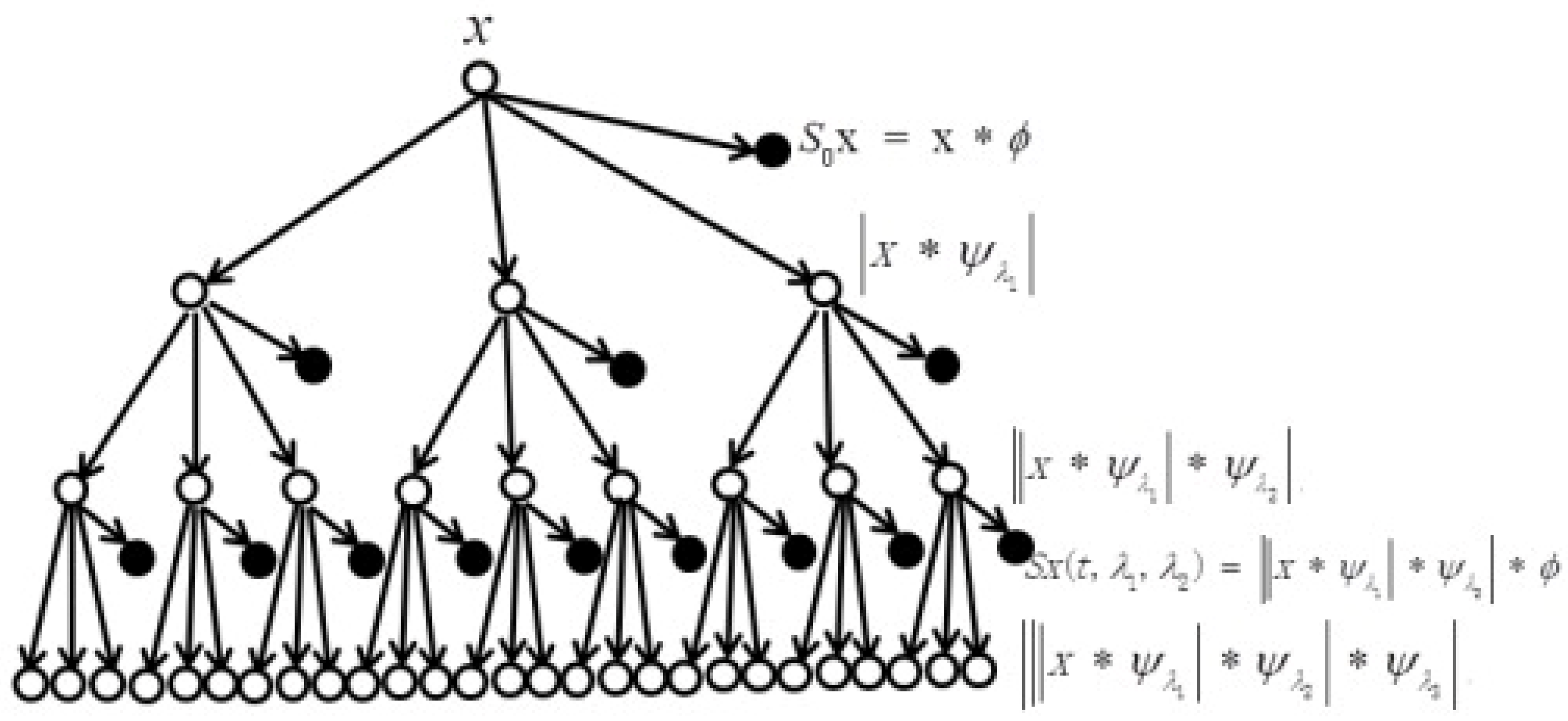
Figure 7.
Multilayer wavelet scattering transform. Unfilled circles stand for the order of the transform. Filled circles stand for the output coefficients of the wavelet scattering transform. The symbol * stands for the convolution process.
Figure 8.
The architecture of the LSTM.
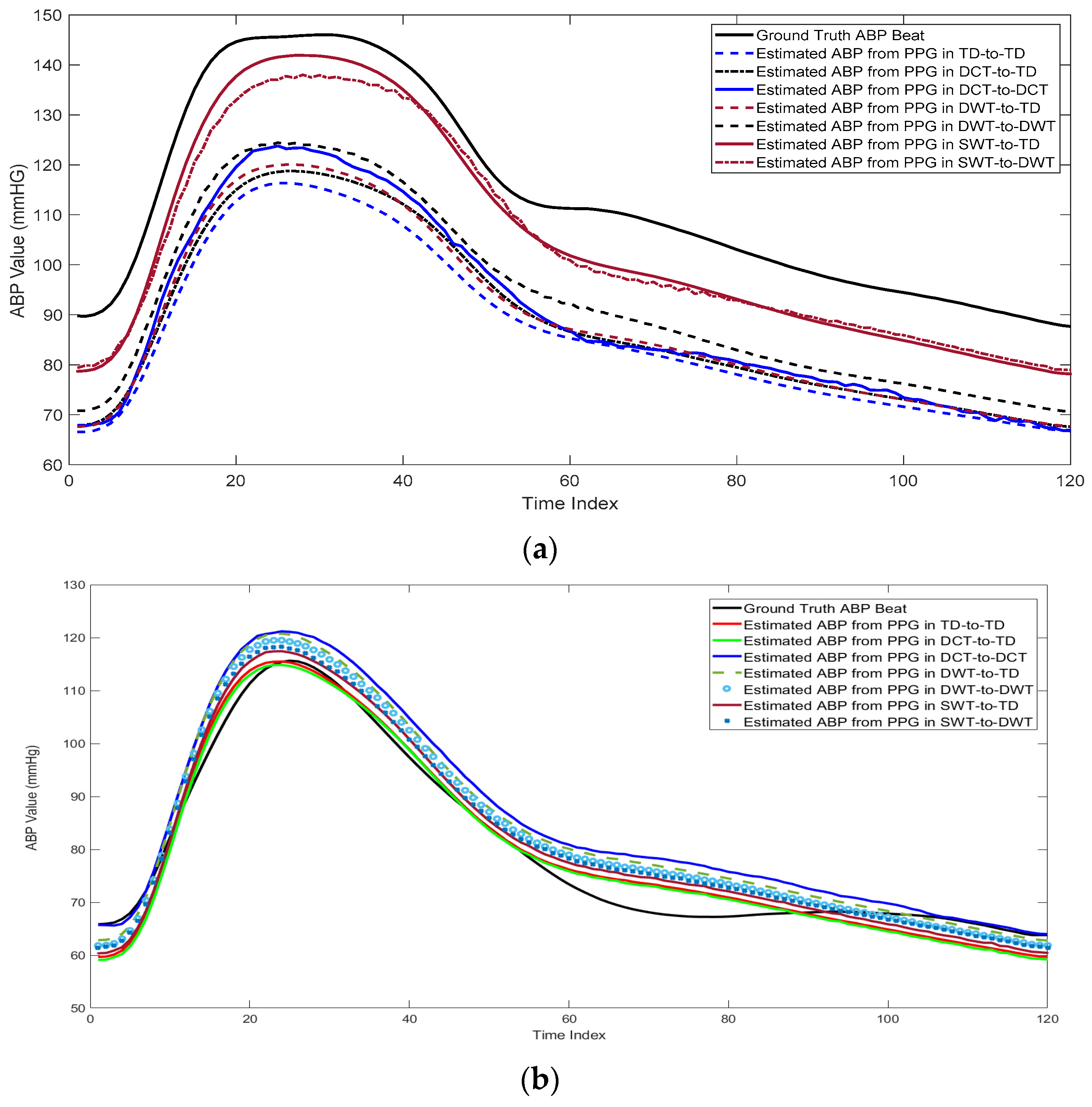
Figure 9.
Comparison between the estimated ABP beats from PPG beats using different transformations in two cases: (a) High blood pressure, (b) normal blood pressure, and (c) low blood pressure.
Figure 10.
The relationship between the predicted and actual SBP and DBP using: (a) Time domain featured, (b) Features in the DCT domain, (c) Features in the DWT domain, and (d) Features in the wavelet scattering domain.
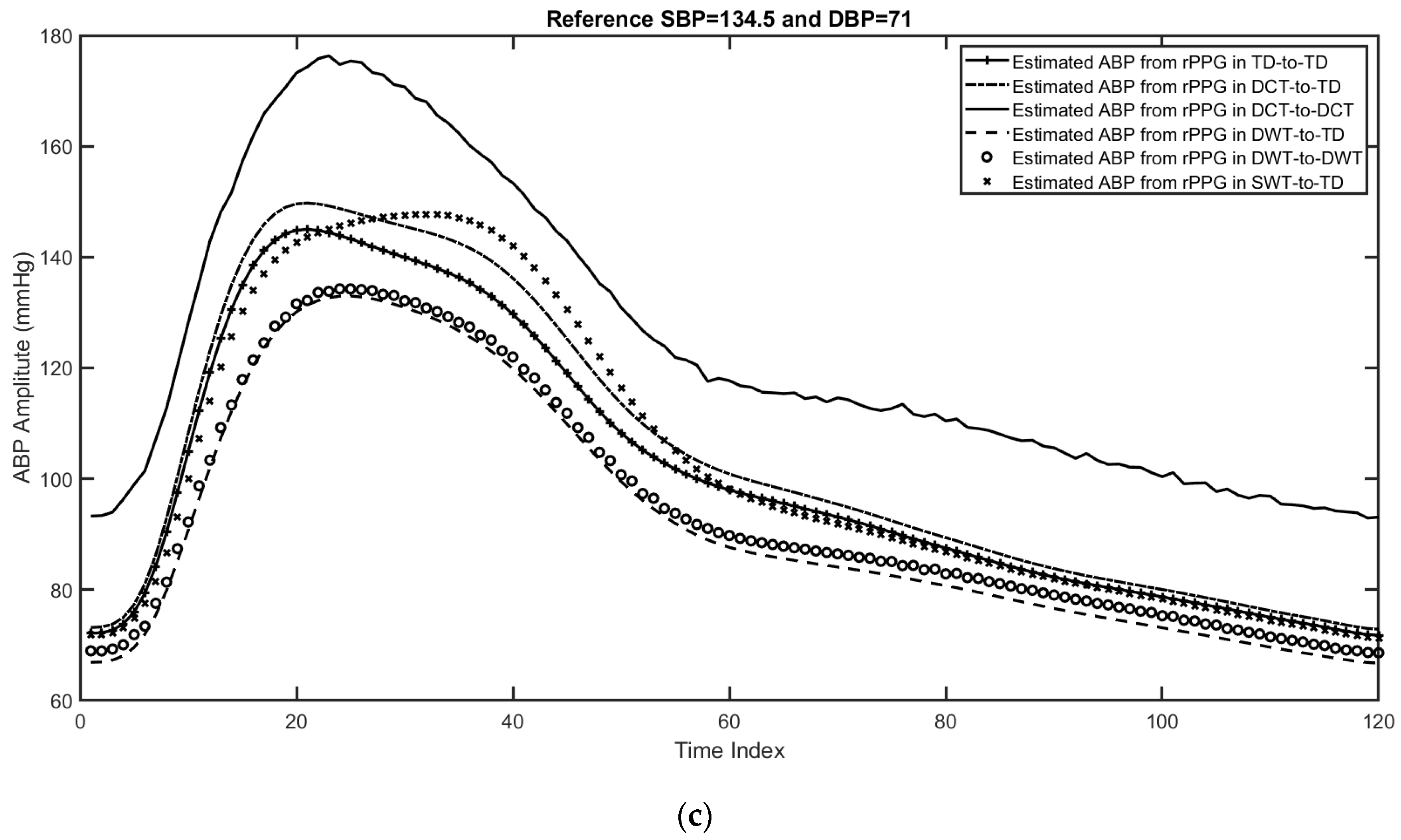
Figure 11.
Three examples for the estimated ABP beats using different feature domains, including the time domain, features in the DCT domain, features in the DWT domain, and features in the wavelet scattering domain. (a) First example with reference SBP = 137 and DBP = 72, (b) second example with reference SBP = 144 and DBP = 73, and (c) third example with reference SBP = 134.5 and DBP = 71.
Table 1.
Network specifications.
| Number of Beats | 158,094 |
| Beat Length (time samples) | 120 |
| Input Feature Domain | One of the following domains:- 1-
Time Domain. - 2-
DCT Domain. - 3-
DWT Domain. - 4-
WST Domain
|
| Number of Channels | 4 × 1 Layer array |
| Layer specifications | - 1-
Sequence input with 120 dimensions - 2-
LSTM with 20 hidden units - 3-
Two fully connected layer - 4-
Regression Output mean-squared-error
|
| Learning Rate | 0.005 |
| Number of Iterations per Epoch | 191 |
| Optimization function | L2-Norm |
| Optimization method | ADAM |
Table 2.
Input and output data size in the two used scenarios for different domains.
Per-Beat
Scenario | Domain | Time | DCT | DWT | WST |
|---|
| PPG2ABP | Input size | 121 × 1 | 120 × 1 | 120 × 1 | 120 × 1 |
| Output size | 120 × 1 | 120 × 1 | 120 × 1 | 120 × 1 |
| PPG2SBP/DBP | Input size | 121 × 1 | 120 × 1 | 120 × 1 | 120 × 1 |
| Output size | 2 × 1 | 2 × 1 | 2 × 1 | 2 × 1 |
Table 3.
Estimated beat-by-beat ABP evaluation using RMSE and MAE for different transformations. Best values are highlighted in bold.
| Domain | Time | DCT | DWT | WST |
|---|
| Case | TD+BI-TD | DCT-TD | DCT-DCT | DWT-TD | DWT-DWT | WST-TD | WST-DWT |
|---|
| RMSE | 11.1663 | 11.3587 | 11.5532 | 10.9905 | 10.8554 | 9.2084 | 8.9935 |
| MAE | 9.8877 | 10.0606 | 10.1669 | 9.7415 | 9.6080 | 7.7671 | 7.6257 |
Table 4.
Estimated SBP and DBP evaluation using RMSE and MAE for different transformations. Best values are highlighted in bold.
| Domain | Time | DCT | DWT | WST |
|---|
| BP | DBP | SBP | DBP | SBP | DBP | SBP | DBP | SBP |
|---|
| RMSE | 9.5636 | 17.6580 | 9.7477 | 17.9762 | 9.4865 | 17.3914 | 6.9164 | 14.2079 |
| MAE | 7.1212 | 13.5720 | 7.2472 | 13.9056 | 7.0517 | 13.3367 | 5.0945 | 10.8358 |
Table 5.
Estimated SBP and DBP evaluation using RMSE and MAE for different transformations. Best values are highlighted in bold.
| Domain | Time | DCT | DWT | WST |
|---|
| BP | DBP | SBP | DBP | SBP | DBP | SBP | DBP | SBP |
|---|
| RMSE | 11.1798 | 17.8066 | 11.7560 | 17.7062 | 11.2555 | 16.9441 | 11.2034 | 15.4742 |
| MAE | 11.1295 | 15.0720 | 11.5511 | 16.7606 | 10.0244 | 14.3486 | 9.5390 | 13.3852 |
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}