
The Effectiveness of Inflammatory Indexes in Assessing Oropharyngeal Cancer Prognosis
 ,
,
Abstract
:1. Introduction
2. Methodology
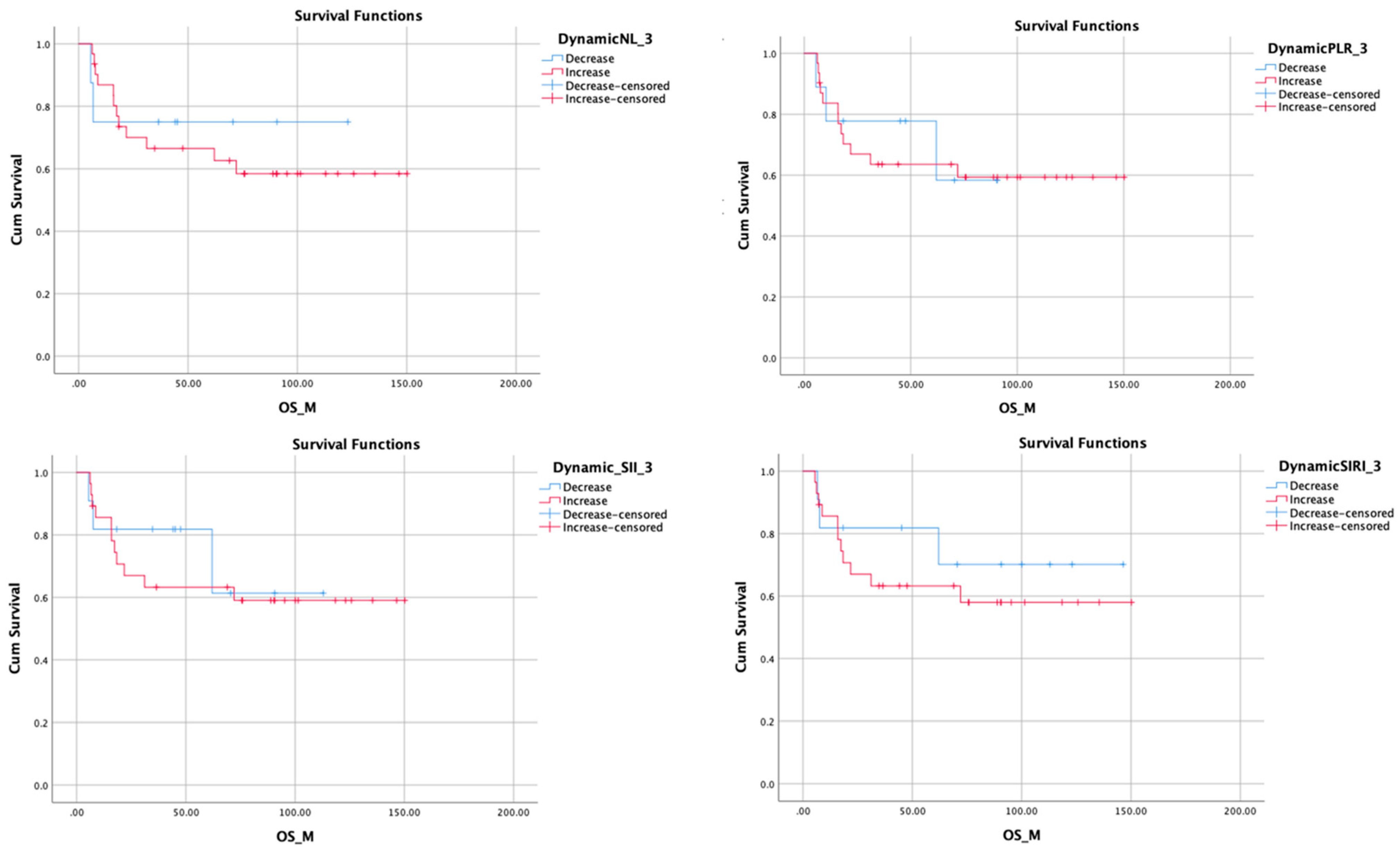
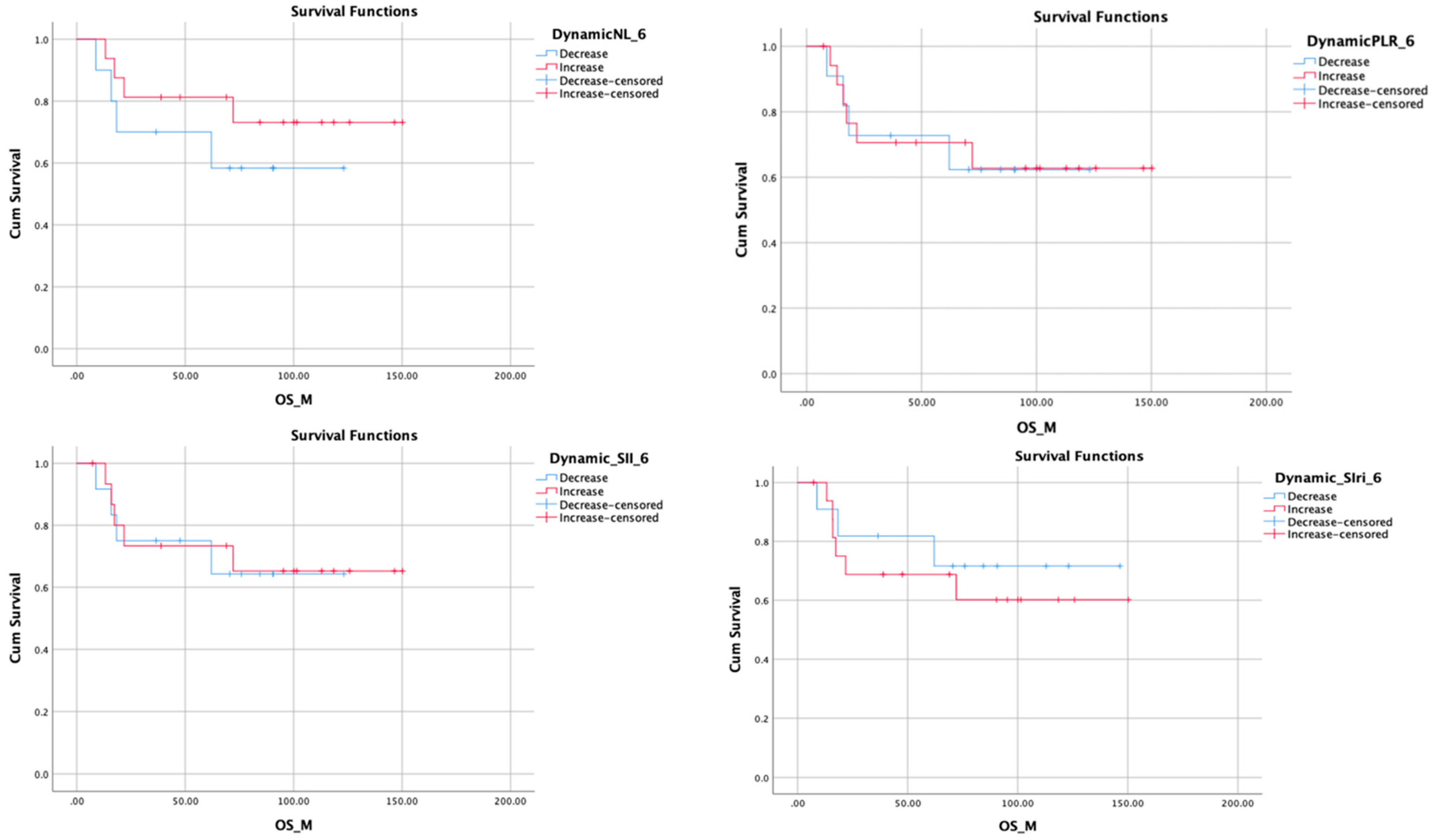
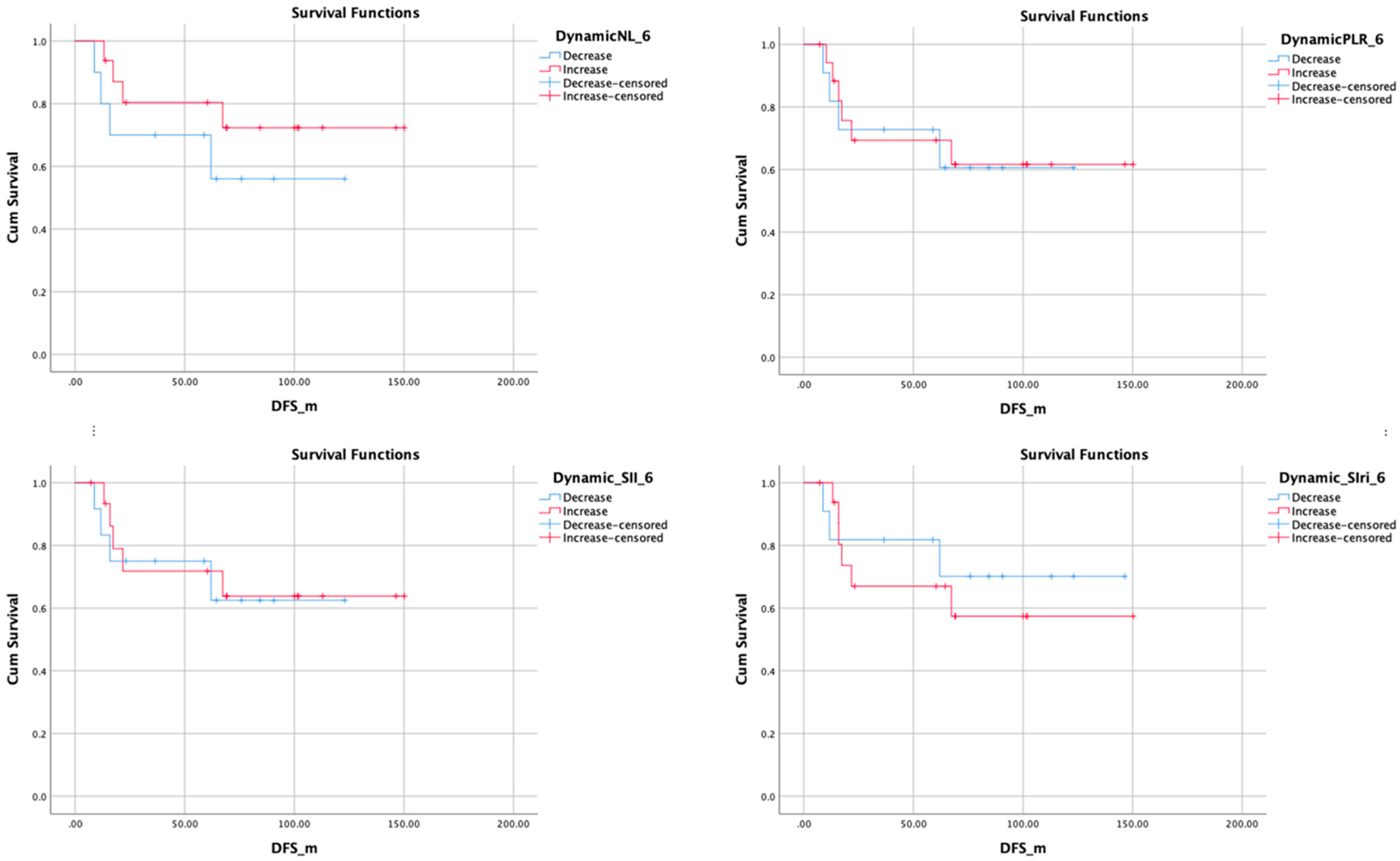
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nøst, T.H.; Alcala, K.; Urbarova, I.; Byrne, K.S.; Guida, F.; Sandanger, T.M.; Johansson, M. Systemic inflammation markers and cancer incidence in the UK Biobank. Eur. J. Epidemiol. 2021, 36, 841–848. [Google Scholar] [CrossRef] [PubMed]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [PubMed]
- Lin, N.; Li, J.; Yao, X.; Zhang, X.; Liu, G.; Zhang, Z.; Weng, S. Prognostic value of neutrophil-to-lymphocyte ratio in colorectal cancer liver metastasis: A meta-analysis of results from multivariate analysis. Int. J. Surg. 2022, 107, 106959. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, R.; Inagawa, S.; Sano, N.; Tadano, S.; Adachi, S.; Yamamoto, M. The neutrophil-to-lymphocyte ratio (NLR) predicts short-term and long-term outcomes in gastric cancer patients. Eur. J. Surg. Oncol. 2018, 44, 607–612. [Google Scholar] [CrossRef]
- Schobert, I.T.; Savic, L.J.; Chapiro, J.; Bousabarah, K.; Chen, E.; Laage-Gaupp, F.; Tefera, J.; Nezami, N.; Lin, M.; Pollak, J.; et al. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as predictors of tumor response in hepatocellular carcinoma after DEB-TACE. Eur. Radiol. 2020, 30, 5663–5673. [Google Scholar] [CrossRef] [PubMed]
- Ferrandino, R.M.; Roof, S.; Garneau, J.; Haidar, Y.; Bates, S.E.; Park, Y.H.A.; Bauml, J.M.; Genden, E.M.; Miles, B.; Sigel, K. Neutrophil-to-lymphocyte ratio as a prognostic indicator for overall and cancer-specific survival in squamous cell carcinoma of the head and neck. Head. Neck. 2020, 42, 2830–2840. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Zhou, P.; Liu, Y.; Wei, H.; Yang, X.; Chen, T.; Xiao, J. Platelet-to-lymphocyte ratio in advanced Cancer: Review and meta-analysis. Clin. Chim. Acta 2018, 483, 48–56. [Google Scholar] [CrossRef]
- Zhang, F.; Gong, W. Prognostic Value of the Platelet-to-Lymphocyte Ratio in Patients with Melanoma: A Meta-Analysis. Front. Oncol. 2020, 10, 1116. [Google Scholar] [CrossRef]
- Sun, L.; Hu, W.; Liu, M.; Chen, Y.; Jin, B.; Xu, H.; Du, S.; Xu, Y.; Zhao, H.; Lu, X.; et al. High Systemic Inflammation Response Index (SIRI) Indicates Poor Outcome in Gallbladder Cancer Patients with Surgical Resection: A Single Institution Experience in China. Cancer Res. Treat. 2020, 52, 1199–1210. [Google Scholar] [CrossRef]
- Xu, Y.; He, H.; Zang, Y.; Yu, Z.; Hu, H.; Cui, J.; Wang, W.; Gao, Y.; Wei, H.; Wang, Z. Systemic inflammation response index (SIRI) as a novel biomarker in patients with rheumatoid arthritis: A multi-center retrospective study. Clin. Rheumatol. 2022, 41, 1989–2000. [Google Scholar] [CrossRef]
- Valero, C.; Pardo, L.; Sansa, A.; Lorenzo, J.G.; López, M.; Quer, M.; León, X. Prognostic capacity of Systemic Inflammation Response Index (SIRI) in patients with head and neck squamous cell carcinoma. Head. Neck. 2020, 42, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Tian, B.W.; Yang, Y.F.; Yang, C.C.; Yan, L.-J.; Ding, Z.-N.; Liu, H.; Xue, J.-S.; Dong, Z.-R.; Chen, Z.-Q.; Hong, J.-G.; et al. Systemic immune-inflammation index predicts prognosis of cancer immunotherapy: Systemic review and meta-analysis. Immunotherapy. 2022, 14, 1481–1496. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Cao, D.; Huang, Y.; Xiong, Q.; Tan, D.; Liu, L.; Lin, T.; Wei, Q. The Prognostic and Clinicopathological Significance of Systemic Immune-Inflammation Index in Bladder Cancer. Front. Immunol. 2022, 13, 865643. [Google Scholar] [CrossRef]
- Liu, J.; Li, S.; Zhang, S.; Liu, Y.; Ma, L.; Zhu, J.; Xin, Y.; Wang, Y.; Yang, C.; Cheng, Y. Systemic immune-inflammation index, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio can predict clinical outcomes in patients with metastatic non-small-cell lung cancer treated with nivolumab. J. Clin. Lab. Anal. 2019, 33, e22964. [Google Scholar] [CrossRef] [PubMed]
- Bosetti, C.; Carioli, G.; Santucci, C.; Bertuccio, P.; Gallus, S.; Garavello, W.; Negri, E.; La Vecchia, C. Global trends in oral and pharyngeal cancer incidence and mortality. Int. J. Cancer. 2020, 147, 1040–1049. [Google Scholar] [CrossRef] [PubMed]
- Yamahara, K.; Mizukoshi, A.; Lee, K.; Ikegami, S. Pretherapeutic nutritional/inflammatory factors as predictors for survival of both early and advanced staged head and neck cancer patients. Auris Nasus Larynx. 2021, 48, 731–737. [Google Scholar] [CrossRef]
- Bossi, P. Prognostic Nutritional Index: An easy nutritional screening for patients with head and neck cancer? ESMO Open 2018, 3, e000449. [Google Scholar] [CrossRef]
- Wang, Y.T.; Kuo, L.T.; Weng, H.H.; Hsu, C.-M.; Tsai, M.-S.; Chang, G.-H.; Lee, Y.-C.; Huang, E.I.; Tsai, Y.-T. Systemic Immun e-Inflammation Index as a Predictor for Head and Neck Cancer Prognosis: A Meta-Analysis. Front. Oncol. 2022, 12, 899518. [Google Scholar] [CrossRef]
- Abelardo, E.; Davies, G.; Kamhieh, Y.; Prabhu, V. Are Inflammatory Markers Significant Prognostic Factors for Head and Neck Cancer Patients? ORL J. Otorhinolaryngol. Relat. Spec. 2020, 82, 235–244. [Google Scholar] [CrossRef]
- Okadome, K.; Baba, Y.; Yagi, T.; Kiyozumi, Y.; Ishimoto, T.M.; Iwatsuki, M.M.; Miyamoto, Y.M.; Yoshida, N.M.; Watanabe, M.M.; Baba, H.M. Prognostic Nutritional Index, Tumor-infiltrating Lymphocytes, and Prognosis in Patients with Esophageal Cancer. Ann. Surg. 2020, 271, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Atasever Akkas, E.; Erdis, E.; Yucel, B. Prognostic value of the systemic immune-inflammation index, systemic inflammation response index, and prognostic nutritional index in head and neck cancer. Eur Arch Otorhinolaryngol. 2023, 280, 3821–3830, Erratum in Eur. Arch. Otorhinolaryngol. 2023, 280, 3831–3833. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Percent | |
|---|---|---|
| Gender | ||
| Male | 136 | 79.1% |
| Female | 36 | 20.9% |
| Ethnicity | ||
| Caucasian | 148 | 86.0% |
| Black | 5 | 2.9% |
| Hispanic or other | 19 | 11.0% |
| Smoking | ||
| No | 68 | 39.5% |
| Fewer than 10 packs | 24 | 14.0% |
| More than 10 packs | 80 | 46.5% |
| Alcohol | ||
| No | 83 | 48.3% |
| Socially | 53 | 30.8% |
| Heavily | 36 | 20.9% |
| Site | ||
| Tonsil | 48 | 27.9% |
| BOT | 76 | 44.2% |
| Soft Palate | 9 | 5.2% |
| Posterior | 11 | 6.4% |
| Overlapping | 28 | 16.3% |
| HPV | ||
| Positive | 66 | 37.7% |
| Negative | 53 | 30.3% |
| N/A | 53 | 30.3% |
| Differentiation | ||
| Well | 11 | 6.4% |
| Moderate | 62 | 36.0% |
| Poor | 47 | 27.3% |
| Undifferentiated | 52 | 30.2% |
| Number | Percentage | |
|---|---|---|
| T staging (7th edition) | ||
| T1 | 24 | 14.0% |
| T2 | 44 | 25.6% |
| T3 | 62 | 36.0% |
| T4 | 42 | 24.4% |
| N staging (7th edition) | ||
| N0 | 31 | 18.0% |
| N1 | 36 | 20.9% |
| N2a | 23 | 13.4% |
| N2b | 39 | 22.7% |
| N2c | 16 | 9.3% |
| N3a | 20 | 11.6% |
| N3b | 7 | 4.1% |
| M staging (7th edition) | ||
| M0 | 119 | 69.2% |
| M1 | 11 | 6.4% |
| M2 | 42 | 24.4% |
| T staging (8th edition) | ||
| T1 | 24 | 14.0% |
| T2 | 44 | 25.6% |
| T3 | 62 | 36.0% |
| T4 | 42 | 24.4% |
| N staging (8th edition) | ||
| N0 | 31 | 18.0% |
| N1 | 24 | 14.0% |
| N2a | 10 | 5.8% |
| N2b | 24 | 14.0% |
| N2c | 10 | 5.8% |
| N3a | 11 | 6.4% |
| N3b | 3 | 1.7% |
| N11 | 20 | 11.6% |
| N22 | 27 | 15.7% |
| N33 | 9 | 5.2% |
| N44 | 3 | 1.7% |
| M staging (8th edition) | ||
| M0 | 119 | 69.2% |
| M1 | 11 | 6.4% |
| M2 | 42 | 24.4% |
| Number | Percentage | |
|---|---|---|
| Treatment Intent | ||
| Curative | 162 | 94.2% |
| Palliative | 10 | 5.8% |
| Primary Treatment | ||
| Chemo/Radiation | 67 | 39.0% |
| Surgery | 99 | 57.6% |
| Radiation | 4 | 2.3% |
| Chemotherapy | 2 | 1.2% |
| Adjuvant Treatment | ||
| None | 66 | 38.4% |
| Chemo/Radiation | 86 | 50.0% |
| Surgery | 9 | 5.2% |
| Radiation | 7 | 4.1% |
| Chemotherapy | 4 | 2.3% |
| Margin Status | ||
| Negative | 32 | 18.6% |
| N/A | 79 | 45.9% |
| Positive | 61 | 35.5% |
| Recurrence | ||
| No | 78 | 45.3% |
| Yes | 41 | 23.8% |
| unknown (?) | 53 | 30.8% |
| Local Recurrence | ||
| Primary Site | 13 | 32.5% |
| Neck | 14 | 35.0% |
| Both | 10 | 25.0% |
| Not specified | 3 | 7.5% |
| Death | ||
| Yes | 59 | 34.3% |
| No | 113 | 65.7% |
| Death Due to Disease | ||
| Yes | 26 | 44.1% |
| No | 33 | 55.9% |
| SIRI | PLR | SII | NLR | PNI | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre-Treatment | 3 Months | 6 Months | Pre-Treatment | 3 Months | 6 Months | Pre-Treatment | 3 Months | 6 Months | Pre-Treatment | 3 Months | 6 Months | Pre-Treatment | ||
| Sex | Male (n:58) | 24.02 | 45.60 | 32.49 | 97.68 | 256.11 | 201.77 | 1199.37 | 2768.84 | 2382.91 | 4.78 | 10.47 | 9.38 | 25.50 |
| Female (n:13) | 25.70 | 19.39 | 29.83 | 192.44 | 242.84 | 112.38 | 2361.78 | 1764.03 | 1145.61 | 7.87 | 6.17 | 5.07 | 25.58 | |
| Ethnicity | Caucasian | 24.29 | 40.86 | 33.25 | 117.49 | 275.14 | 199.92 | 1374.44 | 2443.75 | 2332.70 | 5.32 | 8.96 | 9.25 | 27.33 |
| Black | 24.04 | 33.07 | 26.87 | 13.36 | 8.48 | 5.97 | 871.19 | 550.10 | 390.07 | 2.60 | 3.09 | 2.89 | 22.73 | |
| Hispanic or other | 24.99 | 42.58 | 18.26 | 154.50 | 85.49 | 73.23 | 2156.84 | 4238.48 | 737.31 | 7.51 | 17.67 | 2.89 | 12.33 | |
| Smoking | Non Smoker | 26.14 | 58.19 | 29.57 | 74.50 | 154.08 | 130.45 | 1497.93 | 2463.81 | 2380.28 | 5.79 | 12.52 | 12.15 | 24.69 |
| <10 packs | 42.67 | 24.07 | 22.30 | 81.93 | 258.79 | 88.04 | 1585.58 | 2757.72 | 916.68 | 6.74 | 9.56 | 4.11 | 25.35 | |
| >10 | 19.21 | 34.96 | 34.54 | 143.63 | 304.79 | 229.24 | 1326.05 | 2626.25 | 2229.28 | 4.80 | 8.33 | 7.39 | 26.25 | |
| Alcohol | No Alcohol | 29.23 | 60.87 | 43.60 | 57.79 | 158.41 | 86.25 | 1398.34 | 2733.73 | 1434.51 | 5.71 | 11.04 | 5.92 | 23.21 |
| Social | 29.05 | 28.94 | 20.11 | 137.16 | 252.52 | 266.81 | 1334.03 | 2210.38 | 3598.18 | 5.31 | 9.34 | 13.77 | 25.35 | |
| Heavy | 13.58 | 18.39 | 26.73 | 168.58 | 445.44 | 259.73 | 1501.55 | 2824.19 | 1894.26 | 4.91 | 7.65 | 7.76 | 30.94 | |
| Location Of Tumor | Tonsil | 17.00 | 37.12 | 33.24 | 66.70 | 198.38 | 117.00 | 763.31 | 1661.65 | 1130.60 | 3.18 | 7.50 | 5.47 | 23.86 |
| BOT | 15.50 | 38.36 | 30.87 | 126.10 | 189.46 | 192.35 | 1025.94 | 2126.21 | 2825.55 | 3.87 | 9.30 | 10.56 | 26.54 | |
| Soft Palate | 40.46 | 25.33 | 28.89 | 67.00 | 338.34 | 7.28 | 1313.13 | 2055.45 | 488.15 | 6.47 | 10.56 | 3.28 | 22.04 | |
| Posterior | 35.99 | 99.31 | 31.37 | 194.31 | 312.01 | 278.25 | 3489.36 | 8285.52 | 1615.26 | 12.13 | 23.67 | 7.03 | 23.75 | |
| Overlapping | 41.03 | 31.60 | 37.14 | 127.81 | 579.27 | 452.68 | 2169.05 | 3695.78 | 3532.29 | 7.75 | 8.11 | 13.72 | 27.27 | |
| Hpv | Positive | 25.12 | 37.28 | 27.75 | 100.77 | 189.38 | 170.72 | 1376.81 | 1696.25 | 2285.45 | 5.73 | 7.02 | 9.28 | 28.01 |
| Negative | 28.62 | 46.87 | 39.48 | 75.22 | 329.76 | 154.66 | 1256.59 | 3490.03 | 1538.60 | 5.06 | 12.24 | 6.39 | 23.51 | |
| n/a | 17.78 | 41.04 | 35.52 | 184.46 | 289.60 | 257.41 | 1658.75 | 3317.86 | 2538.07 | 5.26 | 12.12 | 9.39 | 24.51 | |
| Differentiation | Well | 62.30 | 7.98 | .3636 | 75.94 | 1392.63 | 155.45 | 2459.24 | 6017.02 | 310.91 | 9.15 | 4.50 | 1.82 | 32.03 |
| Moderate | 28.71 | 37.46 | 29.44 | 116.78 | 103.07 | 187.14 | 1646.38 | 1495.39 | 3124.95 | 6.49 | 5.60 | 11.80 | 21.27 | |
| Poor | 18.73 | 50.83 | 41.57 | 95.20 | 252.88 | 154.50 | 1205.46 | 2881.12 | 1719.40 | 4.50 | 11.02 | 6.81 | 23.78 | |
| Undiff | 14.85 | 38.32 | 27.68 | 137.21 | 256.19 | 222.52 | 1081.09 | 2933.54 | 1596.62 | 3.95 | 13.13 | 7.11 | 30.79 | |
| Ajcc 7 Staging | T1 | 37.53 | 34.45 | 32.72 | 86.59 | 428.64 | 12.51 | 3057.45 | 2544.49 | 835.32 | 28.33 | 4.68 | 3.50 | 13.81 |
| T2 | 6.34 | 33.34 | 12.77 | 131.98 | 185.00 | 162.98 | 797.70 | 2251.12 | 682.30 | 3.52 | 8.58 | 3.99 | 28.33 | |
| T3 | 29.58 | 46.59 | 44.46 | 97.09 | 163.27 | 125.39 | 1264.57 | 2156.40 | 2832.00 | 4.87 | 9.60 | 12.18 | 27.28 | |
| T4 | 24.21 | 45.75 | 33.05 | 135.52 | 373.51 | 373.49 | 1527.93 | 3672.62 | 3256.58 | 5.28 | 14.23 | 10.07 | 26.79 | |
| N0 | 29.75 | 23.77 | 32.89 | 95.57 | 522.64 | 113.56 | 1512.05 | 2870.39 | 6088.58 | 5.90 | 6.15 | 30.28 | 25.34 | |
| N1 | 24.99 | 16.57 | 13.18 | 131.94 | 285.60 | 163.20 | 1712.47 | 1691.06 | 786.07 | 6.37 | 6.59 | 4.36 | 27.47 | |
| N2a | 11.54 | 44.93 | 33.54 | 99.86 | 94.17 | 235.17 | 795.79 | 1225.86 | 2370.51 | 3.42 | 5.92 | 6.35 | 18.52 | |
| N2b | 22.95 | 44.66 | 15.78 | 140.03 | 178.07 | 312.86 | 1392.75 | 3041.01 | 2016.61 | 5.11 | 14.69 | 7.60 | 25.04 | |
| N2c | 33.07 | 68.57 | 84.92 | 102.17 | 44.39 | 31.50 | 1579.58 | 2189.85 | 2529.08 | 5.55 | 7.49 | 9.09 | 29.87 | |
| N3a | 24.03 | 70.00 | 27.41 | 105.88 | 493.27 | 221.04 | 1314.31 | 6382.21 | 1580.05 | 4.93 | 20.30 | 7.14 | 30.37 | |
| Nx | 21.10 | 24.07 | 19.07 | 126.49 | 341.33 | 147.16 | 1439.00 | 1156.37 | 1025.47 | 6.86 | 4.75 | 5.03 | 17.86 | |
| M0 | 20.98 | 29.86 | 33.77 | 117.54 | 298.81 | 202.49 | 1349.87 | 2026.73 | 1715.13 | 5.23 | 7.57 | 7.16 | 27.43 | |
| M1 | 41.20 | 158.62 | 28.41 | 38.96 | 169.04 | 7.48 | 1013.05 | 9684.81 | 492.24 | 5.18 | 29.81 | 3.29 | 25.51 | |
| Mx | 26.06 | 62.22 | 27.73 | 144.46 | 71.39 | 169.99 | 1824.58 | 3421.94 | 3765.54 | 5.84 | 14.44 | 13.82 | 20.19 | |
| Ajcc 8 Staging | T1 | 37.54 | 34.45 | 32.72 | 86.59 | 428.64 | 12.51 | 3057.45 | 2544.49 | 835.32 | 11.98 | 4.68 | 3.50 | 13.81 |
| T2 | 6.34 | 33.34 | 12.77 | 131.98 | 185.00 | 162.98 | 797.70 | 2251.12 | 682.30 | 3.52 | 8.58 | 3.99 | 28.33 | |
| T3 | 29.58 | 46.59 | 44.46 | 97.09 | 163.27 | 125.39 | 1264.57 | 2156.40 | 2832.00 | 4.87 | 9.60 | 12.18 | 27.28 | |
| T4 | 24.21 | 45.75 | 33.05 | 135.52 | 373.51 | 373.49 | 1527.93 | 3672.62 | 3256.58 | 5.28 | 14.23 | 10.07 | 26.79 | |
| N0 | 29.75 | 23.77 | 32.89 | 95.57 | 522.64 | 113.56 | 1512.05 | 2870.39 | 6088.58 | 5.90 | 6.15 | 30.28 | 25.34 | |
| N1 | 12.50 | 15.07 | 14.19 | 220.35 | 355.47 | 252.51 | 1246.60 | 2009.14 | 1110.16 | 3.81 | 7.76 | 6.40 | 22.60 | |
| N2a | 10.41 | 47.67 | 41.52 | 64.33 | 91.21 | 153.71 | 1080.14 | 1444.49 | 1637.63 | 4.23 | 6.00 | 5.57 | 11.56 | |
| N2b | 25.59 | 60.31 | 11.15 | 128.07 | 221.06 | 652.08 | 1462.76 | 4558.55 | 4060.68 | 5.33 | 22.25 | 14.11 | 27.60 | |
| N2c | 29.68 | 56.42 | 104.46 | 152.48 | 58.29 | 44.35 | 1921.61 | 1916.73 | 3673.00 | 6.42 | 6.08 | 11.45 | 27.86 | |
| N3a | 36.28 | 195.58 | 60.44 | 22.42 | 261.00 | 35.23 | 1161.97 | 14,162.25 | 2927.39 | 4.39 | 40.45 | 9.44 | 28.22 | |
| Nx | - | 29.83 | 19.20 | - | 7.32 | 6.08 | - | 466.76 | 376.52 | - | 2.76 | 2.28 | 15.00 | |
| N1 | 36.11 | 36.54 | 25.15 | 36.23 | 37.53 | 33.45 | 1834.10 | 820.64 | 551.32 | 7.84 | 4.25 | 2.65 | 24.25 | |
| N2 | 19.85 | 43.06 | 32.35 | 125.45 | 126.61 | 213.07 | 818.66 | 1605.68 | 2157.33 | 3.27 | 6.74 | 6.41 | 29.43 | |
| N3 | 3.62 | 28.14 | 19.15 | 244.98 | 570.70 | 267.49 | 1568.20 | 3788.86 | 1243.22 | 5.84 | 13.59 | 6.56 | 33.00 | |
| N | 21.10 | 21.19 | 18.95 | 126.49 | 508.33 | 288.23 | 1439.00 | 1501.17 | 1674.43 | 6.86 | 5.74 | 7.77 | 26.68 | |
| M0 | 20.98 | 29.86 | 33.77 | 117.54 | 298.81 | 202.49 | 1349.87 | 2026.73 | 1715.13 | 5.23 | 7.57 | 7.16 | 27.43 | |
| M1 | 41.20 | 158.62 | 28.41 | 38.96 | 169.04 | 7.48 | 1013.05 | 9684.81 | 492.24 | 5.18 | 29.81 | 3.29 | 25.51 | |
| Mx | 26.06 | 62.22 | 27.73 | 144.46 | 71.39 | 169.99 | 1824.58 | 3421.94 | 3765.54 | 5.84 | 14.44 | 13.82 | 20.19 | |
| Treatment Intent | Curative | 24.51 | 42.30 | 32.07 | 106.10 | 249.51 | 187.40 | 1344.55 | 2523.72 | 2184.06 | 5.20 | 9.61 | 8.69 | 25.53 |
| Palliative | 22.36 | 8.73 | - | 210.43 | 350.29 | - | 2145.17 | 4134.33 | - | 7.05 | 12.02 | - | 25.32 | |
| Primary Treatment | Chemoradiation | 24.96 | 40.97 | 32.85 | 130.96 | 278.00 | 236.48 | 1648.40 | 3098.54 | 2966.08 | 6.22 | 11.13 | 11.34 | 29.40 |
| Surgery | 22.23 | 41.90 | 31.29 | 102.16 | 236.28 | 138.33 | 1200.21 | 2214.22 | 1402.03 | 4.36 | 8.72 | 6.03 | 22.71 | |
| RT | 53.70 | - | - | 11.82 | - | - | 884.54 | - | - | 6.13 | - | - | 22.03 | |
| Chemo | 16.19 | 0.80 | - | 114.40 | 140.95 | - | 974.36 | 456.69 | - | 4.28 | 1.54 | - | 38.55 | |
| Adjuvant Treatment | None | 25.63 | 32.91 | 33.86 | 122.93 | 253.69 | 239.40 | 1644.82 | 2119.68 | 3056.96 | 6.16 | 8.13 | 11.69 | 27.65 |
| CRT | 20.38 | 43.03 | 32.00 | 113.75 | 248.34 | 143.20 | 1202.04 | 2309.15 | 1438.63 | 4.25 | 9.05 | 6.18 | 20.54 | |
| Surgery | 62.15 | 140.38 | 16.71 | 112.51 | 244.76 | 9.13 | 1844.93 | 10,391.99 | 506.74 | 9.73 | 31.90 | 1.86 | 40.56 | |
| RT | 30.63 | 23.79 | - | 13.60 | 425.88 | - | 1009.05 | 4091.68 | - | 4.38 | 16.67 | - | 37.33 | |
| Chemotherapy | 2.45 | 1.53 | 1.04 | 133.02 | 213.35 | 155.38 | 707.88 | 1638.09 | 419.54 | 3.08 | 5.80 | 2.08 | 40.27 | |
| Margin | Negative | 24.52 | 23.77 | 19.02 | 99.02 | 318.56 | 168.88 | 1150.93 | 1367.67 | 895.73 | 4.17 | 5.41 | 4.26 | 31.32 |
| n/a | 24.45 | 55.13 | 41.95 | 122.66 | 161.32 | 171.17 | 1571.42 | 3133.41 | 2847.21 | 5.85 | 12.33 | 10.97 | 25.28 | |
| Positive | 23.92 | 25.02 | 21.55 | 106.02 | 383.01 | 225.86 | 1203.28 | 2252.86 | 1695.84 | 4.96 | 7.32 | 7.01 | 22.68 | |
| Recurrence | No | 14.73 | 30.17 | 30.93 | 113.48 | 164.98 | 191.79 | 1044.07 | 1227.30 | 2267.51 | 4.17 | 6.17 | 9.06 | 27.74 |
| Yes | 28.79 | 48.27 | 18.99 | 167.81 | 500.54 | 210.18 | 1468.14 | 4531.35 | 1222.10 | 5.21 | 15.03 | 5.91 | 28.12 | |
| n/a | 36.86 | 118.27 | 91.94 | 72.02 | 201.41 | 48.68 | 1990.49 | 8565.98 | 4194.39 | 7.48 | 24.14 | 12.66 | 20.16 | |
| Location Of Recurrence * | Primary Site | 21.85 | 38.79 | 26.04 | 252.40 | 437.04 | 98.01 | 1322.54 | 3557.62 | 909.84 | 3.95 | 10.47 | 4.48 | 27.72 |
| Neck | 55.07 | 61.77 | 32.67 | 19.19 | 57.32 | 11.62 | 1427.66 | 1354.85 | 775.20 | 5.86 | 7.33 | 3.36 | 26.98 | |
| Both | 4.02 | 62.65 | 4.94 | 240.94 | 839.74 | 380.83 | 1603.75 | 7847.63 | 1913.25 | 5.97 | 25.04 | 8.38 | 24.51 | |
| n/a | 33.52 | 13.02 | 19.85 | 21.38 | 244.35 | 241.36 | 1676.14 | 1959.92 | 1070.04 | 5.41 | 8.15 | 6.68 | 41.02 | |
| Death ** | Yes | 28.84 | 54.42 | 42.70 | 143.79 | 342.88 | 255.44 | 1650.57 | 3726.64 | 4025.86 | 5.97 | 13.53 | 15.00 | 25.79 |
| No | 21.40 | 33.45 | 26.61 | 95.24 | 205.23 | 152.47 | 1256.99 | 1961.08 | 1238.27 | 4.95 | 7.60 | 5.44 | 25.38 | |
| Death Of Disease | Yes | 29.72 | 32.11 | 18.70 | 205.28 | 600.45 | 392.34 | 1857.69 | 5031.72 | 3361.56 | 6.34 | 16.03 | 7.73 | 32.61 |
| No | 27.96 | 76.73 | 56.69 | 77.90 | 85.32 | 175.58 | 1443.46 | 2421.55 | 4413.37 | 5.60 | 11.03 | 19.25 | 20.07 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, W.; Zeitouni, J.F.; Nguyen, D.K.; Mohiuddin, I.S.; Ward, H.; Satheeshkumar, A.; Dundar, Y. The Effectiveness of Inflammatory Indexes in Assessing Oropharyngeal Cancer Prognosis. Surgeries 2024, 5, 377-390. https://doi.org/10.3390/surgeries5020031
Jang W, Zeitouni JF, Nguyen DK, Mohiuddin IS, Ward H, Satheeshkumar A, Dundar Y. The Effectiveness of Inflammatory Indexes in Assessing Oropharyngeal Cancer Prognosis. Surgeries. 2024; 5(2):377-390. https://doi.org/10.3390/surgeries5020031
Chicago/Turabian StyleJang, Wooyoung, Jad F. Zeitouni, Daniel K. Nguyen, Ismail S. Mohiuddin, Haven Ward, Anu Satheeshkumar, and Yusuf Dundar. 2024. "The Effectiveness of Inflammatory Indexes in Assessing Oropharyngeal Cancer Prognosis" Surgeries 5, no. 2: 377-390. https://doi.org/10.3390/surgeries5020031