
Serum Biomarker Concentrations upon Admission in Acute Traumatic Brain Injury: Associations with TBI Severity, Toxoplasma gondii Infection, and Outcome in a Referral Hospital Setting in Cameroon

 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Area, Design, and Period
2.2. Study Population and Participants
2.3. Sampling Method and Unit
2.4. Laboratory Methods
2.5. Measurement of Blood Fluid Biomarkers (GFAP, Tau, UCHL-1, and NFL)
2.6. Measurement of Toxoplasma gondii IgG Antibodies (ELISA)
2.7. Data Management and Analysis
2.8. Ethical Clearance and Administrative Authorizations
3. Results
3.1. Characteristics of Participants
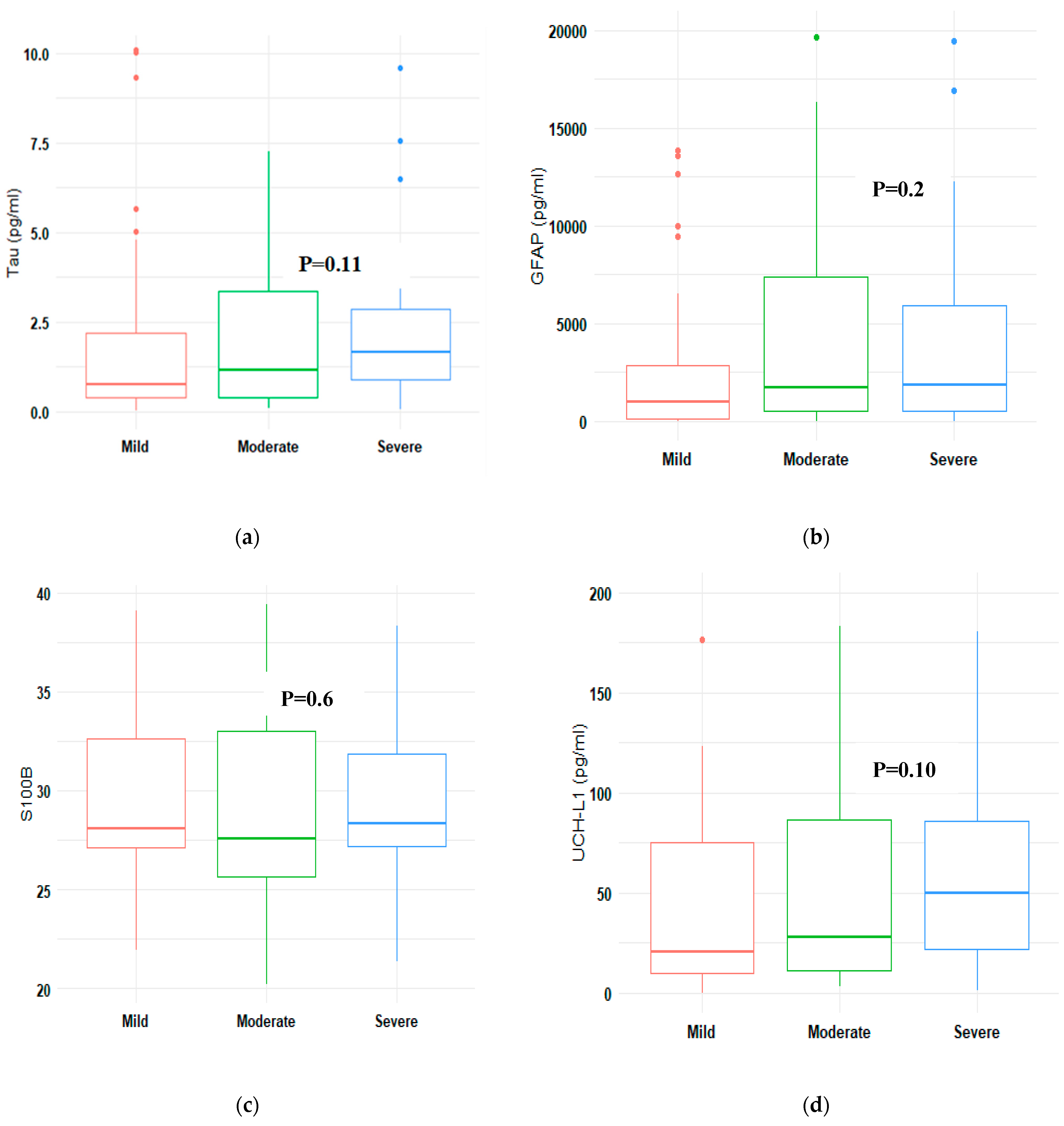
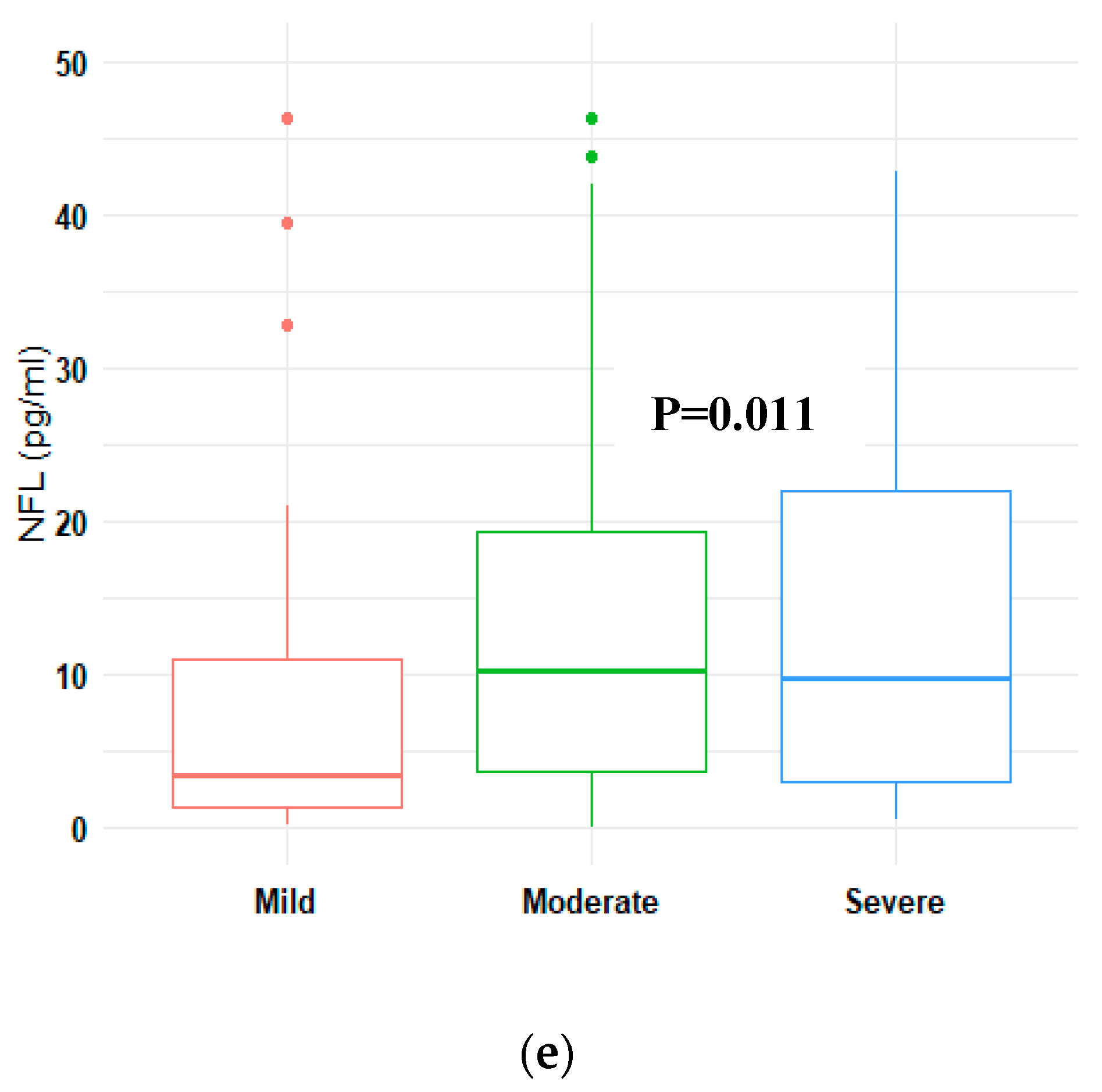
3.2. Serum Concentrations of Biomarkers and TBI Severity and Outcome
3.3. Toxoplasma gondii Infection and Biomarkers Concentrations
4. Discussion
4.1. Concentrations of Serum Biomarkers and the Association with Traumatic Brain Injury Severity
4.2. Concentrations of the Biomarkers and 6 Months Outcome
4.3. Concentrations of the Biomarkers and CT Positive and Negative Scans
4.4. Concentrations of the Biomarkers according to Toxoplasma gondii Infection
5. Strengths and Limitations
6. Conclusions and Implications
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the global incidence of traumatic brain injury. J. Neurosurg. 2018, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wongchareon, K.; Thompson, H.J.; Mitchell, P.H.; Barber, J.; Temkin, N. IMPACT and CRASH prognostic models for traumatic brain injury: External validation in a South-American cohort. Inj. Prev. 2020, 26, 546–554. [Google Scholar] [CrossRef] [PubMed]
- Bazarian, J.J.; Biberthaler, P.; Welch, R.D.; Lewis, L.M.; Barzo, P.; Bogner-Flatz, V.; Brolinson, P.G.; Büki, A.; Chen, J.Y.; Christenson, R.H.; et al. Serum GFAP and UCH-L1 for prediction of absence of intracranial injuries on head CT (ALERT-TBI): A multicentre observational study. Lancet Neurol. 2018, 17, 782–789. [Google Scholar] [CrossRef]
- Brazinova, A.; Rehorcikova, V.; Taylor, M.S.; Buckova, V.; Majdan, M.; Psota, M.; Peeters, W.; Feigin, V.; Theadom, A.; Holkovic, L.; et al. Epidemiology of Traumatic Brain Injury in Europe: A Living Systematic Review. J. Neurotrauma 2021, 38, 1411–1440. [Google Scholar] [CrossRef] [Green Version]
- Kinyanjui, B. Traumatic Brain Injury in Kenya: A Preliminary Review of the Literature. SAGE Open 2016, 6, 2158244016638392. [Google Scholar] [CrossRef] [Green Version]
- Eaton, J.; Hanif, A.B.; Grudziak, J.; Charles, A. Epidemiology, Management, and Functional Outcomes of Traumatic Brain Injury in Sub-Saharan Africa. World Neurosurg. 2017, 108, 650–655. [Google Scholar] [CrossRef] [PubMed]
- Saidi, H.; Mutiso, B.K.; Ogengo, J. Mortality after road traffic crashes in a system with limited trauma data capability. J. Trauma Manag. Outcomes 2014, 8, 4. [Google Scholar] [CrossRef] [Green Version]
- Wong, K.R.; O’brien, W.T.; Sun, M.; Yamakawa, G.; O’brien, T.J.; Mychasiuk, R.; Shultz, S.R.; McDonald, S.J.; Brady, R.D. Serum Neurofilament Light as a Biomarker of Traumatic Brain Injury in the Presence of Concomitant Peripheral Injury. Biomark. Insights 2021, 16, 11772719211053449. [Google Scholar] [CrossRef]
- Adegboyega, G.; Zolo, Y.; Sebopelo, L.A.; Dalle, D.U.; Dada, O.E.; Mbangtang, C.B.; Tetinou, F.; Kanmounye, U.S.; Alalade, A.F. The Burden of Traumatic Brain Injury in Sub-Saharan Africa: A Scoping Review. World Neurosurg. 2021, 156, e192–e205. [Google Scholar] [CrossRef]
- Honeybul, S.; Kolias, A.G. Traumatic Brain Injury: Science, Practice, Evidence and Ethics; Springer: Cham, Switzerland, 2021; p. 347. [Google Scholar]
- Werner, C.; Engelhard, K. Pathophysiology of traumatic brain injury. Br. J. Anaesth. 2007, 99, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Mondello, S.; Sorinola, A.; Czeiter, E.; Vámos, Z.; Amrein, K.; Synnot, A.; Donoghue, E.; Sándor, J.; Wang, K.K.W.; Diaz-Arrastia, R.; et al. Blood-Based Protein Biomarkers for the Management of Traumatic Brain Injuries in Adults Presenting to Emergency Departments with Mild Brain Injury: A Living Systematic Review and Meta-Analysis. J. Neurotrauma 2021, 38, 1086–1106. [Google Scholar] [CrossRef] [Green Version]
- Hergenroeder, G.W.; Redell, J.B.; Moore, A.N.; Dash, P.K. Biomarkers in the Clinical Diagnosis and Management of Traumatic Brain Injury. Mol. Diagn. Ther. 2008, 12, 345–358. [Google Scholar] [CrossRef] [PubMed]
- Zurek, J. Biomarkers in traumatic brain injury. In Essentials of Neuroanesthesia, 1st ed.; Prabhaker, H., Ed.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 587–591. [Google Scholar]
- Slavoaca, D.; Muresanu, D.; Birle, C.; Rosu, O.V.; Chirila, I.; Dobra, I.; Jemna, N.; Strilciuc, S.; Vos, P. Biomarkers in traumatic brain injury: New concepts. Neurol. Sci. 2019, 41, 2033–2044. [Google Scholar] [CrossRef] [PubMed]
- Zetterberg, H.; Smith, D.H.; Blennow, K. Biomarkers of mild traumatic brain injury in cerebrospinal fluid and blood. Nat. Rev. Neurol. 2013, 9, 201–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubenstein, R.; Chang, B.; Yue, J.K.; Chiu, A.; Winkler, E.A.; Puccio, A.M.; Diaz-Arrastia, R.; Yuh, E.L.; Mukherjee, P.; Valadka, A.B.; et al. Comparing Plasma Phospho Tau, Total Tau, and Phospho Tau–Total Tau Ratio as Acute and Chronic Traumatic Brain Injury Biomarkers. JAMA Neurol. 2017, 74, 1063–1072. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.K.; Pareja, J.C.M.; Mondello, S.; Diaz-Arrastia, R.; Wellington, C.; Kenney, K.; Puccio, A.M.; Hutchison, J.; McKinnon, N.; Okonkwo, D.O.; et al. Blood-based traumatic brain injury biomarkers—Clinical utilities and regulatory pathways in the United States, Europe and Canada. Expert Rev. Mol. Diagn. 2021, 21, 1303–1321. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Wiegers, E.; Sewalt, C.; Buki, A.; Citerio, G.; De Keyser, V.; Ercole, A.; Kunzmann, K.; Lanyon, L.; Lecky, F.; et al. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: A European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019, 18, 923–934. [Google Scholar] [CrossRef]
- Najem, D.; Rennie, K.; Ribecco-Lutkiewicz, M.; Ly, D.; Haukenfrers, J.; Liu, Q.; Nzau, M.; Fraser, D.D.; Bani-Yaghoub, M. Traumatic brain injury: Classification, models, and markers. Biochem. Cell Biol. 2018, 96, 391–406. [Google Scholar] [CrossRef]
- Yue, J.K.; Yuh, E.L.; Korley, F.K.; Winkler, E.A.; Sun, X.; Puffer, R.C.; Deng, H.; Choy, W.; Chandra, A.; Taylor, S.R.; et al. Association between plasma GFAP concentrations and MRI abnormalities in patients with CT-negative traumatic brain injury in the TRACK-TBI cohort: A prospective multicentre study. Lancet Neurol. 2019, 18, 953–961. [Google Scholar] [CrossRef]
- Czeiter, E.; Amrein, K.; Gravesteijn, B.Y.; Lecky, F.; Menon, D.K.; Mondello, S.; Newcombe, V.F.; Richter, S.; Steyerberg, E.W.; Vyvere, T.V.; et al. Blood biomarkers on admission in acute traumatic brain injury: Relations to severity, CT findings and care path in the CENTER-TBI study. eBioMedicine 2020, 56, 102785. [Google Scholar] [CrossRef]
- Helmrich, I.R.A.R.; Czeiter, E.; Amrein, K.; Büki, A.; Lingsma, H.F.; Menon, D.K.; Mondello, S.; Steyerberg, E.W.; von Steinbüchel, N.; Wang, K.K.W.; et al. Incremental prognostic value of acute serum biomarkers for functional outcome after traumatic brain injury (CENTER-TBI): An observational cohort study. Lancet Neurol. 2022, 21, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Korley, F.K.; Jain, S.; Sun, X.; Puccio, A.M.; Yue, J.K.; Gardner, R.C.; Wang, K.K.W.; Okonkwo, D.O.; Yuh, E.L.; Mukherjee, P.; et al. Prognostic value of day-of-injury plasma GFAP and UCH-L1 concentrations for predicting functional recovery after traumatic brain injury in patients from the US TRACK-TBI cohort: An observational cohort study. Lancet Neurol. 2022, 21, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Milleville, K.A.; Awan, N.; Disanto, D.; Kumar, R.G.; Wagner, A.K. Early chronic systemic inflammation and associations with cognitive performance after moderate to severe TBI. Brain Behav. Immun.-Health 2020, 11, 100185. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Puvenna, V.; Janigro, D. Biomarkers of Traumatic Brain Injury and Their Relationship to Pathology. In Translational Research in Traumatic Brain Injury; Laskowitz, D., Grant, G., Eds.; CRC Press/Taylor and Francis Group: Boca Raton, FL, USA, 2016; Chapter 12. Available online: https://www.ncbi.nlm.nih.gov/books/NBK326724/ (accessed on 30 March 2023).
- Visser, K.; Koggel, M.; Blaauw, J.; van der Horn, H.J.; Jacobs, B.; van der Naalt, J. Blood-based biomarkers of inflammation in mild traumatic brain injury: A systematic review. Neurosci. Biobehav. Rev. 2022, 132, 154–168. [Google Scholar] [CrossRef]
- World Population Review. Douala Population 2023. Available online: https://worldpopulationreview.com/world-cities/douala-population (accessed on 20 June 2023).
- Benneh, G. Douala Cameroon. Britanica, 2022. Consulted 30.03.2022. Available online: https://www.britannica.com/place/Cameroon (accessed on 18 December 2022).
- Quanterix. Simoa N4PB KIT: Human Neurology 4-Plex “B”. Quanterix Coorporation 2019. 900 Middlesex Turnpike, Building 1 Billerica MA 01821. Available online: https://www.quanterix.com/wp-content/uploads/2020/12/DS-0145_N4PB_Data_Sheet_SR-X_Rev02.pdf (accessed on 16 January 2023).
- Abbasi, M.; Sajjadi, M.; Fathi, M.; Maghsoudi, M. Serum S100B Protein as an Outcome Prediction Tool in Emergency Department Patients with Traumatic Brain Injury. Turk. J. Emerg. Med. 2016, 14, 147–152. [Google Scholar] [CrossRef] [Green Version]
- Welch, R.D.; Ellis, M.; Lewis, L.M.; Ayaz, S.I.; Mika, V.H.; Millis, S.; Papa, L. Modeling the Kinetics of Serum Glial Fibrillary Acidic Protein, Ubiquitin Carboxyl-Terminal Hydrolase-L1, and S100B Concentrations in Patients with Traumatic Brain Injury. J. Neurotrauma 2017, 34, 1957–1971. [Google Scholar] [CrossRef]
- Shahim, P.; Tegner, Y.; Wilson, D.H.; Randall, J.; Skillbäck, T.; Pazooki, D.; Kallberg, B.; Blennow, K.; Zetterberg, H. Blood Biomarkers for Brain Injury in Concussed Professional Ice Hockey Players. JAMA Neurol. 2014, 71, 684–692, Erratum in: JAMA Neurol. 2016, 73, 1160. [Google Scholar] [CrossRef]
- Lorente, L. Biomarkers Associated with the Outcome of Traumatic Brain Injury Patients. Brain Sci. 2017, 7, 142. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Li, J.; Han, L.; Guo, S.; Wang, L.; Xiong, Z.; Chen, Z.; Chen, W.; Liang, J. Serum τ protein as a potential biomarker in the assessment of traumatic brain injury. Exp. Ther. Med. 2016, 11, 1147–1151. [Google Scholar] [CrossRef] [Green Version]
- Mehta, T.; Fayyaz, M.; Giler, G.E.; Kaur, H.; Raikwar, S.P.; Kempuraj, D.; Selvakumar, G.P.; Ahmed, M.E.; Thangavel, R.; Zaheer, S.; et al. Current Trends in Biomarkers for Traumatic Brain Injury. Open Access J. Neurol. Neurosurg. 2020, 12, 86–94. [Google Scholar]
- Diaz-Arrastia, R.; Wang, K.K.; Papa, L.; Sorani, M.D.; Yue, J.K.; Puccio, A.M.; McMahon, P.J.; Inoue, T.; Yuh, E.L.; Lingsma, H.F.; et al. Acute Biomarkers of Traumatic Brain Injury: Relationship between Plasma Levels of Ubiquitin C-Terminal Hydrolase-L1 and Glial Fibrillary Acidic Protein. J. Neurotrauma 2014, 31, 19–25. [Google Scholar] [CrossRef] [PubMed]
- McMahon, P.J.; Panczykowski, D.M.; Yue, J.K.; Puccio, A.M.; Inoue, T.; Sorani, M.D.; Lingsma, H.F.; Maas, A.I.; Valadka, A.B.; Yuh, E.L.; et al. Measurement of the Glial Fibrillary Acidic Protein and Its Breakdown Products GFAP-BDP Biomarker for the Detection of Traumatic Brain Injury Compared to Computed Tomography and Magnetic Resonance Imaging. J. Neurotrauma 2015, 32, 527–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nde, C.J.; Raymond, A.; Saidu, Y.; Cheng, N.I.; Nzuobontane, D.; Atemnkeng, J.T.; Mbacham, W.F. Reaching Universal Health Coverage by 2035: Is Cameroon on Track? Univers. J. Public Health 2019, 7, 110–117. [Google Scholar] [CrossRef] [Green Version]
- Baker, T.L.; Sun, M.; Semple, B.D.; Tyebji, S.; Tonkin, C.J.; Mychasiuk, R.; Shultz, S.R. Catastrophic consequences: Can the feline parasite Toxoplasma gondii prompt the purrfect neuroinflammatory storm following traumatic brain injury? J. Neuroinflamm. 2020, 17, 222. [Google Scholar] [CrossRef]
- Estato, V.; Stipursky, J.; Gomes, F.; Mergener, T.C.; Frazão-Teixeira, E.; Allodi, S.; Tibiriçá, E.; Barbosa, H.S.; Adesse, D. The Neurotropic Parasite Toxoplasma gondii Induces Sustained Neuroinflammation with Microvascular Dysfunction in Infected Mice. Am. J. Pathol. 2018, 188, 2674–2687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gale, S.D.; Erickson, L.D.; Thacker, E.L.; Mitchell, E.L.; Brown, B.L.; Hedges, D.W. Toxoplasma gondii seropositivity and serointensity and cognitive function in adults. PLoS Negl. Trop. Dis. 2020, 14, e0008733. [Google Scholar] [CrossRef]
- Ayyildiz, H.; Kalayci, M.; Karabulut, N.; Karaboga, F. S100B and Latent Toxoplasmosis in Alzheimer’s disease. Int. J. Med. Biochem. 2019, 2, 113–117. [Google Scholar] [CrossRef]
- Sun, M. How Does Toxoplasma Gondii, A Common Worldwide Infection, Affect Brain Injury? Monash University 2019. Available online: https://brainfoundation.org.au/research-grants/2019/neural-infections/ (accessed on 27 December 2022).



{kind=link}
{kind=link}
| Characteristic | N (%) |
|---|---|
| N | 160 |
| Age, Median (IQR) in years | 32 (IQR26, 39) |
| Gender | |
| Female | 16 (10%) |
| Male | 144 (90%) |
| Education | |
| Graduate | 19 (12%) |
| No formal education | 9 (5.6%) |
| Matriculated | 7 (4.4%) |
| Not Known | 2 (1.2%) |
| Post graduate | 1 (0.6%) |
| Primary | 40 (25%) |
| Secondary | 82 (51%) |
| Profession | |
| Employee in service | 30 (19%) |
| Manual workers | 24 (15%) |
| Bike riders | 43 (27%) |
| Student | 16 (10%) |
| Unemployed | 21 (13%) |
| Others | 26 (16%) |
| Marital status | |
| Married | 67 (42%) |
| Not applicable | 6 (3.8%) |
| Single | 86 (54%) |
| Widowed | 1 (0.6%) |
| Medico-social history | |
| Diabetes | 2 (1.2%) |
| Hypertension | 14 (8.8%) |
| Smoking | 22 (14%) |
| Alcohol | 97 (61%) |
| Influence of alcohol | |
| None | 108 (68%) |
| Suspected | 33 (21%) |
| Unknown | 19 (12%) |
| Symptoms of TBI | |
| Loss of consciousness | 152 (95%) |
| Vomiting | 55 (34%) |
| Nausea | 21 (13%) |
| Ear bleed | 20 (12%) |
| Nasal bleed | 43 (27%) |
| Headache | 103 (64%) |
| Seizure | 7 (4.4%) |
| Agitation | 43 (27%) |
| Classification of TBI | |
| Mild | 66 (41%) |
| Moderate | 55 (34%) |
| Severe | 39 (24%) |
| Blood pressure | N = 160 |
| Elevated | 15 (9.4%) |
| Hypertension | 62 (39%) |
| Hypotension | 19 (12%) |
| Normal | 64 (40%) |
| Median Glasgow Coma Scale | 12.0 (8.0, 14.0) |
| Referrals | |
| Direct | 95 (59%) |
| Indirect | 65 (41%) |
| Complementary exams done to characterize injury | N = 160 |
| CT Scan | 125 (78%) |
| If scan or MRI, traumatic abnormalities present | 77 (64%) |
| Type of TBI | N = 77 |
| Cerebral contusion | 25 (32%) |
| Extradural hematoma | 22 (29%) |
| Acute subdural haemorrhage | 18 (23%) |
| Intracerebral haemorrhage | 12 (16%) |
| Cerebral oedema | 10 (13%) |
| Meningeal haemorrhage | 8 (10%) |
| Mass effect pressure | 3 (3.9%) |
| Other type of TBI | 4 (5.2%) |
| Neurosurgery | N = 77 |
| Yes | 17 (22.1%) |
| No | 60 (78%) |
| Biomarkers as Median (IQR) | TBI Cases N = 160 | Controls N = 15 | p-Value |
|---|---|---|---|
| S100B (pg/mL) | 28 (26, 33) | 0 (0, 0) | <0.001 |
| GFAP (pg/mL) | 1244 (277, 4042) | 13 (11, 21) | <0.001 |
| NFL (pg/mL) | 7 (2, 16) | 1 (1, 1) | <0.001 |
| Tau (pg/mL) | 1.15 (0.44, 2.87) | 0.32 (0.20, 0.49) | <0.001 |
| UCH-L1 (pg/mL) | 31 (12, 86) | 7 (4, 9) | <0.001 |
| Biomarkers as Median (IQR) | Controls | Traumatic Brain Injury Severity | p-Value | ||
|---|---|---|---|---|---|
| Mild | Moderate | Severe | |||
| N | 15 | 66 | 55 | 39 | |
| S100B (pg/mL) | 0.0 (0, 0) | 28.1 (27.1, 32.6) | 27.6 (25.6, 33.0) | 28.3 (27.2, 31.9) | <0.001 |
| GFAP (pg/mL) | 13.0 (11, 21) | 1020 (147, 2831) | 1723 (503, 7.403) | 1876 (532, 5903) | <0.001 |
| NFL (pg/mL) | 1.0 (1, 1) | 3.0 (1, 11) | 10.0 (4, 19) | 10.0 (3, 22) | <0.001 |
| Tau (pg/mL) | 0.32 (0.20, 0.49) | 0.76 (0.39, 2.18) | 1.17 (0.40, 3.35) | 1.65 (0.88, 2.85) | <0.001 |
| UCH-L1 (pg/mL) | 7.0 (4, 9) | 20.0 (10, 75) | 28.0 (12, 87) | 50.0 (22, 86) | <0.001 |
| Biomarkers as Median (IQR) | Survival N= 130 | Death, N = 22 | Favorable N = 114 | Unfavorable N = 38 | p-Value (Favourable vs. Unfavourable GOSE | p-Value (Death vs. Survival) |
|---|---|---|---|---|---|---|
| S100B (pg/mL) | 28.1 (26.3, 32.6) | 28.2 (27.2, 33.7) | 28.1 (26.3, 32.6) | 28.0 (26.4, 32.1) | >0.9 | 0.4 |
| GFAP (pg/mL) | 1161 (219, 3349) | 2811 (569, 8611) | 1100 (132, 3310) | 2545 (582, 7356) | 0.026 | 0.087 |
| NFL (pg/mL) | 7.0 (2, 15) | 12.0 (2, 27) | 5.0 (2, 15) | 10.0 (5, 26) | 0.11 | 0.3 |
| Tau (pg/mL) | 0.98 (0.40, 2.31) | 2.84 (1.03, 3.88) | 1.15 (0.40, 2.62) | 1.55 (0.63, 3.44) | 0.3 | 0.017 |
| UCH-L1 (pg/mL) | 24.0 (12, 83) | 53.0 (20, 78) | 30.0 (12, 88) | 40.0 (13, 83) | 0.6 | 0.2 |
| Biomarkers as Median (IQR) | CT Negative N = 44 | CT Positive N = 77 | p-Value (All Severities; Mild, Moderate, Severe) | p-Value (Only Mild TBI) | p-Value (Mild and Moderate) |
|---|---|---|---|---|---|
| S100B (pg/mL) | 28.3 (26.3, 33.0) | 28.0 (26.4, 32.5) | >0.9 | 0.6 | 0.8 |
| GFAP (pg/mL) | 928 (146, 1955) | 1809 (475, 7130) | 0.004 | >0.9 | 0.038 |
| NFL (pg/mL) | 3.0 (2, 10) | 10.0 (4, 22) | 0.002 | 0.2 | 0.005 |
| Tau (pg/mL) | 0.95 (0.39, 1.96) | 1.35 (0.46, 3.14) | 0.2 | 0.4 | 0.7 |
| UCH-L1 (pg/mL) | 21.0 (9, 48) | 42.0 (15, 86) | 0.085 | 0.9 | 0.076 |
| Biomarker as Median (IQR) | Toxoplasma Negative, N = 108 1 | Toxoplasma Positive, N = 52 1 | p-Value 2 |
|---|---|---|---|
| S100B (pg/mL) | 27.2 (24.9, 28.1) | 36.2 (32.6, 37.9) | <0.001 |
| GFAP (pg/mL) | 1651 (351, 5394) | 839 (244, 3360) | 0.4 |
| NFL (pg/mL) | 7.0 (2, 15) | 7.0 (2, 21) | >0.9 |
| Tau (pg/mL) | 1.39 (0.53, 3.39) | 0.82 (0.38, 2.12) | 0.10 |
| UCH-L1 (pg/mL) | 33.0 (13, 94) | 28.0 (10, 68) | 0.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buh, F.C.; Taiwe, G.S.; Kobeissy, F.H.; Wang, K.W.; Maas, A.I.R.; Motah, M.; Meh, B.K.; Youm, E.; Hutchinson, P.J.A.; Sumbele, I.U.N. Serum Biomarker Concentrations upon Admission in Acute Traumatic Brain Injury: Associations with TBI Severity, Toxoplasma gondii Infection, and Outcome in a Referral Hospital Setting in Cameroon. NeuroSci 2023, 4, 164-177. https://doi.org/10.3390/neurosci4030015
Buh FC, Taiwe GS, Kobeissy FH, Wang KW, Maas AIR, Motah M, Meh BK, Youm E, Hutchinson PJA, Sumbele IUN. Serum Biomarker Concentrations upon Admission in Acute Traumatic Brain Injury: Associations with TBI Severity, Toxoplasma gondii Infection, and Outcome in a Referral Hospital Setting in Cameroon. NeuroSci. 2023; 4(3):164-177. https://doi.org/10.3390/neurosci4030015
Chicago/Turabian StyleBuh, Franklin Chu, Germain Sotoing Taiwe, Firas H. Kobeissy, Kevin W. Wang, Andrew I. R. Maas, Mathieu Motah, Basil Kum Meh, Eric Youm, Peter J. A. Hutchinson, and Irene Ule Ngole Sumbele. 2023. "Serum Biomarker Concentrations upon Admission in Acute Traumatic Brain Injury: Associations with TBI Severity, Toxoplasma gondii Infection, and Outcome in a Referral Hospital Setting in Cameroon" NeuroSci 4, no. 3: 164-177. https://doi.org/10.3390/neurosci4030015