
Sound Environment during Dental Treatment in Relation to COVID-19 Pandemic

1
Department of Restorative Dentistry and Endodontology, Osaka University Graduate School of Dentistry, 1-8 Yamadaoka, Suita 565-0871, Osaka, Japan
2
Division for Medical Informatics, Osaka University Dental Hospital, 1-8 Yamadaoka, Suita 565-0871, Osaka, Japan
3
Osaka University, 1-1 Yamadaoka, Suita 565-0871, Osaka, Japan
*
Author to whom correspondence should be addressed.
Acoustics 2023, 5(4), 987-998; https://doi.org/10.3390/acoustics5040056
Submission received: 4 September 2023
/
Revised: 13 October 2023
/
Accepted: 16 October 2023
/
Published: 26 October 2023
(This article belongs to the Special Issue Vibration and Noise)
Abstract
:This study delves into the acoustic environment within dental clinics, particularly focusing on the impact of extraoral suction devices employed for infection control amid the COVID-19 pandemic. The research encompasses a comprehensive investigation, including a questionnaire survey of dental professionals, sound level measurements at suction device openings, acoustic imaging, and a detailed analysis of sound levels and their spectral characteristics during dental procedures. Additionally, ambient sound levels within clinical settings were monitored over two consecutive days. The findings reveal notable observations. Dental professionals expressed concerns regarding increased sound levels and associated distress caused by extraoral suction device operation. Objective measurements identified varying A-weighted sound pressure levels ranging from 86.0 dB to 96.7 dB at suction device openings, highlighting elevated sound pressure levels and a wide frequency range, especially in the vicinity of both the dentist and the patient’s facial area during dental aerosol procedures. On the other hand, for the entire clinical room, the equivalent continuous A-weighted sound pressure level during the consultation hours was not considered problematic. In light of these findings, it becomes evident that there is a pressing necessity to refine the acoustic characteristics of extraoral suction devices to foster a more accommodating acoustic environment for both patients and dental healthcare professionals within dental clinics.
1. Introduction
The Occupational Safety and Health Administration (OSHA) mandates employers to implement hearing conservation programs for their workforce in workplaces where sound levels equal or exceed 85 dB for an eight-hour equivalent continuous A-weighted sound pressure level in dB, referenced to 20 micropascals (LAeq,8h) [1]. Dental facilities are filled with various sounds, and as a result, studies assessing sound levels in dental clinics have been conducted over time. These numerous studies consistently report that dentists’ exposure to noise remains below the threshold for hearing damage risk [2,3,4,5,6,7,8]. However, despite compliance with these standards, further endeavors are warranted to create a comfortable acoustic environment in dental care facilities. Many individuals experience discomfort upon hearing the high-pitched drilling sound associated with dental procedures in a dental clinic [8,9,10,11]. The noise emitted by dental drills can significantly impact the acoustic environment within such clinical settings. Therefore, we have been conducting research with a specific focus on investigating the acoustical characteristics and the factors causing discomfort to patients from dental drilling noise, with a psychoacoustics perspective [11,12,13]. The A-weighted sound pressure level generated by dental drills has been standardized so that it is not expected to exceed 80 dB during idling operation (ISO 14457 [14]). We reported that the unpleasant sensation triggered by dental drill sounds is influenced not solely by the equivalent continuous A-weighted sound pressure level (LAeq) but also by the physical metrics linked to sound quality and prominent frequency components of the noise [12,13].
The COVID-19 pandemic has had a widespread impact on various fields, and it has also significantly affected dentistry [15,16,17]. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of COVID-19, has been detected in saliva [18]. This discovery highlights the potential for asymptomatic COVID-19 carriers among patients, necessitating stringent infection control measures in dentistry. In addition to the Interim Infection Prevention and Control Recommendations for Healthcare Personnel issued by the Centers for Disease Control and Prevention (CDC) [19], new guidelines for dental practices from the Japan Dental Association advocate for the adoption of extraoral suction devices as high-volume evacuators [20]. Osaka University Dental Hospital [21], a prominent national dental hospital in Japan, has strongly encouraged and implemented the use of extraoral suction for all procedures involving droplets and aerosols since the onset of the COVID-19 pandemic for delivering high-quality dental care services. These extraoral suction devices are strategically positioned near patients’ mouths (see Figure 1).
The ongoing research project at Osaka University Dental Hospital aims to create a comfortable environment within dental clinical spaces, catering to the needs of both patients and healthcare professionals [22]. We believe that investigating changes in noise and their impact on healthcare workers during dental treatments is essential. This study encompasses a survey regarding extraoral suction devices involving dentists and dental hygienists working within the clinic. Additionally, we have conducted an analysis of the acoustic characteristics of extraoral suction sounds to gain insights into the current acoustic environment and its effects.
2. Materials and Methods
This study received approval from the Ethics Committee of Osaka University Graduate School of Dentistry and Osaka University Dental Hospital. Informed consent was obtained from all participants.
2.1. Questionnaire Survey
An anonymous survey was administered to dentists working in an outpatient clinic specializing in restorative dentistry and endodontics, as well as dental hygienists at Osaka University Dental Hospital. Participation was voluntary. The questionnaire included the following inquiries:
- “How frequently did you utilize extraoral suction before the COVID-19 pandemic?”
- “Under what circumstances did you use it before the COVID-19 pandemic?”
- “Have you noticed changes in the clinical room’s sound environment compared to before the COVID-19 pandemic?”
- “Are you satisfied with the sound produced by the extraoral suction?”
- “Can you hear other sounds (e.g., voices, drill noise, music, in-hospital broadcasts, telephone, etc.) while using extraoral suction?”
- “Does the sound emitted by the extraoral suction cause you distress?”
Responses were recorded on a 5-point scale for all questions except Question 2, which allowed for free-text descriptions. Participants also provided basic demographic information, including their gender and age group (e.g., 20 s, 30 s, 40 s, and 50 s).
2.2. Measurement of Sound Levels at Extraoral Suction Openings
There are no standard measurement methods for extraoral suction devices. Though the position of the opening of these devices can be adjusted freely, it is typically positioned near the patient’s mouth for aerosol measures, resulting in its proximity to the dentist’s face. Although the sound level at the opening itself may not be at a perceptible level, we investigated the sound level at the opening, because it can serve as a perceptual cue due to the relationship between distance and sound levels. Sound levels (A-weighting, F-time weighting) were measured at the openings of eleven extraoral suction devices in the clinical rooms using a sound level meter (LA-7000, ONO SOKKI Co., Ltd., Yokohama, Japan) [23]. These devices included both mobile and fixed models, with different implementation timing. Measurements were conducted in a quiet room. Fast Fourier transform analysis of the recorded sound (no weighting) was conducted using sound analysis software (ArtemiS SUITE version14, HEAD ACOUSTICS, Herzogenrath, Germany).
2.3. Visualization of Extraoral Suction Sound with Actual Usage Condition
Acoustic imaging of the sound emitted by the extraoral suction was carried out to assess the dispersion of noise of extraoral suction and the positioning of patient and dentist. Mannequins were utilized to simulate a patient and a dentist, positioned on a dental chair unit. The extraoral suction’s opening was placed 15 cm in front of the patient mannequin’s mouth, simulating typical use. An acoustic camera equipped with 64 MEMS microphones (SOUNDCAM 2.0, CAE SOFTWARE UND SYSTEMS GMBH, Gütersloh, Germany) [24] was situated 130 cm in front of the mannequin to represent the dentist. During the measurement, only the extraoral suction was used, and a dental drill and a dental evacuator were not employed.
2.4. Sound Levels Heard by the Dentist during Dental Clinical Treatment with Aerosol Control
We investigated the sounds heard by the dentist during actual dental clinical treatments. Commonly used dental equipment, including the ultrasonic scaler, high-speed dental handpiece, air/water syringe, air polisher, and air abrasion device, generate aerosols and contribute to airborne contamination [25]. We used an extraoral suction device for all these procedures. We placed microphones at both ears of the dentist to record the sounds during treatment. Recording was carried out only with the consent of patients who were provided with explanations. The dentist used a headset with binaural microphones (BHS II, HEAD ACOUSTICS, Herzogenrath, Germany) and recorded sound data with a mobile data acquisition system for sound measurement (SQobold, HEAD ACOUSTICS, Herzogenrath, Germany) [26], as depicted in Figure 2. The recorded sound data were subsequently analyzed using sound analysis software (ArtemiS SUITE version14, HEAD ACOUSTICS, Herzogenrath, Germany).
2.5. Measurement of Sound Levels in the Clinical Room
Sound levels (A-weighting, F-time weighting) were measured in the clinical room for 10 min every hour over the course of two days. Osaka University Dental Hospital is a four-story building housing 19 specialized dental outpatient clinics and dental inpatient wards, equipped with over 200 dental chair units. The sound measurements took place in an outpatient clinic specializing in restorative dentistry and endodontics located on a section of the 3rd floor. A sound level meter (LA-7000, ONO SOKKI Co., Ltd., Yokohama, Japan) was positioned at point A, as indicated in Figure 3, at a height of 120 cm. This positioning ensured that the sound level meter did not interfere with patient movements or treatment procedures and captured not only the sounds of dental treatments but also ambient sounds within the clinical room. The equivalent continuous A-weighted sound pressure level (LAeq) was measured, and sound source analysis was also conducted.
The clinic itself was divided into 16 dental treatment areas with low and high partitions. Each dental chair unit was numbered, as shown in Figure 3. Receptionists were situated in the reception area, which also featured four phones. Four refrigerators containing dental materials were located in the aisle near dental chair units 1 and 2. Sterilized dental instruments needed for dental treatments were stored in metal boxes along the aisle adjacent to dental chair units 10 to 13. An area in front of unit 14 was designated for cleaning dental equipment and sterilizing instruments. These spaces were not fully enclosed private rooms, meaning that sounds could be heard throughout the clinic. The entrance to the clinical room remained open during consultation hours. The clinic serves as an educational facility accommodating dentists, dental hygienists, and dental students, also functioning as an institution for dental education during and after regular consultation hours.
3. Results
3.1. Questionnaire Survey
A total of 45 dental professionals participated in the survey. Data from participants who provided informed consent on the questionnaire sheet were included in the analysis, resulting in responses from 43 dental professionals, including 36 dentists (21 males and 15 females) and seven female dental hygienists across various age groups from their 20 s to 50 s.
Figure 4 illustrates the outcomes of the questionnaire administered to these dental professionals. The responses to Questions 1 and 2 revealed that 90% of the participants infrequently used extraoral suction before the pandemic. The primary reasons for its occasional use were for the removal of shaving powder such as that from temporary teeth or dentures, filling materials, and tartar, rather than for aerosol countermeasures. In response to Question 3, all participants except for one reported that the sound environment had become noisier compared to the pre-COVID-19 pandemic period. Regarding Question 4, none of the respondents selected scale values 1 or 2; instead, more than half of them opted for the highest scale rating of 5, indicating that they perceived the sound of an extraoral suction device as being very noisy. For Question 5, participants noted that it was challenging to hear other sounds due to the noise generated by the extraoral suction. In response to Question 6, which assessed the distress caused by the sound of the extraoral suction device, the results indicated that 70% of the respondents were distressed by the device’s noise. A substantial number of participants found the noise of extraoral suctions not only very noisy but also distressing.
3.2. Measurement of Sound Levels at the Position of the Opening of Extraoral Suctions
The A-weighed sound pressure levels produced by the 11 extraoral suction devices ranged from 86.0 dB to 96.7 dB. Notably, the most recently acquired extraoral suction devices after the COVID-19 pandemic had recorded sound levels over 95 dB. Figure 5a,b depicts the fast Fourier transform (FFT) analysis of the sound of one of the extraoral suction devices. The background noise was 43.9 dB, which included the noise emitted by the refrigerators in the clinical room. The results of FFT indicate that the noise had a wide frequency range, extending up to 20 kHz, in contrast to the background noise.
3.3. Acoustic Imaging of Extraoral Suction Sound with Actual Usage Condition
The acoustic imaging result depicted in Figure 5c focused on the frequency range between 3 kHz and 6 kHz. The image emphasizes the presence of the dentist’s and patient’s faces within the vicinity of the operating extraoral suction device, signifying their exposure to elevated sound levels. The background noise level was registered at 39.8 dB. The acoustic fields are represented by bright spots, with the highest sound pressure level displayed in white, and the lower limit of the set dynamic range is depicted in dark blue. At lower frequencies (below 3 kHz), the acoustic field was extended, whereas at higher frequencies (above 6 kHz), the dispersion range narrowed. Importantly, at various frequency ranges, the areas around the faces of both the dentist and the patient remained enveloped within the noise.
3.4. Sound Quantity and Quality of Noise Heard by the Dentist during Clinical Treatment
We present an illustrative example of the analysis results obtained during a 32-min (1920-s) dental procedure in Figure 6. During the dental procedure, there are variations in the sound level, with fluctuations between louder and quieter moments. In this clinical case, music was playing in the clinical room. The air conditioner was running, and the windows were slightly open for ventilation. The background noise level was 50.2 dB. The suction opening of an extraoral suction device was positioned approximately 15 cm to the left, slightly above the patient’s mouth, resulting in it being at the height of the dentist’s face. The dentist turned the extraoral suction on or off by waving a hand over a sensor near the opening of the extraoral suction as needed during the treatment.
Figure 6a illustrates the amplitude of noise recorded at both ears of the dentist during dental treatment. The occasional increase in amplitude in the left ear (depicted in green) compared to the right ear (indicated in red) can be attributed to the closer proximity of the left ear to the extraoral suction. Figure 6b presents the frequency and intensity of sounds recorded during dental treatment, and Figure 6c represents the variations in A-weighted sound pressure levels. Both datasets in Figure 6b,c were obtained from recordings made at the left ear position. Notably, the periods displaying a colored broad spectrum up to 20 kHz in Figure 6b coincide with the use of the extraoral suction. There are significant variations in frequency characteristics between the periods when the extraoral suction and other equipment were utilized and those during which it was not. In Figure 6c, it can be observed that during these colored spectral periods, indicative of dental treatments involving aerosol procedures, the A-weighted sound pressure level exceeds 80 dB, occasionally approaching 90 dB. It is important to note that the sound level varies significantly during this 32-min dental treatment. The average LAeq over the course of the treatment was 78.2 dB. In Figure 6c, there are intervals between 1680 s and 1800 s when the A-weighted sound pressure level was relatively high. As shown in Figure 6b, the spectrum during this timeframe exhibits characteristics of speech. Further confirmation from the records indicates that during these intervals, the dentist was primarily engaged in providing explanations and instructions to the patient, and despite the elevated sound levels, the dentist did not experience discomfort during this period.
3.5. Sound Levels and Sound Sources in the Clinical Room
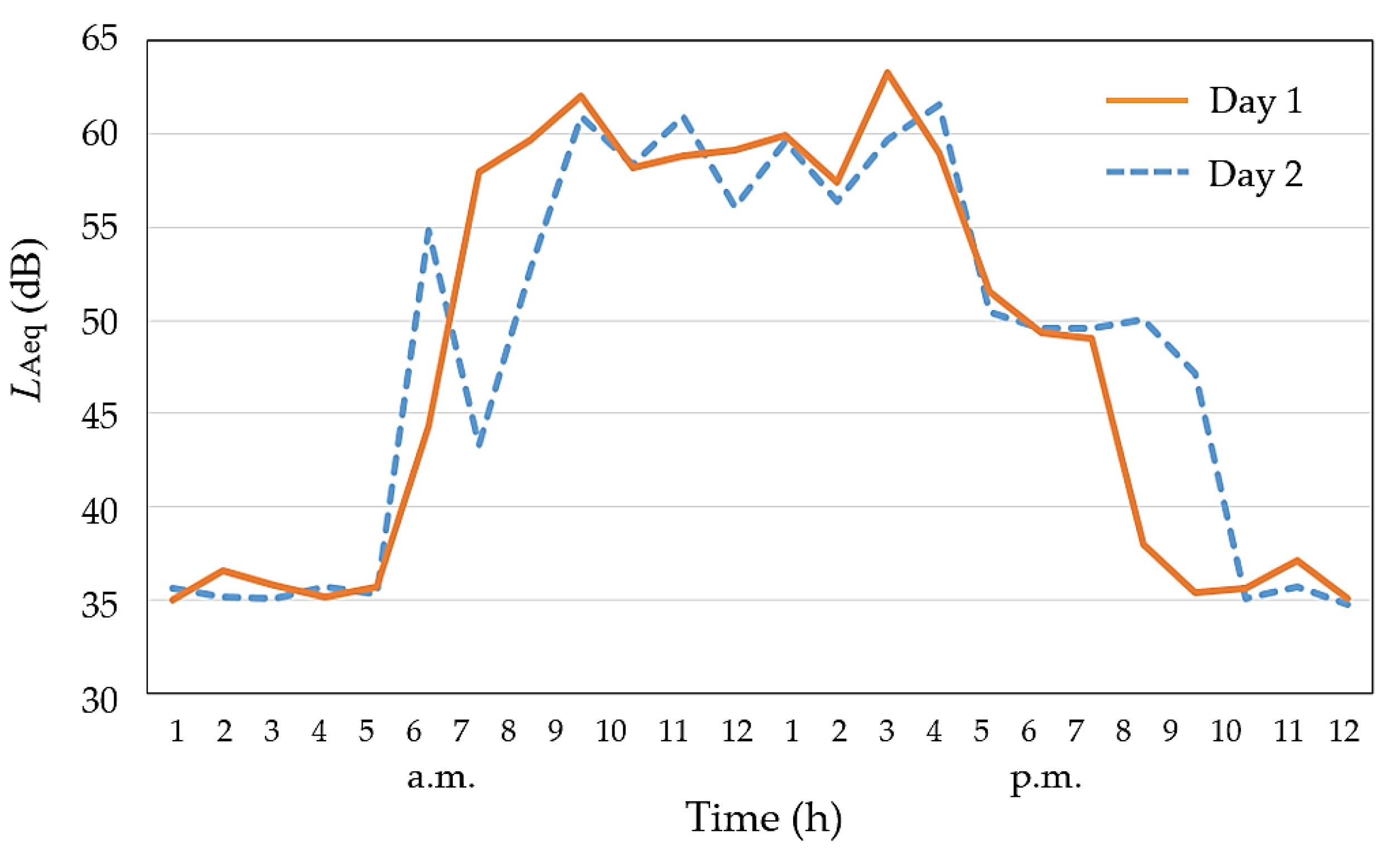
Table 1 presents an hourly breakdown of activities in the clinic where sound measurements were conducted. We conducted a detailed examination of sound sources: Day 1: Prior to the 9 a.m. opening, sounds of cleaning and preparation were audible. Staff exchanged greetings, footsteps were heard, and there were sounds of cleaning the waterlines of dental chair units. Metallic sounds from cleaning instruments clashes were also noticeable. Music started playing in the clinic at 9 a.m. From 9 a.m. to 4 p.m., various treatment sounds, including those from dental evacuators, extraoral suctions, dental drills, ultrasonic scalers, and signal sounds from dental devices, were accompanied by other sounds such as voices, coughing, and ringing telephones. After consultation hours, the sound for maintaining dental chair units and organizing and replenishing dental materials was heard, and dentists and students had time for discussions or training. The room closed at 7 p.m., with post-closing sounds including automatic flushing noises from waterlines, refrigerator noises, and footsteps in the hallway. Day 2 was similar, but cleaning began around 6 o’clock in the morning, and the clinic closed at 8 p.m.
Figure 7 displays the temporal changes in the LAeq of the clinical room over 24 h on Day 1 and Day 2. During both days, most dental chairs were in operation. The A-weighted instantaneous maximum sound level (LAmax) recorded, which reached 88 dB, was due to the sound of dental instruments being dropped during preparation on Day 1. Sound levels during the midnight to early morning hours were consistently very quiet, measuring below 40 dB. The values of LAeq,7h calculated during consultation hours (9 a.m.–4 p.m.) on Day 1 and Day 2 were 59.2 dB and 59.7 dB, respectively. Due to the clinic’s 7 h operating hours, it was not possible to calculate the LAeq,8h here. The results at position A in the clinical room show that being much more than 100 cm away from the nearest dental chair units 11, 12, 15, and 16, the sound level remains relatively quieter than that near dental chairs.
4. Discussion
The COVID-19 pandemic has brought significant changes to the acoustic environment in dental practices. The noise generated by extraoral suction devices, which has a broad frequency range, inadvertently masks essential sounds such as voices and in-hospital broadcasts. Furthermore, it was found that this noise can also obscure sounds like dental drill noise, which has a frequency peak at approximately 6 kHz. This not only affects communication but also poses safety challenges during dental treatment.
Traditionally, infection control measures in dentistry primarily focused on diseases such as hepatitis and AIDS, with an emphasis on preventing contact with blood and mucous membranes. However, the emergence of the COVID-19 pandemic has introduced new challenges to dental practices, highlighting the importance of aerosol infection control measures. In response to the pandemic, extraoral suction has become a key component in infection control measures, primarily aimed at preventing the spread of droplets and aerosols released from the patient’s mouth [25,27,28,29].
Our questionnaire survey results revealed that before the COVID-19 pandemic, extraoral suction devices were primarily used for suctioning dental material powders in the clinical room. Typically, the distance between the ears of the dentist who holds dental materials in hand and the opening of an extraoral suction device was often more than 30 cm. This implies that not only was the frequency of usage lower before the COVID-19 pandemic, but the opening of the device was also positioned away from the dentist’s face, resulting in lower sound levels emitted by the extraoral suction devices that dentists heard. The results of sound levels of extraoral suctions and our acoustic imaging results showed an increase in sound pressure levels around both the patient’s and the dentist’s faces, emphasizing the importance of noise reduction strategies for extraoral suction devices during dental treatments. The sound level at the opening was found to be very high, indicating the presence of a wide range of frequency components. The high sound levels observed corroborate the questionnaire survey results indicating discomfort. Additionally, these results indicate that the impact of the noise of extraoral suctions was localized within a limited range. The manufacturer’s stated A-weighted sound pressure level measurement method was a 100 cm distance, and the opening is oriented in the opposite direction to the position of the sound level meter. When measured under these same conditions, The A-weighted sound pressure level of the noise emitted by the extraoral suction device was approximately 65 dB. These results indicate that noise impact diminishes to some extent when positioned one meter away. However, there is a disconnect from those perceived sound levels by dental professionals and patients.
Many studies on noise in dental facilities have reported that even exposure to sound levels below 85 dB, which are considered the threshold of hearing loss risk in occupational noise exposure [1,30,31], can potentially impact hearing, prompting recommendations for regular hearing assessments and protections [29,32,33,34,35,36,37]. Some studies have specifically highlighted the impact on hearing due to high-frequency components emitted by dental devices [34,35,36,37]. There are several reports on measurements conducted in clinical dental rooms [3,5,6,29]. As several studies focused on measuring the maximum A-weighted sound pressure levels, not the average equivalent continuous A-weighted sound pressure level. Consequently, they reported higher sound levels than our measurements. It is important to note that noise can have the potential to induce both physiological and psychological effects, leading to auditory, cognitive, and sleep disturbances and even cardiovascular issues [38]. In evaluating these results, it is crucial to consider not only the sound level but also the impact of different frequency components. Therefore, further research is necessary to comprehensively investigate both the quantity and quality of noise emitted by dental devices used in conjunction with dental aerosol suction systems during dental treatments, along with their associated physiological and psychological effects.
We acknowledge certain limitations in this study. Firstly, we were unable to calculate measurements based on a full 8 h work shift, which is the standard for occupational noise-induced hearing loss. Although we were unable to provide LAeq,8h, the LAeq,7h values at position A consistently remained below 60 dB during the consultation hours. Additionally, our measurements were conducted at a single location within the clinical room. These limitations will be addressed in future experiments as we continue our research.
5. Conclusions
This study demonstrates that the increased use of extraoral suction devices in response to the COVID-19 pandemic has introduced elevated sound levels into dental clinical settings. These infection control measures are imperative not only for combating COVID-19 but also for addressing potential future infectious diseases, and they will continue to be an integral part of dental clinic practices. These sound levels, combined with other sources of dental equipment noise, have the potential to impact the acoustic comfort of both patients and dental healthcare professionals. Though infection control measures remain essential, addressing acoustic challenges in dental facilities is also crucial. Our results suggest that manufacturers should prioritize noise reduction in the design of these devices. Future research should focus on quieter dental equipment and effective noise control strategies to enhance the dental experience for both patients and professionals.
Author Contributions
Conceptualization, T.Y. and S.K.; methodology, T.Y.; validation, T.Y., K.N., M.H. and S.K.; formal analysis, T.Y. and S.K.; investigation, T.Y.; resources, T.Y., K.N. and M.H.; data curation, T.Y.; writing—original draft preparation, T.Y.; writing—review and editing, T.Y., K.N., M.H. and S.K.; visualization, T.Y. and K.N.; funding acquisition, T.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science, grant number [19K10148, 22K09999].
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Osaka University Graduate School of Dentistry and Osaka University Dental Hospital (protocol code R2-E31, 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
The data required to reproduce this work is included in the paper.
Acknowledgments
The authors extend their sincere thanks to the anonymous reviewers for their valuable contributions and feedback. Additionally, we wish to express our gratitude to H. Shimoda from HEAD Acoustics for their assistance.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Occupational Safety and Health Administration (OSHA). OSHA Technical Manual (OMC), Chapter 5; US Department of Labor: Washington, DC, USA, 2013. Available online: https://www.osha.gov/otm/section-3-health-hazards/chapter-5 (accessed on 10 October 2023).
- Sampaio Fernandes, J.C.; Carvalho, A.P.; Gallas, M.; Vaz, P.; Matos, P.A. Noise levels in dental schools. Eur. J. Dent. Educ. 2006, 10, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Setcos, J.C.; Mahyuddin, A. Noise levels encountered in dental clinical and laboratory practice. Int. J. Prosthodont. 1998, 11, 150–157. [Google Scholar] [PubMed]
- Dierickx, M.; Verschraegen, S.; Wierinck, E.; Willems, G.; van Wieringen, A. Noise Disturbance and Potential Hearing Loss Due to Exposure of Dental Equipment in Flemish Dentists. Int. J. Environ. Res. Public Health 2021, 18, 5617. [Google Scholar] [CrossRef] [PubMed]
- Baseer, M.A.; Al Saffan, A.; AlMasoud, S.M.; Dahy, W.T.; Aldali, H.W.; Walid Bachat, A.M.; Walid Bachat, R.M.; AlMugeiren, O.M. Noise levels encountered in university dental clinics during different specialty treatments. J. Fam. Med. Prim. Care 2021, 10, 2987–2992. [Google Scholar] [CrossRef]
- da Cunha, K.F.; Dos Santos, R.B.; Klien Júnior, C.A. Assessment of noise intensity in a dental teaching clinic. BDJ Open 2017, 3, 17010. [Google Scholar] [CrossRef]
- Goswami, M.; Singh, D.; Vashist, B.; Marwaha, S. Noise levels and sound pollution associated with various operative procedures and equipment in a pediatric dental environment—A clinical study. J. Oral Biol. Craniofac. Res. 2017, 7, 182–187. [Google Scholar] [CrossRef]
- Lehto, T. Dentists’ hearing and exposure to high speed turbine dental drill noise. Proc. Finn. Dent. Soc. 1990, 86, 115–125. [Google Scholar]
- Jiang, P.; Atherton, M.A.; Millar, B.J. A Passive Noise Attenuation Earplug Designed to Minimise Unwanted Air Turbine Driven High-Speed Dental Drill Noise. Eur. J. Prosthodont. Restor. Dent. 2023, 31, 262–277. [Google Scholar]
- Wilson, C.E.; Vaidyanathan, T.K.; Cinotti, W.R.; Cohen, S.M.; Wang, S.J. Hearing-damage Risk and Communication Interference in Dental Practice. J. Dent. Res. 1990, 69, 489–493. [Google Scholar] [CrossRef]
- Yamada, T.; Ebisu, S.; Kuwano, S. A questionnaire survey on the effect of the sound of dental drills on the feeling of patients in dental clinics. Acoust. Sci. Technol. 2006, 27, 305–308. [Google Scholar] [CrossRef]
- Yamada, T.; Kuwano, S.; Ebisu, S.; Hayashi, M. Effect of processing of dental drill noise on subjective impression. Appl. Acoust. 2021, 177, 107895. [Google Scholar] [CrossRef]
- Yamada, T.; Kuwano, S.; Ebisu, S.; Hayashi, M. Statistical analysis for subjective and objective evaluations of dental drill sounds. PLoS ONE 2016, 11, e0159926. [Google Scholar] [CrossRef]
- ISO 14457; Dentistry—Handpieces and Motors. International Organization for Standardization: Geneve, Switzerland, 2017.
- Froum, S.H.; Froum, S.J. Incidence of COVID-19 Virus Transmission in Three Dental Offices: A 6-Month Retrospective Study. Int. J. Periodontics Restor. Dent. 2020, 40, 853–859. [Google Scholar] [CrossRef]
- Wong, C.K.; Tsang, D.N.C.; Chan, R.C.W.; Lam, E.T.K.; Jong, K.K. Infection risks faced by public health laboratory Services Teams when handling specimens associated with coronavirus Disease 2019 (COVID-19). Saf. Health Work 2020, 11, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Kranz, A.M.; Chen, A.; Gahlon, G.; Stein, B.D. 2020 trends in dental office visits during the COVID-19 pandemic. J. Am. Dent. Assoc. 2021, 152, 535–541. [Google Scholar] [CrossRef]
- Iwasaki, S.; Fujisawa, S.; Nakakubo, S.; Kamada, K.; Yamashita, Y.; Fukumoto, T.; Sato, K.; Oguri, S.; Taki, K.; Senjo, H.; et al. Comparison of SARS-CoV-2 detection in nasopharyngeal swab and saliva. J. Infect. 2020, 81, e145–e147. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). 3. Setting-Specific Considerations, Dental Facilities, Interim Infection Prevention and Control Recommendations for Healthcare Personnel during the Coronavirus Disease 2019 (COVID-19) Pandemic; US Department of Health & Human Services: Washington, DC, USA, 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html (accessed on 27 September 2023).
- Japan Dental Association (JDA). Guidelines for Dental Practice Based on New Infectious Diseases, first edition. J. Jpn. Dent. Assoc. 2020, 73, 807–818. (In Japanese) [Google Scholar]
- Osaka University Dental Hospital: Osaka, Japan. Available online: https://hospital.dent.osaka-u.ac.jp/index-e.html (accessed on 27 September 2023).
- Nambu, E.; Nozaki, K.; Tsubokura, M.; Hayashi, M. Numerical simulation of air age in dental offices. Sci. Rep. 2022, 12, 14120. [Google Scholar] [CrossRef]
- Ono Sokki LA-7000, Sound Level Meter. Available online: https://www.onosokki.co.jp/English/hp_e/products/keisoku/s_v/la7000.htm (accessed on 27 September 2023).
- CAE Software und Systems GmbH SoundCam 2.0. Available online: https://soundcam.com/ (accessed on 27 September 2023).
- Matys, J.; Grzech-Leśniak, K. Dental Aerosol as a Hazard Risk for Dental Workers. Materials 2020, 13, 5109. [Google Scholar] [CrossRef]
- Head Acoustics BHS II (Code 3322) Binaural Headset for Aurally Accurate Recording and (with SQobold). Available online: https://cdn.head-acoustics.com/fileadmin/data/en/Data-Sheets/AH-BR/BHS-II-Binaural-Headset-3322-Data-Sheet.pdf (accessed on 27 September 2023).
- Watanabe, J.; Iwamatsu-Kobayashi, Y.; Kikuchi, K.; Kajita, T.; Morishima, H.; Yamauchi, K.; Yashiro, W.; Nishimura, H.; Kanetaka, H.; Egusa, H. Visualization of droplets and aerosols in simulated dental treatments to clarify the effectiveness of oral suction devices. J. Prosthodont. Res. 2023. [Google Scholar] [CrossRef]
- Chavis, S.E.; Hines, S.E.; Dyalram, D.; Wilken, N.C.; Dalby, R.N. Can extraoral suction units minimize droplet spatter during a simulated dental procedure? J. Am. Dent. Assoc. 2021, 152, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Barrett, B.; McGovern, J.; Catanzaro, W.; Coble, S.; Redden, D.; Fouad, A.F. Clinical Efficacy of an Extraoral Dental Evacuation Device in Aerosol Elimination During Endodontic Access Preparation. J. Endodont. 2022, 48, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Guidelines for Preventing Hearing Impairment Due to Noise in Working Space; Ministry of Health, Labour and Welfare: Tokyo, Japan, 2020. Available online: https://www.mhlw.go.jp/content/000628106.pdf (accessed on 27 September 2023). (In Japanese)
- National Institute for Occupational Safety and Health (NIOSH). Criteria for a Recommended Standard: Occupational Exposure to Noise; Revised Criteria; US Department of Health and Human Services: Washington, DC, USA, 1998.
- Al-Rawi, N.H.; Al Nuaimi, A.S.; Sadiqi, A.; Azaiah, E.; Ezzeddine, D.; Ghunaim, Q.; Abbas, Z. Occupational noise-induced hearing loss among dental professionals. Quintessence Int. 2019, 50, 245–250. [Google Scholar]
- Al-Omoush, S.A.; Abdul-Baqi, K.J.; Zuriekat, M.; Alsoleihat, F.; Elmanaseer, W.R.; Jamani, K.D. Assessment of occupational noise-related hearing impairment among dental health personnel. J. Occup. Health. 2020, 62, e12093. [Google Scholar] [CrossRef] [PubMed]
- Mohan, K.M.; Chopra, A.; Guddattu, V.; Singh, S.; Upasana, K. Should Dentists Mandatorily Wear Ear Protection Device to Prevent Occupational Noise-induced Hearing Loss? A Randomized Case-Control Study. J. Int. Soc. Prev. Community Dent. 2022, 12, 513–523. [Google Scholar] [PubMed]
- Henneberry, K.; Hilland, S.; Haslam, S.K. Are dental hygienists at risk for noise-induced hearing loss? A literature review. Can. J. Dent. Hyg. 2021, 55, 110–119. [Google Scholar]
- Myers, J.; John, A.B.; Kimball, S.; Fruits, T. Prevalence of tinnitus and noise-induced hearing loss in dentists. Noise Health 2016, 18, 347–354. [Google Scholar]
- Wilson, J.D.; Darby, M.L.; Tolle, S.L.; Sever, J.C., Jr. Effects of occupational ultrasonic noise exposure on hearing of dental hygienists: A pilot study. J. Dent. Hyg. 2002, 76, 262–269. [Google Scholar]
- Münzel, T.; Gori, T.; Babisch, W.; Basner, M. Cardiovascular effects of environmental noise exposure. Eur. Heart J. 2014, 35, 829–836. [Google Scholar] [CrossRef]
Figure 1.
Extraoral suction device. The suction opening, which can be freely moved, is typically positioned near the patient’s mouth, and activated as needed for specific dental procedures.
Figure 1.
Extraoral suction device. The suction opening, which can be freely moved, is typically positioned near the patient’s mouth, and activated as needed for specific dental procedures.

Figure 2.
A dentist wearing a headset equipped with binaural microphones for recording at the ear position and a mobile data acquisition system.
Figure 2.
A dentist wearing a headset equipped with binaural microphones for recording at the ear position and a mobile data acquisition system.

Figure 3.
Layout of the clinical room used for sound level measurements. A sound level meter for 24 h measurement was positioned at point A.
Figure 3.
Layout of the clinical room used for sound level measurements. A sound level meter for 24 h measurement was positioned at point A.
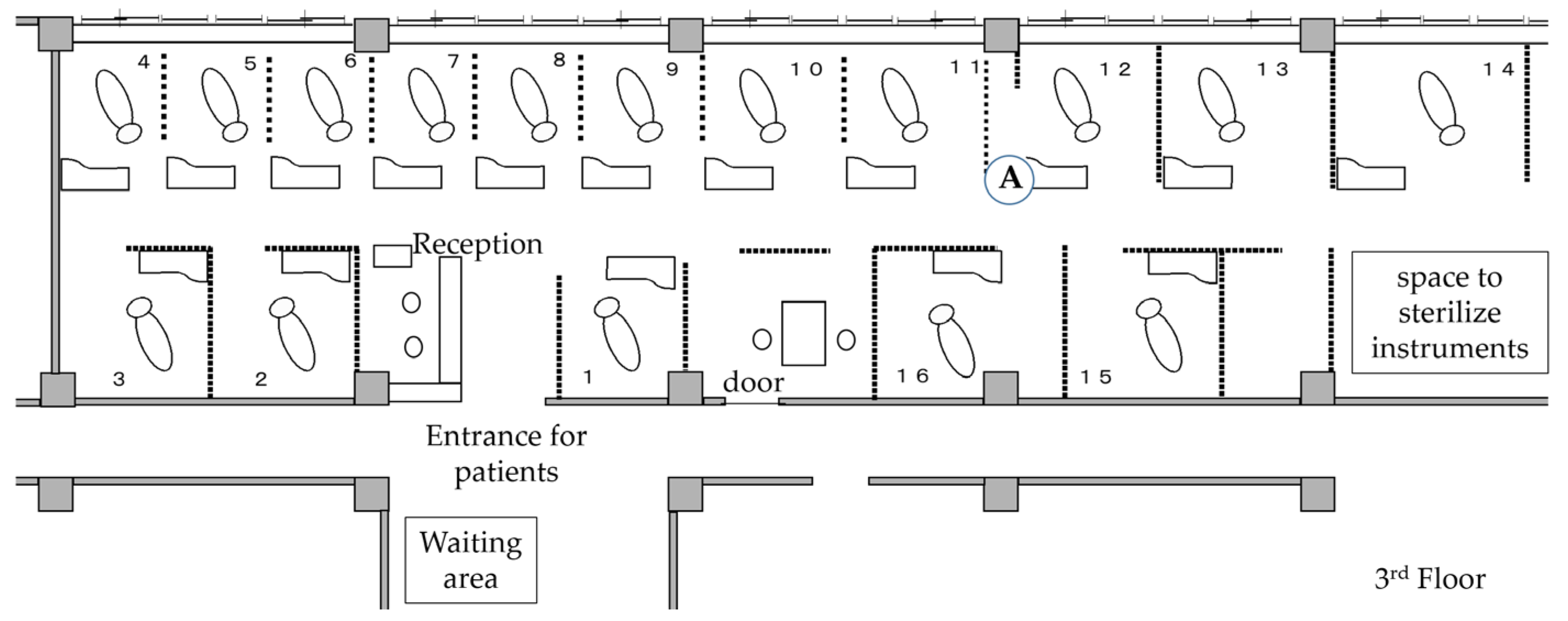
Figure 4.
Responses to the dental professionals’ questionnaire.
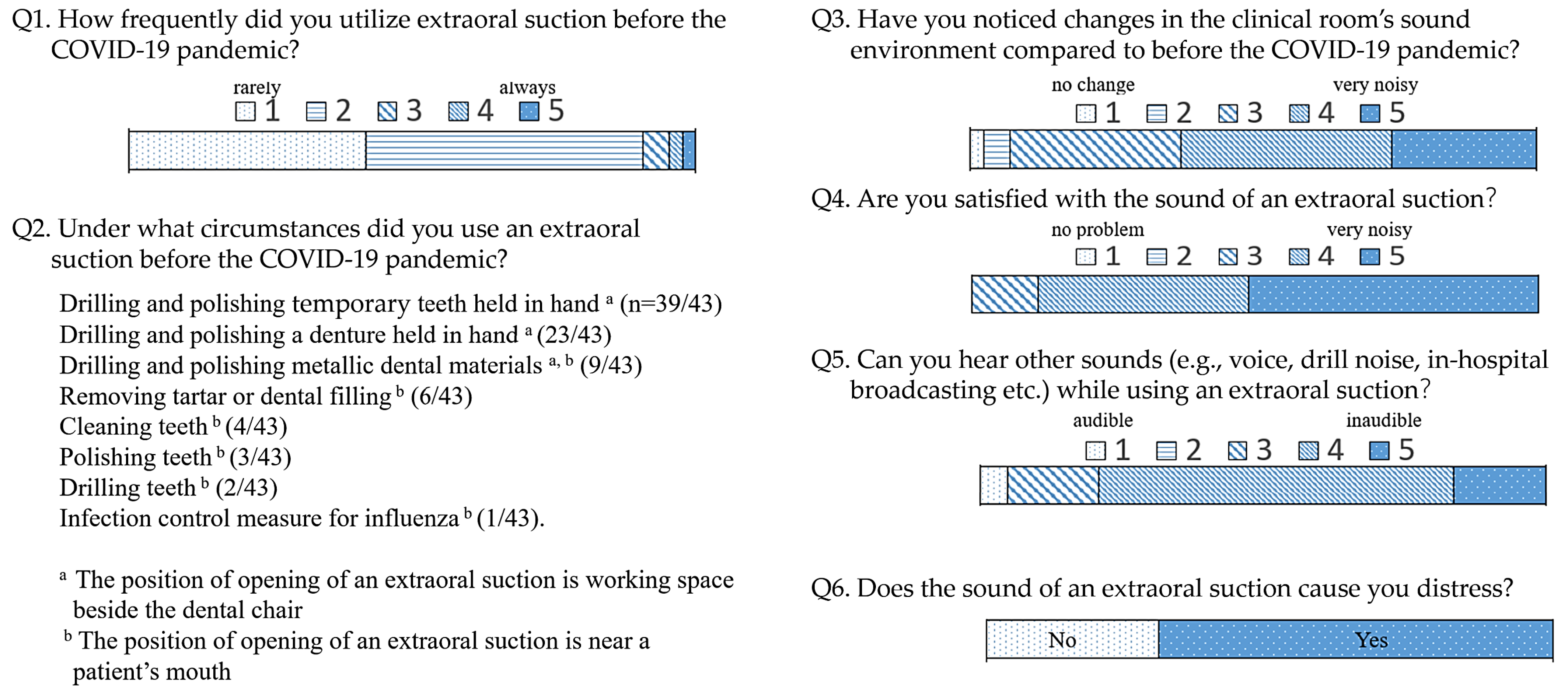
Figure 5.
Characteristics of the noise emitted by an extraoral suction device. (a) Fast Fourier transform analysis (FFT) (Average) of the sound recorded at the extraoral suction opening. The green line represents background noise, while the red line represents the noise generated by the extraoral suction. (b) FFT vs. Time. The color indicates the sound pressure level. (c) An example of acoustic imaging depicting the operational noise of an extraoral suction device. The analyzed frequency range was 3–6 kHz, with a dynamic range of 15 dB SPL.
Figure 5.
Characteristics of the noise emitted by an extraoral suction device. (a) Fast Fourier transform analysis (FFT) (Average) of the sound recorded at the extraoral suction opening. The green line represents background noise, while the red line represents the noise generated by the extraoral suction. (b) FFT vs. Time. The color indicates the sound pressure level. (c) An example of acoustic imaging depicting the operational noise of an extraoral suction device. The analyzed frequency range was 3–6 kHz, with a dynamic range of 15 dB SPL.
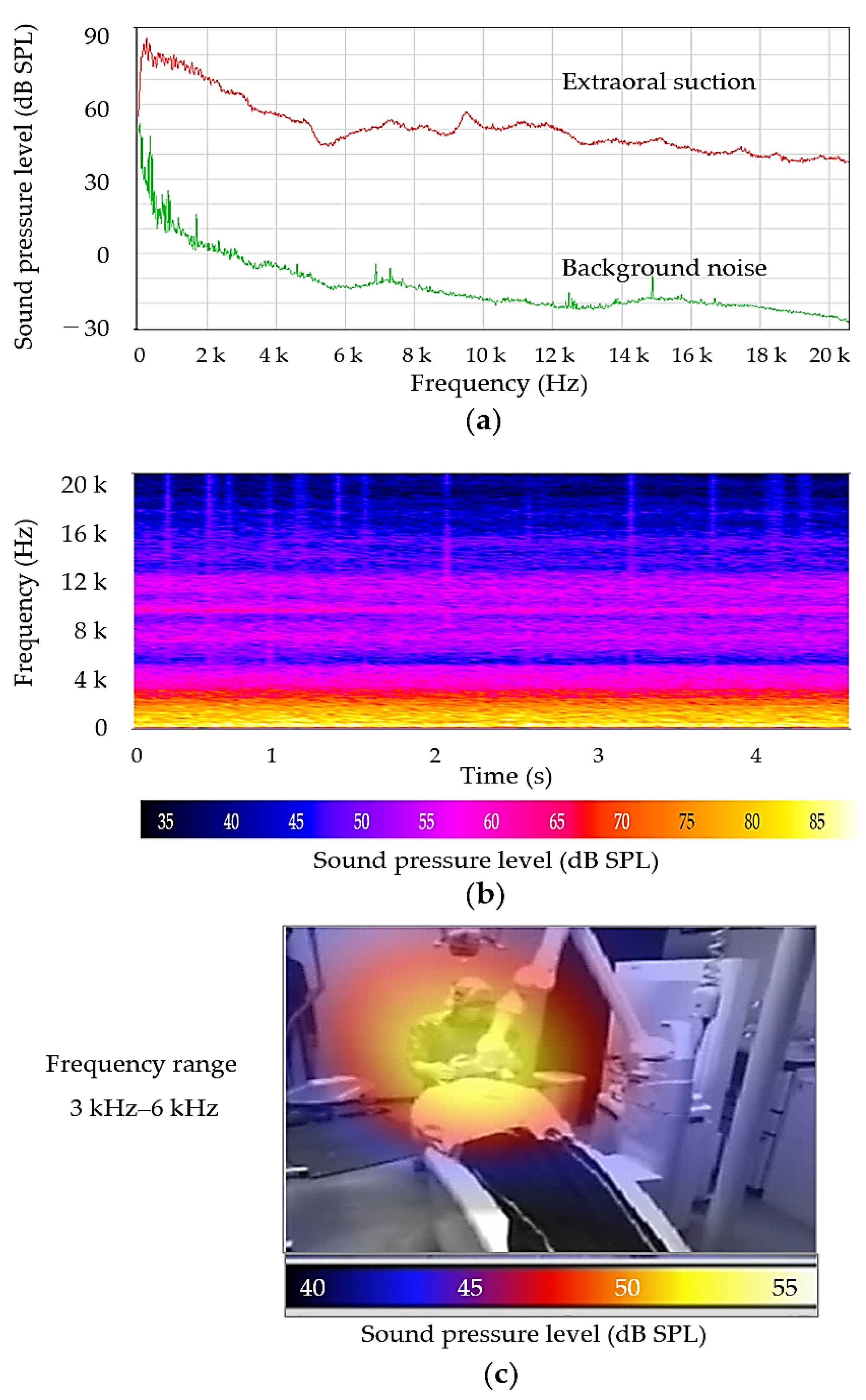
Figure 6.
Variation during a 32-min (1920-s) dental procedure. (a) Amplitude of the sound at both ears of the dentist (green represents the left ear, and red represents the right). (b) FFT (fast Fourier transform) analysis of noise at the left ear. The color indicates the sound pressure level. (c) A-weighted sound pressure levels at the left ear. The average LAeq over the course was 78.2 dB.
Figure 6.
Variation during a 32-min (1920-s) dental procedure. (a) Amplitude of the sound at both ears of the dentist (green represents the left ear, and red represents the right). (b) FFT (fast Fourier transform) analysis of noise at the left ear. The color indicates the sound pressure level. (c) A-weighted sound pressure levels at the left ear. The average LAeq over the course was 78.2 dB.
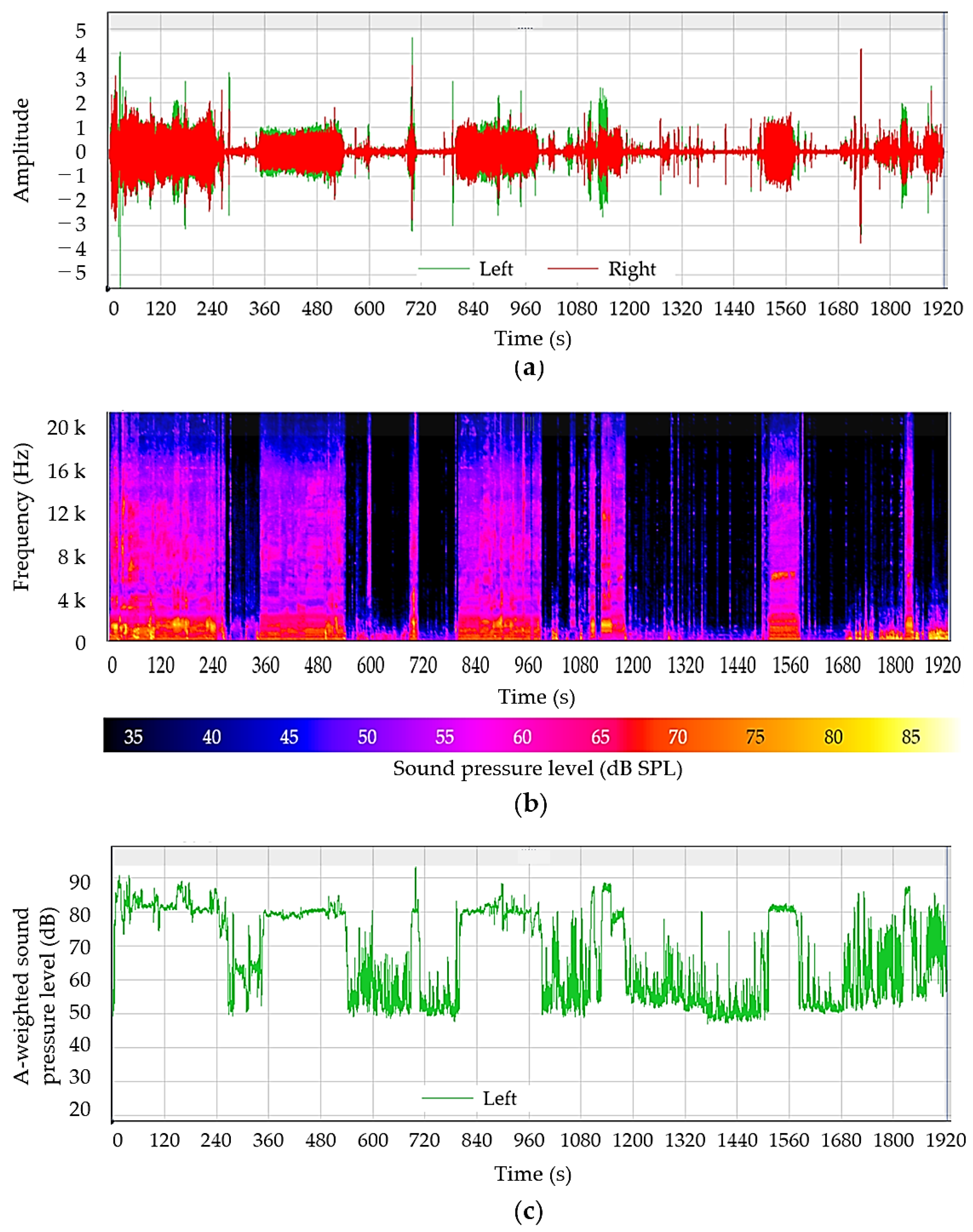
Figure 7.
The temporal changes in the LAeq of the clinical room over 24 h on Day 1 and Day 2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Hourly activities on the measurement days.
| Day 1 | Day 2 | Activity |
|---|---|---|
| 7 a.m. | 6 a.m. | Floor cleaning by cleaning staff |
| 8:30 a.m. | Opening of the clinic for patients Preparation for dental treatment | |
| 9 a.m. | Music broadcast start | |
| 9 a.m.–4 p.m. | Dental examination and treatment | |
| 4:30 p.m. | Music off/clean-up Maintenance of dental chairs and materials | |
| 5 p.m. | Training/discussion for students and dentists | |
| 7 p.m. | 8 p.m. | Close/automatic maintenance |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Yamada, T.; Nozaki, K.; Hayashi, M.; Kuwano, S. Sound Environment during Dental Treatment in Relation to COVID-19 Pandemic. Acoustics 2023, 5, 987-998. https://doi.org/10.3390/acoustics5040056
AMA Style
Yamada T, Nozaki K, Hayashi M, Kuwano S. Sound Environment during Dental Treatment in Relation to COVID-19 Pandemic. Acoustics. 2023; 5(4):987-998. https://doi.org/10.3390/acoustics5040056
Chicago/Turabian StyleYamada, Tomomi, Kazunori Nozaki, Mikako Hayashi, and Sonoko Kuwano. 2023. "Sound Environment during Dental Treatment in Relation to COVID-19 Pandemic" Acoustics 5, no. 4: 987-998. https://doi.org/10.3390/acoustics5040056