
Relationship between Telework Jetlag and Perceived Psychological Distress among Japanese Hybrid Workers
 , , , and
, , , and
Abstract
:1. Introduction
2. Results
2.1. Participant Characteristics
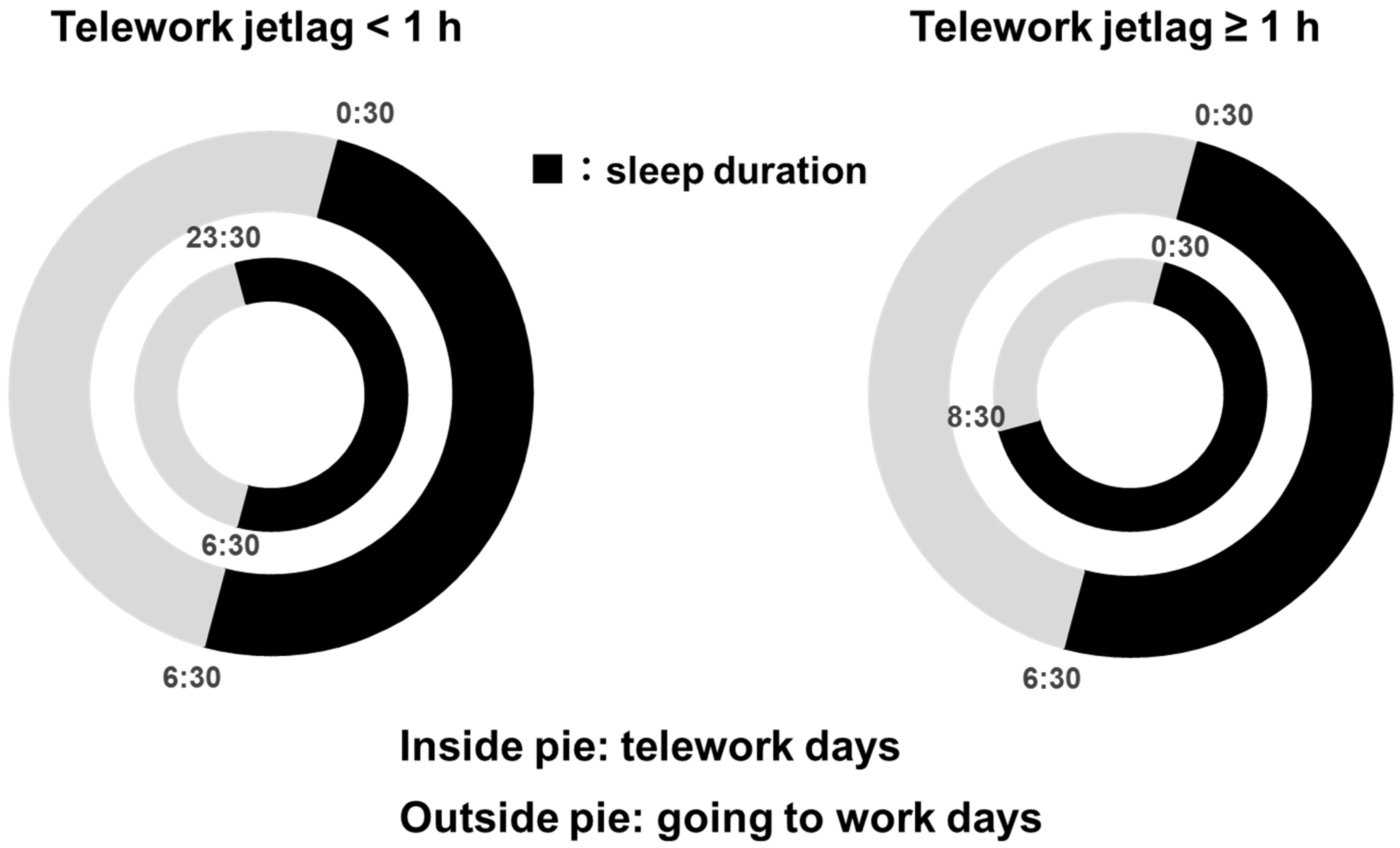
2.2. Prevalence of HPD for Telework Jetlag
2.3. Characteristics of Participants Divided by Telework Jetlag
2.4. Odds Ratio of HPD in Telework Jetlag
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Design, Participants, and Ethical Considerations
5.2. Telework Jetlag and Other Telework Status
5.3. Psychological Distress (Outcome)
5.4. Other Covariates
5.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wittmann, M.; Dinich, J.; Merrow, M.; Roenneberg, T. Social jetlag: Misalignment of biological and social time. Chronobiol. Int. 2006, 23, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Rutters, F.; Lemmens, S.G.; Adam, T.C.; Bremmer, M.A.; Elders, P.J.; Nijpels, G.; Dekker, J.M. Is social jetlag associated with an adverse endocrine, behavioral, and cardiovascular risk profile? J. Biol. Rhythms 2014, 29, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Wirz-Justice, A.; Merrow, M. Life between clocks: Daily temporal patterns of human chronotypes. J. Biol. Rhythms 2003, 18, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Allebrandt, K.V.; Merrow, M.; Vetter, C. Social jetlag and obesity. Curr. Biol. 2012, 22, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Caliandro, R.; Streng, A.A.; van Kerkhof, L.W.M.; van der Horst, G.T.J.; Chaves, I. Social jetlag and related risks for human health: A timely review. Nutrients 2021, 13, 4543. [Google Scholar] [CrossRef]
- Islam, Z.; Akter, S.; Kochi, T.; Hu, H.; Eguchi, M.; Yamaguchi, M.; Kuwahara, K.; Kabe, I.; Mizoue, T. Association of social jetlag with metabolic syndrome among Japanese working population: The Furukawa Nutrition and Health Study. Sleep Med. 2018, 51, 53–58. [Google Scholar] [CrossRef]
- Hu, L.; Harper, A.; Heer, E.; McNeil, J.; Cao, C.; Park, Y.; Martell, K.; Gotto, G.; Shen-Tu, G.; Peters, C.; et al. Social jetlag and prostate cancer incidence in Alberta’s Tomorrow Project: A prospective cohort study. Cancers 2020, 12, 3873. [Google Scholar] [CrossRef]
- Islam, Z.; Hu, H.; Akter, S.; Kuwahara, K.; Kochi, T.; Eguchi, M.; Kurotani, K.; Nanri, A.; Kabe, I.; Mizoue, T. Social jetlag is associated with an increased likelihood of having depressive symptoms among the Japanese working population: The Furukawa Nutrition and Health Study. Sleep 2020, 43, zsz204. [Google Scholar] [CrossRef]
- Mota, M.C.; Silva, C.M.; Balieiro, L.C.T.; Fahmy, W.M.; Marqueze, E.C.; Moreno, C.R.C.; Crispim, C.A. Social jetlag is associated with impaired metabolic control during a 1-year follow-up. Front. Physiol. 2021, 12, 702769. [Google Scholar] [CrossRef]
- Kim, J.H.; Lyu, Y.S.; Kim, S.Y. Impact of social jetlag on weight change in adults: Korean National Health and Nutrition Examination Survey 2016–2017. Int. J. Environ. Res. Public Health 2020, 17, 4383. [Google Scholar] [CrossRef]
- Kelly, R.M.; McDermott, J.H.; Coogan, A.N. Differences in sleep offset timing between weekdays and weekends in 79,161 Adult Participants in the UK Biobank. Clocks Sleep 2020, 4, 658–674. [Google Scholar] [CrossRef] [PubMed]
- Scheer, F.A.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef] [PubMed]
- Archer, S.N.; Laing, E.E.; Möller-Levet, C.S.; van der Veen, D.R.; Bucca, G.; Lazar, A.S.; Santhi, N.; Slak, A.; Kabiljo, R.; von Schantz, M.; et al. Mistimed sleep disrupts circadian regulation of the human transcriptome. Proc. Natl. Acad. Sci. USA 2014, 111, E682–E691. [Google Scholar] [CrossRef] [PubMed]
- Wehr, T.A.; Wirz-Justice, A.; Goodwin, F.K.; Duncan, W.; Gillin, J.C. Phase advance of the circadian sleep-wake cycle as an antidepressant. Science 1979, 206, 710–713. [Google Scholar] [CrossRef]
- Korman, M.; Tkachev, V.; Reis, C.; Komada, Y.; Kitamura, S.; Gubin, D.; Kumar, V.; Roenneberg, T. COVID-19-mandated social restrictions unveil the impact of social time pressure on sleep and body clock. Sci. Rep. 2020, 10, 22225. [Google Scholar] [CrossRef]
- Leone, M.J.; Sigman, M.; Golombek, D.A. Effects of lockdown on human sleep and chronotype during the COVID-19 pandemic. Curr. Biol. 2020, 30, R930–R931. [Google Scholar] [CrossRef]
- Blume, C.; Schmidt, M.H.; Cajochen, C. Effects of the COVID-19 lockdown on human sleep and rest–activity rhythms. Curr. Biol. 2020, 30, R795–R797. [Google Scholar] [CrossRef]
- Bottary, R.; Fields, E.C.; Ugheoke, L.; Denis, D.; Mullington, J.M.; Cunningham, T.J. Changes in sleep regularity and perceived life stress across the COVID-19 Pandemic: A Longitudinal Analysis of a Predominately Female United States Convenience Sample. Clocks Sleep 2022, 5, 1–9. [Google Scholar] [CrossRef]
- Benedict, C.; Brandão, L.E.M.; Merikanto, I.; Partinen, M.; Bjorvatn, B.; Cedernaes, J. Meal and sleep timing before and during the COVID-19 pandemic: A cross-sectional anonymous survey study from Sweden. Clocks Sleep 2021, 3, 251–258. [Google Scholar] [CrossRef]
- Knight, C.; Olaru, D.; Lee, J.; Parker, S. The Loneliness of the Hybrid Worker. MIT Sloan Management Review. 2022. Available online: https://sloanreview.mit.edu/article/the-loneliness-of-the-hybrid-worker/ (accessed on 13 August 2023).
- Buomprisco, G.; Ricci, S.; Perri, R.; De Sio, S. Health and telework: New challenges after COVID-19 pandemic. Eur. J. Public Health 2021, 5, em0073. [Google Scholar] [CrossRef]
- Tavares, A.I. Telework and health effects review. Int. J. Health Care 2017, 3, 30–36. [Google Scholar] [CrossRef]
- Vander Elst, T.; Verhoogen, R.; Sercu, M.; Van den Broeck, A.; Baillien, E.; Godderis, L. Not extent of telecommuting, but job characteristics as proximal predictors of work-related well-being. J. Occup. Environ. Med. 2017, 59, e180–e186. [Google Scholar] [CrossRef] [PubMed]
- Evanoff, B.A.; Strickland, J.R.; Dale, A.M.; Hayibor, L.; Page, E.; Duncan, J.G.; Kannampallil, T.; Gray, D.L. Work-related and personal factors associated with mental well-being during the COVID-19 response: Survey of health care and other workers. J. Med. Internet Res. 2020, 22, e21366. [Google Scholar] [CrossRef] [PubMed]
- Mann, S.; Holdsworth, L. The psychological impact of teleworking: Stress, emotions and health. New Technol. Work Employ. 2003, 18, 196–211. [Google Scholar] [CrossRef]
- Niu, Q.; Nagata, T.; Fukutani, N.; Tezuka, M.; Shimoura, K.; Nagai-Tanima, M.; Aoyama, T. Health effects of immediate telework introduction during the COVID-19 era in Japan: A cross-sectional study. PLoS ONE 2021, 16, e0256530. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Hauret, L.; Fuhrer, C. Digitally transformed home office impacts on job satisfaction, job stress and job productivity. COVID-19 findings. PLoS ONE 2022, 17, e0265131. [Google Scholar] [CrossRef]
- Carillo, K.; Cachat-Rosset, G.; Marsan, J.; Saba, T.; Klarsfeld, A. Adjusting to epidemic-induced telework: Empirical insights from teleworkers in France. Eur. J. Inf. Syst. 2021, 30, 69–88. [Google Scholar] [CrossRef]
- Anderson, A.J.; Kaplan, S.A.; Vega, R.P. The impact of telework on emotional experience: When, and for whom, does telework improve daily affective well-being? Eur. J. Work Organ. Psychol. 2015, 24, 882–897. [Google Scholar] [CrossRef]
- Bailey, D.E.; Kurland, N.B. A review of telework research: Findings, new directions, and lessons for the study of modern work. J. Organ. Behav. 2002, 23, 383–400. [Google Scholar] [CrossRef]
- Shin, B.; El Sawy, O.A.; Sheng, O.R.L.; Higa, K. Telework: Existing research and future directions. J. Organ Comput. Electron. Commer 2000, 10, 85–101. [Google Scholar] [CrossRef]
- Chirico, F.; Zaffina, S.; Di Prinzio, R.R.; Girogi, G.; Ferrari, G.; Capitanelli, I.; Sacco, A.; Szarpak, L.; Nucera, G.; Taino, G.; et al. Working from home in the context of COVID-19: A systematic review of physical and mental health effects on teleworkers. J. Health Soc. Behav. 2021, 6, 319–332. [Google Scholar] [CrossRef]
- Moglia, M.; Hopkins, J.; Bardoel, A. Telework, hybrid work and the United Nation’s Sustainable Development Goals: Towards policy coherence. Sustainability 2021, 13, 9222. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Comprehensive Survey of Living Conditions in 2019. Available online: https://www.mhlw.go.jp/toukei/saikin/hw/k-tyosa/k-tyosa19/index.html (accessed on 13 August 2023). (In Japanese).
- Breslau, N.; Peterson, E.L.; Schultz, L.R.; Chilcoat, H.D.; Andreski, P. Major depression and stages of smoking. A longitudinal investigation. Arch Gen Psychiatry 1998, 55, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Churchill, S.A.; Farrell, L. Alcohol and depression: Evidence from the 2014 health survey for England. Drug Alcohol Depend. 2017, 180, 86–92. [Google Scholar] [CrossRef]
- Gordon, B.R.; McDowell, C.P.; Lyons, M.; Herring, M.P. The effects of resistance exercise training on anxiety: A meta-analysis and meta-regression analysis of randomized controlled trials. Sports Med. 2017, 47, 2521–2532. [Google Scholar] [CrossRef]
- Roenneberg, T.; Kuehnle, T.; Juda, M.; Kantermann, T.; Allebrandt, K.; Gordijn, M.; Merrow, M. Epidemiology of the human circadian clock. Sleep Med. Rev. 2007, 11, 429–438. [Google Scholar] [CrossRef]
- Roenneberg, T.; Pilz, L.K.; Zerbini, G.; Winnebeck, E.C. Chronotype and social jetlag: A (self-) critical review. Biology 2019, 8, 54. [Google Scholar] [CrossRef]
- Jankowski, K.S. Social jet lag: Sleep-corrected formula. Chronobiol. Int. 2017, 34, 531–535. [Google Scholar] [CrossRef]
- Okajima, I.; Komada, Y.; Ito, W.; Inoue, Y. Sleep debt and social jetlag associated with sleepiness, mood, and work performance among workers in Japan. Int. J. Environ. Res. Public. Health 2021, 18, 2908. [Google Scholar] [CrossRef]
- Taylor, A.; Wright, H.R.; Lack, L.C. Sleeping-in on the weekend delays circadian phase and increases sleepiness the following week. Sleep Biol. Rhythm. 2008, 6, 172–179. [Google Scholar] [CrossRef]
- Lee, A.; Myung, S.K.; Cho, J.J.; Jung, Y.J.; Yoon, J.L.; Kim, M.Y. Night shift work and risk of depression: Meta-analysis of observational studies. J. Korean Med. Sci. 2017, 32, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Roenneberg, T.; Kuehnle, T.; Pramstaller, P.P.; Ricken, J.; Havel, M.; Guth, A.; Merrow, M. A marker for the end of adolescence. Curr. Biol. 2004, 14, R1038–R1039. [Google Scholar] [CrossRef] [PubMed]
- Germain, A.; Kupfer, D.J. Circadian rhythm disturbances in depression. Hum. Psychopharmacol. 2008, 23, 571–585. [Google Scholar] [CrossRef] [PubMed]
- Salgado-Delgado, R.; Tapia Osorio, A.; Saderi, N.; Escobar, C. Disruption of circadian rhythms: A crucial factor in the etiology of depression. Depress. Res. Treat. 2011, 2011, 839743. [Google Scholar] [CrossRef] [PubMed]
- Morris, C.J.; Purvis, T.E.; Hu, K.; Scheer, F.A. Circadian misalignment increases cardiovascular disease risk factors in humans. Proc. Natl. Acad. Sci. USA 2016, 113, E1402–E1411. [Google Scholar] [CrossRef]
- Moret, C.; Briley, M. The importance of norepinephrine in depression. Neuropsychiatr. Dis. Treat. 2011, 7, 9–13. [Google Scholar] [CrossRef]
- Herbert, J. Cortisol and depression: Three questions for psychiatry. Psychol. Med. 2013, 43, 449–469. [Google Scholar] [CrossRef]
- Roenneberg, T.; Merrow, M. The circadian clock and human health. Curr. Biol. 2016, 26, R432–R443. [Google Scholar] [CrossRef]
- Kronfeld-Schor, N.; Visser, M.E.; Salis, L.; van Gils, J.A. Chronobiology of interspecific interactions in a changing world. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2017, 372, 20160248. [Google Scholar] [CrossRef]
- Souetre, E.; Salvati, E.; Wehr, T.A.; Sack, D.A.; Krebs, B.; Darcourt, G. Twenty-four-hour profiles of body temperature and plasma TSH in bipolar patients during depression and during remission and in normal control subjects. Am. J. Psychiatry 1988, 145, 1133–1137. [Google Scholar] [CrossRef]
- Steiner, M.; Brown, G.M.; Goldman, S. Nocturnal melatonin and cortisol secretion in newly admitted psychiatric inpatients. Eur. Arch. Psychiatry Clin. Neurosci. 1990, 240, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Peeters, F.; Berkhof, J.; Delespaul, P.; Rottenberg, J.; Nicolson, N.A. Diurnal mood variation in major depressive disorder. Emotion 2006, 6, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Buhr, E.D.; Yoo, S.H.; Takahashi, J.S. Temperature as a universal resetting cue for mammalian circadian oscillators. Science 2010, 330, 379–385. [Google Scholar] [CrossRef] [PubMed]
- McClung, C.A. Circadian genes, rhythms and the biology of mood disorders. Pharmacol. Ther. 2007, 114, 222–232. [Google Scholar] [CrossRef] [PubMed]
- Tsang, A.H.; Barclay, J.L.; Oster, H. Interactions between endocrine and circadian systems. J. Mol. Endocrinol. 2014, 52, R1–R16. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Andrews, G.; Colpe, L.; Hiripi, È.; Mroczek, D.K.; Normand, S.-L.T.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H.; et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef]
- Sakurai, K.; Nishi, A.; Kondo, K.; Yanagida, K.; Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 2011, 65, 434–441. [Google Scholar] [CrossRef]
- Shimomitsu, T. The Final Development of the Brief Job Stress Questionnaire Mainly Used for Assessment of the Individuals. In Ministry of Labour Sponsored Grant for the Prevention of Work-Related Illness: The 1999 Report; CiNii Research: Tokyo, Japan, 2000; pp. 126–164. (In Japanese) [Google Scholar]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Okajima, I.; Nakajima, S.; Kobayashi, M.; Inoue, Y. Development and validation of the Japanese version of the Athens Insomnia Scale. Psychiatry Clin. Neurosci. 2013, 67, 420–425. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | n | % | ||
|---|---|---|---|---|
| Sex | ||||
| Men | 1231 | 68.8 | ||
| Women | 558 | 31.2 | ||
| Age | ||||
| 20–29 | 285 | 15.9 | ||
| 30–39 | 389 | 21.7 | ||
| 40–49 | 477 | 26.7 | ||
| 50–59 | 537 | 30.0 | ||
| ≥60 | 101 | 5.6 | ||
| Living alone | ||||
| No | 1302 | 72.8 | ||
| Yes | 487 | 27.2 | ||
| Occupation | ||||
| Clerks | 337 | 18.8 | ||
| Engineers | 379 | 21.2 | ||
| Field workers | 67 | 3.7 | ||
| Creators | 115 | 6.4 | ||
| Customer service | 69 | 3.9 | ||
| Sales | 716 | 40.0 | ||
| Other | 106 | 5.9 | ||
| Employment position | ||||
| Manager or director | 114 | 6.4 | ||
| Chief | 341 | 19.1 | ||
| Supervisor | 266 | 14.9 | ||
| Regular employee | 1068 | 59.7 | ||
| Commuting time | ||||
| <1 h | 1130 | 63.2 | ||
| ≥1 h | 659 | 36.8 | ||
| Means of commuting | ||||
| Crowded train | 961 | 53.7 | ||
| Uncrowded train | 453 | 25.3 | ||
| On foot | 189 | 10.6 | ||
| Other | 186 | 10.4 | ||
| Work hours in the past 1 month | ||||
| <160 h/m | 515 | 28.8 | ||
| ≥160 and <200 h/m | 954 | 53.3 | ||
| ≥200 h/m | 320 | 17.9 | ||
| Lifestyle | n | % | ||
| Exercise habits | ||||
| Not physically active and no intention to change | 172 | 9.6 | ||
| Not active but intending to change | 442 | 24.7 | ||
| Perform some activity but not enough | 643 | 35.9 | ||
| Regularly active but not in the habit | 235 | 13.1 | ||
| Regularly active in the habit | 297 | 16.6 | ||
| Drinking alcohol | ||||
| Never or rarely | 611 | 34.2 | ||
| Less than 2 d/wk | 484 | 27.1 | ||
| 3–6 d/wk | 364 | 20.3 | ||
| Every day | 330 | 18.4 | ||
| Consumption of caffeine | ||||
| Never or rarely | 155 | 8.7 | ||
| 2–6 d/wk | 331 | 18.5 | ||
| Every day but less than twice a day | 826 | 46.2 | ||
| Every day and more than three times a day | 477 | 26.7 | ||
| Current smoker | ||||
| No | 1321 | 73.8 | ||
| Yes | 468 | 26.2 | ||
| Using electronic terminal outside of work | ||||
| <2 h/d | 860 | 48.1 | ||
| ≥2 h/d | 929 | 51.9 | ||
| Enjoying leisure time | ||||
| Yes | 1171 | 65.5 | ||
| No | 618 | 34.5 | ||
| Sleep duration | ||||
| ≥7 h | 1108 | 61.9 | ||
| <7 h | 681 | 38.1 | ||
| Telework Frequency | n | % |
|---|---|---|
| 1–3 d/m | 321 | 17.9 |
| 1–2 d/wk | 436 | 24.4 |
| 3–4 d/wk | 626 | 35.0 |
| ≥5 d/wk | 406 | 22.7 |
| Telework location | ||
| Living room | 843 | 47.1 |
| Private room | 410 | 22.9 |
| Bedroom | 409 | 22.9 |
| Other | 127 | 7.1 |
| Telework duration | ||
| <1 y | 253 | 14.1 |
| ≥1 y and <1.5 y | 566 | 31.6 |
| ≥1.5 y | 970 | 54.2 |
| Telework jetlag | ||
| <1 h | 1557 | 87.0 |
| ≥1 h | 232 | 13.0 |
| n | % | Mean | SD | |
|---|---|---|---|---|
| Psychological distress | ||||
| NHPD (K6 score < 10) | 1524 | 85.2 | ||
| HPD (K6 score ≥ 10) | 265 | 14.8 | ||
| AIS score | ||||
| <6 | 1150 | 64.3 | ||
| ≥6 | 639 | 35.7 | ||
| Job stressors and social supports | ||||
| Job demands | 8.6 | 1.9 | ||
| Job control | 8.7 | 1.7 | ||
| Supervisor support | 8.1 | 2.2 | ||
| Coworker support | 8.4 | 2.1 |
| Psychological Distress; n (%) | ||||
|---|---|---|---|---|
| Total | NHPD | HPD | p-Value | |
| Telework jetlag | <0.001 * | |||
| <1 h | 1557 | 1343 (86.3) | 214 (13.7) | |
| ≥1 h | 232 | 181 (78.0) | 51 (22.0) | |
| Model 1 | Model 2 | Model 3 | Model 4 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95%CI | OR | 95%CI | OR | 95%CI | OR | 95%CI | ||
| Telework jetlag | |||||||||
| <1 h | 1.00 | 1.00 | 1.00 | 1.00 | |||||
| ≥1 h | 1.82 | 1.26–2.62 | 1.68 | 1.13–2.49 | 1.73 | 1.14–2.63 | 1.80 | 1.16–2.79 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumoto, Y.; Hino, A.; Kumadaki, K.; Itani, O.; Otsuka, Y.; Kaneita, Y. Relationship between Telework Jetlag and Perceived Psychological Distress among Japanese Hybrid Workers. Clocks & Sleep 2023, 5, 604-614. https://doi.org/10.3390/clockssleep5040040
Matsumoto Y, Hino A, Kumadaki K, Itani O, Otsuka Y, Kaneita Y. Relationship between Telework Jetlag and Perceived Psychological Distress among Japanese Hybrid Workers. Clocks & Sleep. 2023; 5(4):604-614. https://doi.org/10.3390/clockssleep5040040
Chicago/Turabian StyleMatsumoto, Yuuki, Ayako Hino, Kunitaka Kumadaki, Osamu Itani, Yuichiro Otsuka, and Yoshitaka Kaneita. 2023. "Relationship between Telework Jetlag and Perceived Psychological Distress among Japanese Hybrid Workers" Clocks & Sleep 5, no. 4: 604-614. https://doi.org/10.3390/clockssleep5040040