1. Introduction
Acute aortic dissection is a rare but lethal cardiac disease involving the aorta, which incident rate is reported as being 11/100,000 individuals [
1]. Its typical symptoms include the acute onset of severe chest or back pain, which can be severe, sharp, or tearing. Although tearing chest pain is a typical symptom, other unspecific symptoms may be present, such as epigastric pain, nausea, and vomiting. Neurologic symptoms are also present in rare cases and often lead to delate diagnosis because they mimic stroke and intracranial hemorrhage. Therefore, it is important to understand acute aortic dissection-induced neurologic symptoms.
Here, we present a case of a 60-year-old male who presented with an acute onset of progressive flaccid hemiplegia on the left side, accompanied with slurred speech. Brain computed tomography showed widening of the cortical sulci and dilatation of the ventricles, without intracranial hemorrhage. When waiting for thrombolysis or thrombectomy intervention, acute chest pain was noted. An emergency computed tomography angiography was done and revealed type A dissection from the ascending aorta with extension to the right external iliac artery, which also involved the brachiocephalic trunk, left common carotid artery, celiac trunk, superior mesenteric artery, and right renal artery. This paper describes the clinical features of type A dissection, especially the neurological symptoms, and highlights the importance of early diagnosis and timely intervention for type A dissection patients.
2. Case Presentation Section
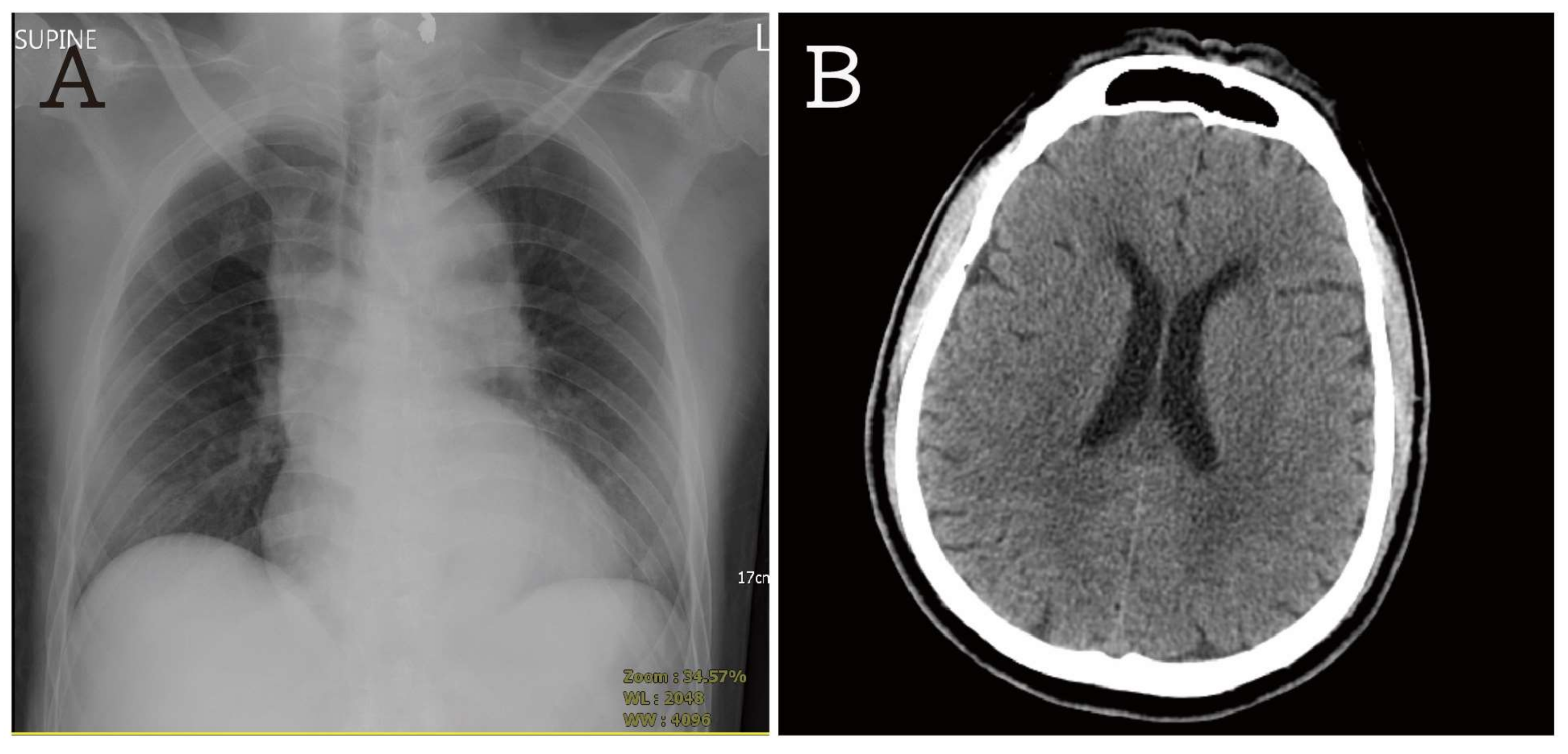
A 60-year-old male presented with acute onset of progressive flaccid hemiplegia on the left side, accompanied with slurred speech. His past medical history revealed poor controlled hypertension for five years. There was no history of trauma. He denied any infection sign, such as fever, chills, cough, nausea, vomiting, and diarrhea. Chest pain or tightness were not reported. There was no neurologic symptom, such as eye deviation, nystagmus, facial paralysis, dysarthria, or saliva drooling. His vital sign revealed a temperature of 36.1 °C, heart rate of 70 beats/min, respiratory rate of 20 breaths/min and blood pressure 136/59 mm Hg. On physical examination, the muscle power of the left extremity decreased and was asymmetric (the muscle strength in the upper extremities was 1/5, but that of the lower extremities was 1/5). The extraocular motion was not checked because the patient could not comply. Laboratory data were collected to rule out infection diseases; the results were: white cell count of 13,970/µL (segment form neutrophils 70.3%, lymphocytes 21.8%, eosinophils 1.1%, and monocytes 6.4%), hemoglobin 10.6 g/dL, platelet counts 180,000/mL, creatinine 1.3 mg/dL, sodium 137 mmol/L, potassium 2.7 mmol/L, glucose 144 mg/dL, alanine aminotransferase 30 U/L, Troponin I < 0.01 µg/L, PT: 12.3 s, APTT: 33.1 s, and INR: 1.19. The electrocardiogram revealed a normal sinus rhythm and prolonged QT. The supine anteroposterior chest view showed widening of the mediastinum (
Figure 1A). Brain computed tomography showed widening of the cortical sulci and dilatation of the ventricles, without intracranial hemorrhage (
Figure 1B). According to the above clinical symptoms and images, a stroke was suspected initially. The neurologists were consulted for thrombolysis or thrombectomy.
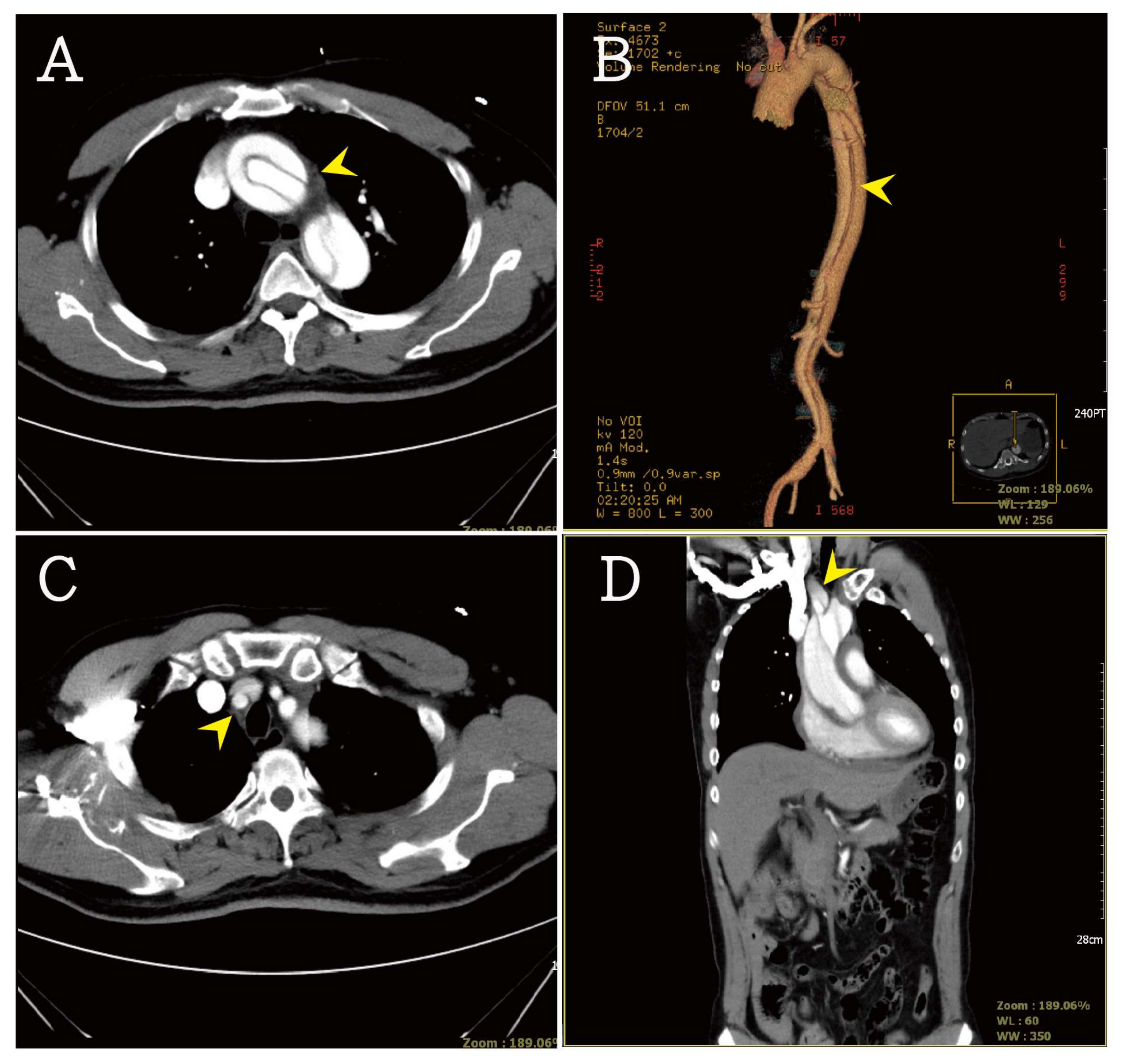
Acute chest pain was noted while waiting for the thrombolysis intervention. An emergency computed tomography angiography was carried out and revealed type A dissection (Stanford classification) from the ascending aorta to the right external iliac artery in the CT scan (
Figure 2A,B). The aortic dissection also involved the brachiocephalic trunk, left common carotid artery, celiac trunk, superior mesenteric artery, and right renal artery (
Figure 2C,D). The hemopericardium was also noted.
According to the above clinical symptoms and images, a type A dissection was suspected. An emergency ascending aorta replacement was arranged. However, during the surgery, a sudden onset of cardiac arrest was noted. Transesophageal echocardiography showed massive pericardic effusion. Resuscitative thoracotomies and open chest cardiac compressions were done. However, recurrent ventricular tachycardia and ventricular fibrillation were noted. After defibrillation and extracorporeal membrane oxygenation (ECMO) setup, the patient was transferred to ICU. Because of the poor outcome, the family asked to remove the patient from ECMO. The patient expired. A written informed consent was obtained from the patient.
3. Discussion
Initial presentation with neurologic symptoms in aortic dissection patients has been rarely reported in previous studies and presents a frequency of about 37.7% [
2,
3,
4]. The predominant neurological symptoms can make it difficult for physicians to diagnose aortic dissection. Misdiagnosis or delayed diagnosis of aortic dissection may lead to catastrophic mortality and morbidity. In these patients, thrombolysis or thrombectomy, which are considered as the emergency stroke therapy, may be life-threatening in case of misdiagnosis of aortic dissection [
5]. Regularly considering the possibility of aortic dissection is important for physicians to manage atypical stroke patients. Routine chest X-ray and physical examination are suggested as the first steps to include or exclude a diagnosis of aortic dissection, especially for patients presenting with hypotension, asymmetrical pulses, or heart murmur [
6]. The initial neurological symptoms in type A aortic dissection were analyzed by Charly Gaul et al. [
7], who described ischemic stroke (15.7%), spinal cord ischemia (1%), ischemic neuropathy (10.8%), hypoxic encephalopathy (2%), and syncope (5.9%). The onset of the neurological symptoms may result from the extension of the dissection to aortic arch vessels, such as the brachiocephalic trunk and the left common carotid artery. The sudden onset of reduced cerebral perfusion and false lumen compressing the neurologic systems is also involved. In the study of Yuji Shono et al. [
5], the involvement of supra-aortic artery and innominate artery was found in 100.0% of type A aortic dissection patients with CNS symptoms. The involvement of the common carotid artery and left subclavian artery was 63.6% and 36.4%, respectively. The involvement of the supra-aortic artery and innominate artery was significant in patients presenting with neurological symptoms.
Hypertension is the most common presentation in acute stroke patients. In a nationally representative large data study, 69% of acute stroke patients had a systolic blood pressure (SBP) higher than 139 mm Hg [
8]. A similar result was reported in the study of J. D. Wallace et al. [
9], which revealed that SBP higher than 150 mm Hg was measured in 84% patients [
9]. Compared to Yuji Shono et al. [
5] analysis, the SBP of aortic dissection patients with neurological symptoms was 114.9 ± 28.9 mm Hg (mean ± SD), and the diastolic blood pressure was 66.5 ± 17.3 mm Hg (mean ± SD). No significant hypertension was reported. In our case, the initial blood pressure was 136/59 mm Hg, with no presentation of hypertension. In patients with neurological symptoms, the presentation of hypertension may be a sign pointing to a diagnosis of stroke.
Serum D-dimer, a fibrin degradation product, is a useful diagnostic tool for deep venous thrombosis, pulmonary embolism, and acute aortic dissection [
10]. A cut-off value, reported for rule-out purposes, is 500 ng/mL that is similar to that indicated for pulmonary embolism and acute aortic dissection [
10,
11,
12]. Using a cut-off value of 500 ng/mL for acute aortic dissection, the analysis revealed a sensitivity of 97%, a negative predictive value of 96%, a specificity of 56%, a positive predictive value of a 60%, positive likelihood ratio of 2.43, and a negative likelihood ratio of 0.06 [
11,
12]. A concentration of serum D-dimer <500 ng/mL is a sensitive screening tool for acute aortic dissection. However, in stroke patients, serum D-dimer is also increased. In 2002, Walter Ageno et al. [
13] reported the serum D-dimer concentration in three major stroke subtypes: cardioembolic (mean ± SEM: 2960 ± 510 ng/mL), atherothrombotic (mean ± SEM: 1340 ± 210 ng/mL), and lacunar (mean ± SEM: 670 ± 80 ng/mL). Serum D-dimer concentration cannot be used to differentiate the diagnosis of stroke and aortic dissection but is a useful rule-out tool for stroke and aortic dissection. Because of the above reasons, we did not measure serum D-dimer concentration in our patient. In our case, we highlighted the clinical features of acute aortic dissection which may be present together with neurological symptoms mimicking stroke and intracranial hemorrhage. We believe that the increased level of serum D-dimer may be significantly different in stroke and aortic dissection patients. This hypothesis needs to be confirmed by further studies. Although no known parameter is useful to provide strong evidence to distinguish these two diseases, a close follow-up of new symptoms, continuous monitoring of vital signs, early image studies, and timely medical and surgical interventions may improve patients’ outcome.

 ,
, 
{kind=link}
{kind=link}

