
SPHYNCS: The Use of the Swiss Narcolepsy Scale in a New Cohort of Patients with Narcolepsy and Its Borderland and Review of the Literature
 , , , , , ,
, , , , , ,  , , , , , , , , ,
, , , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cohort of the Study
2.2. Procedures and Statistical Analysis
3. Results
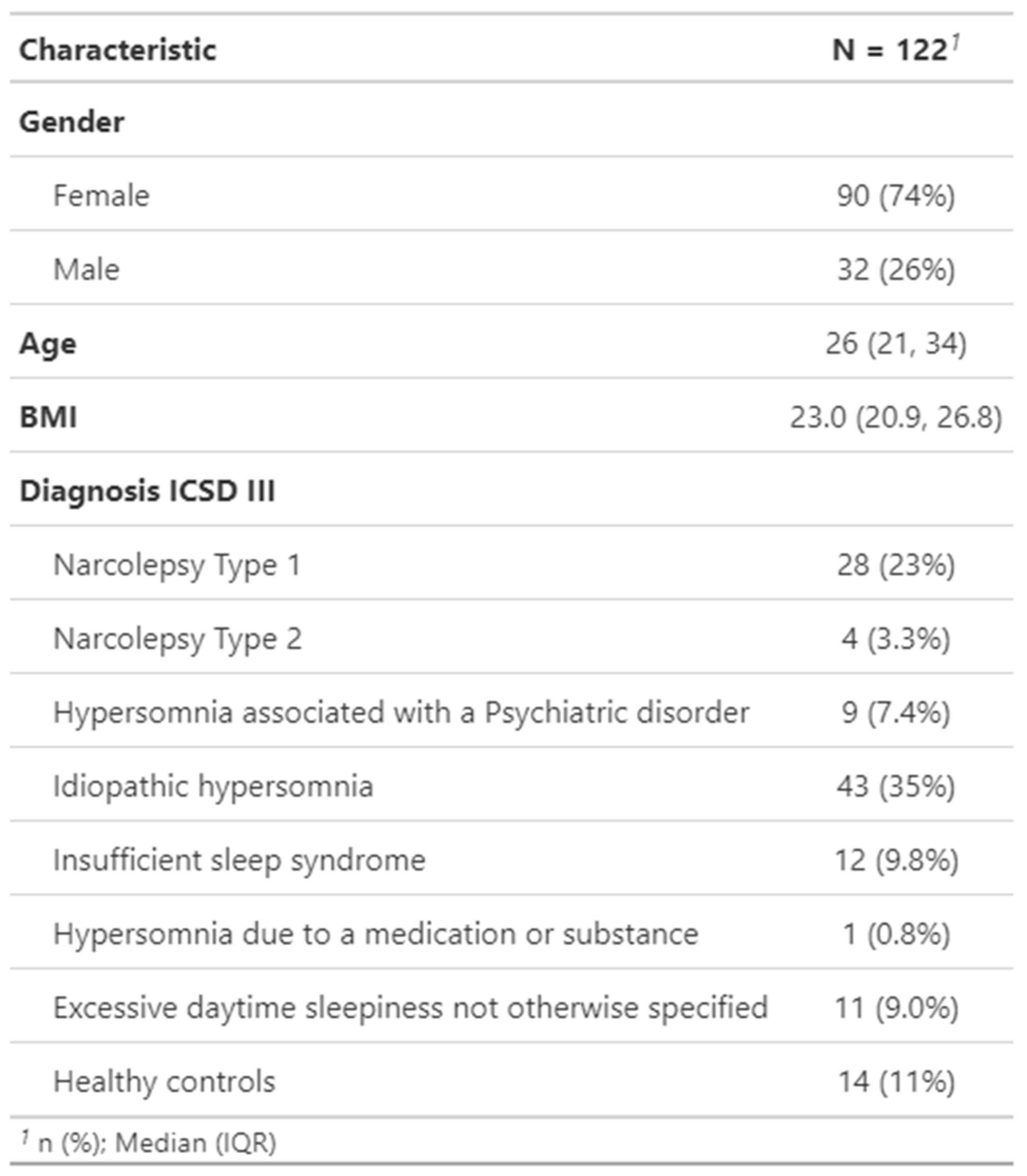
3.1. Characteristics of the Study Population
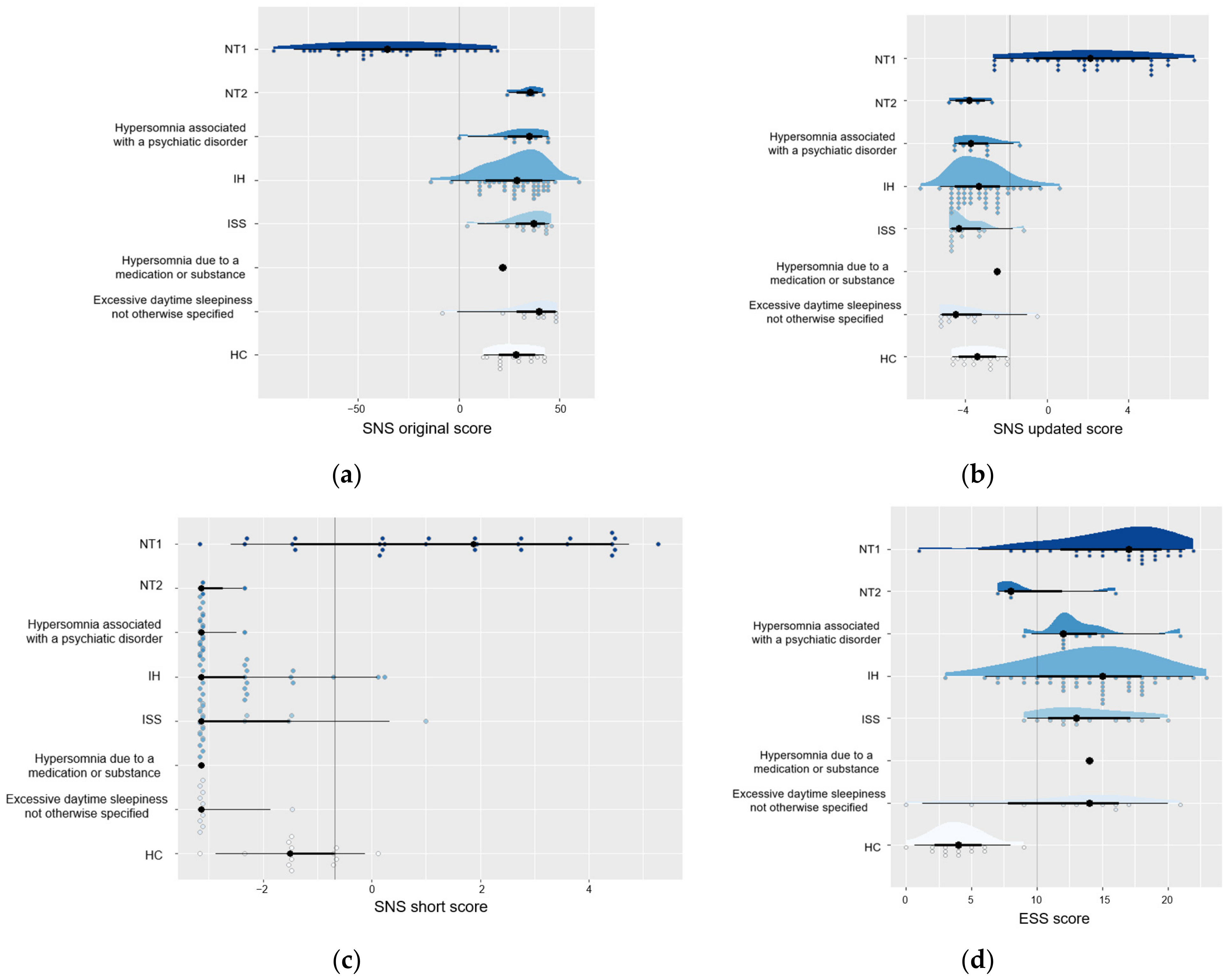
3.2. Diagnostic Accuracy of the SNS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sturzenegger, C.; Bassetti, C.L. The clinical spectrum of narcolepsy with cataplexy: A reappraisal. J. Sleep Res. 2004, 13, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Barateau, L.; Pizza, F.; Chenini, S.; Peter-Derex, L.; Dauvilliers, Y. Narcolepsies, update in 2023. Rev. Neurol. 2023, 179, 727–740. [Google Scholar] [CrossRef] [PubMed]
- Parkes, J.D.; Chen, S.Y.; Clift, S.J.; Dahlitz, M.J.; Dunn, G. The clinical diagnosis of the narcoleptic syndrome. J. Sleep Res. 1998, 7, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Rogers, A.E.; Meehan, J.; Guilleminault, C.; Grumet, F.C.; Mignot, E. HLA DR15 (DR2) and DQB1*0602 typing studies in 188 narcoleptic patients with cataplexy. Neurology 1997, 48, 1550–1556. [Google Scholar] [CrossRef] [PubMed]
- Landtblom, A.M.; Engstrom, M. The sleepy teenager—Diagnostic challenges. Front. Neurol. 2014, 5, 140. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Dauvilliers, Y.; Plazzi, G.; Mayer, G.; Lammers, G.J.; Santamaria, J.; Partinen, M.; Overeem, S.; Del Rio Villegas, R.; Sonka, K.; et al. Idling for Decades: A European Study on Risk Factors Associated with the Delay before a Narcolepsy Diagnosis. Nat. Sci. Sleep 2022, 14, 1031–1047. [Google Scholar] [CrossRef]
- Rocca, F.L.; Pizza, F.; Ricci, E.; Plazzi, G. Narcolepsy during Childhood: An Update. Neuropediatrics 2015, 46, 181–198. [Google Scholar] [CrossRef]
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2023. [Google Scholar]
- Vogel, G. Studies in psychophysiology of dreams. III. The dream of narcolepsy. Arch. Gen. Psychiatry 1960, 3, 421–428. [Google Scholar] [CrossRef]
- Dauvilliers, Y.; Arnulf, I.; Mignot, E. Narcolepsy with cataplexy. Lancet 2007, 369, 499–511. [Google Scholar] [CrossRef]
- Nishino, S.; Ripley, B.; Overeem, S.; Lammers, G.J.; Mignot, E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet 2000, 355, 39–40. [Google Scholar] [CrossRef]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. Sensitivity and specificity of the multiple sleep latency test (MSLT), the maintenance of wakefulness test and the Epworth sleepiness scale: Failure of the MSLT as a gold standard. J. Sleep Res. 2000, 9, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Hublin, C.; Kaprio, J.; Partinen, M.; Koskenvuo, M.; Heikkila, K. The Ullanlinna Narcolepsy Scale: Validation of a measure of symptoms in the narcoleptic syndrome. J. Sleep. Res. 1994, 3, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Sturzenegger, C.; Baumann, C.R.; Lammers, G.J.; Kallweit, U.; van der Zande, W.L.; Bassetti, C.L. Swiss Narcolepsy Scale: A simple screening tool for hypocretin-deficient narcolepsy with cataplexy. Clin. Transl. Neurol. 2018, 2, 2514183X18794175. [Google Scholar]
- Bargiotas, P.; Dietmann, A.; Haynes, A.G.; Kallweit, U.; Calle, M.G.; Schmidt, M.; Mathis, J.; Bassetti, C.L. The Swiss Narcolepsy Scale (SNS) and its short form (sSNS) for the discrimination of narcolepsy in patients with hypersomnolence: A cohort study based on the Bern Sleep-Wake Database. J. Neurol. 2019, 266, 2137–2143. [Google Scholar] [CrossRef] [PubMed]
- Demir, A.B.; Bargiotas, P.; Berktaş, D.T.; İsmailoğulları, S.; Akyıldız, U.O.; Karadeniz, D.; Şenel, G.B.; Bassetti, C.L.A. A Turkish Validity and Reliability Study of the Swiss Narcolepsy Scale. Clin. Transl. Neurosci. 2023, 7, 16. [Google Scholar] [CrossRef]
- Tanioka, K.; Hirasawa, T.; Yanagihara, M.; Takeuchi, N.; Nakayama, H.; Usui, A.; Inoue, Y. Reliability and validity of the Japanese version of the Ullanlinna Narcolepsy Scale and Swiss Narcolepsy Scale for screening Japanese individuals with narcolepsy type 1. Sleep Med. 2023, 109, 245–251. [Google Scholar] [CrossRef]
- Dietmann, A.; Wenz, E.; van der Meer, J.; Ringli, M.; Warncke, J.D.; Edwards, E.; Schmidt, M.H.; Bernasconi, C.A.; Nirkko, A.; Strub, M.; et al. The Swiss Primary Hypersomnolence and Narcolepsy Cohort study (SPHYNCS): Study protocol for a prospective, multicentre cohort observational study. J. Sleep Res. 2021, 30, e13296. [Google Scholar] [CrossRef]
- Bloch, K.E.; Schoch, O.D.; Zhang, J.N.; Russi, E.W. German version of the Epworth Sleepiness Scale. Respiration 1999, 66, 440–447. [Google Scholar] [CrossRef]
- Vignatelli, L.; Plazzi, G.; Barbato, A.; Ferini-Strambi, L.; Manni, R.; Pompei, F.; D’Alessandro, R.; GINSEN. Italian version of the Epworth sleepiness scale: External validity. Neurol. Sci. 2003, 23, 295–300. [Google Scholar] [CrossRef]
- Kaminska, M.; Jobin, V.; Mayer, P.; Amyot, R.; Perraton-Brillon, M.; Bellemare, F. The Epworth Sleepiness Scale: Self-Administration versus Administration by the Physician, and Validation of a French Version. Can. Respir. J. 2010, 17, e27–e34. [Google Scholar] [CrossRef] [PubMed]
- Mignot, E.; Lammers, G.J.; Ripley, B.; Okun, M.; Nevsimalova, S.; Overeem, S.; Vankova, J.; Black, J.; Harsh, J.; Bassetti, C.; et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch. Neurol. 2002, 59, 1553–1562. [Google Scholar] [CrossRef] [PubMed]
- Partinen, M.; Kornum, B.R.; Plazzi, G.; Jennum, P.; Julkunen, I.; Vaarala, O. Narcolepsy as an autoimmune disease: The role of H1N1 infection and vaccination. Lancet Neurol. 2014, 13, 600–613. [Google Scholar] [CrossRef] [PubMed]
- Roya, Y.; Farzaneh, B.; Mostafa, A.D.; Mahsa, S.; Babak, Z. Narcolepsy following COVID-19: A case report and review of potential mechanisms. Clin. Case Rep. 2023, 11, e7370. [Google Scholar] [CrossRef]
- Bostrom, I.; Lindberger, O.; Partinen, M.; Landtblom, A.-M. Vaccination against swine flu caused narcolepsy in several European countries. Health Risk Anal. 2020, 3, 182–187. [Google Scholar] [CrossRef]
- Thorpy, M.; Morse, A.M. Reducing the Clinical and Socioeconomic Burden of Narcolepsy by Earlier Diagnosis and Effective Treatment. Sleep Med. Clin. 2017, 12, 61–71. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| (a) Questions |
|---|
| Q1 How often are you unable to fall asleep? |
| [1] never, [2] rarely (less than once a month), [3] sometimes (1–3 times a month), |
| [4] often (1–2 times a week), and [5] almost always |
| Q2 How often do you feel bad or not well rested in the morning? |
| [1] never, [2] rarely (less than once a month), [3] sometimes (1–3 times a month), |
| [4] often (1–2 times a week), and [5] almost always |
| Q3 How often do you take a nap during the day? |
| [1] never, [2] I would like, but cannot, [3] 1–2 times a week, |
| [4] 3–5 times a week, and [5] almost daily |
| Q4 How often have you experienced weak knees/buckling of the knees during emotions like laughing, happiness, or anger? |
| [1] never, [2] rarely (less than once a month), [3] sometimes (1–3 times a month), |
| [4] often (1–2 times a week), and [5] almost always |
| Q5 How often have you experienced sagging of the jaw during emotions like laughing, happiness, or anger? |
| [1] never, [2] rarely (less than once a month), [3] sometimes (1–3 times a month), |
| [4] often (1–2 times a week), and [5] almost always |
| (b) Formulas for calculation of scores and cut-off values for predicting NT1: |
| SNS score: 6 × Q1 + 9 × Q2 − 5 × Q3 − 11 × Q4 − 13 × Q5 + 20 < 0 |
| Updated SNS score: Q1 × (−0.47) + Q2 × (−0.83) + Q3 × 0.58 + Q4 × 0.56 + Q5 × 1.45 − 2.75 ≥ −1.83 |
| sSNS: Q2 × −0.82 + Q5 × 1.70 − 0.74 ≥ −0.68 |
| Study Population | Epworth Sleepiness Scale | Swiss Narcolepsy Scale (Original Score) | |
|---|---|---|---|
| Sturzenegger & Bassetti, 2004 [1] |
| Significantly higher scores in narcolepsy with cataplexy (17 ± 5) than non-narcoleptics (15 ± 4, p = 0.003) | Sensitivity: 96% Specificity: 98% for detecting narcolepsy with cataplexy against EDS of another origin |
| Sturzenegger et al., 2018 [15] |
| Sensitivity: 91% Specificity: 54% for detecting narcolepsy with cataplexy against EDS of another origin | Sensitivity: 89% and 93% Specificity: 88% and 88% for detecting narcolepsy with cataplexy against EDS of another origin |
| Bargiotas et al., 2019 [16] |
| Sensitivity: 56% Specificity: 68% for detecting NT1 against EDS of another origin | Sensitivity 86% Specificity: 88% for detecting NT1 against EDS of another origin |
| Demir et al., 2023 [17] |
| Higher scores in patients with narcolepsy (NT1 (18.2 ± 3.5) and NT2 (15.5 ± 5.6)) against IH (p = 0.033) | Sensitivity: 90.5% Specificity: 100% for detecting NT1 against EDS of another origin |
| Tanioka et al., 2023 [18] |
| Higher scores in patients with narcolepsy (NT1 (19.2 ± 3.6) and NT2 (19.4 ± 3.5)) against EDS of another origin (p < 0.05) | Sensitivity: 86% Specificity: 86% for detecting NT1 against EDS of another origin |
| Zub et al., 2023 current study |
| Sensitivity: 85% Specificity: 22% for detecting NT1 against patients with other CDH | Sensitivity: 86% Specificity: 96% for detecting NT1 against patients with other CDH |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zub, K.; Warncke, J.D.; van der Meer, J.; Wenz, E.S.; Fregolente, L.G.; Bargiotas, P.; Benbir Şenel, G.; Sturzenegger, C.; Lammers, G.J.; Kallweit, U.; et al. SPHYNCS: The Use of the Swiss Narcolepsy Scale in a New Cohort of Patients with Narcolepsy and Its Borderland and Review of the Literature. Clin. Transl. Neurosci. 2024, 8, 2. https://doi.org/10.3390/ctn8010002
Zub K, Warncke JD, van der Meer J, Wenz ES, Fregolente LG, Bargiotas P, Benbir Şenel G, Sturzenegger C, Lammers GJ, Kallweit U, et al. SPHYNCS: The Use of the Swiss Narcolepsy Scale in a New Cohort of Patients with Narcolepsy and Its Borderland and Review of the Literature. Clinical and Translational Neuroscience. 2024; 8(1):2. https://doi.org/10.3390/ctn8010002
Chicago/Turabian StyleZub, Kseniia, Jan D. Warncke, Julia van der Meer, Elena S. Wenz, Livia G. Fregolente, Panagiotis Bargiotas, Gülçin Benbir Şenel, Christian Sturzenegger, Gert Jan Lammers, Ulf Kallweit, and et al. 2024. "SPHYNCS: The Use of the Swiss Narcolepsy Scale in a New Cohort of Patients with Narcolepsy and Its Borderland and Review of the Literature" Clinical and Translational Neuroscience 8, no. 1: 2. https://doi.org/10.3390/ctn8010002