In Situ Diagnosis of Scabies Using a Handheld Digital Microscope in Resource-Poor Settings—A Proof-of-Principle Study in the Amazon Lowland of Colombia

Abstract
:1. Introduction
2. Material and Methods
2.1. Study Area and Population
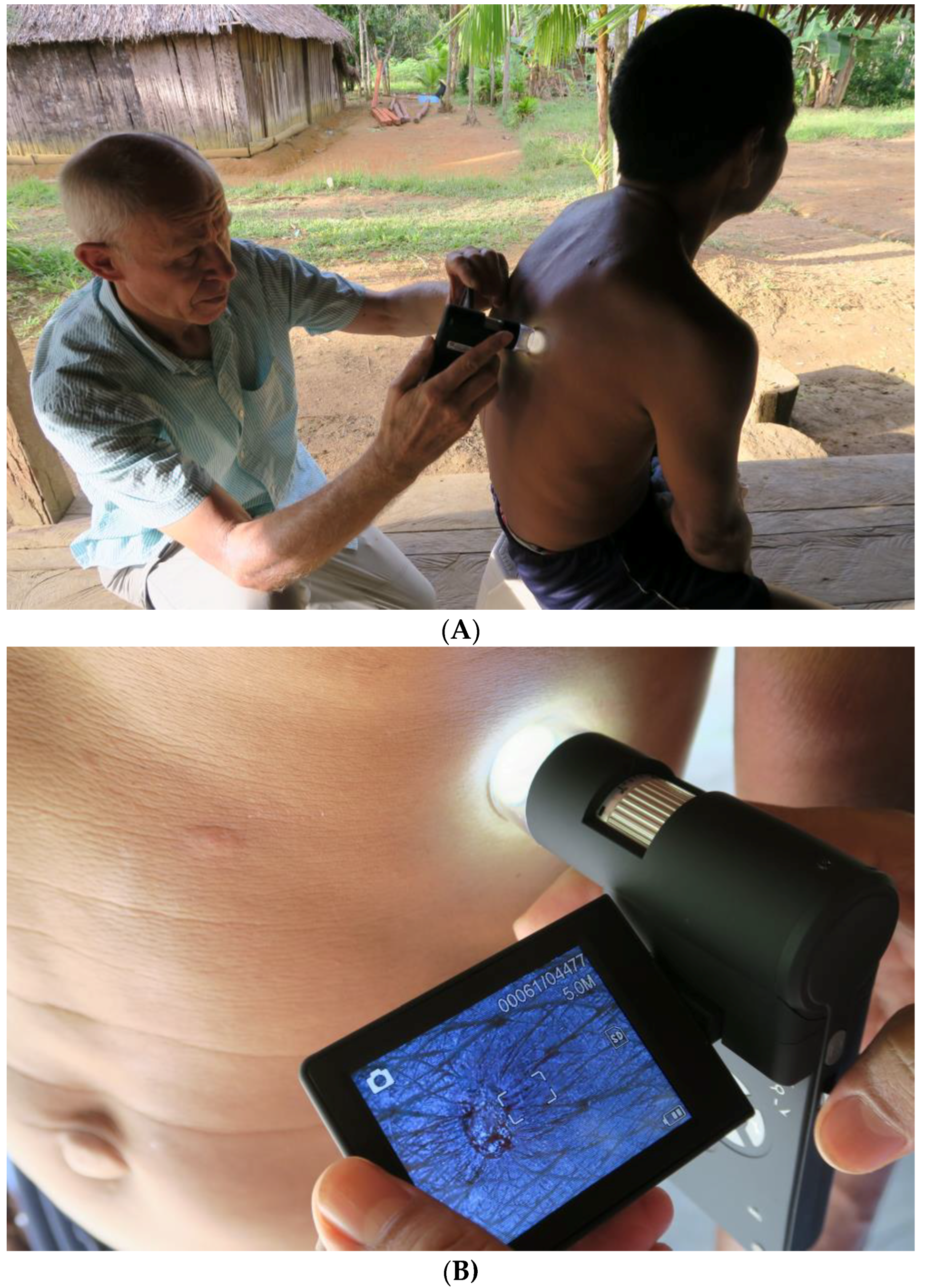
2.2. Study Design and Data Collection
2.3. Diagnosis
2.4. Treatment
3. Results
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Considerations
References
- Engelman, D.; Kiang, K.; Chosidow, O.; McCarthy, J.; Fuller, C.; Lammie, P.; Hay, R.; Steer, A. Toward the global control of human scabies: Introducing the international alliance for the control of scabies. PLoS Negl. Trop. Dis. 2013, 7, e2167. [Google Scholar] [CrossRef] [PubMed]
- Feldmeier, H.; Heukelbach, J. Epidermal parasitic skin diseases: A neglected category of poverty-associated plagues. Bull. World Health Organ. 2009, 87, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Heukelbach, J.; Feldmeier, H. Scabies. Lancet 2006, 367, 1767–1774. [Google Scholar] [CrossRef]
- Berrios, X.; Lagomarsino, E.; Solar, E.; Sandoval, G.; Guzman, B.; Riedel, I. Post-streptococcal acute glomerulonephritis in chile—20 years of experience. Pediatr. Nephrol. 2004, 19, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Hay, R.J.; Steer, A.C.; Engelman, D.; Walton, S. Scabies in the developing world—Its prevalence, complications, and management. Clin. Microbiol. Infect. 2012, 18, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Worth, C.; Heukelbach, J.; Fengler, G.; Walter, B.; Liesenfeld, O.; Feldmeier, H. Impaired quality of life in adults and children with scabies from an impoverished community in Brazil. Int. J. Dermatol. 2012, 51, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Feldmeier, H.; Jackson, A.; Ariza, L.; Calheiros, C.M.L.; de Lima Soares, V.; Hengge, U.R.; Heukelbach, J. The epidemiology of scabies in an impoverished community in rural brazil: Presence and severity of disease are associated with poor living conditions and illiteracy. J. Am. Acad. Dermatol. 2009, 60, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Carapetis, J.R.; Connors, C.; Yarmirr, D.; Krause, V.; Currie, B.J. Success of a scabies control program in an australian aboriginal community. Pediatr. Infect. Dis. J. 1997, 16, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Heukelbach, J.; Wilcke, T.; Winter, B.; Feldmeier, H. Epidemioloy and morbidity of scabies and pediculosis capitis in resource-poor communities in Brazil. Br. J. Dermatol. 2007, 153, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Jackson, A.; Heukelbach, J.; Feldmeier, H. Transmission of scabies in an endemic area. Br. J. Infect. Dis. 2007, 11, 307–308. [Google Scholar]
- Currie, B.J.; Connors, C.M.; Krause, V.L. Scabies programs in aboriginal communities. Med. J. Aust. 1994, 161, 636–637. [Google Scholar] [PubMed]
- Feldmeier, H.; Wilcke, T. Scabies in childhood. In Recent Advances in Pediatrics; David, T.J., Ed.; The Royal Society of Medicine Press: London, UK, 2007; pp. 25–38. [Google Scholar]
- Jackson, A.; Heukelbach, J.; Ferreira da Silva Filho, A.; Barros Campelo Junior, E.; Feldmeier, H. Clinical features and associated morbidity of scabies in a rural community in alagoas, Brazil. Trop. Med. Int. Health 2007, 12, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Cestari, T.F.; Martignago, B.F. Scabies, pediculosis, bedbugs, and stinkbugs: Uncommon presentations. Clin. Dermatol. 2005, 23, 545–554. [Google Scholar] [CrossRef] [PubMed]
- Schmeller, W.; Bendick, C.; Stingl, P. Dermatosen aus drei Kontinenten—Bildatlas der Vergleichenden Dermatologie, 1st ed.; Schattauer: Stuttgart, Germany, 2005; p. 238. [Google Scholar]
- Feldmeier, H. Diagnosis of parasitic skin diseases. In Evidence Based Dermatology, 2nd ed.; Maibach, H., Farzam, G., Eds.; PMPH-USA: Raleigh, NC, USA, 2010; pp. 73–86. [Google Scholar]
- Walton, S.F.; Currie, B.J. Problems in diagnosing scabies, a global disease in human and animal populations. Clin. Microbiol. Rev. 2007, 20, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Mahe, A.; Faye, O.; N’Diaye, H.T.; Ly, F.; Konare, H.; Keita, S.; Traore, A.K.; Hay, R. Definition of an algorithm for the management of common skin diseases at primary health care level in sub-saharan africa. Trans. R. Soc. Trop. Med. Hyg. 2005, 99, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Thielecke, M.; Nordin, P.; Ngomi, N.; Feldmeier, H. Treatment of tungiasis with dimeticone: A proof-of-principle study in rural kenya. PLoS Negl. Trop. Dis. 2014, 8, e3058. [Google Scholar] [CrossRef] [PubMed]
- Aguado Taberné, C.; del Pozo Guzmán, R.; García Aranda, J.M. Tratamiento de las infestaciones cutáneas. In Manual de Terapéutica en Atención Primaria; Central Publications Service of the Basque Government: Vitoria-Gasteiz, Spain, 2006. [Google Scholar]
- Von Humboldt, A. Südamerikanische Reise; Ullstein GmbH: Berlin, Germany, 1981. [Google Scholar]
- Bazin, E. Leçons Théoriques et Cliniques sur les Affections Génériques de la Peau; Adrien Delahaye: Pairs, France, 1862; p. 454. [Google Scholar]
- Dorado, J.G.; Fraile, P.A. Sarna, pediculosis y picaduras de insectos. Pediatríaintegral 2012, 16, 301–320. [Google Scholar]
- Walter, B.; Heukelbach, J.; Fengler, G.; Worth, C.; Hengge, U.; Feldmeier, H. Comparison of dermoscopy, skin scraping, and the adhesive tape test for the diagnosis of scabies in a resource-poor setting. Arch. Dermatol. 2011, 147, 468–473. [Google Scholar] [CrossRef] [PubMed]
- Palicka, P.; Mali, L.; Samsinak, K.; Zitek, K.; Vobrazkov, E. Laboratory diagnosis of scabies. J. Hyg. Epidemiol. Microbiol. Immunol. 1980, 24, 63–70. [Google Scholar] [PubMed]
- Woodley, D.; Saurat, J.H. The burrow ink test and the scabies mite. J. Am. Acad. Dermatol. 1981, 6, 715–722. [Google Scholar] [CrossRef]
- Argenziano, G.; Fabbrocini, G.; Delfino, M. Epiluminescence microscopy: A new approach to in vivo detection of sarcoptes scabiei. Arch. Dermatol. 1997, 133, 751–753. [Google Scholar] [CrossRef] [PubMed]
- Lacarrubba, F.; Musumeci, M.L.; Caltabiano, R.; Impallomeni, R.; West, D.P.; Micali, G. High-magnification videodermatoscopy: A new noninvasive diagnostic tool for scabies in children. Pediatr. Dermatol. 2001, 18, 439–441. [Google Scholar] [CrossRef] [PubMed]
- Longo, C.; Bassoli, S.; Monari, P.; Seidenari, S.; Pellacani, G. Reflectance-mode confocal microscopy for the in vivo detection of sarcoptes scabiei. Arch. Dermatol. 2005, 141, 1336–1337. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, A.; Dehen, L.; Bourrat, E.; Lacroix, C.; Benderdouche, M.; Dubertret, L.; Morel, P.; Feuilhade de Chauvin, M.; Petit, A. Accuracy of standard dermoscopy for diagnosing scabies. J. Am. Acad. Dermatol. 2007, 56, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Yoshizumi, J.; Harada, T. “Wake sign”: An important clue for the diagnosis of scabies. Clin. Exp. Dermatol. 2008, 34, 711–714. [Google Scholar] [CrossRef] [PubMed]
- S1-Leitlinie zu Diagnostik und Therapie der Skabies. Available online: http://www.awmf.org/leitlinien/detail/ll/013-052.html (accessed on 31 January 2006).
- Bhutto, A.M.; Honda, M.; Kubo, Y.; Nonaka, S.; Yoshida, H. Introduction of a fluorescense-microscopic technique for the detection of eggs, egg shells, and mites in scabies. J. Dermatol. 1993, 20, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Uenotsuchi, T.; Moroi, Y.; Urabe, K.; Tsuji, G.; Takahara, M.; Furue, M. The scybala (fecal pellets) of Sacroptes scabiei var. Hominis are obviously stained with chlorazol black E. J. Dermatol. 2004, 31, 511–512. [Google Scholar] [PubMed]
- Neynaber, S.; Wolff, H. Diagnosis of scabies with dermoscopy. Can. Med. Assoc. J. 2008, 178, 1540–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prins, C.; Stucki, L.; French, L.; Saurat, J.H.; Braun, R.P. Dermoscopy for the in vivo detection of sarcoptes scabiei. Dermatology 2004, 208, 241–243. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Community | Number of Participants | Age in Years Median (Range) | Males/Females | Scabies Diagnosed a (%) |
|---|---|---|---|---|
| Cariyá | 11 | 29 (3–88) | 4/7 | 6 (54.5) |
| Santa Catalina | 51 | 19 (2–71) | 28/23 | 8 (15.7) |
| Barrio 12 de Octubre | 49 | 12 (3 months–77) | 21/28 | 10 (20.4) |
| Total | 111 | 15 (3 months–88) | 53/58 | 24 (21.6) |
| Characteristics | Frequency (n/%) |
|---|---|
| Number of topographic areas affected | |
| 1–5 | 10/(41.6%) |
| 6–10 | 13/(54.1%) |
| >10 | 1/(4.31%) |
| Appearance of lesions (weeks ago) | |
| <4 weeks | 6/(25.0%) |
| 4–12 weeks | 14/(58.3%) |
| >12 weeks | 4/(16.6%) |
| Type of lesion a | |
| Papule | 23/(95.8%) |
| Vesicle | 16/(66.6%) |
| Nodule | 2/(8.3%) |
| Crusted lesion b | 15/(62.5%) |
| Excoriation/desquamation | 19/(79.1%) |
| Bacterial superinfection c | 15/(62.5%) |
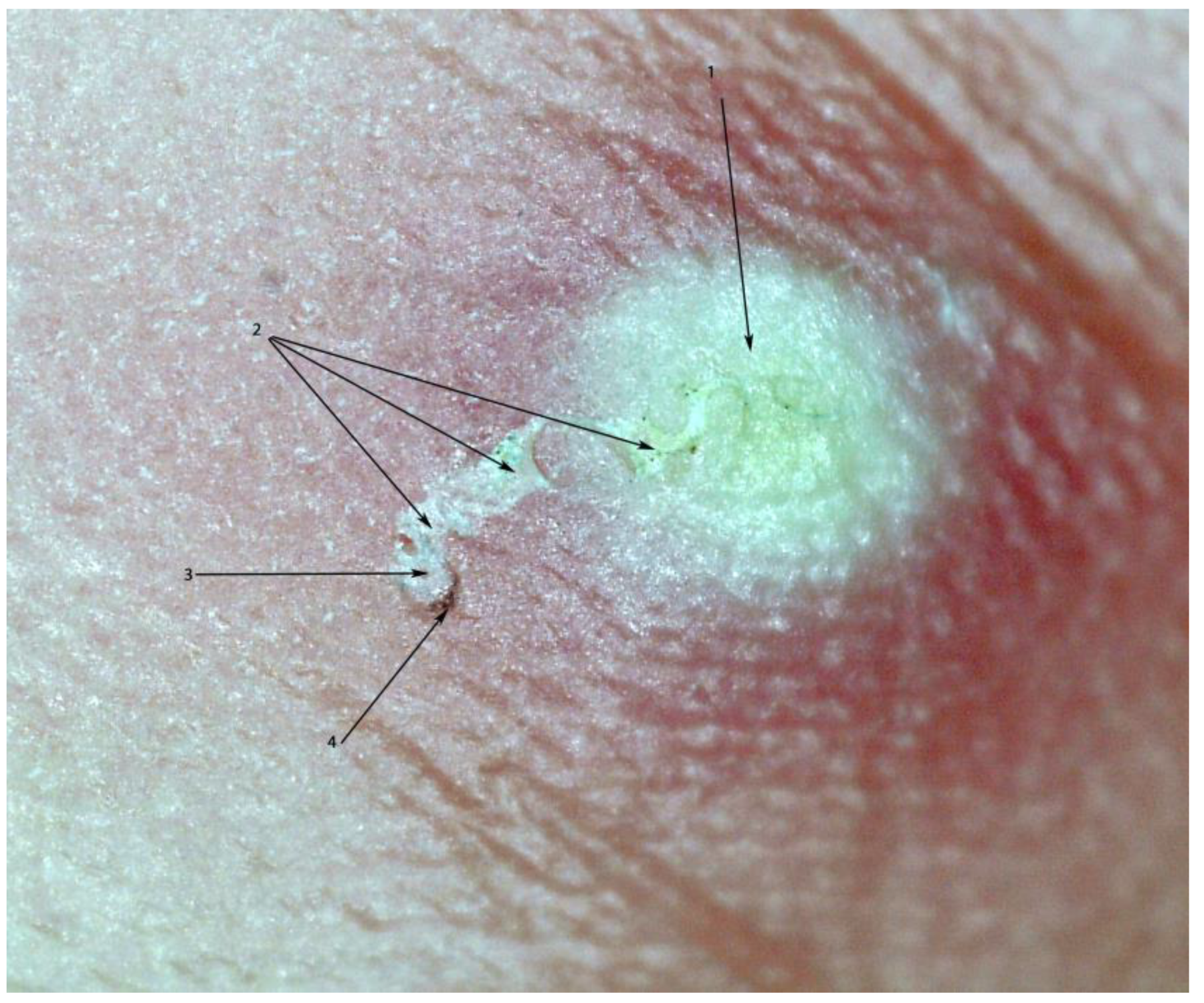
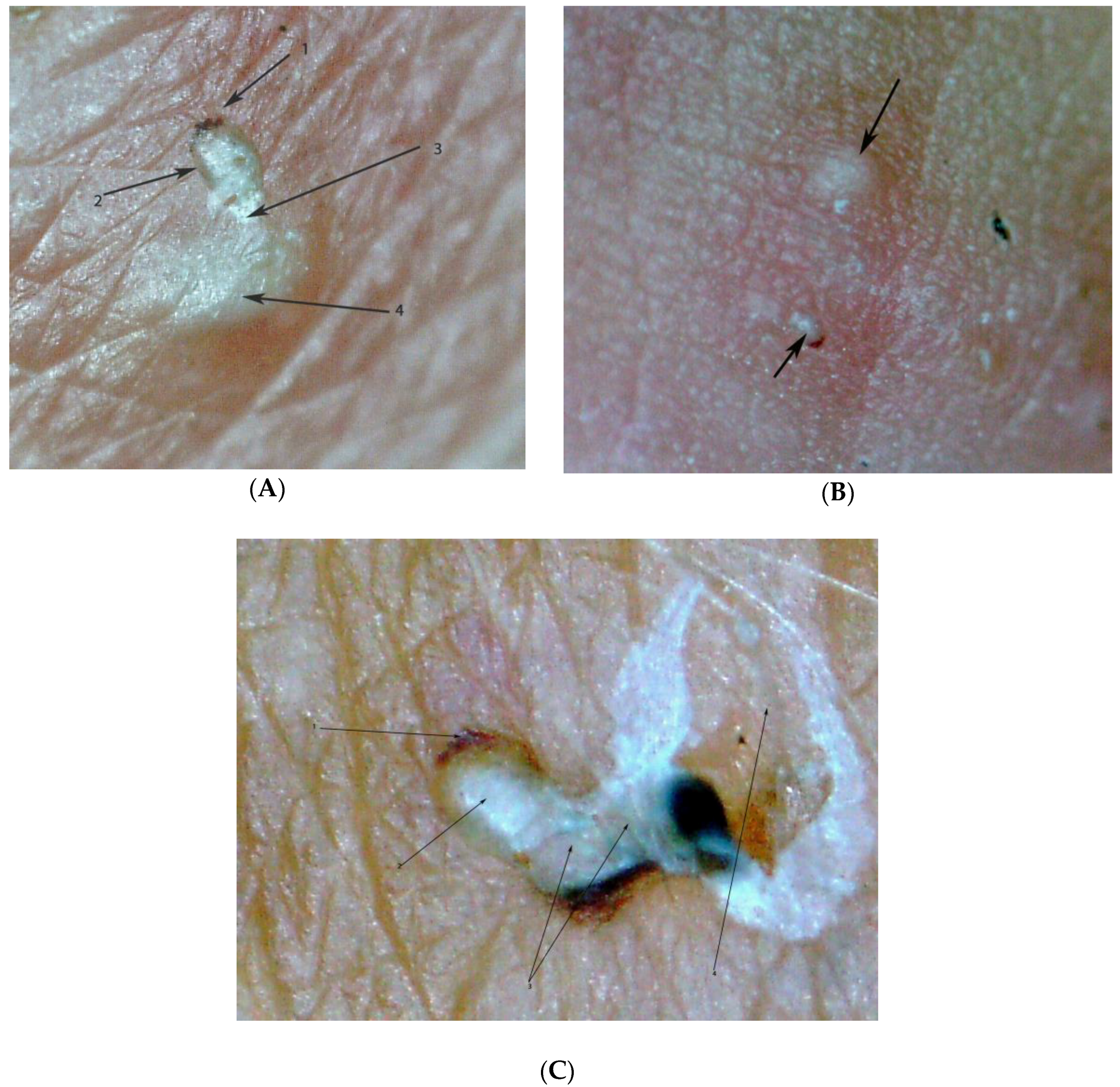
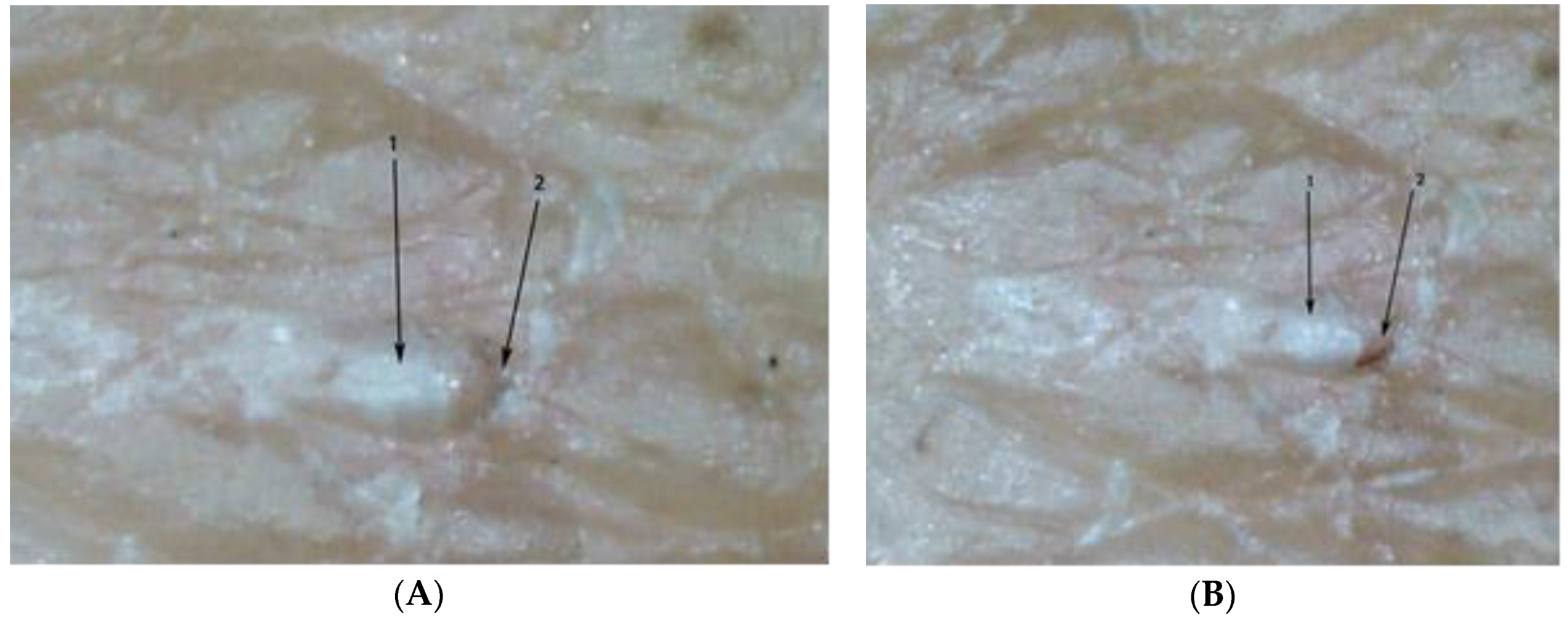
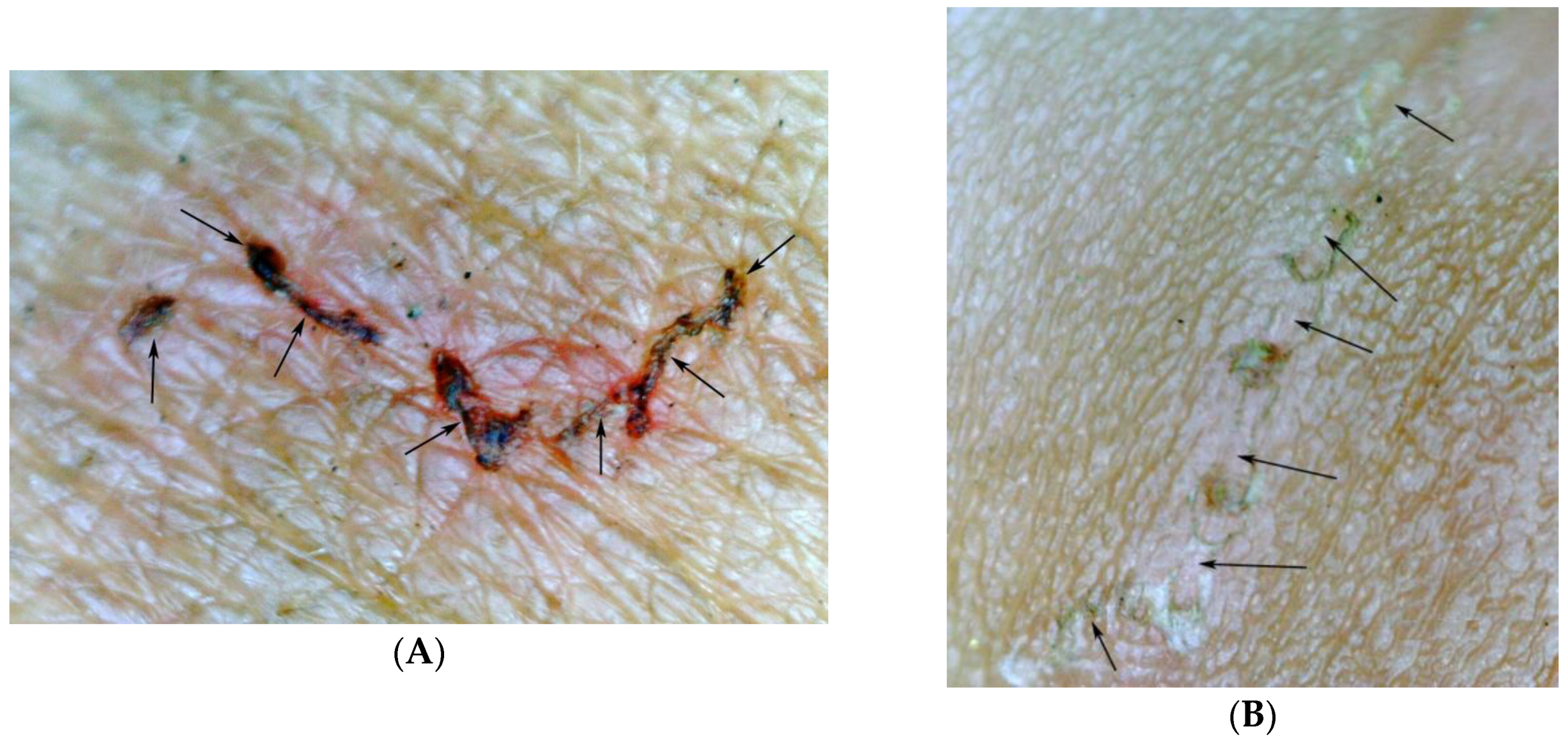
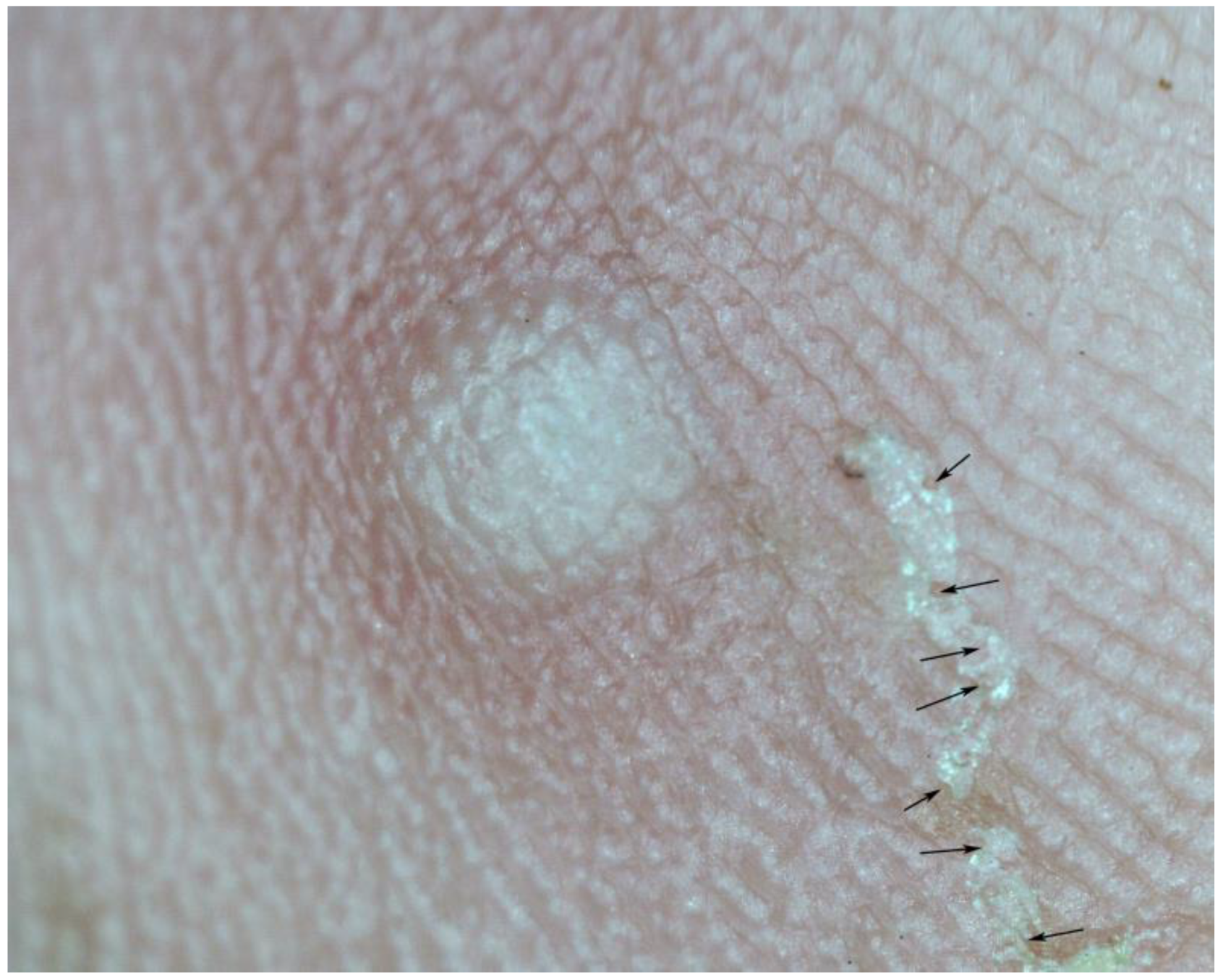
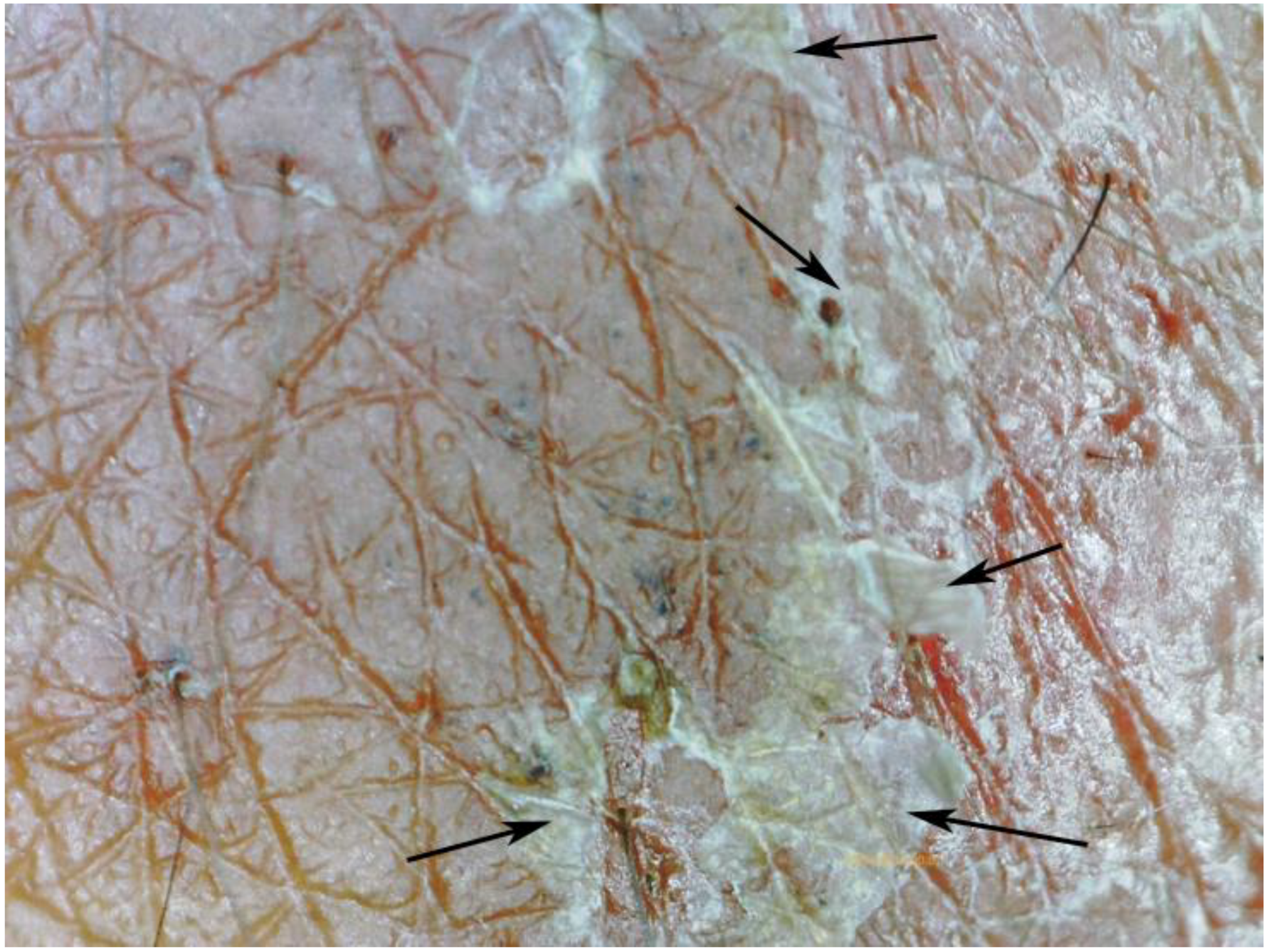
| Characteristics b | Frequency (n/%) |
|---|---|
| Tunnel without mite | 8/(33.7%) |
| Tunnel with mite | 24/(100%) |
| Tunnel with mite present in the acarine eminence | 23/(95.8%) |
| Tunnel with mite in the middle of the tunnel | 1 |
| Tunnel with faecal pellets | 8/(33.3%) |
| Partially or totally obliterated tunnel | 16/(66.7%) |
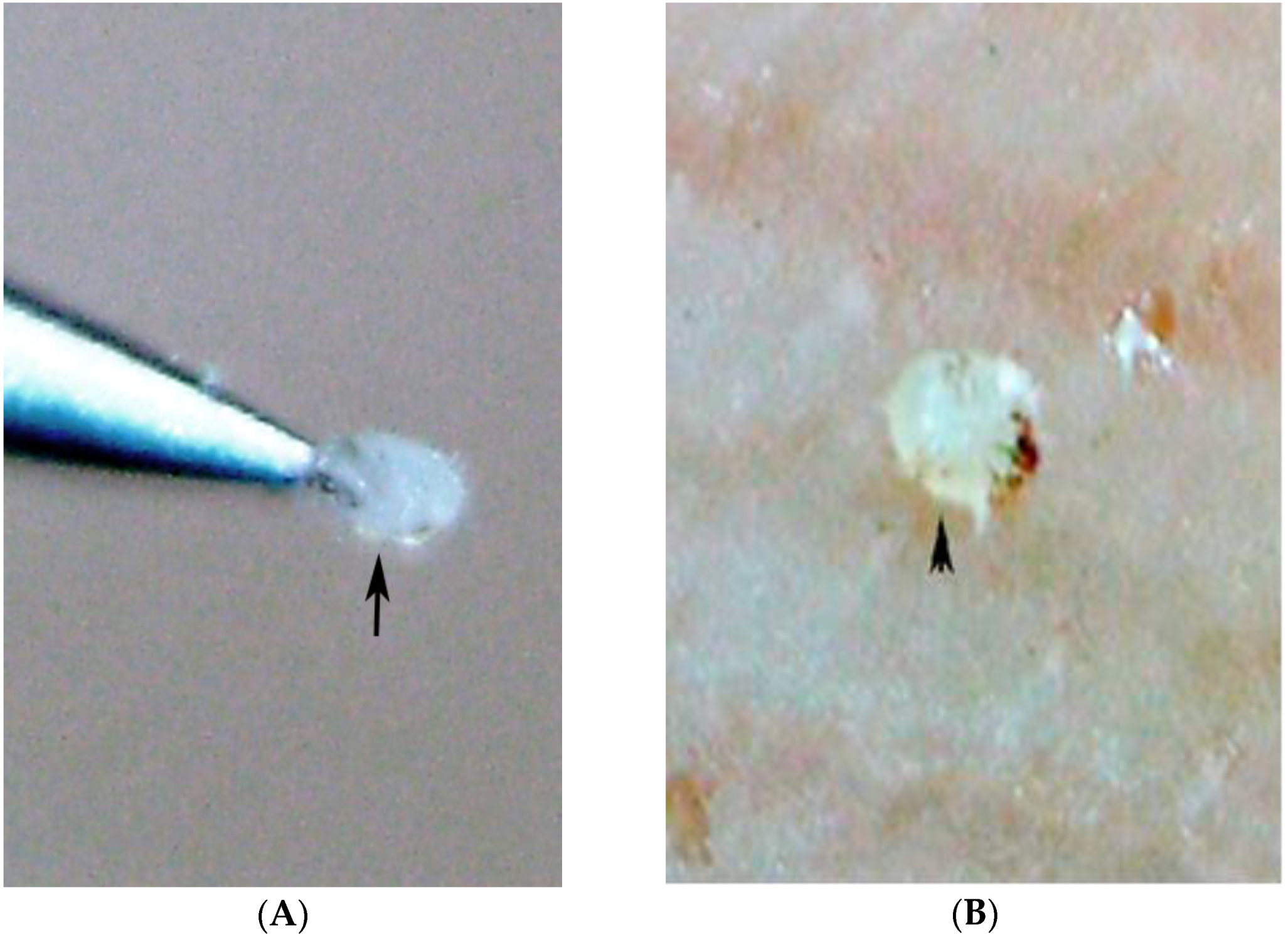
| Extraction of mite by experienced mother | 24/(100%) c |
| Pearly vesicle surrounded by erythema | 17/(70.8%) |
| Circumscribed hyperpigmentation | 22/(91.6%) |
| Micro-haemorrhagia | 4/(16.6%) |
| Excoriation/desquamation of the corneal layer | 19/(79.1%) d |
| Nodule containing mite | 1/(4.1%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, H.; Trujillo-Trujillo, J.; Feldmeier, H. In Situ Diagnosis of Scabies Using a Handheld Digital Microscope in Resource-Poor Settings—A Proof-of-Principle Study in the Amazon Lowland of Colombia. Trop. Med. Infect. Dis. 2018, 3, 116. https://doi.org/10.3390/tropicalmed3040116
Miller H, Trujillo-Trujillo J, Feldmeier H. In Situ Diagnosis of Scabies Using a Handheld Digital Microscope in Resource-Poor Settings—A Proof-of-Principle Study in the Amazon Lowland of Colombia. Tropical Medicine and Infectious Disease. 2018; 3(4):116. https://doi.org/10.3390/tropicalmed3040116
Chicago/Turabian StyleMiller, Hollman, Julian Trujillo-Trujillo, and Hermann Feldmeier. 2018. "In Situ Diagnosis of Scabies Using a Handheld Digital Microscope in Resource-Poor Settings—A Proof-of-Principle Study in the Amazon Lowland of Colombia" Tropical Medicine and Infectious Disease 3, no. 4: 116. https://doi.org/10.3390/tropicalmed3040116