Eccentric Overload Flywheel Training in Older Adults


{kind=link}
{kind=link}
Abstract
1. Introduction
2. Literature Review
2.1. Search Strategy
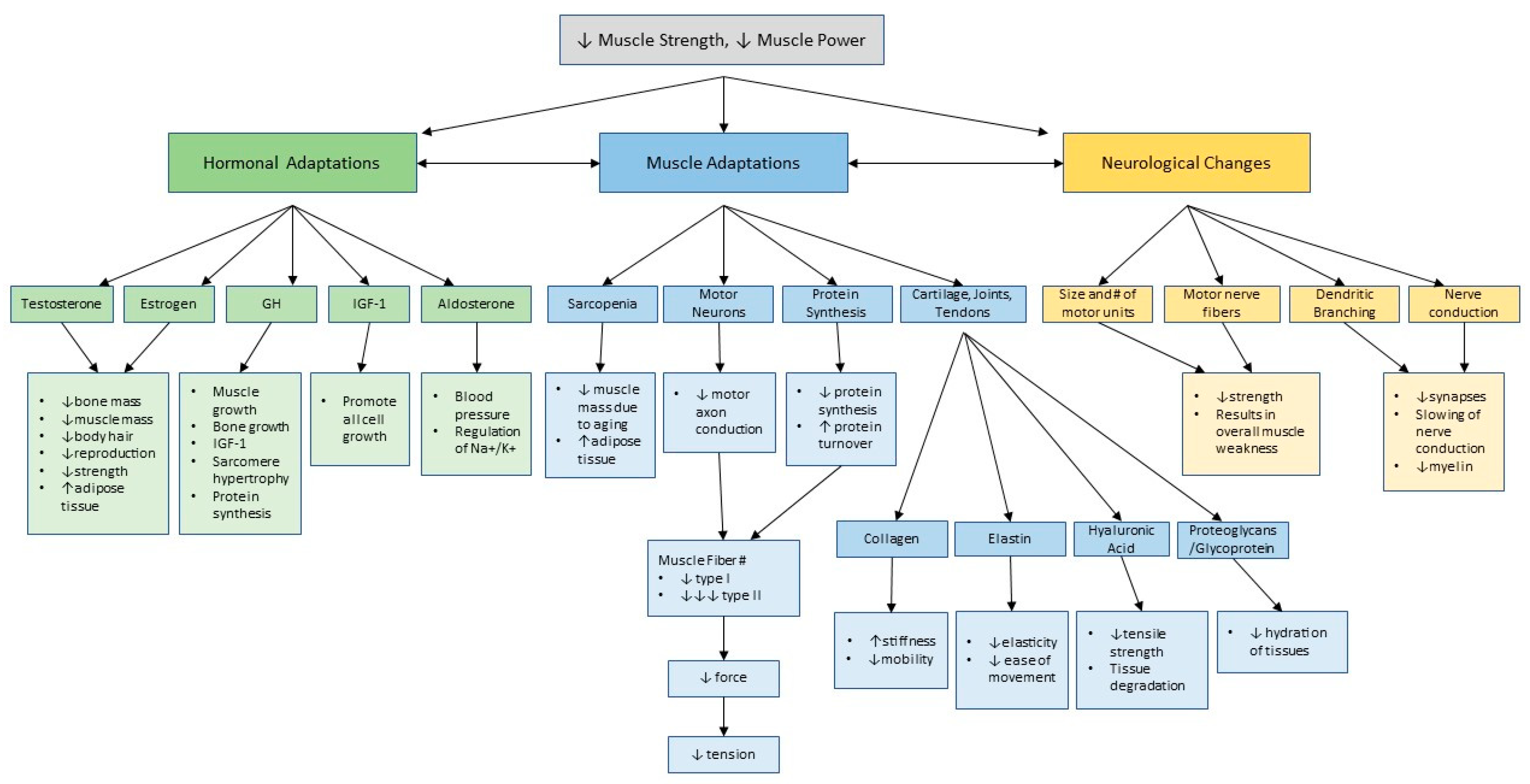
2.2. Physiological Adaptations to Aging: Muscle Strength and Power
2.3. Traditional (TR) Strength and Power Training for Older Adults
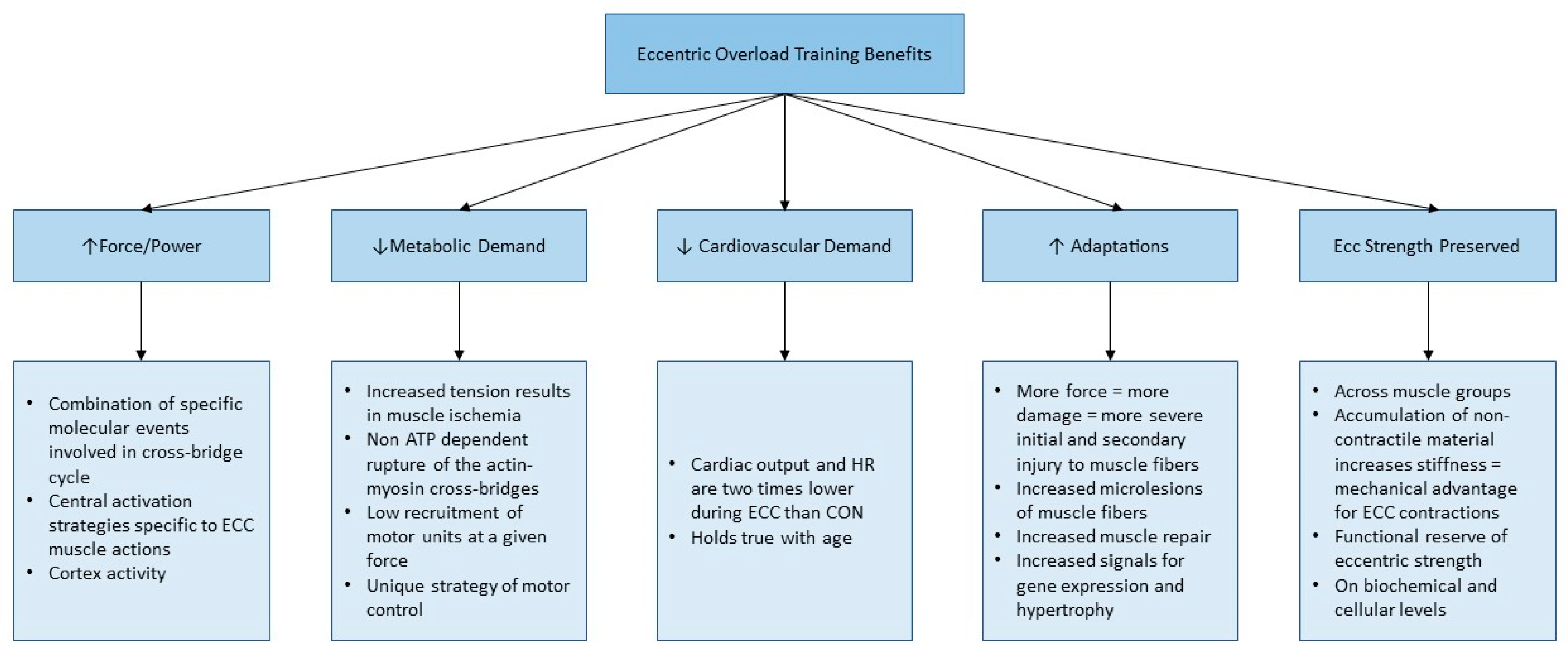
2.4. Eccentric Overload (EO) Training for Older Adults
2.5. Methodology of Flywheel EO Training
2.5.1. Principles of Flywheel Exercise
2.5.2. Commercial Flywheel Devices and Exercise Choice
2.5.3. Flywheel Training Adaptations
2.5.4. Application of Flywheel EO Training to Older Adults
3. Conclusions
Funding
Conflicts of Interest
References
- Algilani, S.; Östlund-Lagerström, L.; Kihlgren, A.; Blomberg, K.; Brummer, R.J.; Schoultz, I. Exploring the concept of optimal functionality in old age. J. Multidiscip. Healthc. 2014, 7, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Hunter, G.R.; McCarthy, J.P.; Bamman, M.M. Effects of resistance training on older adults. Sports Med. 2004, 34, 329–348. [Google Scholar] [CrossRef] [PubMed]
- American College of Sports Medicine; Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Hairi, N.N.; Cumming, R.G.; Naganathan, V.; Handelsman, D.J.; Le Couteur, D.G.; Creasey, H.; Waite, L.M.; Seibel, M.J.; Sambrook, P.N. Loss of muscle strength, mass (sarcopenia), and quality (specific force) and its relationship with functional limitation and physical disability: The Concord Health and Ageing in Men Project. J. Am. Geriatr. Soc. 2010, 58, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Pizzigalli, L.; Filippini, A.; Ahmaidi, S.; Jullien, H.; Rainoldi, A. Prevention of Falling Risk in Elderly People: The Relevance of Muscular Strength and Symmetry of Lower Limbs in Postural Stability. J. Strength Cond. Res. 2011, 25, 567. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.E.; Weir, J.P. ASEP Procedures Recommendation I: Accurate Assessment of Muscular Strength and Power. J. Exerc. Physiol. Online 2001, 4, 1–21. [Google Scholar]
- Bonder, B.R.; Dal Bello-Haas, V. Functional Performance in Older Adults, 4th ed.; F.A. Davis Company: Philadelphia, PA, USA, 2018. [Google Scholar]
- Siff, M.C. Biomechanical Foundations of Strength and Power Training. In Biomechanics in Sport: Performance Enhancement and Injury Prevention; Wiley-Blackwell: Oxford, UK, 2008. [Google Scholar]
- Roig, M.; O’Brien, K.; Kirk, G.; Murray, R.; McKinnon, P.; Shadgan, B.; Reid, W.D. The effects of eccentric versus concentric resistance training on muscle strength and mass in healthy adults: A systematic review with meta-analysis. Br. J. Sports Med. 2009, 43, 556–568. [Google Scholar] [CrossRef] [PubMed]
- Bean, J.F.; Kiely, D.K.; Herman, S.; Leveille, S.G.; Mizer, K.; Frontera, W.R.; Fielding, R.A. The relationship between leg power and physical performance in mobility-limited older people. J. Am. Geriatr. Soc. 2002, 50, 461–467. [Google Scholar] [PubMed]
- Evans, W.J. Exercise Strategies Should Be Designed to Increase Muscle Power. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M309–M310. [Google Scholar] [CrossRef]
- Skelton, D.A.; Kennedy, J.; Rutherford, O.M. Explosive power and asymmetry in leg muscle function in frequent fallers and non-fallers aged over 65. Age Ageing 2002, 31, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Henwood, T.R.; Riek, S.; Taaffe, D.R. Strength Versus Muscle Power-Specific Resistance Training in Community-Dwelling Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2008, 63, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Reid, K.F.; Fielding, R.A. Skeletal Muscle Power: A Critical Determinant of Physical Functioning In Older Adults. Exerc. Sport Sci. Rev. 2012, 40, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Fatouros, I.G.; Kambas, A.; Katrabasas, I.; Nikolaidis, K.; Chatzinikolaou, A.; Leontsini, D.; Taxildaris, K. Strength training and detraining effects on muscular strength, anaerobic power, and mobility of inactive older men are intensity dependent. Br. J. Sports Med. 2005, 39, 776–780. [Google Scholar] [CrossRef] [PubMed]
- Vandervoort, A.A. Aging of the human neuromuscular system. Muscle Nerv. 2002, 25, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Miszko, T.A.; Cress, M.E.; Slade, J.M.; Covey, C.J.; Agrawal, S.K.; Doerr, C.E. Effect of Strength and Power Training on Physical Function in Community-Dwelling Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, M171–M175. [Google Scholar] [CrossRef]
- Granacher, U.; Zahner, L.; Gollhofer, A. Strength, power, and postural control in seniors: Considerations for functional adaptations and for fall prevention. Eur. J. Sport Sci. 2008, 8, 325–340. [Google Scholar] [CrossRef]
- Doig, M.; Macintyre, D.L.; Eng, J.J.; Narici, M.V.; Maganaris, C.N.; Reid, W.D. Preservation of eccentric strength in older adults: Evidence, mechanisms and implications for training and rehabilitation. Exp. Gerontol. 2010, 45, 400–409. [Google Scholar] [CrossRef]
- Foldvari, M.; Clark, M.; Laviolette, L.C.; Bernstein, M.A.; Kaliton, D.; Castaneda, C.; Pu, C.T.; Hausdorff, J.M.; Fielding, R.A.; Singh, M.A. Association of Muscle Power With Functional Status in Community-Dwelling Elderly Women. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, M192–M199. [Google Scholar] [CrossRef]
- Komi, P. Strength and Power in Sport; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Latham, N.K.; Bennett, D.A.; Stretton, C.M.; Anderson, C.S. Systematic review of progressive resistance strength training in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 48–61. [Google Scholar] [CrossRef]
- Seguin, R.; Nelson, M.E. The benefits of strength training for older adults. Am. J. Prev. Med. 2003, 25 (Suppl. 2), 141–149. [Google Scholar] [CrossRef]
- Cress, N.; Peters, K.; Chandler, J. Eccentric and concentric force-velocity relationships of the quadriceps femoris muscle. J. Orthop. Sports Phys. Ther. 1992, 16, 82–86. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Friedmann-Bette, B.; Bauer, T.; Kinscherf, R.; Vorwald, S.; Klute, K.; Bischoff, D.; Müller, H.; Weber, M.A.; Metz, J.; Kauczor, H.U.; et al. Effects of strength training with eccentric overload on muscle adaptation in male athletes. Eur. J. Appl. Physiol. 2010, 108, 821–836. [Google Scholar] [CrossRef] [PubMed]
- Gault, M.L.; Willems, M.E.T. Aging, Functional Capacity and Eccentric Exercise Training. Aging Dis. 2013, 4, 351–363. [Google Scholar] [CrossRef] [PubMed]
- Isner-Horobeti, M.E.; Dufour, S.P.; Vautravers, P.; Geny, B.; Coudeyre, E.; Richard, R. Eccentric Exercise Training: Modalities, Applications and Perspectives. Sports Med. 2013, 43, 483–512. [Google Scholar] [CrossRef] [PubMed]
- Hedayatpour, N.; Falla, D. Physiological and Neural Adaptations to Eccentric Exercise: Mechanisms and Considerations for Training. BioMed Res. Int. 2015, 193741, 7. [Google Scholar] [CrossRef] [PubMed]
- Norrbrand, L.; Fluckey, J.D.; Pozzo, M.; Tesch, P.A. Resistance training using eccentric overload induces early adaptations in skeletal muscle size. Eur. J. Appl. Physiol. 2008, 102, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Reeves, N.D.; Maganaris, C.N.; Longo, S.; Narici, M.V. Differential adaptations to eccentric versus conventional resistance training in older humans. Exp. Physiol. 2009, 94, 825–833. [Google Scholar] [CrossRef]
- Onambélé, G.L.; Maganaris, C.N.; Mian, O.S.; Tam, E.; Rejc, E.; McEwan, I.M.; Narici, M.V. Neuromuscular and balance responses to flywheel inertial versus weight training in older persons. J. Biomech. 2008, 41, 3133–3138. [Google Scholar] [CrossRef]
- Tesch, P.A.; Fernandez-Gonzalo, R.; Lundberg, T.R. Clinical Applications of Iso-Inertial, Eccentric-Overload (YoYoTM) Resistance Exercise. Front. Physiol. 2017, 8, 241. [Google Scholar] [CrossRef]
- Bruseghini, P.; Calabria, E.; Tam, E.; Milanese, C.; Oliboni, E.; Pezzato, A.; Pogliaghi, S.; Salvagno, G.L.; Schena, F.; Mucelli, R.P.; et al. Effects of eight weeks of aerobic interval training and of isoinertial resistance training on risk factors of cardiometabolic diseases and exercise capacity in healthy elderly subjects. Oncotarget. 2015, 6, 16998–17015. [Google Scholar] [CrossRef]
- Clark, D.J.; Patten, C. Eccentric versus concentric resistance training to enhance neuromuscular activation and walking speed following stroke. Neurorehabilit. Neural Repair. 2013, 27, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Vásquez-Morales, A.; Sanz-Valero, J.; Wanden-Berghe, C. Eccentric exercise as preventive physical option in people over 65 years: A systematic review of the scientific literature. Enferm. Clin. 2013, 23, 48–55. [Google Scholar] [CrossRef]
- Semmler, J.G.; Kornatz, K.W.; Dinenno, D.V.; Zhou, S.; Enoka, R.M. Motor unit synchronisation is enhanced during slow lengthening contractions of a hand muscle. J. Physiol. (Lond.) 2002, 545, 681–695. [Google Scholar] [CrossRef] [PubMed]
- Knuttgen, H.G.; Petersen, F.B.; Klausen, K. Oxygen uptake and heart rate responses to exercise performed with concentric and eccentric muscle contractions. Med. Sci. Sports. 1971, 3, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Illera-Domínguez, V.; Nuell, S.; Carmona, G.; Padullés Riu, J.M.; Padullés, X.; Lloret, M.; Cussó, M.R.; Alomar, X.; Cadefau, J.A. Early Functional and Morphological Muscle Adaptations During Short-Term Inertial-Squat Training. Front. Physiol. 2018, 9, 1265. [Google Scholar] [CrossRef] [PubMed]
- Gerber, J.P.; Marcus, R.L.; Dibble, L.E.; Greis, P.E.; Burks, R.T.; LaStayo, P.C. Effects of early progressive eccentric exercise on muscle size and function after anterior cruciate ligament reconstruction: A 1-year follow-up study of a randomized clinical trial. Phys. Ther. 2009, 89, 51–59. [Google Scholar] [CrossRef] [PubMed]
- LaStayo, P.C.; Pierotti, D.J.; Pifer, J.; Hoppeler, H.; Lindstedt, S.L. Eccentric ergometry: Increases in locomotor muscle size and strength at low training intensities. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 278, R1282–R1288. [Google Scholar] [CrossRef]
- Fernandez-Gonzalo, R.; Fernandez-Gonzalo, S.; Turon, M.; Prieto, C.; Tesch, P.A.; del Carmen García-Carreira, M. Muscle, functional and cognitive adaptations after flywheel resistance training in stroke patients: A pilot randomized controlled trial. J. Neuroeng. Rehabil. 2016, 13, 37. [Google Scholar] [CrossRef]
- Hortobágyi, T.; DeVita, P. Favorable neuromuscular and cardiovascular responses to 7 days of exercise with an eccentric overload in elderly women. J. Gerontol. A Biol. Sci. Med. Sci. 2000, 55, B401–B410. [Google Scholar] [CrossRef]
- LaStayo, P.C.; Ewy, G.A.; Pierotti, D.D.; Johns, R.K.; Lindstedt, S. The positive effects of negative work: Increased muscle strength and decreased fall risk in a frail elderly population. J. Gerontol. A Biol. Sci. Med. Sci. 2003, 58, M419–M424. [Google Scholar] [CrossRef]
- Carroll, K.M.; Wagle, J.P.; Sato, K.; Taber, C.B.; Yoshida, N.; Bingham, G.E.; Stone, M.H. Characterising overload in inertial flywheel devices for use in exercise training. Sports Biomech. 2018, 18, 390–401. [Google Scholar] [CrossRef] [PubMed]
- Suchomel, T.J.; Wagle, J.P.; Douglas, J.; Taber, C.B.; Harden, M.; Haff, G.G. Implementing eccentric resistance training-part 1: A brief review of existing methods. J. Funct. Morphol. Kinesiol. 2019, 4, 38. [Google Scholar] [CrossRef]
- Norrbrand, L.; Pozzo, M.; Tesch, P.A. Flywheel resistance training calls for greater eccentric muscle activation than weight training. Eur. J. Appl. Physiol. 2010, 110, 997–1005. [Google Scholar] [CrossRef] [PubMed]
- Alkner, B.A.; Bring, D.K.I. Muscle activation during gravity-independent resistance exercise compared to common exercises. Aerosp. Med. Hum. Perform. 2019, 90, 506–512. [Google Scholar] [CrossRef] [PubMed]
- de Hoyo, M.; de la Torre, A.; Pradas, F.; Sanudo, B.; Carrasco, L.; Mateo-Cortes, J.; Dominguez-Cobo, S.; Fernandes, O.; Gonzalo-Skok, O. Effects of eccentric overload bout on change of direction and performance in soccer players. Int. J. Sports Med. 2015, 36, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Bollinger, L.M.; Brantley, J.T.; Tarlton, J.K.; Baker, P.A.; Seay, R.F.; Abel, M.G. Construct Validity, Test-Retest Reliability, and Repeatability of Performance Variables Using a Flywheel Resistance Training Device. J. Strength Cond. Res. 2018, in press. [Google Scholar] [CrossRef] [PubMed]
- Weakley, J.; Fernández-Valdés, B.; Thomas, L.; Ramirez-Lopez, C.; Jones, B. Criterion Validity of Force and Power Outputs for a Commonly Used Flywheel Resistance Training Device and Bluetooth App. J. Strength Cond. Res. 2019, 33, 1180. [Google Scholar] [CrossRef]
- Sanchez, F.J.N.; de Villarreal, E.S.S. Does flywheel paradigm training improve muscle volume and force? A meta-analysis. J. Strength Cond. Res. 2017, 31, 3177–3186. [Google Scholar] [CrossRef]
- Petrie, H.; Wernstal, F.; Mattsson, C.M. Effects of flywheel training on strength-related variables: A meta-analysis. Sports Med. Open 2018, 4, 55. [Google Scholar] [CrossRef]
- Maroto-Izquierdo, S.; García-López, D.; Fernandez-Gonzalo, R.; Moreira, O.C.; González-Gallego, J.; de Paz, J.A. Skeletal muscle functional and structural adaptations after eccentric overload flywheel resistance training: A systematic review and meta-analysis. J. Sci. Med. Sport 2017, 20, 943–951. [Google Scholar] [CrossRef]
- Vicens-Bordas, J.; Esteve, E.; Fort-Vanmeerhaeghe, A.; Bandholm, T.; Thorborg, K. Is inertial flywheel resistance training superior to gravity-dependent resistance training in improving muscle strength? A systematic review with meta-analyses. J. Sci. Med. Sport 2018, 21, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Sañudo, B.; González-Navarrete, Á.; Álvarez-Barbosa, F.; de Hoyo, M.; del Pozo, J.; Rogers, M.E. Effect of Flywheel Resistance Training on Balance Performance in Older Adults. A Randomized Controlled Trial. J. Sports Sci. Med. 2019, 18, 344–350. [Google Scholar] [PubMed]
- Glenn, J.M.; Gray, M.; Vincenzo, J.; Paulson, S.; Powers, M. An evaluation of functional sit-to-stand power in cohorts of health adults aged 18–97 years. J. Aging Phys. Act. 2017, 25, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Gonzalo, R.; Lundberg, T.R.; Alvarez-Alvarez, L.; de Paz, J.A. Muscle damage responses and adaptations to eccentric-overload resistance exercise in men and women. Eur. J. Appl. Physiol. 2014, 114, 1075–1084. [Google Scholar] [CrossRef] [PubMed]
- Sarmiento, S.; Rodriguez-Matoso, D.; Henriquez del Pino, Y.; Alvarez-Pinera, L.; Garcia-Manso, J.M.; Rodriguez-Ruiz, D. Effects of flywheel resistance training for gait improvement in female Alzheimer’s patients. J. Strength Cond. Res. 2014, 28 (Suppl. 1), 48. [Google Scholar]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kowalchuk, K.; Butcher, S. Eccentric Overload Flywheel Training in Older Adults. J. Funct. Morphol. Kinesiol. 2019, 4, 61. https://doi.org/10.3390/jfmk4030061
Kowalchuk K, Butcher S. Eccentric Overload Flywheel Training in Older Adults. Journal of Functional Morphology and Kinesiology. 2019; 4(3):61. https://doi.org/10.3390/jfmk4030061
Chicago/Turabian StyleKowalchuk, Kelsi, and Scotty Butcher. 2019. "Eccentric Overload Flywheel Training in Older Adults" Journal of Functional Morphology and Kinesiology 4, no. 3: 61. https://doi.org/10.3390/jfmk4030061
APA StyleKowalchuk, K., & Butcher, S. (2019). Eccentric Overload Flywheel Training in Older Adults. Journal of Functional Morphology and Kinesiology, 4(3), 61. https://doi.org/10.3390/jfmk4030061