Validation of Cardiorespiratory Fitness Measurements in Adolescents

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Procedures
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Parrett, A.L.; Valentine, R.J.; Arngrimsson, S.A.; Castelli, D.M.; Evans, E.M. Adiposity and aerobic fitness are associated with metabolic disease risk in children. Appl. Physiol. Nutr. Metab. 2011, 36, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Lukacs, A.; Varga, B.; Kiss-Toth, E.; Soos, A.; Barkai, L. Factors influencing the diabetes-specific health-related quality of life in children and adolescents with type 1 diabetes mellitus. J. Child Heal. Care 2014, 18, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Twisk, J.W.R.; Kemper, H.C.G.; Mechelen, W. Van Tracking of activity and fitness and the relationship with cardiovascular disease risk factors. Med. Sci. Sport. Exerc. 2000, 1455–1461. [Google Scholar] [CrossRef]
- Houston, E.L.; Baker, J.S.; Buchan, D.S.; Stratton, G.; Fairclough, S.J.; Foweather, L.; Gobbi, R.; Graves, L.E.F.; Hopkins, N.; Boddy, L.M. Cardiorespiratory fitness predicts clustered cardiometabolic risk in 10–11.9-year-olds. Eur. J. Pediatr. 2013, 172, 913–918. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.P.; Boddy, L.M.; Savory, L.A.; Denton, S.J.; Kerr, C.J. Associations between cardiorespiratory fitness, physical activity and clustered cardiometabolic risk in children and adolescents: The HAPPY study. Eur. J. Pediatr. 2012, 171, 1317–1323. [Google Scholar] [CrossRef] [PubMed]
- Chaddock, L.; Hillman, C.H.; Pontifex, M.B.; Johnson, C.R.; Raine, L.B.; Kramer, A.F. Childhood aerobic fitness predicts cognitive performance one year later. J. Sports Sci. 2012, 30, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Haapala, E.A. Cardiorespiratory Fitness and Motor Skills in Relation to Cognition and Academic Performance in Children – A Review by. J. Hum. Kinet. 2013, 36, 55–68. [Google Scholar] [CrossRef]
- Chaddock, L.; Erickson, K.I.; Prakash, R.S.; Vanpatter, M.; Voss, M.W.; Pontifex, M.B.; Raine, L.B.; Hillman, C.H.; Kramer, A.F. Basal ganglia volume is associated with aerobic fitness in preadolescent children. Dev. Neurosci. 2010, 32, 249–256. [Google Scholar] [CrossRef]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Pontifex, M.B.; Raine, L.B.; Johnson, C.R.; Chaddock, L.; Voss, M.W.; Cohen, N.; Kramer, A.F.; Hillman, C.H. Cardiorespiratory Fitness and the Flexible Modulation of Cognitive Control in Preadolescent Children. J. Cogn. Neurosci. 2010, 23, 1332–1345. [Google Scholar] [CrossRef]
- Chaddock, L.; Erickson, K.I.; Prakash, R.S.; Kim, J.S.; Voss, M.W.; VanPatter, M.; Pontifex, M.B.; Raine, L.B.; Konkel, A.; Hillman, C.H.; et al. A neuroimaging investigation of the association between aerobic fitness, hippocampal volume, and memory performance in preadolescent children. Brain Res. 2014, 1358, 172–183. [Google Scholar] [CrossRef] [PubMed]
- Huotari, P.; Nupponen, H.; Mikkelsson, L.; Laakso, L.; Kujala, U. Adolescent physical fitness and activity as predictors of adulthood activity. J. Sports Sci. 2011, 29, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Jose, K.A.; Blizzard, L.; Dwyer, T.; Mckercher, C.; Venn, A.J. Childhood and adolescent predictors of leisure time physical activity during the transition from adolescence to adulthood: A population based cohort study. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Davis, J. Direct determination of aerobic power. In Physiological Assessment of Human Fitness; Human Kinetics: Champaign, IL, USA, 1995; pp. 9–17. [Google Scholar]
- Ward, A.; Ebbeling, C.; Ahlquist, L. Indirect methods for estimation of aerobic power. In Physiological Assessment of Human Fitness; Human Kinetics: Champaign, IL, USA, 1995; pp. 37–56. [Google Scholar]
- Van Mechelen, W.; Hlobil, H.; Kemper, H.C.G. Validation of two running tests as estimates of maximal aerobic power in children. Eur. J. Appl. Physiol. 1986, 55, 503–506. [Google Scholar] [CrossRef]
- Mayorga-Vega, D.; Aguilar-Soto, P.; Viciana, J. Criterion-related validity of the 20-m shuttle run test for estimating cardiorespiratory fitness: A meta-analysis. J. Sport. Sci. Med. 2015, 14, 536–547. [Google Scholar]
- Meredith, M.; Welk, G. FITNESSGRAM®/ACTIVITYGRAM® Test Administration Manual, 4th ed.; Human Kinetics: Champaign, IL, USA, 2013; Available online: www.cooperinstitute.org/vault/2440/web/files/662.pdf (accessed on 31 December 2017).
- Kabiri, L.S.; Mitchell, K.; Brewer, W.; Ortiz, A. Muscular and Cardiorespiratory Fitness in Homeschool versus Public School Children Running. Pediatr. Exerc. Sci. 2017, 29, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Mahar, M.T.; Welk, G.J.; Rowe, D.A.; Crotts, D.J.; Mciver, K.L. Development and Validation of a Regres- sion Model to Estimate VO2peak From PACER 20-m Shuttle Run Performance. J. Phys. Act. Health 2006, 3, 34–46. [Google Scholar] [CrossRef]
- Jurca, R.; Jackson, A.S.; Lamonte, M.J.; Morrow, J.R., Jr.; Blair, S.N.; Wareham, N.J.; Haskell, W.L.; Van Mechelen, W.; Church, T.S.; Jakicic, J.M. Assessing Cardiorespiratory Fitness Without Performing Exercise Testing. Am. J. Prev. Med. 2005, 29, 185–193. [Google Scholar] [CrossRef]
- Jackson, A.S.; Sui, X.; Connor, D.P.O.; Church, T.S.; Lee, D.; Artero, E.G.; Blair, S.N. Longitudinal Cardiorespiratory Fitness Alogrithms for Clinical Settings. Am. J. Prev. Med. 2012, 43, 512–519. [Google Scholar] [CrossRef]
- Duffield, R.; Dawson, B.; Pinnington, H.; Wong, P. Accuracy and reliabillity of a Cosmed K4b 2 portable gas aScience, Exercisenalysis system. J. Sci. Med. Sport 2004, 7, 11–22. [Google Scholar] [CrossRef]
- Schrack, J.A.; Simonsick, E.M.; Ferrucci, L. Comparison of the Cosmed K4b2 Portable Metabolic System in Measuring Steady-State Walking Energy Expenditure. PLoS ONE 2010, 5, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.; Oliveira, N.L.; Aires, L.; Mota, J.; Oliveira, J.; Ribeiro, J.C. Calculation and validation of models for estimating VO2max from the 20-m shuttle run test in children and adolescents Gustavo. Arch. Exerc. Heal. Dis. 2012, 2, 145–152. [Google Scholar] [CrossRef]
- Mahar, M.T.; Guerieri, A.M.; Hanna, M.S.; Kemble, C.D. Estimation of Aerobic Fitness from 20-m Multistage Shuttle Run Test Performance. Am. J. Prev. Med. 2011, 41, S117–S123. [Google Scholar] [CrossRef] [PubMed]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice, 3rd ed.; F.A. Davis Company: Philadelphia, PA, USA, 2015; p. 525. [Google Scholar]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physical Activity Level | Description | Score |
|---|---|---|
| 1 | Inactive or little activity other than usual daily activities. | 0.00 |
| 2 | Regularly (≥5 d/wk) participate in physical activities requiring low levels of exertion that result in slight increases in breathing and heart rate for at least 10 min at a time. | 0.32 |
| 3 | Participate in aerobic exercises such as brisk walking, jogging or running, cycling, swimming, or vigorous sports at a comfortable pace or other activities requiring similar levels of exertion for 20 to 60 min per week. | 1.06 |
| 4 | Participate in aerobic exercises such as brisk walking, jogging or running at a comfortable pace, or other activities requiring similar levels of exertion for 1 to 3 h per week. | 1.76 |
| 5 | Participate in aerobic exercises such as brisk walking, jogging or running at a comfortable pace, or other activities requiring similar levels of exertion for over 3 h per week. | 3.03 |
| Variables | All Participants (n = 46) Mean ± SD [range] |
|---|---|
| Age (years) | 14.56 ± 1.69; [12.00–18.00] |
| Height (cm) | 165.65 ± 10.05; [147.00–188.00] |
| Weight (kg) | 60.44 ± 13.57; [38.20, 93.80] |
| BMI (kg/m2) | 21.88 ± 3.91; [16.20–33.40] |
| BMI Percentiles (%) | 61.89 ± 26.35; [9.00, 98.00] |
| Bodyfat % (DXA) | 24.27 ±8.35; [13.20, 45.10] |
| Pubertal Level (PDS) | 2.71 ± 0.81; [0.00, 4.00] |
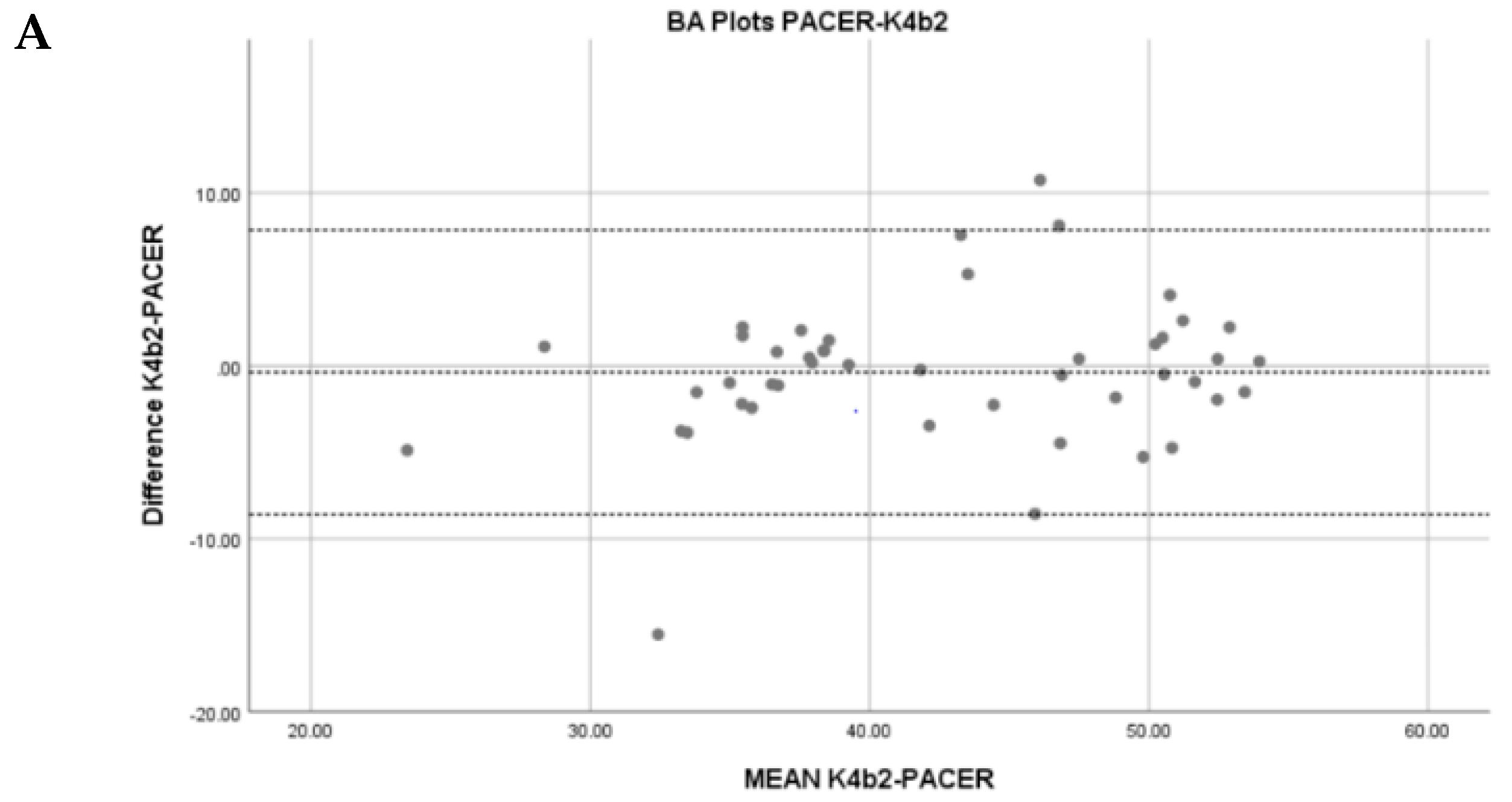
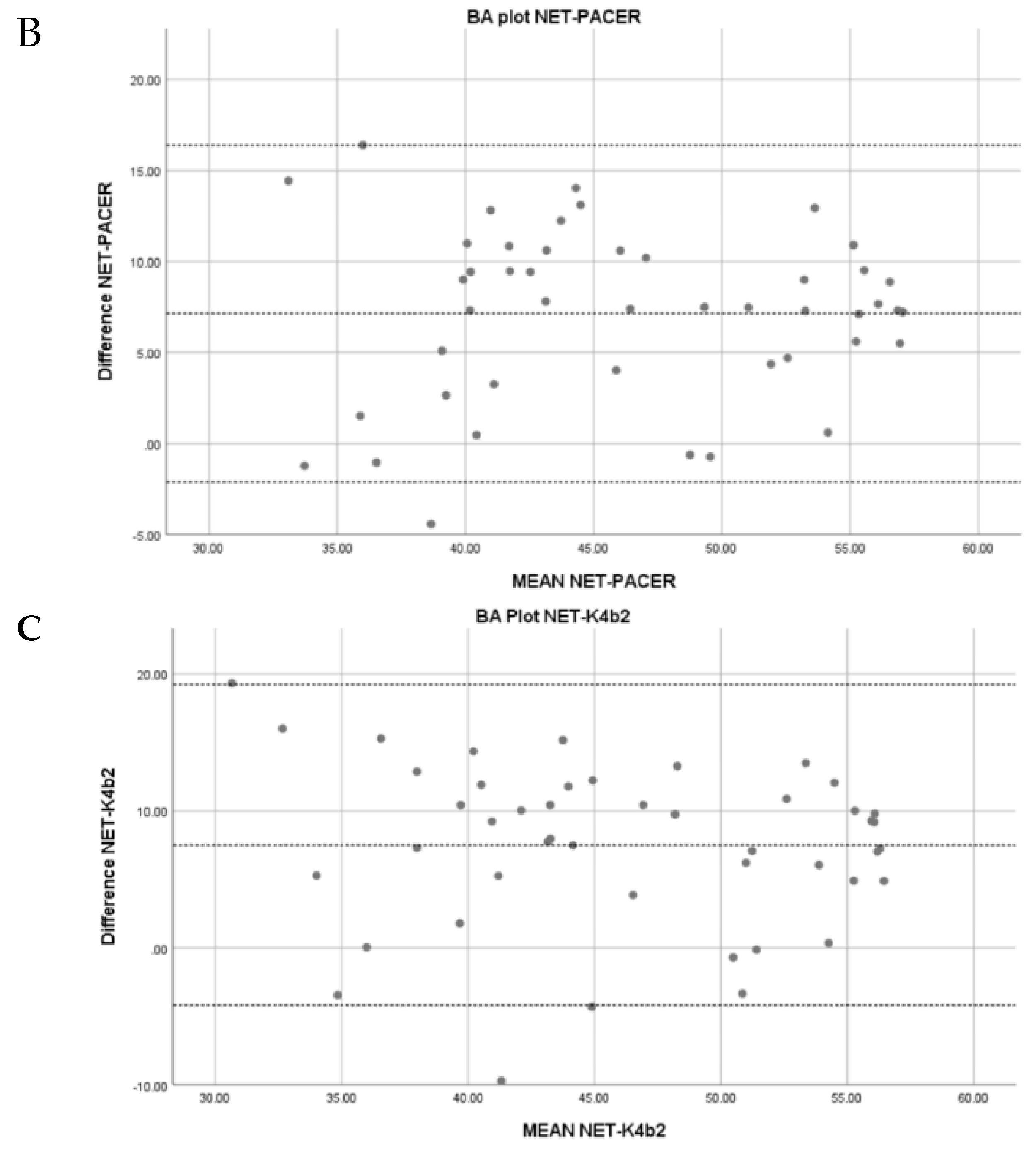
| K4b2 VO2max (mL/kg/min) | 42.29 ± 8.37; [20.99, 54.09] |
| PACER VO2max Estimate (mL/kg/min) | 42.67 ± 7.49; [25.88, 54.20] |
| NET VO2max Estimate (mL/kg/min) | 49.82 ± 7.67; [33.11, 60.99] |
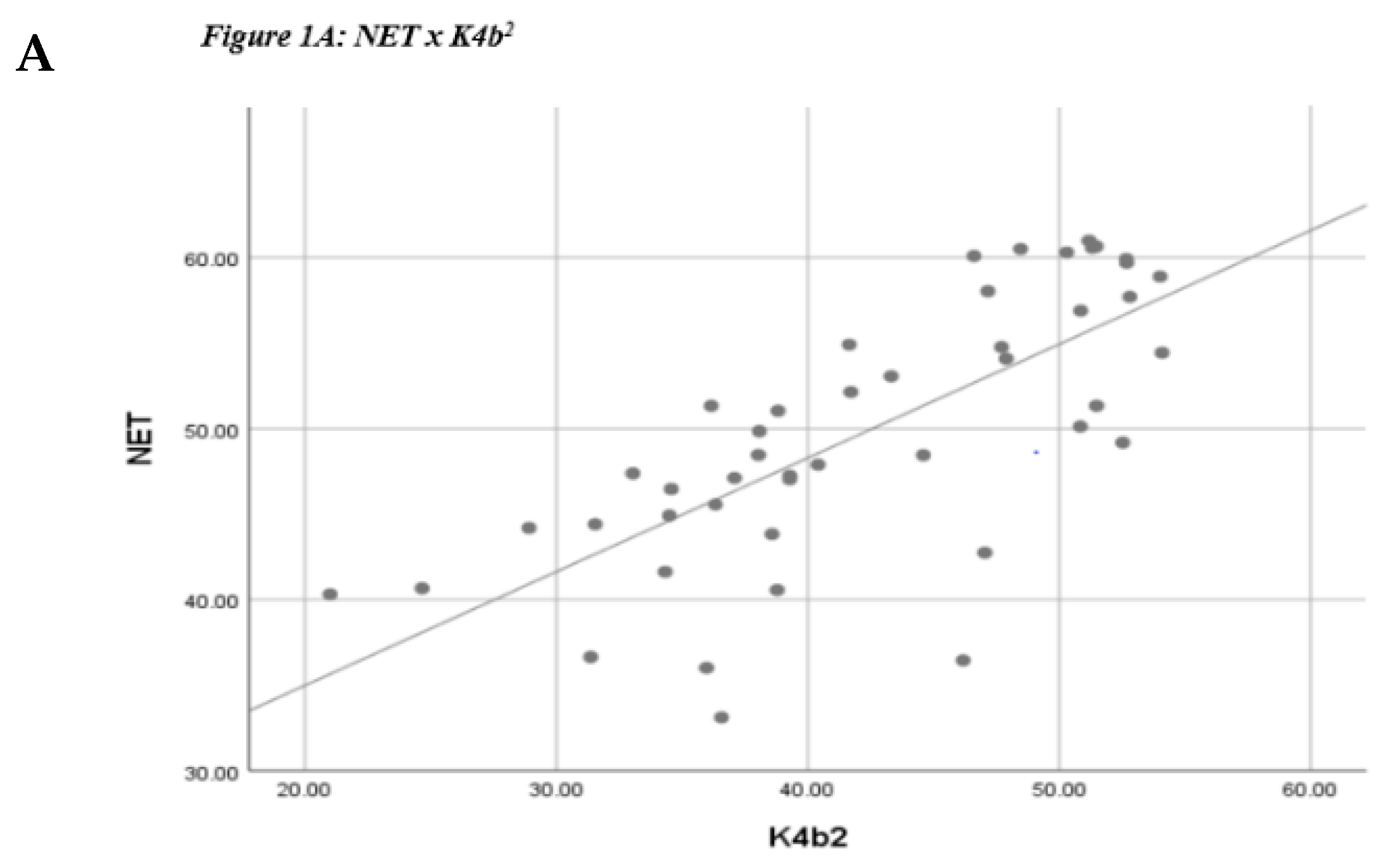
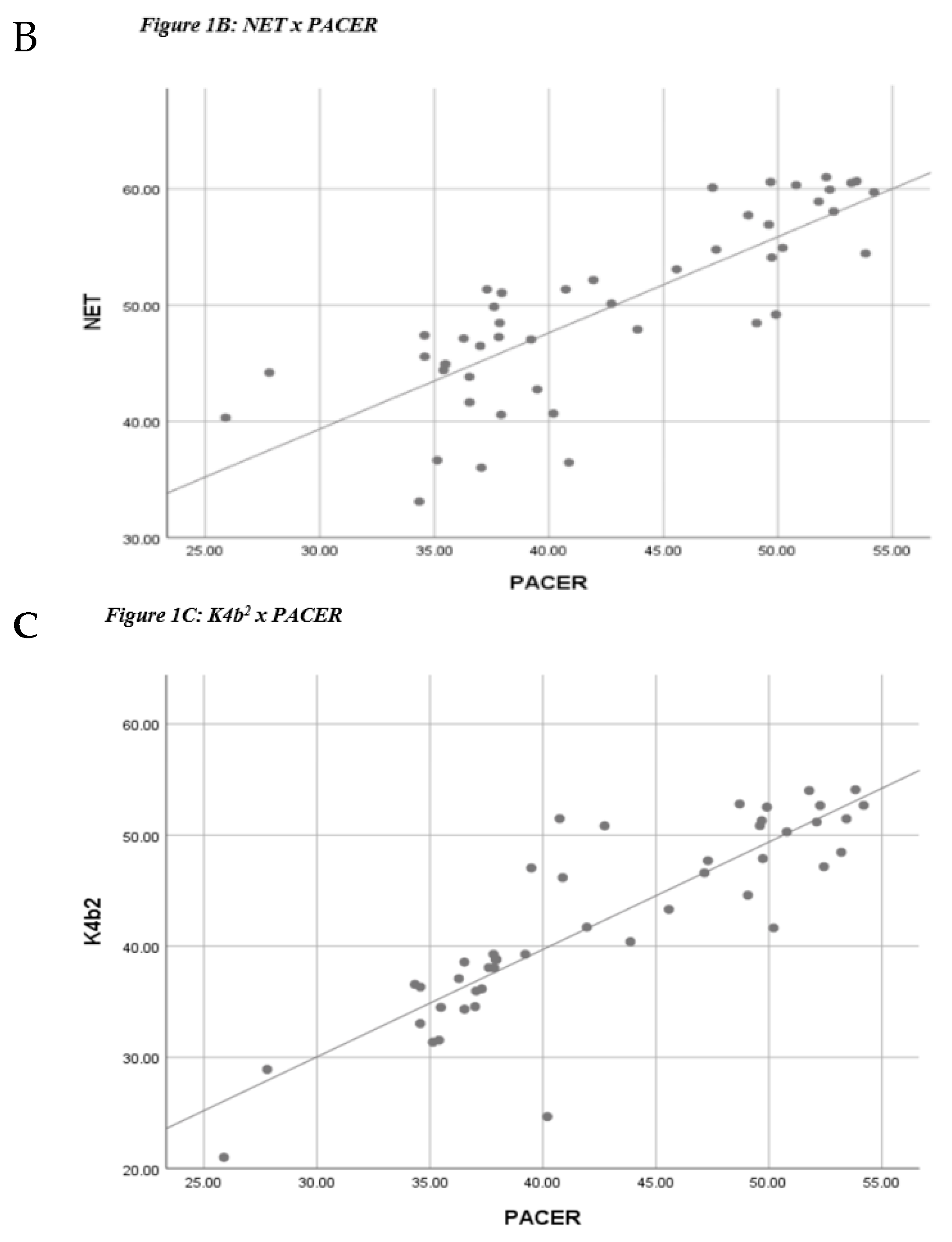
| Correlations | |||
|---|---|---|---|
| PACER | NET | K4B2 | |
| PACER | |||
| NET | r = 0.81; p < 0.001 r2 = 0.65 ICC = 0.72 SEE = 8.53 mL/kg/min [0.57, 0.99] | ||
| K4B2 | r = 0.87; p < 0.001 r2 = 0.75 ICC = 0.93 SEE = 4.17 mL/kg/min [0.70, 1.0] | r = 0.73; p < 0.001 r2 = 0.53 ICC = 0.67 SEE = 9.56 mL/kg/min [0.50, 0.97] | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Migliano, P.; Kabiri, L.S.; Cross, M.; Butcher, A.; Frugé, A.; Brewer, W.; Ortiz, A. Validation of Cardiorespiratory Fitness Measurements in Adolescents. J. Funct. Morphol. Kinesiol. 2019, 4, 44. https://doi.org/10.3390/jfmk4030044
Migliano P, Kabiri LS, Cross M, Butcher A, Frugé A, Brewer W, Ortiz A. Validation of Cardiorespiratory Fitness Measurements in Adolescents. Journal of Functional Morphology and Kinesiology. 2019; 4(3):44. https://doi.org/10.3390/jfmk4030044
Chicago/Turabian StyleMigliano, Pedro, Laura S. Kabiri, Megan Cross, Allison Butcher, Amy Frugé, Wayne Brewer, and Alexis Ortiz. 2019. "Validation of Cardiorespiratory Fitness Measurements in Adolescents" Journal of Functional Morphology and Kinesiology 4, no. 3: 44. https://doi.org/10.3390/jfmk4030044