
Safeguarding against Dementia in Aboriginal and Torres Strait Islander Communities through the Optimisation of Primary Health Care: A Project Protocol
 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Aims and Objectives
- Strengthen clinical performance for preventing, identifying, treating, and managing potentially modifiable risk factors associated with dementia.
- Strengthen the availability of preventative health and health promotion services for safeguarding against dementia.
- Integrate clinical performance and service strengthening strategies and programs into ongoing practice and organisation policies and procedures.
- 4.
- Strengthen the capacity of PHC staff to undertake CQI and deliver best practice care for the prevention, identification, treatment, and management of dementia risk in everyday clinical practice.
- 5.
- Strengthen the capacity of Aboriginal and Torres Strait Islander communities to understand dementia and health promotion approaches to safeguarding against dementia.
- 6.
- Integrate capacity-strengthening strategies into ongoing organisational practice, policies, and procedures.
- Utilise a participatory action research approach to identify and co-develop PHC deliverable dementia safeguarding strategies, programs, and resources.
- Utilise a continuous quality improvement methodology to implement and evaluate PHC deliverable strategies and programs, for strengthening clinical service performance and the availability of health services for safeguarding against dementia in Aboriginal and Torres Strait Islander communities.
- Evaluate this approach and methodology for appropriateness, effectiveness, and sustainability in achieving the project aims and objectives and answering the research question.
- Work with PHC staff to identify opportunities for training on CQI and dementia safeguarding practices.
- Work with the community to identify opportunities for strengthening the knowledge and understanding of dementia and associated safeguarding strategies.
- Integrate dementia safeguarding strategies and programs into clinical practice and organisation policies and procedures.
- Integrate community and staff capacity-building strategies into organisation policies and procedures.
- Synthesise the evidence into a culturally appropriate framework and accompanying tool kit for Aboriginal and Torres Strait Islander PHC organisations to identify, implement, and evaluate their own dementia safeguarding practice and service improvements.
3. Research Question
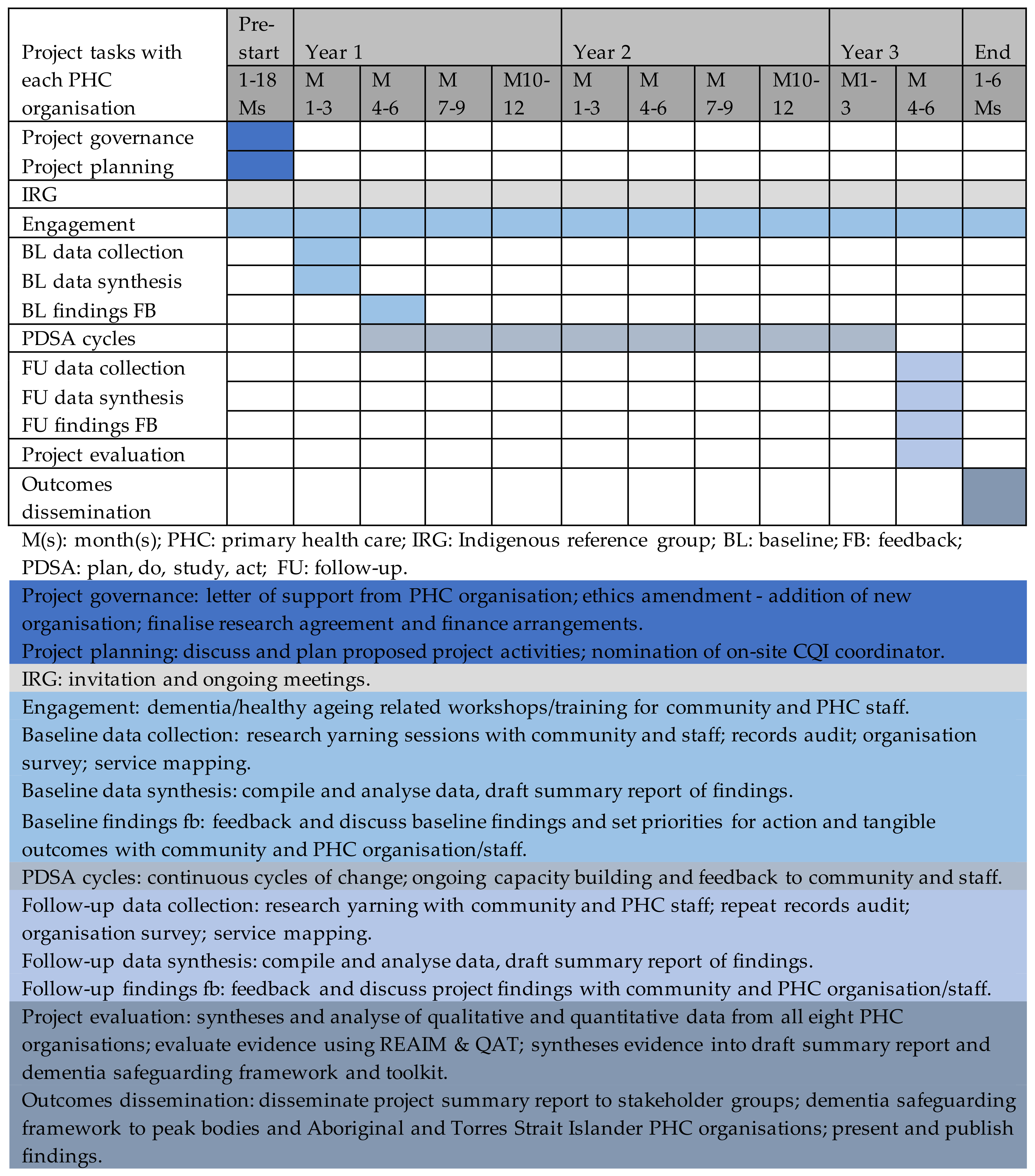
4. Methodology and Methods
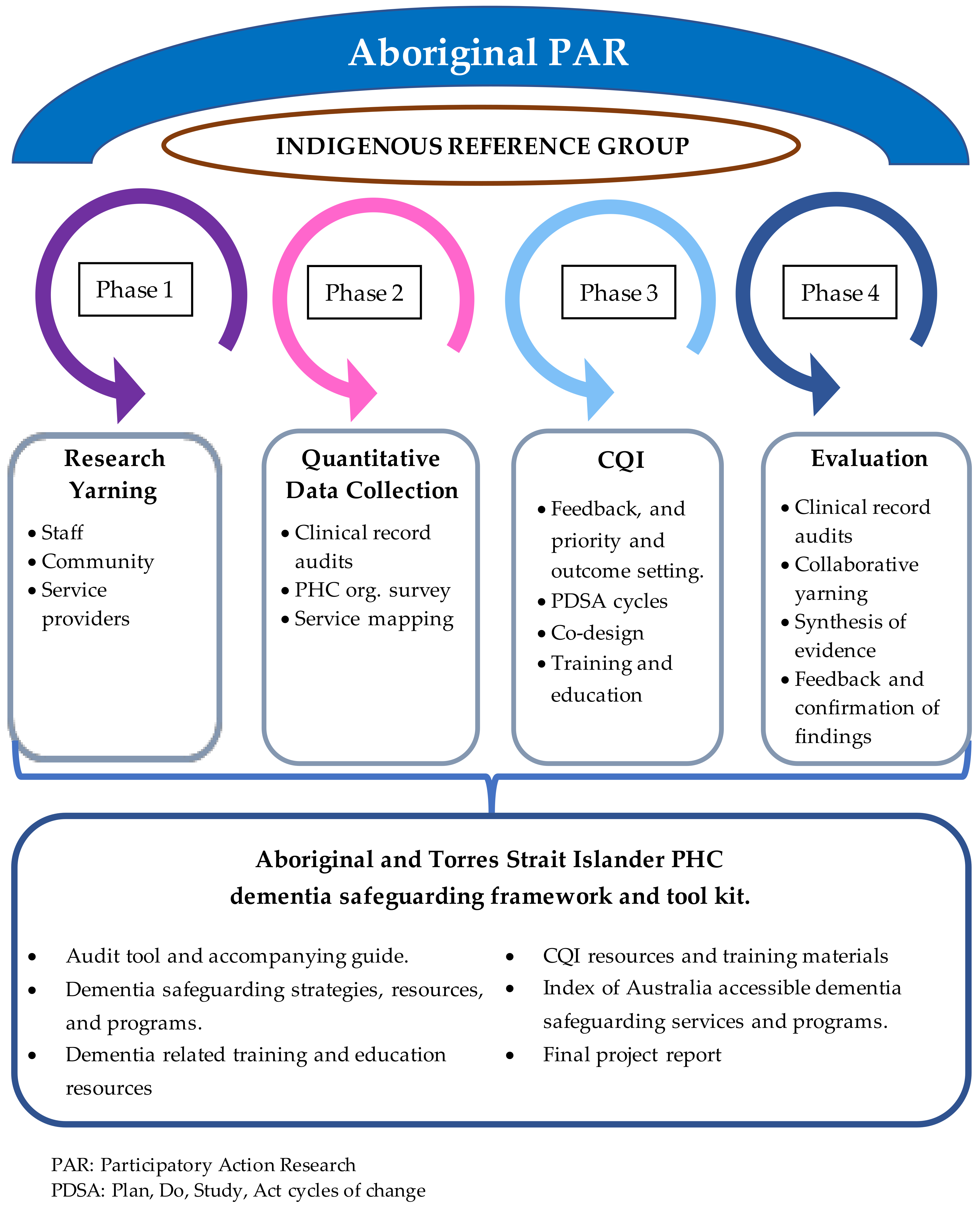
4.1. Design
4.2. Setting
4.3. Facilitation
4.4. Indigenous Reference Group
4.5. Engagement Activities
5. Aboriginal Participatory Action Research (APAR)
- The involvement of Aboriginal co-researchers in supporting communities to collectively identify risk and protective factors;
- A research process that respects Indigenous peoples as experts-by-experience of their own health, their families, and their communities;
- Indigenous leadership and governance and the establishment of local Indigenous community reference groups;
- Localised knowledge generation;
- Community-level feedback and dissemination;
- The enactment of the NHMRC Indigenous core values;
- The application of nine guiding principles: (i) Indigenous health being viewed in a holistic context; (ii) Indigenous choice being a central health service provision; (iii) care being culturally informed; (iv) the impact of colonisation on physical and mental health; (v) human rights being respected; (vi) the impact of racism, stigma, contextual adversity, and disadvantage; (vii) the centrality of Indigenous kinship; (viii) the diversity of Indigenous peoples and their environments and circumstances; and (ix) the recognition of their strengths and abilities and connection to community and country.
6. Phase One: Yarning
- Aboriginal and/or Torres Strait Islander Elders, community members, and dementia advocates, aged 18 years and over, who are a regular client at the participating PHC organisation;
- Aboriginal and/or Torres Strait Islander PHC staff including management, administration, clinical and non-clinical staff, and service providers, with the aim to have mixed representation from each group.
7. Phase Two: Quantitative Data Collection
7.1. Clinical Records Audit
7.2. PHC Organisation Survey
7.3. Health Service Mapping
7.4. Data Analysis
8. Phase Three: CQI Activities
PDSA Cycles
- (i)
- Review and discuss the qualitative and quantitative evidence in the baseline findings summary report and work together to identify the strengths, limitations, and gaps in current clinical performance and health services;
- (ii)
- In consideration of all the evidence, identify opportunities for clinical and/or health service strengthening activities, confirm one to two priorities for action, and break them down into tangible outcomes;
- (iii)
- Work together as a multidisciplinary team to develop an action plan to address each priority, including the aim, objectives, and outcome measures, an appropriate strategy or program to implement, the resources and steps required for implementation, a subset of data (e.g., smoking status and health organisation response) from the clinical records to be collected and reviewed to measure progress, and opportunities to merge with existing policies and processes.
9. Phase Four: Evaluation
10. Project Evaluation
Project Outcomes
- I
- Workforce capacity of the partnering Aboriginal and Torres Strait Islander PHC organisation to provide clinical care and health services in accordance with clinical best practice guidelines [42,43] for the prevention, early identification, treatment, and management of risk factors associated with dementia in Aboriginal and Torres Strait Islander peoples;
- II
- The knowledge and capacity of Aboriginal and/or Torres Strait Islander peoples to understand dementia, recognise protective and risk factors, and respond with appropriate preventative health and health promotion strategies to help safeguard themselves, their kin, and the broader community against dementia in later life.
- I
- Clinical service performance for the prevention, early identification, treatment, and management of risk factors associated with dementia in Aboriginal and Torres Strait Islander peoples;
- II
- The availability of health services for promoting health and preventing or managing risk factors associated with dementia in Aboriginal and Torres Strait Islander peoples;
- III
- Integration of changes to clinical service performance and available health services for safeguarding Aboriginal and/or Torres Strait Islander clients against dementia in later life.
11. Aboriginal and Torres Strait Islander Research Quality Evaluation
12. Data Management
13. Project Outputs
14. Dissemination
15. Limitations
16. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Bureau of Statistics. (2015–2017). Life Tables for Aboriginal and Torres Strait Islander Australians. ABS. Available online: https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/aboriginal-and-torres-strait-islander-life-expectancy-estimates/latest-release (accessed on 15 October 2023).
- World Health Organization. Ageing and Health; World Health Organization: Geneva, Switzerland, 2022; Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 15 October 2023).
- Australian Institute of Health and Welfare. Dementia in Australia; AIHW: Canberra, Australia, 2021.
- Temple, J.; Wilson, T.; Radford, K.; LoGiudice, D.; Utomo, A.; Anstey, K.J.; Eades, S. Demographic drivers of the growth of the number of Aboriginal and Torres Strait Islander people living with dementia, 2016–2051. Australas. J. Ageing 2022, 41, e320–e327. [Google Scholar] [CrossRef]
- Radford, K.; Mack, H.A.; Draper, B.; Chalkley, S.; Daylight, G.; Cumming, R.; Bennett, H.; Delbaere, K.; Broe, G.A. Prevalence of dementia in urban and regional Aboriginal Australians. Alzheimer’s Dement. 2015, 11, 271–279. [Google Scholar] [CrossRef]
- Russell, S.G.; Quigley, R.; Thompson, F.; Sagigi, B.; LoGiudice, D.; Smith, K.; Pachana, N.; Miller, G.; Strivens, E. Prevalence of dementia in the Torres Strait. Australas. J. Ageing 2021, 40, e125–e132. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.; Flicker, L.; Lautenschlager, N.; Almeida, O.; Atkinson, D.; Dwyer, A.; LoGiudice, D. High prevalence of dementia and cognitive impairment in Indigenous Australians. Neurology 2008, 71, 1470–1473. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Radford, K.; Lavrencic, L.M.; Delbaere, K.; Draper, B.; Cumming, R.; Daylight, G.; Mack, H.A.; Chalkley, S.; Bennett, H.; Garvey, G.; et al. Factors Associated with the High Prevalence of Dementia in Older Aboriginal Australians. J. Alzheimers Dis. 2019, 70, S75–S85. [Google Scholar] [CrossRef]
- Russell, S.G.; Quigley, R.; Thompson, F.; Sagigi, B.; Miller, G.; LoGiudice, D.; Smith, K.; Pachana, N.A.; Strivens, E. Factors associated with the increased risk of dementia found in the Torres Strait. Australas. J. Ageing 2022, 41, 88–96. [Google Scholar] [CrossRef]
- Smith, K.; Flicker, L.; Dwyer, A.; Atkinson, D.; Almeida, O.P.; Lautenschlager, N.T.; LoGiudice, D. Factors associated with dementia in Aboriginal Australians. Aust. N. Z. J. Psychiatry 2010, 44, 888–893. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, D.; Smith, K.; Fenner, S.; Hyde, Z.; Atkinson, D.; Skeaf, L.; Malay, R.; Flicker, L. Incidence and predictors of cognitive impairment and dementia in Aboriginal Australians: A follow-up study of 5 years. Alzheimers Dement. 2016, 12, 252–261. [Google Scholar] [CrossRef]
- Fogarty, W.; Bulloch, H.; McDonnell, S.; Davis, M. Deficit Discourse and Indigenous Health; Lowitja Institute: Melbourne, VIC, Australia, 2018; Available online: https://www.lowitja.org.au/page/services/resources/Cultural-and-social-determinants/racism/Deficit-Discourse-and-Indigenous-Health (accessed on 15 October 2023).
- Menzies, K. Understanding the Australian Aboriginal experience of collective, historical and intergenerational trauma. Int. Soc. Work 2019, 62, 1522–1534. [Google Scholar] [CrossRef]
- Paradies, Y. Colonisation, racism and indigenous health. J. Popul. Res. 2016, 33, 83–96. [Google Scholar] [CrossRef]
- National Aboriginal Community Controlled Health Organisations (ACCHOs). 2022. Available online: https://www.naccho.org.au/acchos/ (accessed on 15 October 2023).
- Panaretto, K.S.; Wenitong, M.; Button, S.; Ring, I.T. Aboriginal community controlled health services: Leading the way in primary care. Med. J. Aust. 2014, 200, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Percival, N.; O’Donoghue, L.; Lin, V.; Tsey, K.; Bailie, R.S. Improving Health Promotion Using Quality Improvement Techniques in Australian Indigenous Primary Health Care. Front. Public Health 2016, 4, 53. [Google Scholar] [CrossRef] [PubMed]
- Bryant, J.; Noble, N.; Freund, M.; Rumbel, J.; Eades, S.; Sanson-Fisher, R.; Lowe, M.; Walsh, J.; Piterman, L.; Koch, S.; et al. How can dementia diagnosis and care for Aboriginal and Torres Strait Islander people be improved? Perspectives of healthcare providers providing care in Aboriginal community controlled health services. BMC Health Serv. Res. 2021, 21, 699. [Google Scholar] [CrossRef]
- Godbee, K.; Gunn, J.; Lautenschlager, N.T.; Curran, E.; Palmer, V.J. Implementing dementia risk reduction in primary care: A preliminary conceptual model based on a scoping review of practitioners’ views. Prim. Health Care Res. Dev. 2019, 20, e140. [Google Scholar] [CrossRef]
- Baum, F.; MacDougall, C.; Smith, D. Participatory action research. J. Epidemiol. Community Health 2006, 60, 854–857. [Google Scholar] [CrossRef]
- Lowitja Institute. National CQI Framework for Aboriginal and Torres Strait Islander Primary Health Care 2015–2025; Lowitja Institute: Melbourne, VIC, Australia, 2015; Available online: https://www.naccho.org.au/continual-quality-improvement-cqi/ (accessed on 15 October 2023).
- Drawson, A.S.; Toombs, E.; Mushquash, C.J. Indigenous Research Methods: A Systematic Review. Int. Indig. Policy J. 2017, 8. [Google Scholar] [CrossRef]
- Dudgeon, P.; Bray, A.; Darlaston-Jones, D.; Walker, R. Aboriginal Participatory Action Research: An Indigenous Research Methodology Strengthening Decolonisation and Social and Emotional Wellbeing, Discussion Paper; The Lowitja Institute: Melbourne, VIC, Australia, 2020; Available online: https://www.lowitja.org.au/page/services/resources/Cultural-and-social-determinants/mental-health/aboriginal-participatory-action-research-an-indigenous-research-methodology-strengthening-decolonisation-and-social-and-emotional-wellbeing (accessed on 15 October 2023).
- Bessarab, D.; Ng’andu, B. Yarning About Yarning as a Legitimate Method in Indigenous Research. Int. J. Crit. Indig. Stud. 2010, 3, 37–50. [Google Scholar] [CrossRef]
- Smith, R.L.; Devine, S.; Preston, R. Recommended methodologies to determine Australian Indigenous community members’ perceptions of their health needs: A literature review. Aust. J. Prim. Health 2020, 26, 95–103. [Google Scholar] [CrossRef]
- Sollecito, W.; Johnson, J. McLaughlin and Kaluzny’s Continuous Quality Improvement in Health Care; Jones & Bartlett Publishers: Burlington, MA, USA, 2011. [Google Scholar]
- National Aboriginal Community Controlled Health Organisation. National Framework for Continuous Quality Improvement in Primary Health Care for Aboriginal and Torres Strait Islander People 2018–2023; National Aboriginal Community Controlled Health Organisation: Canberra, Australia, 2018; Available online: https://www.naccho.org.au/publications-resources/ (accessed on 15 October 2023).
- Bailie, R.; Bailie, J.; Larkins, S.; Broughton, E. Editorial: Continuous Quality Improvement (CQI)—Advancing Understanding of Design, Application, Impact, and Evaluation of CQI Approaches. Front. Public Health 2017, 5, 306. [Google Scholar] [CrossRef]
- Sibthorpe, B.; Gardner, K.; Chan, M.; Dowden, M.; Sargent, G.; McAullay, D. Impacts of continuous quality improvement in Aboriginal and Torres Strait islander primary health care in Australia. J. Health Organ Manag. 2018, 32, 545–571. [Google Scholar] [CrossRef]
- Taylor, M.J.; McNicholas, C.; Nicolay, C.; Darzi, A.; Bell, D.; Reed, J.E. Systematic review of the application of the plan-do-study-act method to improve quality in healthcare. BMJ Qual. Saf. 2014, 23, 290–298. [Google Scholar] [CrossRef] [PubMed]
- LoGiudice, D.; Smith, K.; Thomas, J.; Lautenschlager, N.T.; Almeida, O.P.; Atkinson, D.; Flicker, L. Kimberley Indigenous Cognitive Assessment tool (KICA): Development of a cognitive assessment tool for older indigenous Australians. Int. Psychogeriatr. 2006, 18, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.; Gilchrist, L.; Taylor, K.; Clinch, C.; Logiudice, D.; Edgill, P.; Ratcliffe, J.; Flicker, L.; Douglas, H.; Bradley, K.; et al. Good Spirit, Good Life: A Quality of Life Tool and Framework for Older Aboriginal Peoples. Gerontologist 2021, 61, e163–e172. [Google Scholar] [CrossRef]
- Harfield, S.; Pearson, O.; Morey, K.; Kite, E.; Canuto, K.; Glover, K.; Gomersall, J.S.; Carter, D.; Davy, C.; Aromataris, E.; et al. Assessing the quality of health research from an Indigenous perspective: The Aboriginal and Torres Strait Islander quality appraisal tool. BMC Med. Res. Methodol. 2020, 20, 79. [Google Scholar] [CrossRef] [PubMed]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health 2015, 42, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Thematic Analysis: Apractical Guide; Sage Publications: London, UK, 2021. [Google Scholar]
- Bailie, C.; Matthews, V.; Bailie, J.; Burgess, P.; Copley, K.; Kennedy, C.; Moore, L.; Larkins, S.; Thompson, S.; Bailie, R.S. Determinants and Gaps in Preventive Care Delivery for Indigenous Australians: A Cross-sectional Analysis. Front. Public Health 2016, 4, 34. [Google Scholar] [CrossRef]
- Bailie, J.; Matthews, V.; Laycock, A.; Schultz, R.; Burgess, C.P.; Peiris, D.; Larkins, S.; Bailie, R. Improving preventive health care in Aboriginal and Torres Strait Islander primary care settings. Glob. Health 2017, 13, 48. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Menzies School of Health Research. One21seventy; Health Centre and Community Survey (HCCS), Menzies School of Health Research: Darwin, Australia, 2014; Available online: https://www.menzies.edu.au/page/Resources/Health_Centre_and_Community_Survey_HCCS/ (accessed on 15 October 2023).
- Belfrage, M.; Hughson, J.; Douglas, H.; LoGiudice, D. Best-Practice Guide to Cognitive Impairment and Dementia Care for Aboriginal and Torres Strait Islander People Attending Primary Care, Version 1.1; University of Melbourne: Melbourne, Australia, 2020; Available online: https://www.racgp.org.au/clinical-resources/clinical-guidelines/guidelines-by-topic/accepted-clinical-guidelines/best-practice-guide-to-cognitive-impairment (accessed on 15 October 2023).
- National Aboriginal Community Controlled Health Organisation (NACCHO); The Royal Australian College of General Practitioners (RACGP). National Guide to a Preventive Health Assessment for Aboriginal and Torres Strait Islander People, 3rd ed.; RACGP: East Melbourne, VIC, Australia, 2018. Available online: https://www.racgp.org.au/clinical-resources/clinical-guidelines/key-racgp-guidelines/view-all-racgp-guidelines/national-guide (accessed on 15 October 2023).
- Slattery, P.; Saeri, A.K.; Bragge, P. Research co-design in health: A rapid overview of reviews. Health Res. Policy Syst. 2020, 18, 17. [Google Scholar] [CrossRef]
- Agency for Clinical Innovation. Co-Design Toolkit: Working as Equals in Leadership, Design and Decision Making; Agency for Clinical Innovation: St Leonards, NSW, Australia, 2023. Available online: https://aci.health.nsw.gov.au/projects/co-design (accessed on 15 October 2023).
- RE-AIM. Improving Public Health Relevance and Population Health Impact. Available online: https://re-aim.org/ (accessed on 19 May 2022).
- Australian Institute of Aboriginal and Torres Strait Islander Studies (AIATSIS). AIATSIS Code of Ethics for Aboriginal and Torres Strait Islander Research; AIATSIS: Canberra, Australia, 2020. Available online: https://aiatsis.gov.au/research/ethical-research/code-ethics (accessed on 15 October 2023).
- National Health and Medical Research Council. Management of Data and Information in Research: A Guide Supporting the Australian Code for the Responsible Conduct of Research; National Health and Medical Research Council: Canberra, Australia, 2019. Available online: https://www.nhmrc.gov.au/about-us/publications/australian-code-responsible-conduct-research-2018 (accessed on 15 October 2023).
- Australian Institute of Health and Welfare. Cardiovascular Disease, Diabetes and Chronic Kidney Disease—Australian Facts: Aboriginal and Torres Strait Islander People 2015; AIHW: Canberra, Australia, 2015. Available online: https://www.aihw.gov.au/reports/heart-stroke-vascular-diseases/cardiovascular-diabetes-chronic-kidney-risk-factor/summary (accessed on 15 October 2023).
- Bailie, R.; Si, D.; Connors, C.; Weeramanthri, T.; Clark, L.; Dowden, M.; O’Donohue, L.; Condon, J.; Thompson, S.; Clelland, N. Study protocol: Audit and best practice for chronic disease extension (ABCDE) project. BMC Health Serv. Res. 2008, 8, 184. [Google Scholar] [CrossRef] [PubMed]
- Howard, K.; White, S.; Salkeld, G.; McDonald, S.; Craig, J.C.; Chadban, S.; Cass, A. Cost-Effectiveness of Screening and Optimal Management for Diabetes, Hypertension, and Chronic Kidney Disease: A Modeled Analysis. Value Health 2010, 13, 196–208. [Google Scholar] [CrossRef] [PubMed]
- Peiris, D.; Wright, L.; News, M.; Corcoran, K. Community-Based Chronic Disease Prevention and Management for Aboriginal People in New South Wales, Australia: Mixed Methods Evaluation of the 1 Deadly Step Program. JMIR Mhealth Uhealth 2019, 7, e14259. [Google Scholar] [CrossRef] [PubMed]
- Bradley, K.; Smith, R.; Hughson, J.A.; Atkinson, D.; Bessarab, D.; Flicker, L.; Radford, K.; Smith, K.; Strivens, E.; Thompson, S.; et al. Let’s CHAT (community health approaches to) dementia in Aboriginal and Torres Strait Islander communities: Protocol for a stepped wedge cluster randomised controlled trial. BMC Health Serv. Res. 2020, 20, 208. [Google Scholar] [CrossRef]
- Mateo-Arriero, I.; Lalovic, A.; Dowden, G.; Markey, L.; Cox, K.L.; Flicker, L.; Bessarab, D.; Thompson, S.; Kickett, C.; Woods, D.; et al. Co-design of dementia prevention program for Aboriginal Australians (DAMPAA). Alzheimer’s Dement. 2023, 19, 4564–4571. [Google Scholar] [CrossRef]
- Coalition of Peaks and The Australian Government. National Agreement on Closing the Gap; Department of the Prime Minister and Cabinet: Barton, ACT, Australia, 2020. Available online: https://www.coalitionofpeaks.org.au/national-agreement-on-closing-the-gap (accessed on 15 October 2023).
- Department of Health. National Aboriginal and Torres Strait Islander Health Plan 2021–2031; Commonwealth of Australia: Canberra, Australia, 2021; Publications Number: DT0002195. Available online: https://www.health.gov.au/resources/publications/national-aboriginal-and-torres-strait-islander-health-plan-2021-2031?language=en (accessed on 15 October 2023).



{kind=link}
{kind=link}
| 1. Basic demographic information. 2. Health service utilisation. 3. Conditions, diagnoses, and family health history. 4. Medication (current) polypharmacy and medication review. 5. Clinical measurements, investigations, intervention, treatment, management, and monitoring. | 6. Hearing and vision screening, intervention, and monitoring. 7. Mental health, emotional and social well-being screening, intervention, treatment, management, and monitoring. 8. Cognitive function screening, assessment, treatment, management, and monitoring. 9. Support services assessment and utilisation. |
| Evaluation Parameters | Evaluation Measures | Evaluation Data Source |
|---|---|---|
| Reach | The number, proportion, and representation of
|
|
| Effectiveness | Impact of CQI activities toward achieving project outcomes:
|
|
| Adoption |
|
|
| Implementation |
|
|
| Maintenance |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hornby-Turner, Y.C.; Russell, S.G.; Quigley, R.; Matthews, V.; Larkins, S.; Hayman, N.; Lakhan, P.; Flicker, L.; Smith, K.; McKeown, D.; et al. Safeguarding against Dementia in Aboriginal and Torres Strait Islander Communities through the Optimisation of Primary Health Care: A Project Protocol. Methods Protoc. 2023, 6, 103. https://doi.org/10.3390/mps6050103
Hornby-Turner YC, Russell SG, Quigley R, Matthews V, Larkins S, Hayman N, Lakhan P, Flicker L, Smith K, McKeown D, et al. Safeguarding against Dementia in Aboriginal and Torres Strait Islander Communities through the Optimisation of Primary Health Care: A Project Protocol. Methods and Protocols. 2023; 6(5):103. https://doi.org/10.3390/mps6050103
Chicago/Turabian StyleHornby-Turner, Yvonne C., Sarah G. Russell, Rachel Quigley, Veronica Matthews, Sarah Larkins, Noel Hayman, Prabha Lakhan, Leon Flicker, Kate Smith, Dallas McKeown, and et al. 2023. "Safeguarding against Dementia in Aboriginal and Torres Strait Islander Communities through the Optimisation of Primary Health Care: A Project Protocol" Methods and Protocols 6, no. 5: 103. https://doi.org/10.3390/mps6050103