
Anti-Inflammatory Diet for Women with Interstitial Cystitis/Bladder Pain Syndrome: The AID-IC Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Development of AID-IC Therapeutic and Control Diets
2.1.1. AID-IC Therapeutic Diet
2.1.2. Control Diet
2.2. Recruitment and Screening
2.3. Intervention
2.4. Data Collection
2.4.1. Health and Dietary Information
2.4.2. Disease Activity
2.4.3. Palatability and Acceptability of AID-IC Therapeutic Diet
2.4.4. Participant Experience
2.5. Data Analysis
3. Results
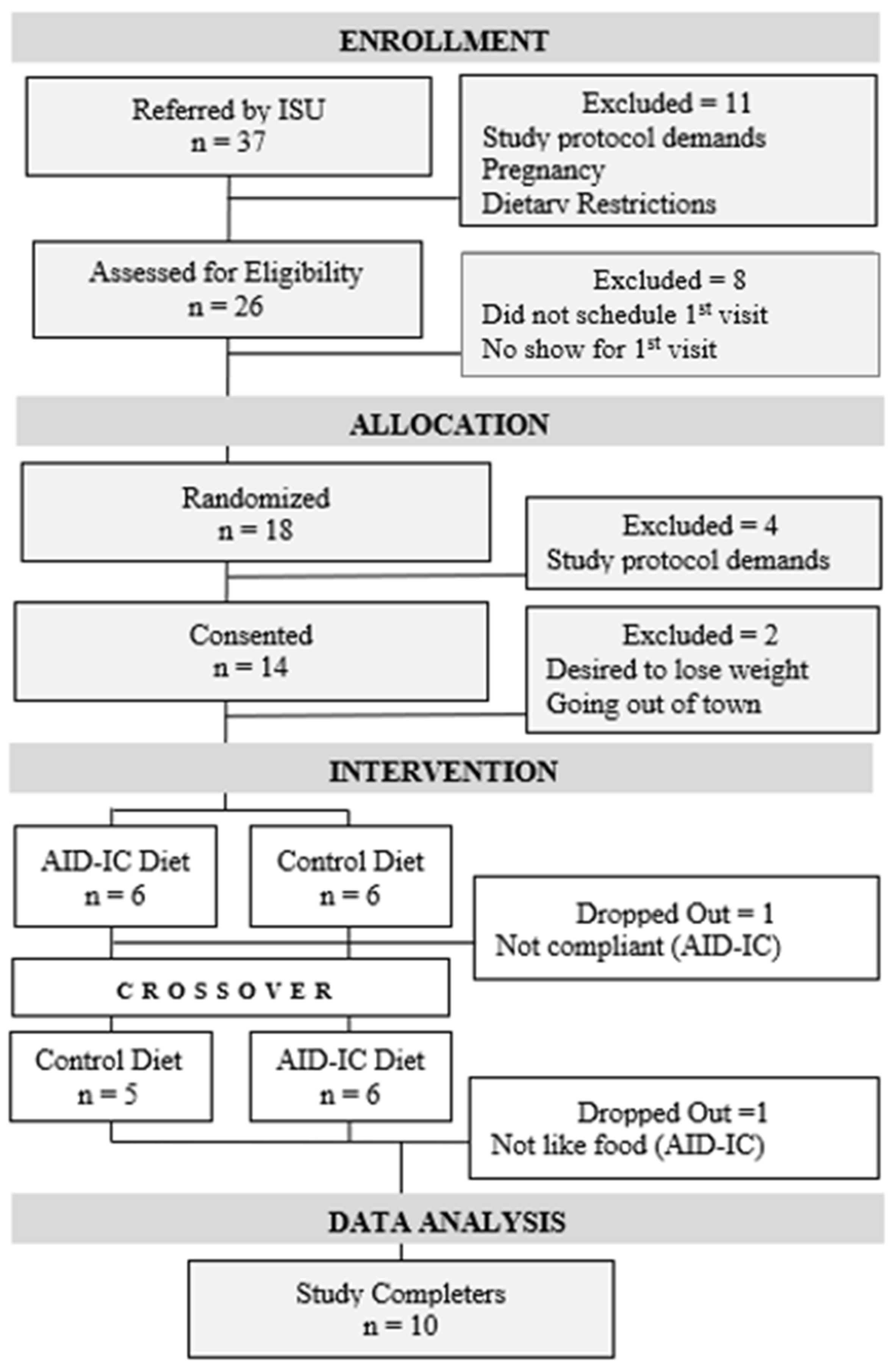
3.1. Participant Flow and Demographics
3.2. Nutrient Composition Therapeutic vs. Control Diets
3.3. Impact of Diet on Disease Activity
3.4. Patient Experience
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Berry, S.H.; Elliott, M.N.; Suttorp, M.; Bogart, L.M.; Stoto, M.A.; Eggers, P.; Nyberg, L.; Clemens, J.Q. Prevalence of symptoms of bladder pain syndrome/interstitial cystitis among adult females in the United States. J. Urol. 2011, 186, 540–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahnama’I, M.S.; Javan, A.; Vyas, N.; Lovasz, S.; Singh, N.; Cervigni, M.; Pandey, S.; Wyndaele, J.J.; Taneja, R. Bladder pain syndrome and interstitial cystitis beyond horizon: Reports from the Global Interstitial Cystitis/Bladder Pain Society (GIBS) meeting 2019. Anesthesiol. Pain Med. 2020, 10, e101848. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Miki, M.; Yamada, T. Interstitial cystitis in Japan. Br. J. Urol. 2001, 86, 634–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bade, J.J.; Rijcken, B.; Mensink, H.J. Interstitial cystitis in The Netherlands: Prevalence, diagnostic criteria and therapeutic preferences. J. Urol. 1995, 154, 2035–2037. [Google Scholar] [CrossRef]
- Suskind, A.M.; Berry, S.H.; Ewing, B.A.; Elliott, M.N.; Suttorp, M.J.; Clemens, J.Q. The prevalence and overlap of interstitial cystitis/bladder pain syndrome and chronic prostatitis/chronic pelvic pain syndrome in men: Results of the RAND Interstitial Cystitis Epidemiology male study. J. Urol. 2013, 189, 141–145. [Google Scholar] [CrossRef] [Green Version]
- Hanno, P.M.; Burks, D.A.; Clemens, J.Q.; Dmochowski, R.R.; Erickson, D.; Fitzgerald, M.P.; Forrest, J.B.; Gordon, B.; Gray, M.; Mayer, R.D.; et al. AUA guideline for the diagnosis and treatment of interstitial cystitis/bladder pain syndrome. J. Urol. 2011, 185, 2162–2170. [Google Scholar] [CrossRef]
- McKernan, L.C.; Walsh, C.G.; Reynolds, W.S.; Crofford, L.J.; Dmochowski, R.R.; Williams, D.A. Psychosocial comorbidities in interstitial cystitis/bladder pain syndrome (IC/BPS): A systematic review. Neurourol. Urodyn. 2018, 37, 926–941. [Google Scholar] [CrossRef]
- Sutcliffe, S.; Bradley, C.S.; Clemens, J.Q.; James, A.S. Urologic chronic pelvic pain syndrome flares and their impact: Qualitative analysis in the MAPP Network. Int. Urogynecol. J. 2015, 26, 1047–1060. [Google Scholar] [CrossRef] [Green Version]
- Akiyama, Y. Biomarkers in interstitial cystitis/bladder pain syndrome with and without Hunner lesion: A review and future perspectives. Diagnostics 2021, 11, 2238. [Google Scholar] [CrossRef]
- Jiang, Y.H.; Peng, C.H.; Liu, H.T.; Kuo, H.C. Increased pro-inflammatory cytokines, C-reactive protein and nerve growth factor expressions in serum of patients with interstitial cystitis/bladder pain syndrome. PLoS ONE 2013, 8, e76779. [Google Scholar] [CrossRef]
- Chung, S.D.; Liu, H.T.; Lin, H.; Kuo, H.C. Elevation of serum c-reactive protein in patients with OAB and IC/BPS implies chronic inflammation in the urinary bladder. Neurourol. Urodyn. 2011, 30, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.H.; Jhang, J.F.; Hsu, Y.H.; Ho, H.C.; Wu, Y.H.; Kuo, H.C. Urine cytokines as biomarkers for diagnosing interstitial cystitis/bladder pain syndrome and mapping its clinical characteristics. Am. J. Physiol. Physiol. 2020, 318, F1391–F1399. [Google Scholar] [CrossRef] [PubMed]
- Koziol, J.A.; Clark, D.C.; Gittes, R.F.; Tan, E. The natural history of interstitial cystitis: A survey of 374 patients. J. Urol. 1993, 149, 465–469. [Google Scholar] [CrossRef]
- Interstitial Cystitis Association. Available online: www.ichelp.org/icdietsurvey (accessed on 31 December 2014).
- Warren, J.W.; Brown, J.; Tracy, J.K.; Langenberg, P.; Wesselmann, U.; Greenberg, P. Evidence based criteria for the pain of interstitial cystitis/painful bladder syndrome in women. Urology 2008, 71, 444–448. [Google Scholar] [CrossRef] [Green Version]
- Bassaly, R.; Downes, K.; Hart, S. Dietary consumption triggers in interstitial cystitis/bladder pain syndrome patients. Female Pelvic Med. Reconstr. Surg. 2011, 17, 36–39. [Google Scholar] [CrossRef]
- O’Hare, P.G., 3rd; Hoffmann, A.R.; Allen, P.; Gordon, B.; Salin, L.; Whitmore, K. Interstitial cystitis patients’ use and rating of complementary and alternative medicine therapies. Int. Urogynecol. J. 2013, 24, 977–982. [Google Scholar] [CrossRef]
- Shorter, B.; Ackerman, M.; Varvara, M.; Moldwin, R.M. Statistical validation of the Shorter-Moldwin Food Sensitivity Questionnaire for patients with interstitial cystitis/bladder pain syndrome. J. Urol. 2014, 191, 1793–1801. [Google Scholar] [CrossRef]
- ACOG Committee on Practice Bulletins—Gynecology. ACOG Practice Bulletin No. 51. Chronic pelvic pain. Obstet. Gynecol. 2004, 103, 589–605. [Google Scholar] [CrossRef]
- Haefner, H.K.; Collins, M.E.; Davis, G.D.; Edwards, L.; Foster, D.C.; Hartmann ED, H.; Kaufman, R.H.; Lynch, P.J.; Margesson, L.J.; Moyal-Barracco, M.; et al. The vulvodynia guideline. J. Low. Genit. Tract Dis. 2005, 9, 40–51. [Google Scholar] [CrossRef]
- Hanno, P.M.; Erickson, D.; Moldwin, R.; Faraday, M.M. Diagnosis and treatment of interstitial cystitis/bladder pain syndrome: AUA guideline amendment. J. Urol. 2015, 193, 1545–1553. [Google Scholar] [CrossRef]
- Homma, Y.; Ueda, T.; Tomoe, H.; Interstitial cystitis guideline committee. Japanese Urological Association. Clinical guidelines for interstitial cystitis and hypersensitive bladder syndrome. Int. J. Urol. 2009, 16, 597–615. [Google Scholar] [CrossRef] [PubMed]
- Estaban, M.; Adot, J.M.; Arlandis, S.; Working Group for Recommendations of the Diagnosis and Management of Bladder Pain Syndrome. Recommendations for the diagnosis and management of bladder pain syndrome: Spanish urological association consensus document. Actas Urol. Esp. 2013, 39, 365–472. [Google Scholar] [CrossRef]
- Parsons, C.L. The role of the urinary epithelium in the pathogenesis of interstitial cystitis/prostatitis/urethritis. Urology 2007, 69, 9–16. [Google Scholar] [CrossRef]
- Tillisch, K. The effects of gut microbiota on CNS function in humans. Gut Microbes 2014, 5, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Nazif, O.; Teichman, J.M.; Gebhart, G.F. Neural upregulation in interstitial cystitis. Urology 2007, 69, 24–33. [Google Scholar] [CrossRef] [PubMed]
- Elliott, R.A.; Kapoor, S.; Tincello, D.G. Expression and distribution of the sweet taste receptor isoforms T1R2 and T1R3 in human and rat bladders. J. Urol. 2011, 186, 2455–2462. [Google Scholar] [CrossRef] [Green Version]
- Manzel, A.; Muller, D.N.; Hafler, D.A.; Erdman, S.E.; Linker, R.A.; Kleinewietfeld, M. Role of “Western diet” in inflammatory autoimmune diseases. Curr. Allergy Asthma Rep. 2014, 14, 404. [Google Scholar] [CrossRef] [Green Version]
- Shivappa, N.; Steck, S.; Hurley, T.; Hussey, J.; Hébert, J. Designing and developing a literature-derived, population-based dietary inflammatory index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef] [Green Version]
- Tamma, S.M.; Shorter, B.; Toh, K.-L.; Moldwin, R.; Gordon, B. Influence of polyunsaturated fatty acids on urologic inflammation. Int. Urol. Nephrol. 2015, 47, 1753–1761. [Google Scholar] [CrossRef]
- Liu, F.H.; Liu, C.; Gong, T.T.; Gao, S.; Sun, H.; Jiang, Y.T.; Zhang, J.Y.; Zhang, M.; Gao, C.; Li, X.Y.; et al. Dietary Inflammatory Index and Health Outcomes: An Umbrella Review of Systematic Review and Meta-Analyses of Observational Studies. Front. Nutr. 2021, 8, 647122. [Google Scholar] [CrossRef]
- Hébert, J.R.; Shivappa, N.; Wirth, M.D.; Hussey, J.R.; Hurley, T.G. Perspective: The Dietary Inflammatory Index (DII)-Lessons Learned, Improvements Made, and Future Directions. Adv. Nutr. 2019, 10, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Qi, M.-Y.; Liu, S.; Song, X.-T.; Zhang, J.-N.; Zhai, Y.-F.; Lu, M.-H.; Han, H.-B.; Lian, Z.-X.; Yao, Y.-C. TLR4 overexpression enhances saturated fatty acid-induced inflammatory cytokine gene expression in sheep. Eur. J. Inflamm. 2018, 16, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Milanski, M.; Degasperi, G.; Coopoe, A. Saturated fatty acids produce an inflammatory response predominantly through the activation of TLR4 signaling in hypothalamus: Implications for the pathogenesis of obesity. J. Neurosci. 2009, 29, 359–370. [Google Scholar] [CrossRef]
- Lancaster, G.I.; Langley, K.G.; Berglund, N.A.; Kammoun, H.L.; Reibe, S.; Estevez, E.; Weir, J.; Mellett, N.A.; Pernes, G.; Conway, J.R.W.; et al. Evidence that TLR4 Is not a receptor for saturated fatty acids but mediates lipid-induced inflammation by reprogramming macrophage metabolism. Cell Metab. 2018, 27, 1096–1110.e5. [Google Scholar] [CrossRef] [Green Version]
- Oberbach, A.; Schlichting, N.; Heinrich, M.; Till, H.; Stolzenburg, J.-U.; Neuhaus, J. Free fatty acid palmitate impairs vitality and function of cultured human bladder smooth muscle cells. PLoS ONE 2012, 7, e41026. [Google Scholar] [CrossRef] [Green Version]
- Maserejian, N.N.; Giovannucci, E.L.; McVary, K.T.; McGrother, C.; McKinlay, J.B. Dietary macronutrient and energy intake and urinary incontinence in women. Am. J. Epidemiol. 2010, 171, 1116–1125. [Google Scholar] [CrossRef]
- Winkvist, A.; Bärebring, L.; Gjertsson, I.; Ellegård, L.; Lindqvist, H.M. A randomized controlled cross-over trial investigating the effect of anti-inflammatory diet on disease activity and quality of life in rheumatoid arthritis: The Anti-inflammatory Diet In Rheumatoid Arthritis (ADIRA) study protocol. Nutr. J. 2018, 17, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clemens, J.Q.; Calhoun, E.A.; Litwin, M.S.; McNaughton-Collins, M.; Kusek, J.W.; Crowley, E.M.; Landis, J.R.; Urologic Pelvic Pain Collaborative Research Network. Validation of a modified National Institutes of Health chronic prostatitis symptom index to assess genitourinary pain in both men and women. Urology 2009, 74, 983–987. [Google Scholar] [CrossRef] [Green Version]
- Rosen, R.; Brown, C.; Heiman, J.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R., Jr. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex Marital Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef]
- Bogart, L.M.; Suttopr, M.J.; Elliott, M.N.; Clemens, J.Q.; Berry, S.H. Validation of a quality-of-life scale for women with bladder pain syndrome/interstitial cystitis. Qual. Life Res. 2012, 21, 1665–1670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genoni, A.; Lo, J.; Lyons-Wall, P.; Devine, A. Compliance, palatability and feasibility of paleolithic and Australian guide to healthy eating diets in healthy women: A 4-week dietary intervention. Nutrients 2016, 8, 481. [Google Scholar] [CrossRef] [PubMed]
- Hanley, R.S.; Stoffel, J.T.; Zagha, R.M.; Mourtzinos, A.; Bresette, J.F. Multimodal therapy for painful bladder syndrome/interstitial cystitis: Pilot study combining behavioral, pharmacologic, and endoscopic therapies. Int. Braz. J. Urol. 2009, 35, 467–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herati, A.; Shorter, B.; Sadek, M.; Levey, H.; Okhunov, Z.; Moldwin, R. The effects of caffeine on the symptoms of interstitial cystitis/painful bladder syndrome: A randomized, placebo-controlled double blind study. J. Urol. 2011, 185, e325. [Google Scholar] [CrossRef]
- Oh-oka, H. Clinical efficacy of 1-year intensive systematic dietary manipulation as complementary and alternative medicine therapies on female patients with interstitial cystitis/bladder pain syndrome. Urology 2017, 106, 50–54. [Google Scholar] [CrossRef]
- Lebowitz, B.D.; Vitiello, B.; Norquist, G.S. Approaches to multisite clinical trials: The National Institute of Mental Health perspective. Schizophr. Bull. 2003, 29, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Constable, L.; Pirie, D.; Gillies, K.; McCann, S.; Breeman, S.; Glazener, C. The importance of rapport and relationship building when recruiting to clinical trials: A qualitative investigation of trial recruitment consultations in a surgical RCT. Trials 2015, 16, O37. [Google Scholar] [CrossRef]
- Robison, L.; Cho, Y.; Viecelli, A.K.; Johnson, D.W.; Hawley, C.M.; Valks, A.; Paul-Brent, P.A.; Stastny, R.; Varghese, J.; Kiriwandeniya, C.; et al. Australasian Kidney Trials Network. Conducting clinical trials during the COVID-19 pandemic—A collaborative trial network response. Trials 2021, 22, 278. [Google Scholar] [CrossRef] [PubMed]
- Clemson University. Available online: https://hgic.clemson.edu/factsheet/planning-meals-for-a-family (accessed on 1 October 2021).
- Armstrong, S.; Arsenault, M.; Betwick, S. Menu Planning in Long Term Care and Canada’s Food Guide; Dietitians of Canada: Toronto, ON, Canada, 2019; p. 37. [Google Scholar]
- van der Sman, R.G.M. Impact of Processing Factors on Quality of Frozen Vegetables and Fruits. Food Eng. Rev. 2020, 12, 399–420. [Google Scholar] [CrossRef]
- Aydinlar, E.I.; Dikmen, P.Y.; Tiftikci, A.; Saruc, M.; Aksu, M.; Gunsoy, H.G.; Tozun, N. IgG-based elimination diet in migraine plus irritable bowel syndrome. Headache 2013, 53, 514–525. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Enrollment | Allocation | Intervention | |||||
|---|---|---|---|---|---|---|---|
| Time Point | Pre-Intervention | Start 1st 10 Weeks | End 1st 10 Weeks | Wash Out 2 Weeks | Start 2nd 10 Weeks | End 2nd 10 Weeks | |
| ENROLLMENT | |||||||
| Eligibility screen | X | ||||||
| Randomization | X | ||||||
| Information consent | X | ||||||
| INTERVENTION | |||||||
| AID IC then Control | X | X | X | X | |||
| Control then AID IC | X | X | X | X | |||
| ASSESSMENTS | |||||||
| ASA24 | X | X | X | X | |||
| Kilocalorie requirements | X | X | |||||
| Primary outcomes (quality of life) * | |||||||
| GUPI | X | X | X | X | |||
| FSFI | X | X | X | X | |||
| RICE | X | X | X | X | |||
| Secondary outcomes (inflammatory markers, acceptability of therapeutic diet) | |||||||
| Tumor Necrosis Factor-alpha ** | X | X | X | X | |||
| Interleukin-1 ** | X | X | X | X | |||
| C-reactive protein ** | X | X | X | X | |||
| Palatability survey | 5 weeks (AID-IC) | 5 weeks (AID-IC) | |||||
| Dietary Inflammation Index | X | ||||||
| Focus group findings | X | ||||||
| Demographics, Comorbid Conditions, Trigger Foods | No. | % |
|---|---|---|
| Race/Ethnicity | ||
| White/Non-Hispanic | 10 | 100 |
| Age Range | ||
| 25 to 34 years | 1 | 10 |
| 35 to 44 years | 1 | 10 |
| 45 to 54 years | 4 | 40 |
| 55 to 64 years | 1 | 10 |
| 64 to 75 years | 3 | 30 |
| Annual Income | ||
| Prefer not to answer | 1 | 10 |
| USD 35,000 to USD 49,999 | 1 | 10 |
| USD 50,000 to USD 74,499 | 3 | 30 |
| USD 75,000 to USD 99,999 | 1 | 10 |
| Over USD 100,000 | 4 | 40 |
| Comorbid Conditions | ||
| Overweight/obesity | 8 | 80 |
| Hypertension | 2 | 30 |
| Other chronic pain condition | 7 | 70 |
| Trigger Foods | ||
| Tomatoes/tomato products | 6 | 60 |
| Alcohol | 5 | 50 |
| Spicy Foods | 5 | 50 |
| Citrus Food | 3 | 3 |
| Coffee | 3 | 3 |
| Pre-Control Diet | Post-Control Diet | p Value | Pre-Test Diet | Post-Test Diet | p Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Std. Dev. | Mean | Std. Dev. | Mean | Std. Dev. | Mean | Std. Dev. | |||
| E-DII Score * | −0.63 | 1.44 | −1.35 | 1.63 | 0.21 | −1.61 | 1.53 | −1.38 | 1.89 | 0.05 |
| Energy (kcalories) | 1796.29 | 809.06 | 1757.80 | 639.76 | 0.91 | 1736.31 | 675.05 | 1578.08 | 715.07 | 0.62 |
| Protein (g) | 78.14 | 30.10 | 79.59 | 19.08 | 0.90 | 79.31 | 26.38 | 83.29 | 41.95 | 0.80 |
| Total Fat (g) | 0.55 | 0.80 | 0.34 | 0.54 | 0.49 | 0.55 | 1.02 | 0.39 | 0.72 | 0.70 |
| MUFA (g) ** | 22.28 | 11.08 | 23.36 | 10.75 | 0.83 | 23.36 | 16.40 | 21.27 | 10.04 | 0.74 |
| PUFA (g) ** | 27.22 | 14.84 | 27.23 | 11.32 | 0.99 | 28.46 | 11.70 | 26.52 | 20.57 | 0.80 |
| Solid Fats (g) | 26.90 | 18.41 | 25.33 | 16.37 | 0.84 | 26.89 | 25.46 | 22.33 | 16.94 | 0.64 |
| Saturated Fats (g) | 258.28 | 93.90 | 290.57 | 114.74 | 0.50 | 253.89 | 115.93 | 256.55 | 78.89 | 0.10 |
| Cholesterol (mg) | 184.28 | 60.90 | 245.18 | 223.21 | 0.42 | 295.95 | 127.58 | 264.75 | 206.40 | 0.69 |
| Carbohydrates (g) | 206.13 | 106.54 | 196.56 | 89.89 | 0.83 | 191.77 | 87.05 | 168.72 | 84.36 | 0.56 |
| Fiber (g) | 22.55 | 8.43 | 18.11 | 7.09 | 0.22 | 21.46 | 4.46 | 20.30 | 7.19 | 0.67 |
| Refined Grains (oz) | 3.25 | 2.45 | 3.87 | 2.38 | 0.57 | 2.05 | 1.86 | 2.38 | 2.28 | 0.73 |
| Beta-carotene (mcg) | 7457.66 | 9168.47 | 4761.02 | 4634.70 | 0.66 | 3411.50 | 2044.78 | 5446.77 | 3281.86 | 0.40 |
| Alpha carotene (mcg) | 979.49 | 1021.02 | 678.60 | 1033.62 | 0.45 | 444.87 | 587.42 | 461.78 | 876.36 | 0.11 |
| Beta-cryptoxanthin (mcg) | 115.63 | 68.72 | 65.02 | 58.28 | 0.42 | 112.90 | 111.79 | 53.64 | 51.05 | 0.96 |
| Thiamin (mg) | 1.21 | 0.45 | 1.28 | 0.50 | 0.52 | 1.22 | 0.44 | 1.25 | 0.59 | 0.88 |
| Riboflavin (mg) | 1.59 | 0.62 | 1.68 | 0.53 | 0.09 | 1.92 | 0.84 | 1.96 | 0.95 | 0.91 |
| Niacin (mg) | 21.08 | 8.73 | 20.24 | 4.92 | 0.74 | 22.02 | 7.95 | 20.86 | 15.21 | 0.83 |
| Vitamin B6 (mg) | 1.82 | 0.49 | 1.73 | 0.60 | 0.72 | 2.21 | 0.36 | 2.02 | 0.89 | 0.54 |
| Vitamin B12 (mcg) | 3.61 | 1.74 | 3.95 | 2.12 | 0.80 | 4.55 | 1.96 | 5.20 | 2.95 | 0.57 |
| Vitamin C (mg) | 85.82 | 41.42 | 64.33 | 35.36 | 0.70 | 113.83 | 59.07 | 60.69 | 31.67 | 0.02 |
| Vitamin D (mg) | 19.30 | 7.44 | 18.99 | 10.03 | 0.70 | 19.19 | 5.69 | 13.99 | 6.28 | 0.07 |
| Vitamin E (mg) | 0.77 | 1.33 | 0.04 | 0.14 | 0.23 | 0.21 | 0.65 | 0.00 | 0.00 | 0.33 |
| Folic acid (mcg) | 335.80 | 73.28 | 361.63 | 130.46 | 0.94 | 388.88 | 115.09 | 420.02 | 227.52 | 0.70 |
| Iron (mg) | 10.78 | 3.42 | 13.76 | 4.47 | 0.10 | 11.24 | 3.87 | 14.59 | 9.27 | 0.31 |
| Magnesium (mg) | 315.78 | 121.63 | 298.49 | 113.52 | 0.60 | 333.82 | 86.85 | 316.31 | 171.70 | 0.78 |
| Selenium (mcg) | 110.57 | 35.83 | 107.77 | 29.56 | 0.11 | 108.10 | 44.64 | 120.05 | 90.48 | 0.71 |
| Zinc (mg) | 9.44 | 3.62 | 11.98 | 4.44 | 0.75 | 11.12 | 4.40 | 10.69 | 6.79 | 0.87 |
| Timepoint | N * | Mean | Std. Dev. | p-Value | |
|---|---|---|---|---|---|
| Therapeutic Diet | RICE ** | 9 | 11.33 | 8.22 | 0.05 |
| GUPI, ** Pain | 9 | 18.33 | 2.30 | 0.31 | |
| GUPI, Urinary symptoms | 9 | 3.83 | 2.70 | 0.09 | |
| GUPI, Quality of life | 9 | 7.33 | 2.64 | 0.28 | |
| GUPI, total | 9 | 7.33 | 2.64 | 0.28 | |
| FSFI ** | 9 | 3.11 | 2.06 | 0.40 | |
| Control Diet | RICE | 9 | 12.56 | 6.18 | 0.06 |
| GUPI, Pain | 9 | 19.17 | 1.60 | 0.40 | |
| GUPI, Urinary symptoms | 9 | 4.33 | 2.63 | 0.23 | |
| GUPI, Quality of life | 9 | 8.61 | 3.12 | 0.23 | |
| GUPI, total | 9 | 8.61 | 3.12 | 0.23 | |
| FSFI | 9 | 1.44 | 1.87 | 0.26 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gordon, B.; Blanton, C.; Ramsey, R.; Jeffery, A.; Richey, L.; Hulse, R. Anti-Inflammatory Diet for Women with Interstitial Cystitis/Bladder Pain Syndrome: The AID-IC Pilot Study. Methods Protoc. 2022, 5, 40. https://doi.org/10.3390/mps5030040
Gordon B, Blanton C, Ramsey R, Jeffery A, Richey L, Hulse R. Anti-Inflammatory Diet for Women with Interstitial Cystitis/Bladder Pain Syndrome: The AID-IC Pilot Study. Methods and Protocols. 2022; 5(3):40. https://doi.org/10.3390/mps5030040
Chicago/Turabian StyleGordon, Barbara, Cynthia Blanton, Rebekah Ramsey, Andrea Jeffery, Laura Richey, and Rachel Hulse. 2022. "Anti-Inflammatory Diet for Women with Interstitial Cystitis/Bladder Pain Syndrome: The AID-IC Pilot Study" Methods and Protocols 5, no. 3: 40. https://doi.org/10.3390/mps5030040