Older African American Men’s Perspectives on Factors That Influence Type 2 Diabetes Self-Management and Peer-Led Interventions


Abstract
:1. Introduction
1.1. Barriers to T2D Illness Management among Older Black Men
1.2. Interventions to Improve Older Black Men’s T2D Management
2. Methods
2.1. Study Design
2.2. Participant Characteristics
2.3. Participant Recruitment and Data Collection
- “When you were growing up, what did you learn about being a man from the men in your community?”
- “How has what you learned about being a man from men in your community impacted your decisions about your health?”
- “In your opinion, what kinds of things do you think a community health worker could do in your community to support men trying to manage their diabetes?”
- “What sorts of things would you rather a community health worker not do?”
2.4. Data Management and Analysis
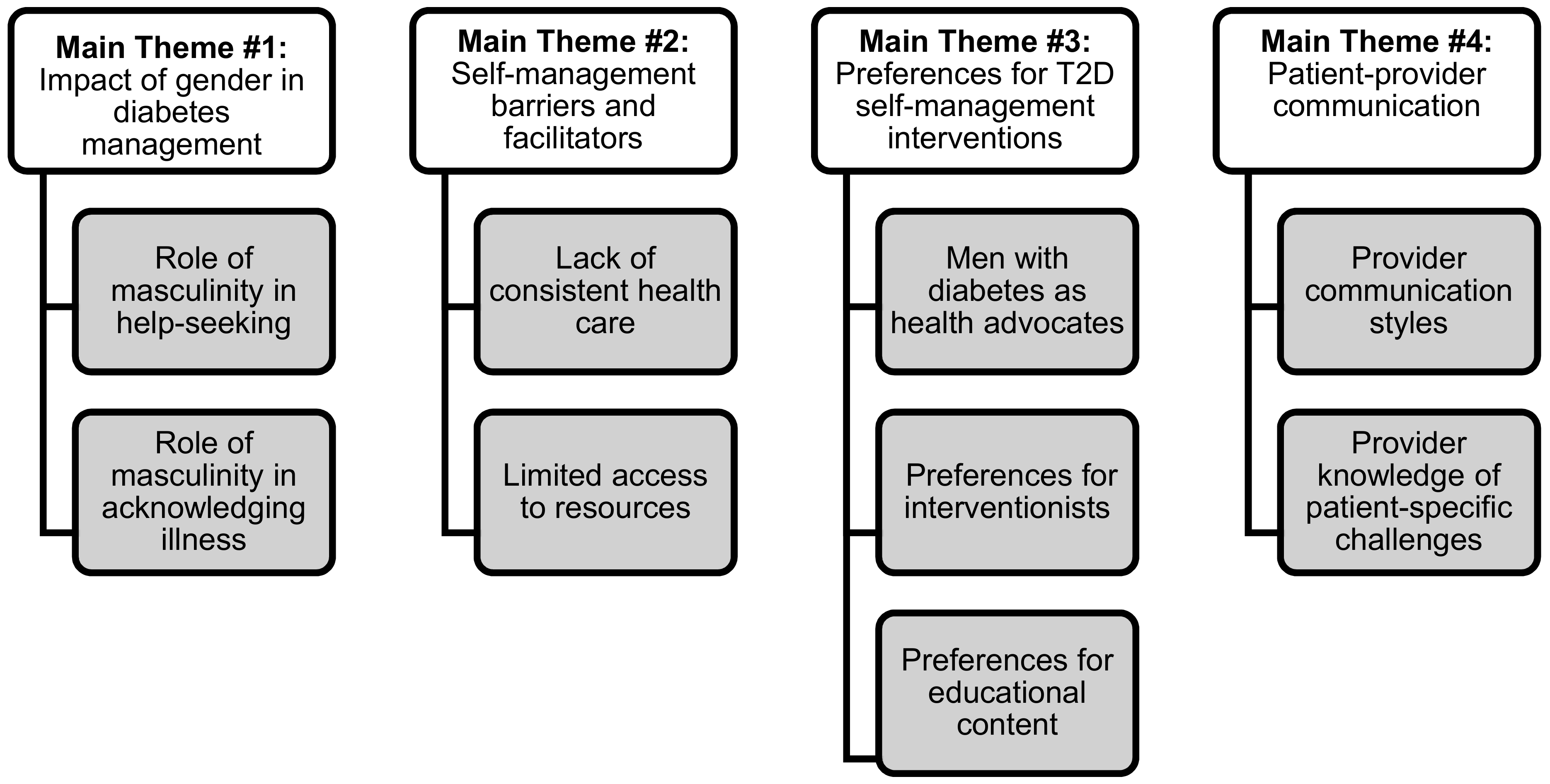
3. Results
“When I found out I had cancer I got pretty scared and I ran for two years… without treatment. I went and had a biopsy … and he told me I had cancer. It was extremely aggressive and … I wasn’t playing superman, I was just scared. And I was scared to tell anybody that I was scared. Men ain’t scared, we’re superman and batman. I’ll beat up your Rottweiler.”
“The assumption is that all I got to do is tell this gentlemen that ‘oh, you need a glucose meter,’ … but now what we forget [is] that people are living to eat whatever food they can really afford. Now, it may or may not be the appropriate food for a diabetic … we need to know what financial conditions … they have.” Yet another participant reflected on his experiences with accessing consistent care, stating, “and every time I went to the doctor, it was so frustrating. Every time I went to that clinic I had a different doctor.” Other in-depth qualitative studies have documented that consistency in interacting with the same health provider is both perceived as a hallmark of patient-centered care and is reported to be an important motivator for medically underserved patients to adhere to preventive and other treatment recommendations for managing their conditions [31].
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in the United States; US Department of Health and Human Services: Atlanta, GA, USA, 2017. [Google Scholar]
- Egede, L.E.; Mueller, M.; Echols, C.L.; Gebregziabher, M. Longitudinal differences in glycemic control by race/ethnicity among veterans with type 2 diabetes. Med. Care 2010, 48, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Liburd, L.C.; Namageyo-Funa, A.; Jack, L., Jr. Understanding “masculinity” and the challenges of managing type-2 diabetes among African-American men. J. Natl. Med. Assoc. 2007, 99, 550–552, 554–558. [Google Scholar] [PubMed]
- Griffith, D.M.; Metzl, J.M.; Gunter, K. Considering intersections of race and gender in interventions that address US men’s health disparities. Public Health 2011, 125, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.; Watkins, D.C.; Kieffer, E.; Spencer, M.; Piatt, G.; Nicklett, E.J.; Lebron, A.; Espitia, N.; Palmisano, G. An Exploratory Study of the Impact of Gender on Health Behavior among African American and Latino Men with Type 2 Diabetes. Am. J. Men’s Health 2017. [Google Scholar] [CrossRef] [PubMed]
- Cornish, E.K.; McKissic, S.A.; Dean, D.A.; Griffith, D.M. Lessons learned about motivation from a pilot physical activity intervention for African American men. Health Promot. Pract. 2017, 18, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.M.; Cornish, E.K.; McKissic, S.A.; Dean, D.A. Differences in Perceptions of the Food Environment Between African American Men Who Did and Did Not Consume Recommended Levels of Fruits and Vegetables. Health Educ. Behav. 2016, 43, 648–655. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.M.; Thorpe, R.J. Men’s physical health and health behaviors. In APA Handbook of Men and Masculinities; Wong, J.Y., Wester, S.R., Eds.; American Psychological Association: Washington, DC, USA, 2016; pp. 709–730. [Google Scholar]
- Courtenay, W.H. Constructions of masculinity and their influence on men’s well-being: A theory of gender and health. Soc. Sci. Med. 2000, 50, 1385–1401. [Google Scholar] [CrossRef]
- Seawell, A.H.; Hurt, T.R.; Shirley, M.C. The influence of stress, gender, and culture on Type 2 diabetes prevention and management among Black men: A qualitative analysis. Am. J. Men’s Health 2016, 10, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.; Kieffer, E.C.; Sinco, B.; Anderson, M. Psychosocial factors that influence health care use and self-management for African American and Latino men with type 2 diabetes: An exploratory study. J. Men’s Stud. 2015, 23, 161–176. [Google Scholar] [CrossRef]
- Plowden, K.O.; Young, A.E. Sociostructural factors influencing health behaviors of urban African-American men. J. Natl. Black Nurses Assoc. 2003, 14, 45–51. [Google Scholar] [PubMed]
- Harvey, I.S.; Alston, R.J. Understanding preventive behaviors among mid-Western African-American men: A pilot qualitative study of prostate screening. J. Men’s Health 2011, 8, 140–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherman, L.D.; Hawkins, J.M.; Bonner, T. An Analysis of the Recruitment and Participation of African American Men in Type 2 Diabetes Self-Management Research: A Review of the Published Literature. Soc. Work Public Health 2017, 32, 38–48. [Google Scholar] [CrossRef] [PubMed]
- Norris, S.L.; Engelgau, M.M.; Narayan, K.V. Effectiveness of self-management training in type 2 diabetes. Diabetes Care 2001, 24, 561–587. [Google Scholar] [CrossRef] [PubMed]
- Spencer, M.S.; Rosland, A.M.; Kieffer, E.C.; Sinco, B.R.; Valerio, M.; Palmisano, G.; Anderson, M.; Guzman, J.R.; Heisler, M. Effectiveness of a community health worker intervention among African American and Latino adults with type 2 diabetes: A randomized controlled trial. Am. J. Public Health 2011, 101, 2253–2260. [Google Scholar] [CrossRef] [PubMed]
- Crabtree, K.; Sherrer, N.; Rushton, T.; Willig, A.; Agne, A.; Shelton, T.; Cherrington, A. Diabetes connect: African American men’s preferences for a community-based diabetes management program. Diabetes Educator 2015, 41, 118–126. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.; Kieffer, E.C.; Sinco, B.; Spencer, M.; Anderson, M.; Rosland, A. Does gender influence participation? Predictors of participation in a community health worker diabetes management intervention with African American and Latino adults. Diabetes Educator 2013, 39, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Hurt, T.R.; Seawell, A.H.; O’Connor, M.C. Developing effective diabetes programming for Black men. Glob. Qual. Nurs. Res. 2015, 2. [Google Scholar] [CrossRef] [PubMed]
- Maulsby, C.; Millett, G.; Lindsey, K.; Kelley, R.; Johnson, K.; Montoya, D.; Holtgrave, D. A systematic review of HIV interventions for black men who have sex with men (MSM). BMC Public Health 2013, 13, 625. [Google Scholar] [CrossRef] [PubMed]
- Balls-Berry, J.; Watson, C.; Kadimpati, S.; Crockett, A.; Mohamed, E.A.; Brown, I.; Davis, O.I. Black men’s perceptions and knowledge of diabetes: A church-affiliated barbershop focus group study. J. Racial Ethn. Dispar. 2015, 2, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Davis, O. (Re) framing Health Literacy: Transforming the Culture of Health in the Black Barbershop. West. J. Black Stud. 2011, 35, 176–186. [Google Scholar]
- Smith, J.A.; Osborn, M. Interpretative phenomenological analysis. In Qualitative Psychology: A Practical Guide to Research Methods; Smith, J.A., Ed.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2003; pp. 51–80. [Google Scholar]
- Michigan Center for Urban African American Aging. Participant Resource Pool. Available online: https://mcuaaar.wayne.edu/ (accessed on 26 June 2018).
- Krueger, R.A.; Casey, M.A. Designing and conducting focus group interviews. In Social Analysis, Selected Tools and Techniques; Krueger, R.A., Casey, M.A., Donner, J., Kirsch, S., Maack, J.N., Eds.; Social Development Publications: Washington, DC, USA, 2002; pp. 4–23. [Google Scholar]
- Watkins, D.C. Qualitative research: The importance of conducting research that doesn’t “count”. Health Promot. Pract. 2012, 13, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Watkins, D.C.; Gioia, D. Mixed Methods Research: Pocket Guides to Social Work Research Methods Series; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Ali, N.; Bamidele, O.; Gurch, R.; Hoskin, P.; McCaughan, E. Constructions of Masculinity and Help-Seeking for Prostate Cancer. Divers. Equal. Health Care 2017, 14, 254–256. [Google Scholar]
- Mackenzie, S. Reframing masculinity: Structural vulnerability and HIV among black men who have sex with men and women. Cult. Health Sex. 2018, 19, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.M.; Gilbert, K.L.; Bruce, M.A.; Thorpe, R.J. Masculinity in Men’s Health: Barrier or Portal to Healthcare? In Men’s Health in Primary Care; Humana Press: Cham, Switzerland, 2016; pp. 19–31. [Google Scholar]
- Raja, S.; Hasnain, M.; Vadakumchery, T.; Hamad, J.; Shah, R.; Hoersch, M. Identifying elements of patient-centered care in underserved populations: A qualitative study of patient perspectives. PLoS ONE 2015, 10, e0126708. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.M.; Mitchell, J. The Doctor Never Listens: Older African American Men’s Perceptions of Patient–Provider Communication. Soc. Work Res. 2018, 42, 57–63. [Google Scholar] [CrossRef]


{kind=link}
| African American Men(n = 12) | |
|---|---|
| Education | |
| High School Diploma | 1 |
| Some College or More | 11 |
| Employment | |
| Employed | 0 |
| Not Employed/Retired | 12 |
| Marital Status | |
| Not Married | 1 |
| Married | 8 |
| Divorced/Widowed | 3 |
| Average Age | 75 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hawkins, J.; Mitchell, J.; Piatt, G.; Ellis, D. Older African American Men’s Perspectives on Factors That Influence Type 2 Diabetes Self-Management and Peer-Led Interventions. Geriatrics 2018, 3, 38. https://doi.org/10.3390/geriatrics3030038
Hawkins J, Mitchell J, Piatt G, Ellis D. Older African American Men’s Perspectives on Factors That Influence Type 2 Diabetes Self-Management and Peer-Led Interventions. Geriatrics. 2018; 3(3):38. https://doi.org/10.3390/geriatrics3030038
Chicago/Turabian StyleHawkins, Jaclynn, Jamie Mitchell, Gretchen Piatt, and Deborah Ellis. 2018. "Older African American Men’s Perspectives on Factors That Influence Type 2 Diabetes Self-Management and Peer-Led Interventions" Geriatrics 3, no. 3: 38. https://doi.org/10.3390/geriatrics3030038
APA StyleHawkins, J., Mitchell, J., Piatt, G., & Ellis, D. (2018). Older African American Men’s Perspectives on Factors That Influence Type 2 Diabetes Self-Management and Peer-Led Interventions. Geriatrics, 3(3), 38. https://doi.org/10.3390/geriatrics3030038