
Deep Learning Method for Precise Landmark Identification and Structural Assessment of Whole-Spine Radiographs
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials
2.1. Dataset
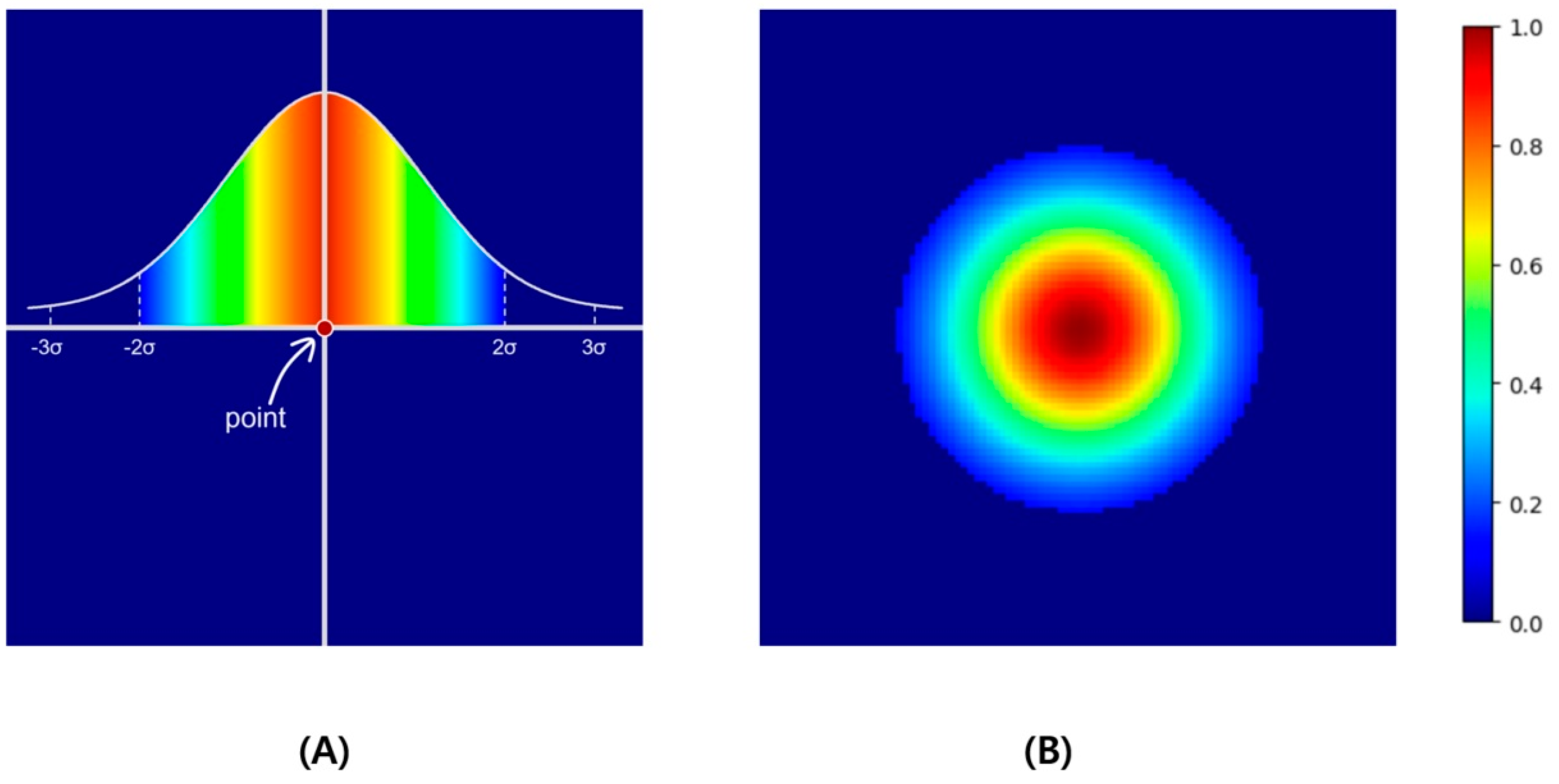
2.2. Learning of Heatmap-Based Landmark Detection
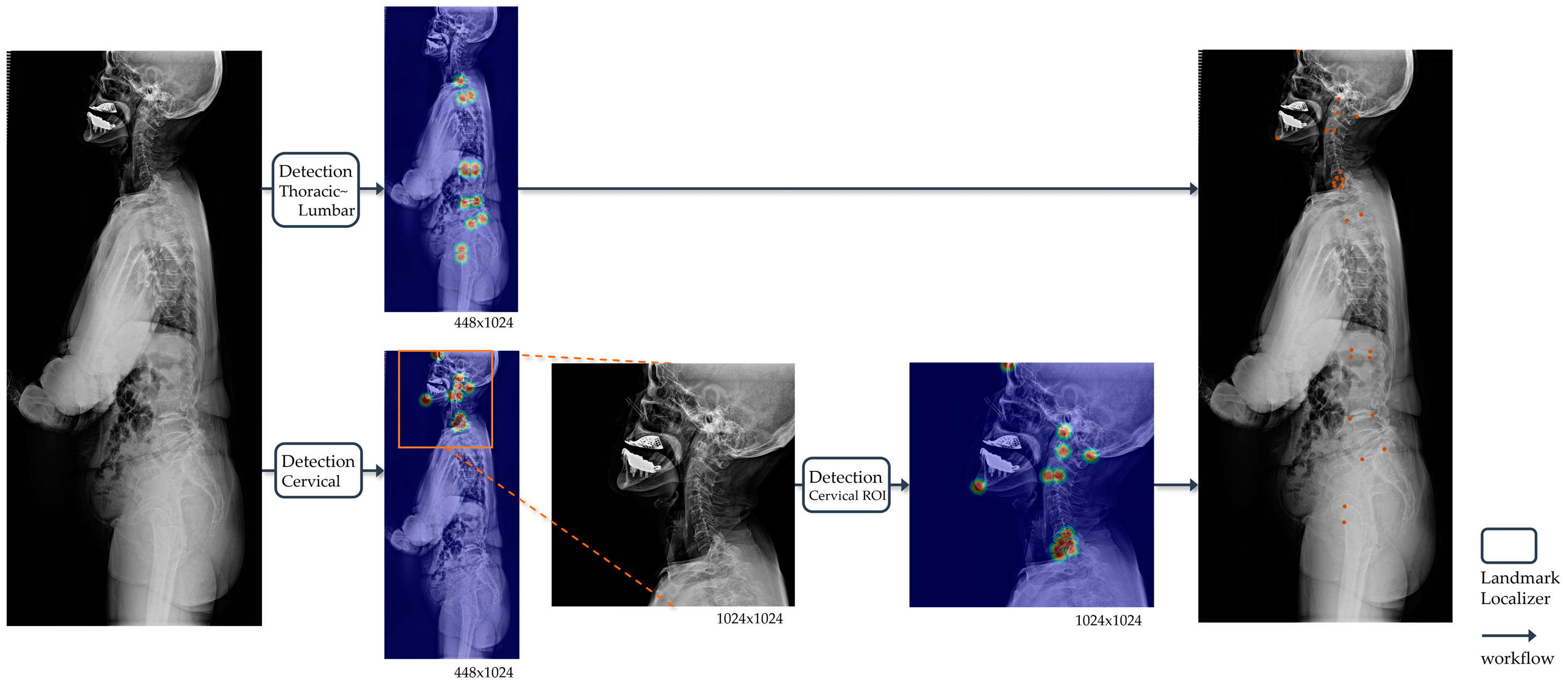
2.3. Workflow of the Landmark Detection in Whole-Spine Lateral Radiographs
2.4. Training Details
2.5. Measurement of Spinal Parameters
2.6. Statistical Analysis
3. Results
3.1. Dataset Demographic
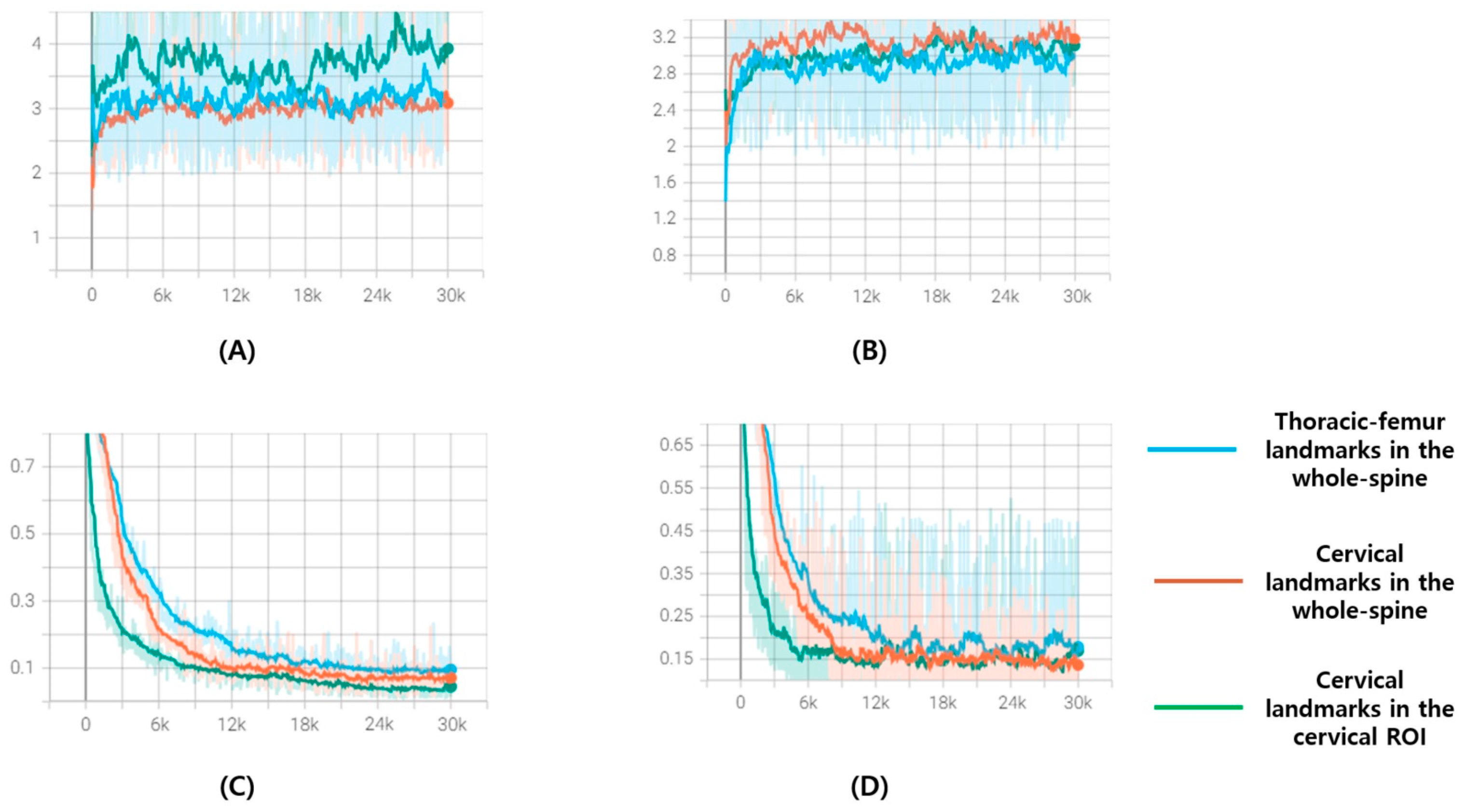
3.2. Performance of the Landmark Localizer
3.3. Inter-Rater Reliability between the Two Human Experts and Developed Deep Learning Model
3.4. Performance Evaluation of the Spinal Parameters of the Deep Learning Model
3.5. Predicted Spinal Parameters of the External Validation Dataset
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Le Huec, J.C.; Charosky, S.; Barrey, C.; Rigal, J.; Aunoble, S. Sagittal imbalance cascade for simple degenerative spine and consequences: Algorithm of decision for appropriate treatment. Eur. Spine J. 2011, 20 (Suppl. S5), 699–703. [Google Scholar] [CrossRef] [PubMed]
- Carman, D.L.; Browne, R.H.; Birch, J.G. Measurement of scoliosis and kyphosis radiographs. Intraobserver and interobserver variation. J. Bone Jt. Surg. Am. 1990, 72, 328–333. [Google Scholar] [CrossRef]
- Summers, R.M. Deep learning and computer-aided diagnosis for medical image processing: A personal perspective. In Deep Learning and Convolutional Neural Networks for Medical Image Computing; Lu, L., Zheng, Y., Carneiro, G., Yang, L., Eds.; Springer International Publishing AG: Cham, Switzerland, 2017; pp. 3–10. [Google Scholar] [CrossRef]
- Sun, H.; Zhen, X.; Bailey, C.; Rasoulinejad, P.; Yin, Y.; Li, S. Direct Estimation of Spinal Cobb Angles by Structured Multi-Output Regression; Springer International Publishing: Cham, Switzerland, 2017; pp. 529–540. [Google Scholar] [CrossRef]
- Wu, H.; Bailey, C.; Rasoulinejad, P.; Li, S. Automated comprehensive adolescent idiopathic scoliosis assessment using MVC-Net. Med. Image Anal. 2018, 48, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.; De Silva, T.; Ketcha, M.D.; Vijayan, R.; Doerr, S.; Uneri, A.; Vedula, S.; Theodore, N.; Siewerdsen, J.H. Automatic vertebrae localization in spine CT: A deep-learning approach for image guidance and surgical data science. In Proceedings of the SPIE 10951, Medical Imaging 2019: Image-Guided Procedures, Robotic Interventions, and Modeling, 109510S (8 March 2019), San Diego, CA, USA, 17–19 February 2019. [Google Scholar] [CrossRef]
- Jakobsen, I.M.G.; Plocharski, M. Automatic detection of cervical vertebral landmarks for fluoroscopic joint motion analysis. In Image Analysis. SCIA 2019. Lecture Notes in Computer Science; Felsberg, M., Forssén, P.E., Sintorn, I.M., Unger, J., Eds.; Springer: Cham, Switzerland, 2019; Volume 11482, pp. 209–220. [Google Scholar] [CrossRef]
- Isensee, F.; Petersen, J.; Klein, A.; Zimmerer, D.; Jaeger, P.F.; Kohl, S.; Wasserthal, J.; Koehler, G.; Norajitra, T.; Wirkert, S.; et al. Abstract: nnU-Net: Self-adapting framework for U-Net-based medical image segmentation. In Bildverarbeitung für die Medizin; Springer Fachmedien Wiesbaden: Wiesbaden, Germany, 2019; Volume 22. [Google Scholar] [CrossRef]
- Alejandro, N.; Yang, K.; Deng, J. Stacked hourglass networks for human pose estimation. In Proceedings of the Computer Vision–ECCV 2016: 14th European Conference, Amsterdam, The Netherlands, 11–14 October 2016; Proceedings Part VIII 14. Springer International Publishing: Cham, Switzerland, 2016. [Google Scholar]
- Kumar, H.; Marks, T.K.; Mou, W.; Wang, Y.; Jones, M.; Cherian, A.; Koike-Akino, T.; Liu, X.; Feng, C. Luvli face alignment: Estimating landmarks’ location, uncertainty, and visibility likelihood. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Seattle, WA, USA, 13–19 June 2020. [Google Scholar]
- Zhang, Z.; Chai, K.; Yu, H.; Majaj, R.; Walsh, F.; Wang, E.; Mahbub, U.; Siegelmann, H.; Kim, D.; Rahman, T. Neuromorphic high-frequency 3D dancing pose estimation in dynamic environment. Neurocomputing 2023, 547, 126388. [Google Scholar] [CrossRef]
- Kebaish, K.M.; Neubauer, P.R.; Voros, G.D.; Khoshnevisan, M.A.; Skolasky, R.L. Scoliosis in adults aged forty years and older: Prevalence and relationship to age, race, and gender. Spine 2011, 36, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Noh, S.H.; Lee, H.S.; Park, G.E.; Ha, Y.; Park, J.Y.; Kuh, S.U.; Chin, D.K.; Kim, K.S.; Cho, Y.E.; Kim, S.H.; et al. Predicting mechanical complications after adult spinal deformity operation using a machine learning based on modified global alignment and proportion scoring with body mass index and bone mineral density. Neurospine 2023, 20, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Noh, S.H.; Ha, Y.; Park, J.Y.; Kuh, S.U.; Chin, D.K.; Kim, K.S.; Cho, Y.E.; Lee, H.S.; Kim, K.H. Modified global alignment and proportion scoring with body mass index and bone mineral density analysis in global alignment and proportion score of each 3 categories for predicting mechanical complications after adult spinal deformity surgery. Neurospine 2021, 18, 484–491. [Google Scholar] [CrossRef] [PubMed]
- Diebo, B.G.; Shah, N.V.; Boachie-Adjei, O.; Zhu, F.; Rothenfluh, D.A.; Paulino, C.B.; Schwab, F.J.; Lafage, V. Adult spinal deformity. Lancet 2019, 394, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Le Huec, J.C.; Thompson, W.; Mohsinaly, Y.; Barrey, C.; Faundez, A. Sagittal balance of the spine. Eur. Spine J. 2019, 28, 1889–1905. [Google Scholar] [CrossRef] [PubMed]
- Barrey, C.; Jund, J.; Noseda, O.; Roussouly, P. Sagittal balance of the pelvis-spine complex and lumbar degenerative diseases. A comparative study about 85 cases. Eur. Spine J. 2007, 16, 1459–1467. [Google Scholar] [CrossRef] [PubMed]
- Weng, C.H.; Wang, C.L.; Huang, Y.J.; Yeh, Y.C.; Fu, C.J.; Yeh, C.Y.; Tsai, T.T. Artificial intelligence for automatic measurement of sagittal vertical axis using ResUNet framework. J. Clin. Med. 2019, 8, 1826. [Google Scholar] [CrossRef] [PubMed]
- Galbusera, F.; Niemeyer, F.; Wilke, H.J.; Bassani, T.; Casaroli, G.; Anania, C.; Costa, F.; Brayda-Bruno, M.; Sconfienza, L.M. Fully automated radiological analysis of spinal disorders and deformities: A deep learning approach. Eur. Spine J. 2019, 28, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Yeh, Y.C.; Weng, C.H.; Huang, Y.J.; Fu, C.J.; Tsai, T.T.; Yeh, C.Y. Deep learning approach for automatic landmark detection and alignment analysis in whole-spine lateral radiographs. Sci. Rep. 2021, 11, 7618. [Google Scholar] [CrossRef] [PubMed]
- Zhou, G.; Jiang, W.; Lai, K.; Zheng, Y. Automatic measurement of spine curvature on 3-D ultrasound volume projection image with phase features. IEEE Trans. Med Imaging 2017, 36, 1250–1262. [Google Scholar] [CrossRef]
- Bernstein, P.; Metzler, J.; Weinzierl, M.; Seifert, C.; Kisel, W.; Wacker, M. Radiographic scoliosis angle estimation: Spline-based measurement reveals superior reliability compared to traditional COBB method. Eur. Spine J. 2021, 30, 676–685. [Google Scholar] [CrossRef] [PubMed]
- Weng, C.H.; Huang, Y.J.; Fu, C.J.; Yeh, Y.C.; Yeh, C.Y.; Tsai, T.T. Automatic recognition of whole-spine sagittal alignment and curvature analysis through a deep learning technique. Eur. Spine J. 2022, 31, 2092–2103. [Google Scholar] [CrossRef] [PubMed]
- Roussouly, P.; Gollogly, S.; Berthonnaud, E.; Dimnet, J. Classification of the normal variation in the sagittal alignment of the human lumbar spine and pelvis in the standing position. Spine 2005, 30, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.; Wang, G.; Sun, J.; Lv, G. Correlations between the inflection point and spinal sagittal alignment in asymptomatic adults. Eur. Spine J. 2020, 29, 2272–2280. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
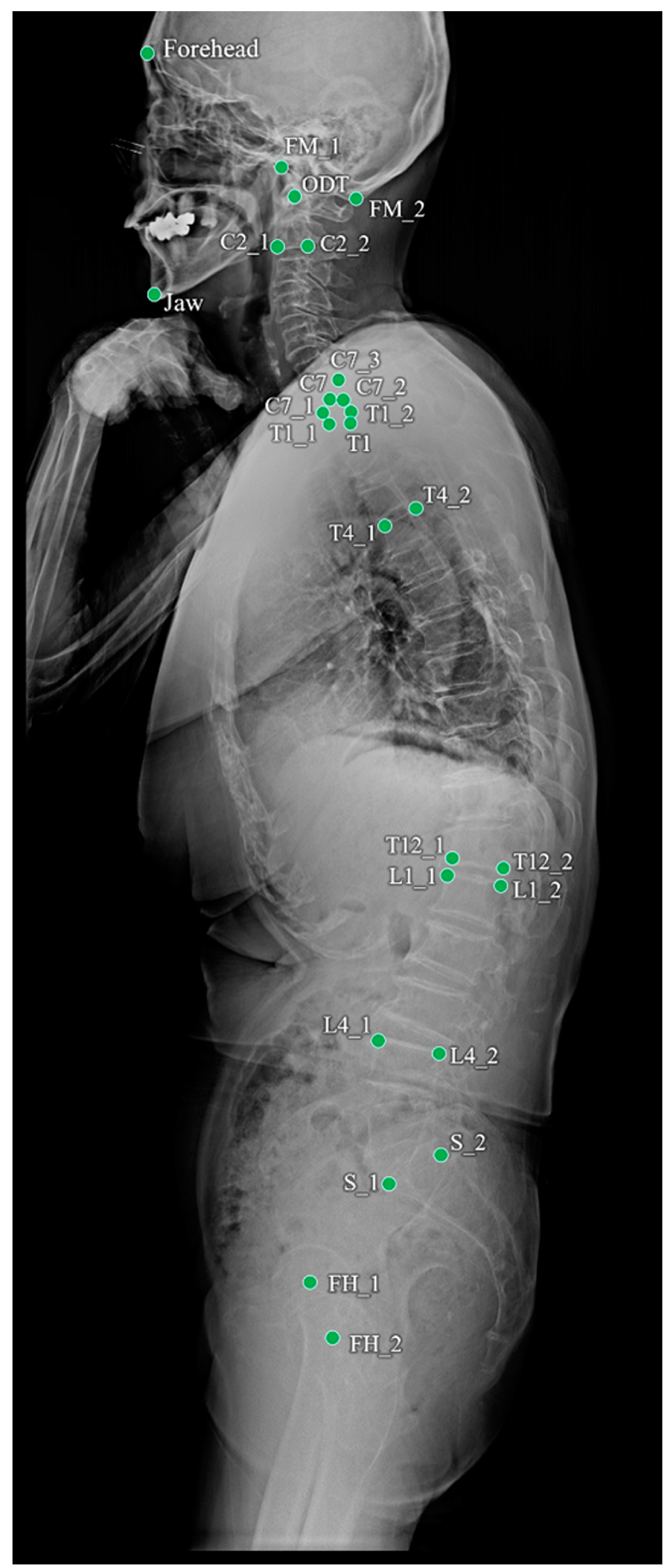
| Name | Description |
|---|---|
| FH_1 | Center of the Femur head |
| FH_2 | Center of the Femur head |
| S_1 | Anterior point of the upper endplate of the sacrum |
| S_2 | Posterior point of the upper endplate of the sacrum |
| L1_1 | Anterior point of the upper endplate of the L1 vertebra |
| L1_2 | Posterior point of the upper endplate of the L1 vertebra |
| L4_1 | Anterior point of the upper endplate of the L4 vertebra |
| L4_2 | Posterior point of the upper endplate of the L4 vertebra |
| T4_1 | Anterior point of the upper endplate of the T4 vertebra |
| T4_2 | Posterior point of the upper endplate of the T4 vertebra |
| T12_1 | Anterior point of the lower endplate of the T12 vertebra |
| T12_2 | Posterior point of the lower endplate of the T12 vertebra |
| T1 | Center of the T1 vertebral body |
| Forehead | Forehead |
| FM_1 | Anterior point of the foramen magnum |
| FM_2 | Posterior point of the foramen magnum |
| ODT | Odontoid |
| Jaw | Jaw |
| C2_1 | Anterior point of the lower endplate of the C2 vertebra |
| C2_2 | Posterior point of the lower endplate of the C2 vertebra |
| C7 | Center of the C7 vertebral body |
| C7_1 | Anterior point of the lower endplate of the C7 vertebra |
| C7_2 | Posterior point of the lower endplate of the C7 vertebra |
| C7_3 | Posterior point of the upper endplate of the C7 vertebra |
| T1_1 | Anterior point of the upper endplate of the T1 vertebra |
| T1_2 | Posterior point of the upper endplate of the T1 vertebra |
| Name | Measurement | |
|---|---|---|
| PI | Pelvic Incidence | The angle between the line connecting the center of femur heads and the center of the sacrum’s upper endplate, and the perpendicular line of the sacrum’s upper endplate. |
| PT | Pelvic Tilt | The angle between the line connecting the center of the femur heads and the center of the sacrum’s upper endplate, and the vertical. |
| SS | Sacral Slope | The angle between the sacrum’s upper endplate and the horizontal. |
| LL | Lumbar Lordosis | The angle between the upper endplate of L1 and the endplate of the sacrum. |
| L4S1 | L4S1 Lordosis | The angle between the upper endplate of L4 and the endplate of the sacrum. |
| TK | Thoracic Kyphosis | The angle between the upper endplate of T4 and the lower endplate of T12. |
| TPA | T1pelvic Angle | The angle between the line connecting the center of the T1 vertebral body and the center of the femur heads, and the line connecting the center of the femur heads and the center of the sacrum’s upper endplate. |
| CBVA | Chin-Brow Vertical Angle | The angle between the line connecting the forehead and chin, and the vertical. |
| C2C7 | C2C7 Angle (Cervical Lordosis Angle) | The angle between the lower endplate of C2 and the lower endplate of C7. |
| TS | T1 Slope | The angle between the upper endplate of T1 and the horizontal. |
| TS-CL | T1 Slope—Cervical Lordosis | T1 slope minus cervical lordosis. |
| ODHA | Odontoid hip axis angle | The angle between the line connecting the odontoid to the center of femur heads, and the vertical. |
| PI-LL | Pelvic Incidence—Lumbar Lordosis | Pelvic Incidence minus Lumbar Lordosis |
| SSA | Spino-Sacral Angle | The angle between the line connecting the center of the C7 body and the center of the sacrum’s upper endplate, and sacrum’s upper endplate. |
| SVA | Sagittal Vertical Axis | Distance between the vertical line at the center of the C7 body and a posterior point of the sacrum’s upper endplate. |
| Parameters | R1 versus R2 | DL versus R1 | DL versus R2 |
|---|---|---|---|
| PI (°) | 0.978 | 0.891 | 0.889 |
| PT (°) | 0.981 | 0.923 | 0.915 |
| SS (°) | 0.962 | 0.905 | 0.897 |
| LL (°) | 0.957 | 0.921 | 0.915 |
| L4S1 (°) | 0.961 | 0.901 | 0.894 |
| TK (°) | 0.979 | 0.945 | 0.931 |
| TPA (°) | 0.945 | 0.894 | 0.884 |
| CBVA (°) | 0.951 | 0.907 | 0.901 |
| C2C7 (°) | 0.947 | 0.887 | 0.881 |
| TS (°) | 0.923 | 0.915 | 0.909 |
| TS-CL (°) | 0.914 | 0.909 | 0.897 |
| ODHA (°) | 0.928 | 0.903 | 0.891 |
| PI-LL (°) | 0.927 | 0.896 | 0.884 |
| SSA (°) | 0.944 | 0.945 | 0.925 |
| SVA (mm) | 0.957 | 0.912 | 0.902 |
| Parameters | Ground Truth | Parameter Error | Correlation Analysis | Wilcoxon Signed-Rank Test | |
|---|---|---|---|---|---|
| R | p Value | p Value | |||
| PI (°) | 53.8 ± 18.8° | 2.6 ± 3.1° | 0.982 | <0.001 * | 0.497 |
| PT (°) | 14.8 ± 11.3° | 1.8 ± 2.2° | 0.917 | 0.512 | |
| SS (°) | 39.4 ± 7.9° | 2.2 ± 3.4° | 0.912 | 0.459 | |
| LL (°) | 41.2 ± 17.3° | 5.7 ± 3.5° | 0.991 | 0.279 | |
| L4S1 (°) | 30.7 ± 11.6° | 4.5 ± 2.8° | 0.857 | 0.247 | |
| TK (°) | 27.2 ± 11.2° | 5.5 ± 4.5° | 0.812 | 0.078 | |
| TPA (°) | 24.9 ± 23.2° | 1.8 ± 1.1° | 0.792 | 0.758 | |
| CBVA (°) | 1.8 ± 5.2° | 0.7 ± 0.6° | 0.984 | 0.678 | |
| C2C7 (°) | 13.6 ± 9.7° | 5.5 ± 6.5° | 0.845 | 0.598 | |
| TS (°) | 22.8 ± 10.2° | 5.7 ± 6.2° | 0.784 | 0.084 | |
| TS-CL (°) | 9.8 ± 2.4° | 4.1 ± 5.9° | 0.809 | 0.097 | |
| ODHA (°) | 4.3 ± 5.4° | 0.2 ± 0.2° | 0.978 | 0.594 | |
| PI-LL (°) | 12.1 ± 7.5° | 3.0 ± 4.5° | 0.962 | 0.596 | |
| SSA (°) | 120.1 ± 12.4° | 3.3 ± 2.5° | 0.927 | 0.492 | |
| SVA (mm) | 22.1 ± 19.2 mm | 3.0 ± 2.9 mm | 0.986 | 0.745 | |
| Parameters | Ground Truth | Parameter Error | External-Validation Dataset 1 Error | External-Validation Dataset 2 Error | External-Validation Dataset 3 Error | External-Validation Dataset 4 Error | p-Value |
|---|---|---|---|---|---|---|---|
| PI (°) | 53.8 ± 18.8° | 2.7 ± 3.1° | 3.3 ± 2.1° | 2.2 ± 3.9° | 4.2 ± 2.4° | 3.6 ± 2.1° | 0.479 |
| PT (°) | 14.8 ± 11.3° | 1.9 ± 2.2° | 2.7 ± 2.0° | 2.2 ± 2.7° | 2.5 ± 1.2° | 2.3 ± 1.3° | 0.545 |
| SS (°) | 39.4 ± 7.9° | 2.2 ± 3.4° | 2.3 ± 3.3° | 3.6 ± 2.2° | 3.8 ± 2.4° | 3.6 ± 3.0° | 0.471 |
| LL (°) | 41.2 ± 17.3° | 5.7 ± 3.5° | 5.1 ± 3.0° | 6.2 ± 4.4° | 5.6 ± 3.6° | 4.2 ± 3.3° | 0.784 |
| L4S1 (°) | 30.7 ± 11.6° | 4.5 ± 2.8° | 5.2 ± 2.5° | 4.2 ± 2.6° | 4.4 ± 3.1° | 5.0 ± 2.4° | 0.612 |
| TK (°) | 27.2 ± 11.2° | 5.5 ± 4.5° | 5.9 ± 4.4° | 5.9 ± 5.2° | 4.2 ± 3.8° | 5.0 ± 4.4° | 0.274 |
| TPA (°) | 24.9 ± 23.2° | 1.8 ± 1.1° | 1.4 ± 1.8° | 1.9 ± 1.7° | 1.9 ± 1.9° | 1.5 ± 1.1° | 0.798 |
| CBVA (°) | 1.8 ± 5.2° | 0.7 ± 0.6° | 0.6 ± 0.4° | 0.4 ± 0.2° | 0.8 ± 1.4° | 0.8 ± 1.0° | 0.571 |
| C2C7 (°) | 13.6 ± 9.7° | 5.5 ± 6.5° | 4.6 ± 4.4° | 5.4 ± 5.2° | 4.8 ± 5.4° | 5.8 ± 4.0° | 0.435 |
| TS (°) | 22.8 ± 10.2° | 5.7 ± 6.2° | 4.4 ± 4.4° | 5.1 ± 6.1° | 5.7 ± 4.6° | 5.4 ± 6.4° | 0.645 |
| TS-CL (°) | 9.8 ± 2.4° | 4.1 ± 5.9° | 4.5 ± 6.3° | 4.1 ± 5.3° | 3.9 ± 4.4° | 3.7 ± 4.8° | 0.421 |
| ODHA (°) | 4.3 ± 5.4° | 0.2 ± 0.2° | 0.1 ± 0.4° | 0.1 ± 0.2° | 0.1 ± 0.3° | 0.3 ± 0.9° | 0.764 |
| PI-LL (°) | 12.1 ± 7.5° | 3.0 ± 4.5° | 3.1 ± 4.9° | 2.0 ± 2.7° | 2.4 ± 4.8° | 2.1 ± 3.2° | 0.841 |
| SSA (°) | 120.1 ± 12.4° | 3.3 ± 2.5° | 3.2 ± 2.6° | 4.0 ± 2.48° | 3.1 ± 2.4° | 3.9 ± 2.5° | 0.623 |
| SVA (mm) | 22.1 ± 19.2 mm | 3.0 ± 2.9 mm | 2.0 ± 2.5 mm | 2.9 ± 2.5 mm | 2.7 ± 1.1 mm | 2.9 ± 1.5 mm | 0.812 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noh, S.H.; Lee, G.; Bae, H.-J.; Han, J.Y.; Son, S.J.; Kim, D.; Park, J.Y.; Choi, S.K.; Cho, P.G.; Kim, S.H.; et al. Deep Learning Method for Precise Landmark Identification and Structural Assessment of Whole-Spine Radiographs. Bioengineering 2024, 11, 481. https://doi.org/10.3390/bioengineering11050481
Noh SH, Lee G, Bae H-J, Han JY, Son SJ, Kim D, Park JY, Choi SK, Cho PG, Kim SH, et al. Deep Learning Method for Precise Landmark Identification and Structural Assessment of Whole-Spine Radiographs. Bioengineering. 2024; 11(5):481. https://doi.org/10.3390/bioengineering11050481
Chicago/Turabian StyleNoh, Sung Hyun, Gaeun Lee, Hyun-Jin Bae, Ju Yeon Han, Su Jeong Son, Deok Kim, Jeong Yeon Park, Seung Kyeong Choi, Pyung Goo Cho, Sang Hyun Kim, and et al. 2024. "Deep Learning Method for Precise Landmark Identification and Structural Assessment of Whole-Spine Radiographs" Bioengineering 11, no. 5: 481. https://doi.org/10.3390/bioengineering11050481