
Ultrasound Imaging in Football Players with Previous Multiple Ankle Sprains: Keeping a Close Eye on Superior Ankle Retinaculum

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
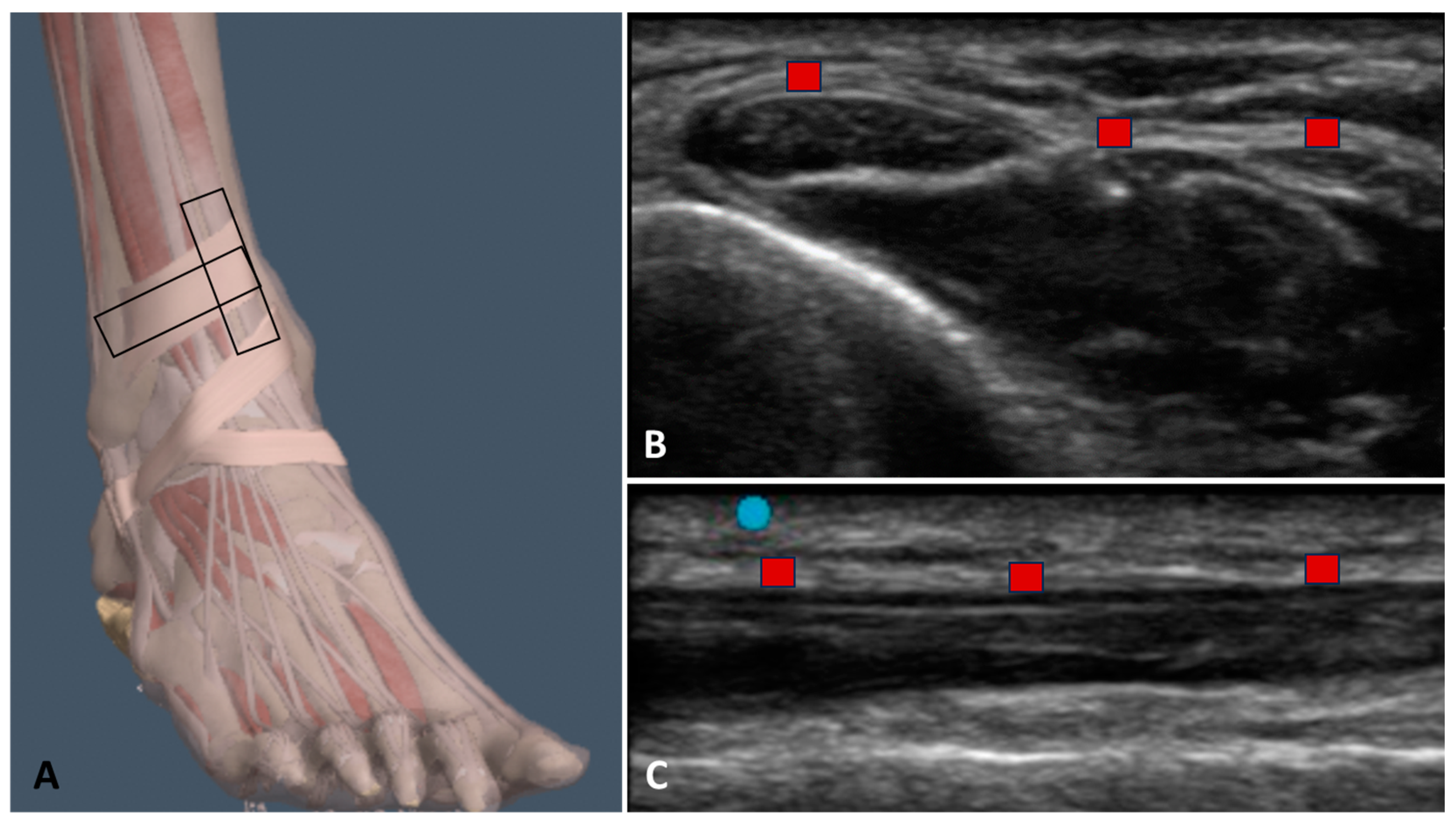
2.3. Ultrasound Examination Measurements
2.4. Statistical Analysis
3. Results
3.1. Ultrasound Measurements of the Superior Extensor Ankle Retinaculum
3.1.1. Group 1 (Football Players with Previous Multiple Ankle Sprains)
3.1.2. Group 2 (Healthy Volunteers)
3.2. Ultrasound Measurements of the Superior Extensor Ankle Retinaculum: Comparison between Previous Multiple Ankle Sprains and Healthy Sides in Group 1
3.3. Ultrasound Measurements of the Superior Extensor Ankle Retinaculum: Comparison between Two Sides in Group 2
3.4. Ultrasound Measurements of the Superior Extensor Ankle Retinaculum: Comparison between the Previously Sprained Side of Group 1 with the Corresponding Side in Group 2
3.5. Ultrasound Measurements of the Superior Extensor Ankle Retinaculum: Comparison between the Healthy Side of Group 1 with the Corresponding Side in Group 2
3.6. Echogenicity Measurements
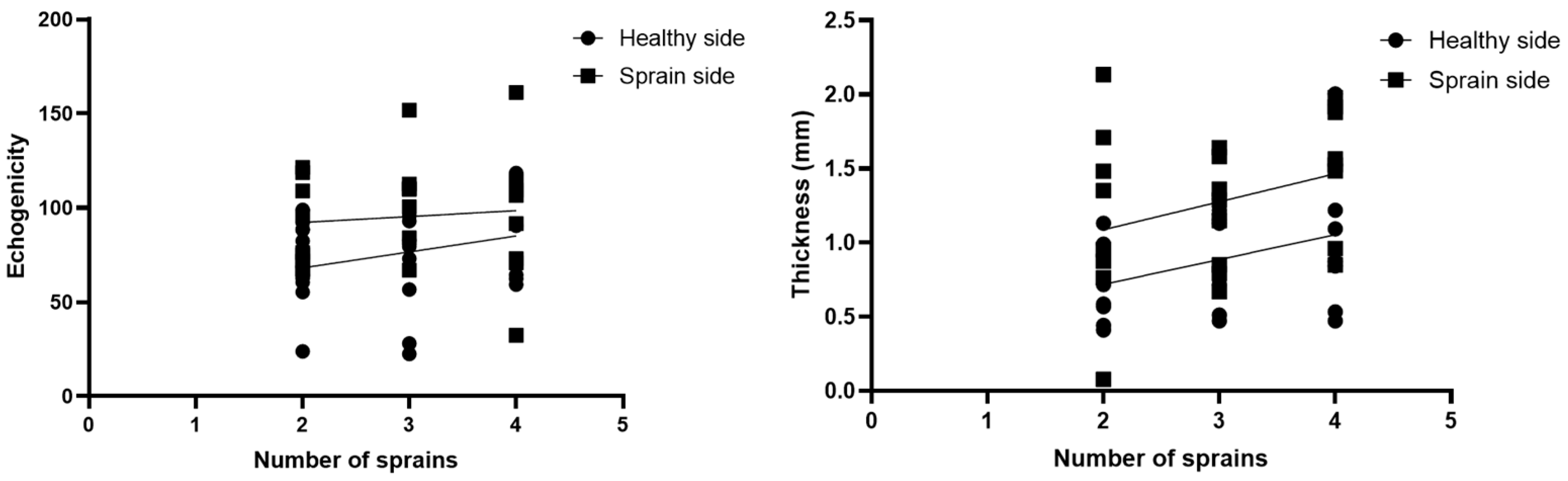
3.7. Correlations US Measurements and Number of Ankle Sprains
3.8. Intra-Rater Reliability
4. Discussion
Limitation of Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- FIFA. FIFA Big Count; FIFA Communications Division, Information Services: Zürichberg, Switzerland, 2006; Available online: https://www.fifa.com/mm/document/fifafacts/%20bcoffsurv/%20bigcount.%20statspackage_%207024.pdf (accessed on 28 February 2024).
- Gurau, T.V.; Gurau, G.; Voinescu, D.C.; Anghel, L.; Onose, G.; Iordan, D.A.; Munteanu, C.; Onu, I.; Musat, C.L. Epidemiology of Injuries in Men’s Professional and Amateur Football (Part I). J. Clin. Med. 2023, 12, 5569. [Google Scholar] [CrossRef] [PubMed]
- Gurau, T.V.; Gurau, G.; Musat, C.L.; Voinescu, D.C.; Anghel, L.; Onose, G.; Munteanu, C.; Onu, I.; Iordan, D.A. Epidemiology of Injuries in Professional and Amateur Football Men (Part II). J. Clin. Med. 2023, 12, 6293. [Google Scholar] [CrossRef] [PubMed]
- Hägglund, M.; Waldén, M.; Magnusson, H.; Kristenson, K.; Bengtsson, H.; Ekstrand, J. Injuries affect team performance negatively in professional football: An 11-year follow-up of the UEFA Champions League injury study. Br. J. Sports Med. 2013, 47, 738–742. [Google Scholar] [CrossRef] [PubMed]
- Roe, M.; Murphy, J.C.; Gissane, C.; Blake, C. Time to get our four priorities right: An 8-year prospective investigation of 1326 player-seasons to identify the frequency, nature, and burden of time-loss injuries in elite Gaelic football. PeerJ 2018, 6, e4895. [Google Scholar] [CrossRef] [PubMed]
- López-Valenciano, A.; Ruiz-Pérez, I.; Garcia-Gómez, A.; Vera-Garcia, F.J.; De Ste Croix, M.; Myer, G.D.; Ayala, F. Epidemiology of injuries in professional football: A systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Injury incidence and injury patterns in professional football: The UEFA injury study. Br. J. Sports Med. 2011, 45, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Shalaj, I.; Tishukaj, F.; Bachl, N.; Tschan, H.; Wessner, B.; Csapo, R. Injuries in professional male football players in Kosovo: A descriptive epidemiological study. BMC Musculoskel. Disord. 2016, 17, 338. [Google Scholar] [CrossRef] [PubMed]
- Junge, A.; Dvořák, J. Football injuries during the 2014 FIFA World Cup. Br. J. Sports Med. 2015, 49, 599–602. [Google Scholar] [CrossRef] [PubMed]
- Pfirrmann, D.; Herbst, M.; Ingelfinger, P.; Simon, P.; Tug, S. Analysis of Injury Incidences in Male Professional Adult and Elite Youth Soccer Players: A Systematic Review. J. Athl. Train. 2016, 51, 410–424. [Google Scholar] [CrossRef] [PubMed]
- Ekstrand, J.; Tropp, H. The incidence of ankle sprains in soccer. Foot Ankle 1990, 11, 41–44. [Google Scholar] [CrossRef]
- Junge, A.; Dvorak, J. Soccer injuries: A review on incidence and prevention. Sports Med. 2004, 34, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Woods, C.; Hawkins, R.; Hulse, M.; Hodson, A. The Football Association Medical Research Programme: An audit of injuries in professional football: An analysis of ankle sprains. Br. J. Sports Med. 2003, 37, 233–238. [Google Scholar] [CrossRef]
- Hawkins, R.D.; Fuller, C.W. A prospective epidemiological study of injuries in four English professional football clubs. Br. J. Sports Med. 1999, 33, 196–203. [Google Scholar] [CrossRef]
- Waldén, M.; Hägglund, M.; Ekstrand, J. Injuries in Swedish elite football—A prospective study on injury definitions, risk for injury and injury pattern during 2001. Scand. J. Med. Sci. Sports 2005, 15, 118–125. [Google Scholar] [CrossRef]
- Giza, E.; Fuller, C.; Junge, A.; Dvorak, J. Mechanisms of foot and ankle injuries in soccer. Am. J. Sports Med. 2003, 31, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Andersen, T.E.; Floerenes, T.W.; Arnason, A.; Bahr, R. Video analysis of the mechanisms for ankle injuries in football. Am. J. Sports Med. 2004, 32 (Suppl. 1), 69S–79S. [Google Scholar] [CrossRef]
- Demondion, X.; Canella, C.; Moraux, A.; Cohen, M.; Bry, R.; Cotton, A. Retinacular disorders of the ankle and foot. Semin. Musculoskelet. Radiol. 2010, 14, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Numkarunarunrote, N.; Malik, A.; Aguiar, R.O.; Trudell, D.J.; Resnick, D. Retinacula of the foot and ankle: MRI with anatomic correlation in cadavers. Am. J. Roentgenol. 2007, 188, W348–W354. [Google Scholar] [CrossRef]
- Stecco, A.; Stecco, C.; Macchi, V.; Porzionato, A.; Ferraro, C.; Masiero, S.; De Caro, R. RMI study and clinical correlations of ankle retinacula damage and outcomes of ankle sprain. Surg. Radiol. Anat. 2011, 33, 881–890. [Google Scholar] [CrossRef]
- Bianchi, S.; Becciolini, M. Ultrasound Features of Ankle Retinacula: Normal Appearance and Pathologic Findings. J. Ultrasound Med. 2019, 38, 3321–3334. [Google Scholar] [CrossRef]
- Pirri, C.; Stecco, A.; Stecco, C.; Özçakar, L. Ultrasound imaging and Fascial Manipulation: ’Adding a twist‘ on the ankle retinacula. J. Bodyw. Mov. Ther. 2024, 37, 90–93. [Google Scholar] [CrossRef] [PubMed]
- Pirri, C.; Stecco, A.; Stecco, C.; Özçakar, L. Ultrasound imaging and Fascial Manipulation for rigid retinacula in two cases of complex regional pain syndrome. Med. Ultrason. 2022, 24, 372–374. [Google Scholar] [CrossRef] [PubMed]
- Pirri, C.; Stecco, C.; Güvener, O.; Mezian, K.; Ricci, V.; Jačisko, J.; Fojtik, P.; Kara, M.; Chang, K.V.; Dughbaj, M.; et al. EURO-MUSCULUS: European Musculoskeletal Ultrasound Study Group in Physical and Rehabilitation Medicine. EURO-MUSCULUS/USPRM Dynamic Ultrasound Protocols for Ankle/Foot. Am. J. Phys. Med. Rehabil. 2024, 103, e29–e34. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef]
- Grob, A.T.; Veen, A.A.; Schweitzer, K.J.; Withagen, M.I.; van Veelen, G.A.; van der Vaart, C.H. Measuring echogenicity and area of the puborectalis muscle: Method and reliability. Ultrasound Obstet. Gynecol. 2014, 44, 481–485. [Google Scholar] [CrossRef]
- Cohen, J. Things I have learned (so far). Am. Psychol. 1990, 45, 1304–1312. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Pirri, C.; Caroccia, B.; Angelini, A.; Piazza, M.; Petrelli, L.; Caputo, I.; Montemurro, C.; Ruggieri, P.; De Caro, R.; Stecco, C. A New Player in the Mechanobiology of Deep Fascia: Yes-Associated Protein (YAP). Int. J. Mol. Sci. 2023, 24, 15389. [Google Scholar] [CrossRef]
- Pirri, C.; Petrelli, L.; Pérez-Bellmunt, A.; Ortiz-Miguel, S.; Fede, C.; De Caro, R.; Miguel-Pérez, M.; Stecco, C. Fetal Fascial Reinforcement Development: From “a White Tablet” to a Sculpted Precise Organization by Movement. Biology 2022, 11, 735. [Google Scholar] [CrossRef]
- Pirri, C.; Pirri, N.; Porzionato, A.; Boscolo-Berto, R.; De Caro, R.; Stecco, C. Inter- and Intra-Rater Reliability of Ultrasound Measurements of Superficial and Deep Fasciae Thickness in Upper Limb. Diagnostics 2022, 12, 2195. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data | Group 1 | Group 2 | p-Value Group 1 vs. Group 2 |
|---|---|---|---|
| Age, year | 29.96 ± 10.54 | 28.09 ± 12.38 | p = 0.14 |
| Weight, kg | 69.22 ± 6.1 | 72.60 ± 12.20 | p = 0.45 |
| Height, cm | 174.3 ± 4.83 | 171.30 ± 6.76 | p = 0.55 |
| Descriptive Statistics | H. Side (long.) | H. Side (trans.) | S. Side (long.) | S. Side (trans.) |
|---|---|---|---|---|
| Number of values | 25 | 25 | 25 | 25 |
| Minimum | 0.41 | 0.44 | 0.67 | 0.50 |
| Maximum | 2 | 1.72 | 2.14 | 2.51 |
| Mean | 0.90 | 0.92 | 1.3 | 1.33 |
| Std. deviation | 0.4 | 0.44 | 0.44 | 0.51 |
| Std. error of mean | 0.08 | 0.08 | 0.08 | 0.1 |
| Descriptive Statistics | R. Side (long.) | R. Side (transv.) | L. Side (long.) | L. Side (transv.) |
|---|---|---|---|---|
| Number of values | 25 | 25 | 25 | 25 |
| Minimum | 0.41 | 0.43 | 0.43 | 0.44 |
| Maximum | 2.1 | 2.1 | 1.9 | 1.9 |
| Mean | 0.90 | 0.83 | 0.90 | 0.90 |
| Std. deviation | 0.44 | 0.42 | 0.43 | 0.44 |
| Std. error of mean | 0.08 | 0.08 | 0.08 | 0.08 |
| Type of Comparison | Mean Diff. | p-Value |
|---|---|---|
| Group 1 S. side (long.) vs. group 2 c.s. (long.) Group 1 S. side (transv.) vs. group 2 c.s. (transv.) | 0.3902 0.4981 | p = 0.003 p = 0.004 |
| Type of Comparison | Mean Diff. | p-Value |
|---|---|---|
| Group 1 H. side (long.) vs. group 2 c.s. (long.) Group 1 H. side (transv.) vs. group 2 c.s. (transv.) | −0.045 0.027 | p = 0.68 p = 0.82 |
| Descriptive Statistics | H. Side (Group 1) | S. Side (Group 1) | R. Side (Group 2) | L. Side (Group 2) |
|---|---|---|---|---|
| Number of values | 25 | 25 | 25 | 25 |
| Minimum | 36.58 | 45.05 | 46.2 | 41.91 |
| Maximum | 166.1 | 158.9 | 145.7 | 133.8 |
| Mean | 93.84 | 94.61 | 80.80 | 89.44 |
| Std. deviation | 29.10 | 27.17 | 29.04 | 26.72 |
| Type of Comparison | Mean Diff. | p-Value |
|---|---|---|
| Group 1 H. side vs. group 1 S. side | −0.77 | p = 0.99 |
| Group 1 H. side vs. group 2 c.s. | 13.04 | p = 0.35 |
| Group 1 H. side vs. group 2 c.s. | 4.39 | p = 0.94 |
| Group 1 S. side vs. group 2 c.s. | 13.81 | p = 0.31 |
| Group 1 S. side vs. group 2 c.s. | 5.16 | p = 0.91 |
| Group 2 right vs. group 2 left | −8.64 | p = 0.69 |
| Type of Axis | ICC |
|---|---|
| Group 1 H. side (long.) | 0.90 (0.89–0.94) |
| Group 1 H. side (transv.) | 0.92 (0.88–0.96) |
| Group 1 S. side (long.) | 0.91 (0.88–0.94) |
| Group 1 S. side (transv.) | 0.92 (0.88–0.96) |
| Group 2 left (long.) | 0.90 (0.89–0.94) |
| Group 2 left (transv.) | 0.91 (0.89–0.96) |
| Group 2 right (long.) | 0.90 (0.89–0.94) |
| Group 2 right (transv.) | 0.91 (0.89–0.94) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pirri, C.; Pirri, N.; Guidolin, D.; Macchi, V.; Porzionato, A.; De Caro, R.; Stecco, C. Ultrasound Imaging in Football Players with Previous Multiple Ankle Sprains: Keeping a Close Eye on Superior Ankle Retinaculum. Bioengineering 2024, 11, 419. https://doi.org/10.3390/bioengineering11050419
Pirri C, Pirri N, Guidolin D, Macchi V, Porzionato A, De Caro R, Stecco C. Ultrasound Imaging in Football Players with Previous Multiple Ankle Sprains: Keeping a Close Eye on Superior Ankle Retinaculum. Bioengineering. 2024; 11(5):419. https://doi.org/10.3390/bioengineering11050419
Chicago/Turabian StylePirri, Carmelo, Nina Pirri, Diego Guidolin, Veronica Macchi, Andrea Porzionato, Raffaele De Caro, and Carla Stecco. 2024. "Ultrasound Imaging in Football Players with Previous Multiple Ankle Sprains: Keeping a Close Eye on Superior Ankle Retinaculum" Bioengineering 11, no. 5: 419. https://doi.org/10.3390/bioengineering11050419