An Explorative Study of Qualities in Interactive Processes with Children and Their Parents in Music Therapy during and after Pediatric Hematopoietic Stem Cell Transplantation

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Previous Randomized Study
2.2. Music Therapy Protocol in the Randomized Study
2.3. Participants in the Interview Study
2.4. Thematic Analysis of Audio-Recorded Interviews: Procedure
2.5. Line of Argument Concerning Role and Task of the Interviewer
3. Results
3.1. Thematic Analysis: Compilation of Results
3.2. From the Analysis
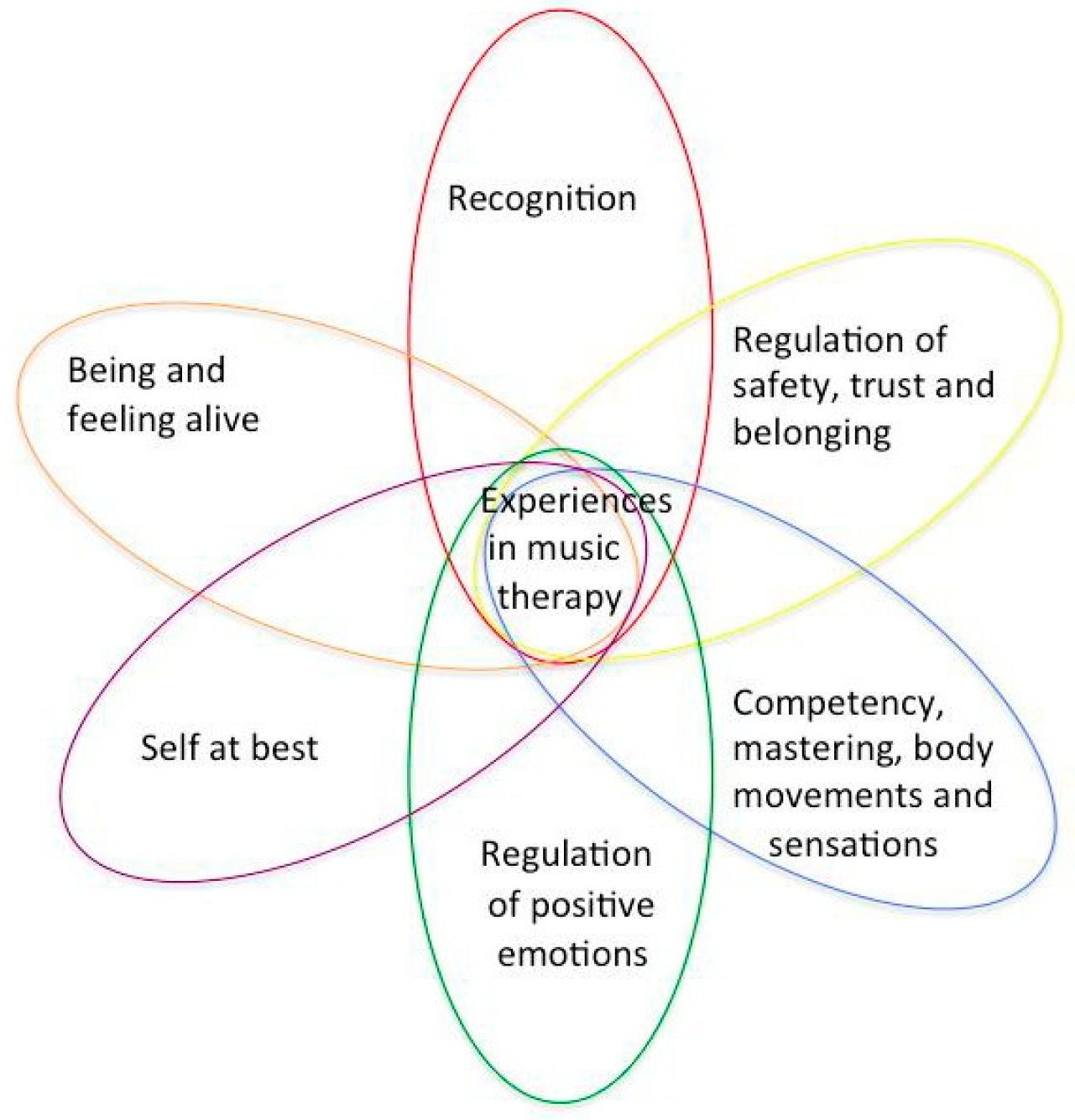
3.3. Compiled Themes from the Analysis
- Being and feeling alive
- Regulation of positive emotions, affects
- Competency, mastering body movements and sensations
- Recognition in meeting the therapist, themselves with family members and the music
- Self at best, experiencing self in relation, self-assertion
- Regulation of safety, trust, and belonging
4. Discussion
4.1. Limitations
4.2. Further Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Questions |
| In the following, the questions of the inquiry are described with their underlying intention. |
| How was it to be involved in music therapy? |
| The focus of this question was the overall experience of the participants, child as well as parents and siblings, of being involved with music therapy. The focus was on the general experience of the entire music therapy process. |
| How was it to play music in this way? |
| The focus was on the phenomenological subjective experience of interacting and collaborating with the music therapist when musicking, to find the participants’ descriptions of experiencing the musicking in detailed and concrete ways. The musicking is assumed to contain/encompass collaborative and interactive regulation. |
| What was the best/the worst? |
| In this question, the focus was on finding and exploring even more specific moments in the interaction and collaboration, moments with both a positive and negative experiential flavor. |
| Is there anything special you remember from when you played, sang, improvised? |
| This question was connected to the previous one, and was intended to deepen the exploration of memories from the music therapy process. It is assumed that moments of interaction and collaboration that stand out in memory carry a certain affective quality or intensity. As such, they were assumed to contain potential for change. |
| How was it to get music therapy during the HSCT/after the HSCT? |
| It was important to evaluate the participants’ experience of being involved in music therapy both during and after HSCT, to understand how this affected the experience of music therapy. |
| The therapist’s perspective: Ad hoc questions formulated when meeting the child and the parents. |
| According to the assumptions behind the format of the collaborative interview, the opportunity to explore collaborative and interactive qualities of a certain therapeutic intervention is connected to the therapist’s subjective perspective of the collaboration. Therefore, this theme of inquiry was explored to access the memories and experiences of the participants. This is further discussed in the Discussion section of the paper. The last two questions were intended to facilitate reflection by the participants on the overall process from a meta-perspective. |
| 1. How was it to be involved in music therapy? |
| 1.1. Musicality was evoked |
| Mother: We noticed in A, A loves music. (A) |
| Laughter during interview when listening to recordings from the MT sessions. (B) |
| Mother: I am moved when C tells us this. (C) |
| Mother: When we came home, D wanted a guitar. D got more interested in music. (D) |
| During the interview, participants shared memories through singing together. (E) |
| Mother: I myself like music, we sing in church. (F) |
| 1.2. Monotonous isolation was broken |
| Mother: The thing was that we got away from it, A could leave the room. (A) |
| Child: I got cheerful, happy when T came into my room. (C) |
| Mother: Asked after each session, when is next. (D) |
| Father: When T came, E wanted to leave E’s mom and that was fun for all of us. (E) |
| 1.3. A “sense of normality” was evoked |
| Mother: A became revived, could come out—it was life in it. (A) |
| Mother: B had a positive experience, felt better, became less gloomy. B breathed more freely. (B) |
| Mother: After C sang together with T, C experienced it [the treatment] differently. (C) |
| Mother: all of us got happy, [sibling] too. Joy, happy, to feel alive. (F) |
| 1.4. Child’s competencies were activated |
| Mother: A got a task and purpose. (A) |
| During the interview, B played recordings of the songs B made together with T and expressed in head nods that it was familiar for B to sing songs and that it felt safe for B to sing. (B) |
| Mother: It was good that B could decide/suggest. (B) |
| Child: When I sang with T, I forgot the pain. (C) |
| 1.5. Music therapy offered pain diversion |
| Mother: Became easier [for B] to breathe. It affected the senses. (B) |
| Child: When I met T in MT I forgot the pain. (C) |
| Father: E became happy, and at the same time very tired. (E) |
| 1.6. Music therapy evoked regulation of different kinds of affects |
| Mother about B: Easier to breathe, affected B’s mind. It was like T captured when B was enclosed a clam like. (B) |
| Child: I felt joy when T entered my room. I love music. (C) |
| Mother: We felt safe and happy after each MT session. (D) |
| Father: When they have fun, I also feel happy. Mother: It helped me to see them happy, [because] it was very hard. (E) |
| Mother: F became happier, F smiled at once. We all became happy. (F) |
| 2. How was it to play music in this way? |
| 2.1. Music therapy activated bodily sensations and affects |
| Mother: A felt happy, A recognized, longed [for MT]. It was fun. How it felt in the body. (A) |
| B smiled and nodded during interview. Father confirmed that B felt safe. (B) |
| Mother: D got more interested, happy after each meeting. D shows during interview: “aha!” you can do this! (D) |
| Father: It was great fun, E became happy. It was fun for all of us. (E) |
| Mother: That half hour, was very fun, F liked, danced. (F) |
| 2.2. Emergence of interactive regulation |
| Father and B conveyed that it suited B, it was familiar to B to play and sing, B knew many songs before. Father expressed that the familiar became safe for B. (B) |
| Child: I noticed that the pain was affected, I could also listen. (C) |
| During interview, D showed a video on the iPhone from one MT session, and conveyed that it was fun and important. (D) |
| Mother: When T learned a song from our native country, F started to dance, it evoked something. (F) |
| 3. What was the best/the worst? |
| 4. Is there anything special you remember from when you played, sang, improvised? |
| 3, 4 Evoked positive experiences also contrasted with the longing for more sessions |
| Mother: It was fun to play together. T always took her time. We felt recognized. We felt remembered, one is a human being. One feels warmth in heart. (A) |
| Father: I remember when we wrote songs, it was nice interplay. B revived, felt confident in her/him self. It was laughter, hilariousness. (B) |
| Child: Remember once we could not do anything [play, due to too much pain], did not feel good when she left. Once, in the shower the pain went down when I started to sing. (C) |
| Mother: D felt sad the last time. Then D got more aroused. It was too short. (D) |
| Father: Noticed that E became happier, that E and E’s sibling played together and that sibling helped E to play. Sibling waited for T all the time. Every second day would have been better. (E) |
| Mother: Once, new energy when Fs uncle came. Relatives [from…] took part. (F) |
| 5. How was it to get music therapy during the HSCT/after HSCT? |
| 5. The experienced period was appreciated |
| Mother: We found it was best as it was. (A) |
| Father: Better during HSCT, a break in the room. Mother: 100% best—if not, we had not created/written those songs! (B) |
| Child: It was best during HSCT, it was when I needed it. (C) |
| Mother: It was best after HSCT, D had more strength. (D) |
| Mother: Perhaps better during HSCT. Mother expressed it would have felt better when the child was small. We are one. (F) |
| 6. The therapist’s perspective: Ad hoc questions formulated when meeting the child and parents. |
| 6. Mutuality and sharing in the collaboration |
| Recollects A’s musicality with many songs of A’s own. Mother and Father met A, A engaged them. (A) |
| B does not speak but shows a positive face and nods. B and Father convey that it suited B very well, it was familiar to B to sing, B knew many songs before. Father thinks that the familiar became safe for B. (B) |
| Recollects C’s curiosity, and that they made music together. Remembers that C had pain, and now asks how it was for C to play in spite of pain. (C) |
| Recollects the family as four strongly tight together. A lot of energy. Sibling, when E was tired, played, and it was good for E. Sibling helped E to become interested, helped the little sibling. T sometimes felt she interrupted. E was in the music together with E’s sibling. They really interacted, interplayed. (E) |
| T and F meet each other through playing together for a while, since F immediately turns towards the instruments that F recognizes from the MT sessions. T remembers it being simple, F’s positive expectancies and desire to be with the music. T also remembers that mother supported through her personality and way of engaging. It was helpful to the T. (F) |
| When T and D meet, they reconnect nonverbally and remain in interactive musicking during the interview, without any verbal dialogue. The meeting seemed like a continuation of their former process. D, through verbal statements from the mother, conveyed that the music therapy was too short. (D) |
| 1. How was it to be involved in music therapy? |
| 1.1. The entire experience evoked musicality, both in the here and now and as a recollecting process of former experiences of music. 1.2. Music therapy was experienced as a break in the monotonous isolation necessary for the treatment. This was assumed to contribute to the participant’s capacity to preserve a connection to life outside the hospital. 1.3. The music therapy sessions evoked a sense of “normality” connected to the participant’s normal life and a sense of being in life, being alive. 1.4. Music therapy evoked participants’ own competencies, like former musical activities and a general sensorimotor competency. 1.5. Music therapy evoked diversion from pain, and presumably also from fear. 1.6. Music therapy activated affects: curiosity, joy, liveliness, and energy arousal. |
| 2. How was it to play music in this way? |
| 2.1. Music therapy activated bodily sensations of joy, curiosity, and energy arousal, which is a deeper level of experiencing and regulating one’s affects. 2.2. Music therapy generated and evoked memories of experiences of competency, self at best, self-assertion. The act of learning and playing songs was connected to the ability to express a sense of self. In the domain of interaction and regulation, the sharing and regulating with the therapist, parents, and siblings generated experiences of recognition and positive affects in meeting and interactive regulation. It is assumed that it also generated memories of interactive regulation and self-regulation. Sensorimotor, tactile, auditory, and visual experiences of handling instruments, singing, and making body movements were assumed to evoke implicit memories of competency, self-regulation, and interactive regulation of arousal levels and affects. These, in turn, amplified experiences of safety and trust, affirmation and confirmation. In the following, responses to two questions are depicted together, since the answers conveyed that they were connected according the experiences of the participants. The question about what was the best/the worst (question 3) seemed to be equal to memories of “special moments” (question 4). The questions were: |
| 3. What was the best/the worst? |
| 4. Is there anything special you remember from when you played, sang, improvised? |
| The responses illuminate highlights of being recognized and confirmed. Sometimes tiredness and pain were in the way. The experience often evoked a longing for more sessions. The evoked positive experiences also contrasted with the longing for and shortage of sessions. Some participants remembered specific songs they learned or composed. Others remembered moments of change, such as when the therapist left or ended a session, which triggered feelings of sadness or worry. |
| 5. How was it to get music therapy during the HSCT/after the HSCT? |
| All participants appreciated the period they experienced. Some emphasized that they appreciated music therapy both during and after HSCT. |
| 6. The therapist’s perspective: Ad hoc questions formulated when meeting the child and parents. |
| The therapist’s memories of each participant and her/his family were taken as a point of departure in each interview. Through the recollecting process in the meeting, six personalized narratives emerged. The common ingredient in each meeting appeared to be how the child, during music therapy, reconnected to his/her relationship with music. The parents were often part of the process, present in different ways depending on the age of the child. Some were just present in the room and some actively took part in the musical interaction. From the perspective of the therapist, they were all felt to be facilitators of the process. The therapist remembered several moments of meeting and of interaction characterized by positive emotions such as joy, laughter, and curiosity. She also remembered how the children’s specific sense of self, or character, was displayed during music therapy. In the process of recollection, the therapist often described her sense of mutuality or reciprocity in the collaboration, and she also expressed how she learned from the meetings. One meeting, with participant D, induced a kind of continuation of the therapeutic process as D stayed in a nonverbal interaction, playing on different instruments with the therapist during the whole interview. |
References
- Miano, M.; Labopin, M.; Hartmann, O.; Angelucci, E.; Cornish, J.; Gluckman, E.; Locatelli, F.; Fischer, A.; Egeler, R.M.; Or, R.; et al. Haematopoietic stem cell transplantation trends in children over the last three decades: A survey by the paediatric diseases working party of the european group for blood and marrow transplantation. Bone Marrow Transpl. 2007, 39, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Remberger, M.; Ackefors, M.; Berglund, S.; Blennow, O.; Dahllöf, G.; Dlugosz, A.; Garming -Legert, K.; Gertow, J.; Gustafsson, B.; Hassan, M.; et al. Improved survival after allogeneic hematopoietic stem cell transplantation in recent years. A single-center study. Biol. Blood Marrow Transpl. 2011, 17, 1688–1697. [Google Scholar] [CrossRef] [PubMed]
- Tanzi, E.M. Health-related quality of life of hematopoietic stem cell transplant childhood survivors: State of the science. J. Pediatr. Oncol. Nurs. 2011, 28, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Rodgers, C.; Wills-Bagnato, P.; Sloane, R.; Hockenberry, M. Health-related quality of life among children and adolescents during hematopoietic stem cell transplant recovery. J. Pediatr. Oncol. Nurs. 2015, 32, 329–336. [Google Scholar] [CrossRef]
- Tremolada, M.; Bonichini, S.; Pillon, M.; Messina, C.; Carli, M. Quality of life and psychosocial sequelae in children undergoing hematopoietic stem-cell transplantation: A review. Pediatr. Transpl. 2009, 13, 955–970. [Google Scholar] [CrossRef] [PubMed]
- Rodday, A.M.; Terrin, N.; Leslie, L.K.; Graham, R.J.; Parsons, S.K. Understanding the relationship between child health-related quality of life and parent emotional functioning in pediatric hematopoietic stem cell transplant. J. Pediatr. Psychol. 2017, 42, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Tremolada, M.; Bonichini, S.; Basso, G.; Pillon, M. Post-traumatic stress symptoms and post-traumatic growth in 223 childhood cancer survivors: Predictive risk factors. Front. Psychol. 2016, 7, 287. [Google Scholar] [CrossRef]
- Stuber, M.L.; Nader, K.; Yasuda, P.; Pynoos, R.S.; Cohen, S. Stress responses after pediatric bone marrow transplantation: Preliminary results of a prospective longitudinal study. J. Am. Acad. Child Adolesc. Psychiatry 1991, 30, 952–957. [Google Scholar] [CrossRef]
- Buchbinder, D.; Kelly, D.L.; Duarte, R.F.; Auletta, J.J.; Bhatt, N.; Byrne, M.; DeFilipp, Z.; Gabriel, M.; Mahindra, A.; Norkin, M.; et al. Neurocognitive dysfunction in hematopoietic cell transplant recipients: Expert review from the late effects and quality of life working committee of the cibmtr and complications and quality of life working party of the EBMT. Bone Marrow Transpl. 2018, 53, 535–555. [Google Scholar] [CrossRef]
- Cozolino, L.J. The Neuroscience of Psychotherapy: Healing the Social Brain; W.W. Norton & Co.: New York, NY, USA, 2010; p. 262. [Google Scholar]
- Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Publishing: Arlington, VA, USA, 2013.
- Siegel, D.J. The Developing Mind: Toward a Neurobiology of Interpersonal Experience; Guilford Press: New York, NY, USA, 1999; pp. 253–258. [Google Scholar]
- Phipps, S.; Dunavant, M.; Lensing, S.; Rai, S.N. Psychosocial predictors of distress in parents of children undergoing stem cell or bone marrow transplantation. J. Pediatr. Psychol. 2005, 30, 139–153. [Google Scholar] [CrossRef]
- Jobe-Shields, L.; Alderfer, M.A.; Barrera, M.; Vannatta, K.; Currier, J.M.; Phipps, S. Parental depression and family environment predict distress in children before stem cell transplantation. J. Dev. Behav. Pediatr. 2009, 30, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Packman, W.; Weber, S.; Wallace, J.; Bugescu, N. Psychological effects of hematopoietic sct on pediatric patients, siblings and parents: A review. Bone Marrow Transpl. 2010, 45, 1134–1146. [Google Scholar] [CrossRef] [PubMed]
- Switzer, G.E.; Bruce, J.; Kiefer, D.M.; Kobusingye, H.; Drexler, R.; Besser, R.M.; Confer, D.L.; Horowitz, M.M.; King, R.J.; Shaw, B.E.; et al. Health-related quality of life among pediatric hematopoietic stem cell donors. J. Pediatr. 2016, 178, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Hutt, D.; Nehari, M.; Munitz-Shenkar, D.; Alkalay, Y.; Toren, A.; Bielorai, B. Hematopoietic stem cell donation: Psychological perspectives of pediatric sibling donors and their parents. Bone Marrow Transpl. 2015, 50, 1337–1342. [Google Scholar] [CrossRef] [PubMed]
- Riva, R.; Forinder, U.; Arvidson, J.; Mellgren, K.; Toporski, J.; Winiarski, J.; Norberg, A.L. Patterns of psychological responses in parents of children that underwent stem cell transplantation. Psychooncology 2014, 23, 1307–1313. [Google Scholar] [CrossRef] [PubMed]
- Wills, T.A.; Simons, J.S.; Sussman, S.; Knight, R. Emotional self-control and dysregulation: A dual-process analysis of pathways to externalizing/internalizing symptomatology and positive well-being in younger adolescents. Drug Alcohol Depend. 2016, 163 (Suppl. 1), S37–S45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowlby, J.; Wiking, P.; Risholm Mothander, P. En Trygg Bas: Kliniska Tillämpningar av Anknytningsteorin; Natur & Kultur: Stockholm, Sweden, 2010; pp. 144–148. [Google Scholar]
- Bergsten, K. Affektfokuserad Psykodynamisk Terapi: Teori, Empiri och Praktik; Natur & Kultur: Stockholm, Sweden, 2015; pp. 44–45. [Google Scholar]
- Stern, D.N. The Interpersonal World of the Infant: A View from Psychoanalysis and Developmental Psychology; Basic Books: New York, NY, USA, 2000; pp. 111–114. [Google Scholar]
- Chanda, M.L.; Levitin, D.J. The neurochemistry of music. Trends Cogn. Sci. 2013, 17, 179–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finn, S.; Fancourt, D. The biological impact of listening to music in clinical and nonclinical settings: A systematic review. Prog. Brain Res. 2018, 237, 173–200. [Google Scholar] [CrossRef]
- Fancourt, D.; Ockelford, A.; Belai, A. The psychoneuroimmunological effects of music: A systematic review and a new model. Brain Behav. Immun. 2014, 36, 15–26. [Google Scholar] [CrossRef]
- Moore, K.S. A systematic review on the neural effects of music on emotion regulation: Implications for music therapy practice. J. Music 2013, 50, 198–242. [Google Scholar] [CrossRef]
- Theorell, T. Psychological Health Effects of Musical Experiences [Elektronisk Resurs]: Theories, Studies and Reflections in Music Health Science; Springer: Dordrecht, The Netherlands, 2014; pp. 9–16, 33–48. [Google Scholar]
- Juslin, P.N.; Sloboda, J.A. Handbook of Music and Emotion: Theory, Research, and Applications; Oxford University Press: Oxford, UK, 2010; pp. 3–5. [Google Scholar]
- Sena Moore, K.; Hanson-Abromeit, D. Theory-guided therapeutic function of music to facilitate emotion regulation development in preschool-aged children. Front. Hum. Neurosci. 2015, 9, 572. [Google Scholar] [CrossRef] [PubMed]
- Malloch, S.; Trevarthen, C. Communicative Musicality: Exploring the Basis of Human Companionship; Oxford University Press: Oxford, UK, 2008; p. 9. [Google Scholar]
- Dun, B. Children with cancer. In Guidelines for Music Therapy Practice in Pediatric Care [Elektronisk Resurs]; Bradt, J., Ed.; Barcelona Publishers: Gilsum, NH, USA, 2012; pp. 363–406. [Google Scholar]
- Trondalen, G. Intersubjectivity and Development as a dialogical continuum. In Relational Music Therapy: An Intersubjective Perspective; Barcelona Publishers: Dallas, TX, USA, 2016; pp. 11–37. [Google Scholar]
- Birnbaum, J.C. Intersubjectivity and nordoff-robbins music therapy. Music Ther. Perspect. 2014, 32, 30–37. [Google Scholar] [CrossRef]
- Stige, B. Culture-Centered Music Therapy; Barcelona Publications: Gilsum, NH, USA, 2002; pp. 105–107. [Google Scholar]
- Small, C. Musicking—The meanings of performing and listening. A lecture. Music Educ. Res. 1999, 1, 9–22. [Google Scholar] [CrossRef]
- DeNora, T. The pebble in the pond: Musicing, therapy, community. Nord. J. Music Ther. 2005, 14, 57–66. [Google Scholar] [CrossRef]
- Robb, S.L.; Clair, A.A.; Watanabe, M.; Monahan, P.O.; Azzouz, F.; Stouffer, J.W.; Ebberts, A.; Darsie, E.; Whitmer, C.; Walker, J.; et al. A non-randomized [corrected] controlled trial of the active music engagement (ame) intervention on children with cancer. Psychooncology 2008, 17, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.N.; Nilsson, S.; Hellstrom, A.L.; Bengtson, A. Music therapy to reduce pain and anxiety in children with cancer undergoing lumbar puncture: A randomized clinical trial. J. Pediatr. Oncol. Nurs. 2010, 27, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Barrera, M.E.; Rykov, M.H.; Doyle, S.L. The effects of interactive music therapy on hospitalized children with cancer: A pilot study. Psychooncology 2002, 11, 379–388. [Google Scholar] [CrossRef]
- Tucquet, B.; Leung, M. Music therapy services in pediatric oncology: A national clinical practice review. J. Pediatr. Oncol. Nurs. 2014, 31, 327–338. [Google Scholar] [CrossRef]
- Robb, S.L.; Ebberts, A.G. Songwriting and digital video production interventions for pediatric patients undergoing bone marrow transplantation, part I: An analysis of depression and anxiety levels according to phase of treatment. J. Pediatr. Oncol. Nurs. 2003, 20, 2–15. [Google Scholar] [CrossRef]
- Robb, S.L.; Burns, D.S.; Stegenga, K.A.; Haut, P.R.; Monahan, P.O.; Meza, J.; Stump, T.E.; Cherven, B.O.; Docherty, S.L.; Hendricks-Ferguson, V.L.; et al. Randomized clinical trial of therapeutic music video intervention for resilience outcomes in adolescents/young adults undergoing hematopoietic stem cell transplant: A report from the children’s oncology group. Cancer 2014, 120, 909–917. [Google Scholar] [CrossRef]
- Uggla, L.; Bonde, L.O.; Svahn, B.M.; Remberger, M.; Wrangsjö, B.; Gustafsson, B. Music therapy can lower the heart rates of severely sick children. Acta Paediatr. 2016, 105, 1225–1230. [Google Scholar] [CrossRef] [PubMed]
- Uggla, L.; Bonde, L.O.; Hammar, U.; Wrangsjo, B.; Gustafsson, B. Music therapy supported the health-related quality of life for children undergoing haematopoietic stem cell transplants. Acta Paediatr. 2018, 107, 1986–1994. [Google Scholar] [CrossRef] [PubMed]
- Trondalen, G. Bonde LO. Music Therapy: Models and Interventions. In Music, Health, and Wellbeing; MacDonald, R.A.R., Kreutz, G., Mitchell, L., Eds.; Oxford University Press: Oxford, UK, 2012; pp. 40–61. [Google Scholar]
- Fosha, D.; Siegel, D.J.; Solomon, M.F. The Healing Power of Emotion: Affective Neuroscience, Development, Clinical Practice; W.W. Norton & Co.: New York, NY, USA, 2009; pp. 132–133. [Google Scholar]
- Bonde, L.O.R. Musikterapi Teori Uddannelse Praksis Forskning en Håndbog om Musikterapi i Danmark; Klim: Århus, Danmark, 2014; p. 144. [Google Scholar]
- Murphy, K.; Wheeler, B.L. Music Therapy Research [Elektronisk Resurs], 3rd ed.; Barcelona Publishers: Dallas, TX, USA, 2016. [Google Scholar]
- Andersen, T.; Weine, B.; Hopstadius, K. Reflekterande Processer: Samtal och Samtal om Samtalen; Studentlitteratur: Lund, Sweden, 2011; pp. 149–162. [Google Scholar]
- Blom, K.M. Experiences of Transcendence and the Process of Surrender in Guided Imagery and Music (GIM). Ph.D. Thesis, Aalborg University, Aalborg, Denmark, 7 November 2014. [Google Scholar]
- Kvale, S.; Brinkmann, S. Interviews: Learning the Craft of Qualitative Research Interviewing, 2nd ed.; Sage Publications: Los Angeles, CA, USA, 2009. [Google Scholar]
- Andersen, T. Researching client-therapist relationships: A collaborative study for informing therapy. J. Syst. Ther. 1997, 16, 125–133. [Google Scholar] [CrossRef]
- Blom, K.M. Samspela, samtala, samforska—Om ömsesidiga processer I terapi och forskning. Fokus På Familien 2006, 34, 256–275. [Google Scholar]
- Fosha, D. The Transforming Power of Affect: A Model for Accelerated Change; Basic Books, Co.: New York, NY, USA, 2000; pp. 126–129, 146–148. [Google Scholar]
- Sander, L.W. Thinking differently principles of process in living systems and the specificity of being known. Psychoanal. Dialogues 2002, 12, 11–42. [Google Scholar] [CrossRef]
- Change in Psychotherapy: A Unifying Paradigm; W.W. Norton & Co.: New York, NY, USA, 2010; pp. 54–74.
- Tronick, E. The Neurobehavioral and Social Emotional Development of Infants and Children; W. W. Norton & Co.: New York, NY, USA, 2007; pp. 155–230, 397–500. [Google Scholar]
- Schore, A.N. Affect Regulation & the Repair of the Self; W.W. Norton: New York, NY, USA, 2003; pp. 151–278. [Google Scholar]
- Steele, K.; Boon, S.; van der Hart, O. Treating Trauma-Related Dissociation: A Practical, Integrative Approach; W. W. Norton & Company: New York, NY, USA, 2017. [Google Scholar]
- Bonde, L.O.; Blom, K.M. Music listening and the experience of surrender. In Cultural Psychology of Musical Experience; Information Age Publishing, Inc.: Charlotte, NC, USA, 2016; pp. 207–234. [Google Scholar]
- Fukunishi, I.; Tsuruta, T. Alexithymic characteristics in children with refractory hematological diseases. Psychosomatics 2001, 42, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Phipps, S.; Klosky, J.L.; Long, A.; Hudson, M.M.; Huang, Q.; Zhang, H.; Noll, R.B. Posttraumatic stress and psychological growth in children with cancer: Has the traumatic impact of cancer been overestimated? J. Clin. Oncol. 2014, 32, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Mårtenson Blom, K.; Wrangsjö, B. Intersubjektivitet: Det Mellanmänskliga i Vård och Vardag; Studentlitteratur: Lund, Sweden, 2013; p. 15. [Google Scholar]
- Bjørkvold, J.-R.; Nilsson, L.; Schollin-Borg, K. Den Musiska Människan; Runa: Stockholm, Sweden, 2005; pp. 26–29. [Google Scholar]
- Stern, D.N. Forms of Vitality: Exploring Dynamic Experience in Psychology, the Arts, Psychotherapy, and Development; Oxford University Press: Oxford, UK, 2010; pp. 3–18. [Google Scholar]


© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uggla, L.; Mårtenson Blom, K.; Bonde, L.O.; Gustafsson, B.; Wrangsjö, B. An Explorative Study of Qualities in Interactive Processes with Children and Their Parents in Music Therapy during and after Pediatric Hematopoietic Stem Cell Transplantation. Medicines 2019, 6, 28. https://doi.org/10.3390/medicines6010028
Uggla L, Mårtenson Blom K, Bonde LO, Gustafsson B, Wrangsjö B. An Explorative Study of Qualities in Interactive Processes with Children and Their Parents in Music Therapy during and after Pediatric Hematopoietic Stem Cell Transplantation. Medicines. 2019; 6(1):28. https://doi.org/10.3390/medicines6010028
Chicago/Turabian StyleUggla, Lena, Katarina Mårtenson Blom, Lars Ole Bonde, Britt Gustafsson, and Björn Wrangsjö. 2019. "An Explorative Study of Qualities in Interactive Processes with Children and Their Parents in Music Therapy during and after Pediatric Hematopoietic Stem Cell Transplantation" Medicines 6, no. 1: 28. https://doi.org/10.3390/medicines6010028