The Effectiveness of a Resilience Intervention Program on Emotional Intelligence of Adolescent Students with Hearing Loss


Abstract
:1. Introduction
2. Methods
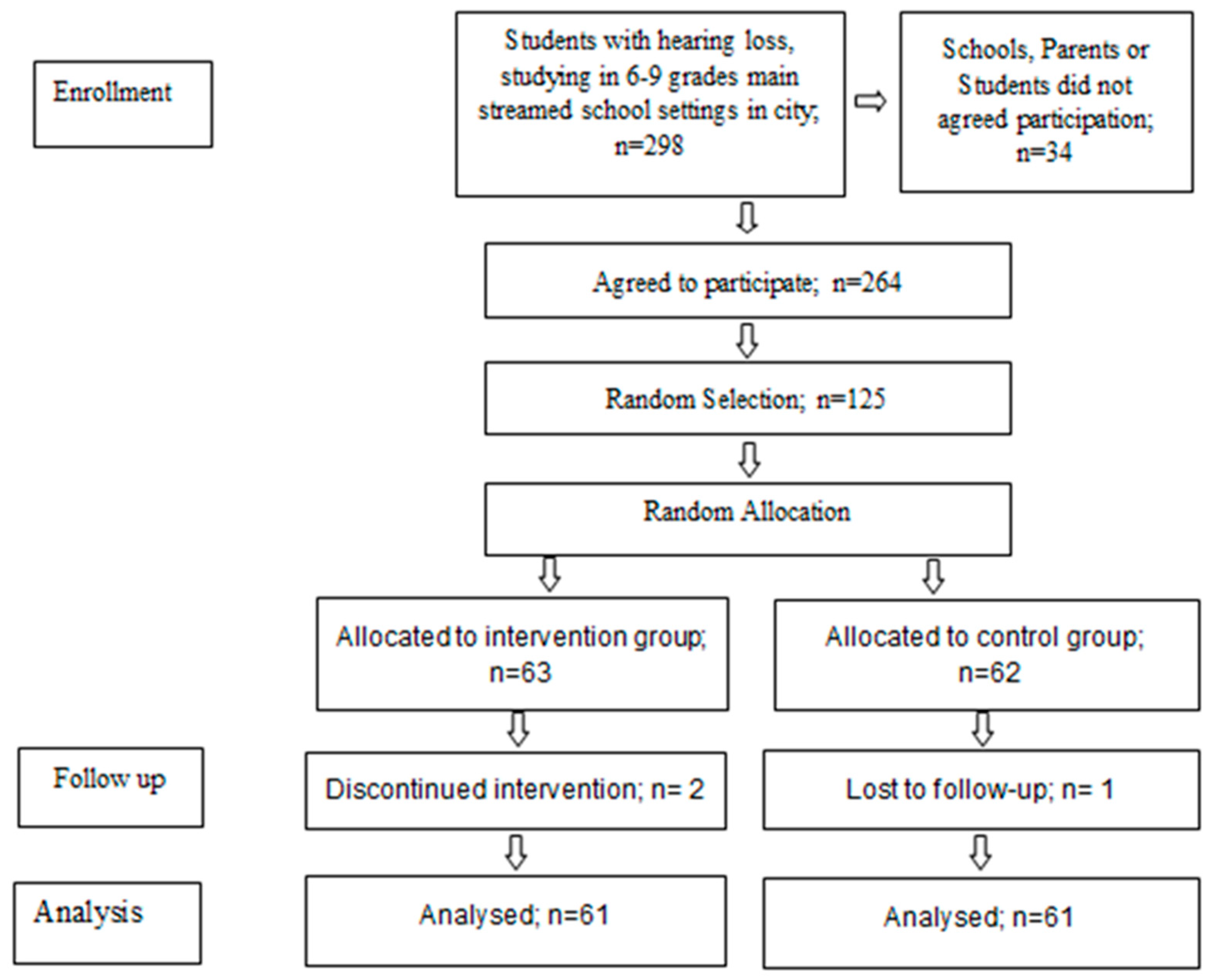
2.1. Participants
2.2. Measurements
2.2.1. Resilience Scale
2.2.2. Emotional Intelligence Scale
2.3. Intervention
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mayer, J.D. What is emotional intelligence? In Emotional Development and Emotional Intelligence: Implications for Educators; Salovey, P., Sluyter, D., Eds.; Basic Books: New York, NY, USA, 1997; pp. 3–31. [Google Scholar]
- Lukomski, J. Deaf college students’ perceptions of their social-emotional adjustment. J. Deaf Stud. Deaf Educ. 2007, 12, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, M.F.; Christenson, S.L.; Evelo, D.L.; Hurley, C.M. Dropout prevention for youth with disabilities: Efficacy of a sustained school engagement procedure. Except. Child. 1998, 65, 7–21. [Google Scholar] [CrossRef]
- Irvin, J.L.; Richardson, T.L. The importance of emotional intelligence during transition into middle school. Middle Sch. J. 2002, 33, 55–58. [Google Scholar] [CrossRef]
- Calderon, R.; Greenberg, M.T. Social and Emotional Development of Deaf Children. Family, School and Program Effects. In The Oxford Handbook of Deaf Studies, Language, and Education; Marschark, M., Spencer, P.E., Eds.; Oxford University Press: New York, NY, USA, 2003; pp. 177–189. [Google Scholar]
- Aras, I.; Stevanović, R.; Vlahović, S.; Stevanović, S.; Kolarić, B.; Kondić, L. Health related quality of life in parents of children with speech and hearing impairment. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Akram, B.; Hameed, B. Adaptive Emotional Abilities of Adolescents with Hearing Impairment. Pak. J. Psychol. Res. 2014, 29, 103–123. [Google Scholar]
- Dyck, M.J.; Farrugia, C.; Shochet, I.M.; Holmes-Brown, M. Emotion recognition/understanding ability in hearing or vision-impaired children: Do sounds, sights, or words make the difference? J. Child Psychol. Psychiatry 2004, 45, 789–800. [Google Scholar] [CrossRef]
- Jambor, E.; Elliott, M. Self-esteem and coping strategies among deaf students. J. Deaf Stud. Deaf Educ. 2005, 10, 63–81. [Google Scholar] [CrossRef]
- Fellinger, J.; Holzinger, D.; Sattel, H.; Laucht, M. Mental health and quality of life in deaf pupils. Eur. Child Adolesc. Psychiatry 2008, 17, 414–423. [Google Scholar] [CrossRef]
- Masten, A.S. Ordinary magic: Resilience processes in development. Am. Psychol. 2001, 56, 227–238. [Google Scholar] [CrossRef]
- Masten, A.S. Ordinary Magic: Resilience in Development; The Guilford Press: New York, NY, USA, 2014. [Google Scholar]
- Masten, A.S. Global perspectives on resilience in children and youth. Child Dev. 2014, 85, 6–20. [Google Scholar] [CrossRef]
- Masten, A.S. Resilience in children threatened by extreme adversity: Frameworks for research, practice, and translational synergy. Dev. Psychopathol. 2011, 23, 493–506. [Google Scholar] [CrossRef] [PubMed]
- Schneider, T.R.; Lyons, J.B.; Khazon, S. Emotional intelligence and resilience. Personal. Individ. Differ. 2013, 55, 909–914. [Google Scholar] [CrossRef]
- Armstrong, A.R.; Galligan, R.F.; Critchley, C.R. Emotional intelligence and psychological resilience to negative life events. Personal. Individ. Differ. 2011, 51, 331–336. [Google Scholar] [CrossRef]
- Folkman, S.; Moskowitz, J.T. Positive affect and the other side of coping. Am. Psychol. 2000, 55, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Barrett, L.F.; Gross, J.J. Emotional Intelligence: A Process Model of Emotion Representation and Regulation. In Emotions and Social Behavior. Emotions: Currrent Issues and Future Directions; Mayne, T.J., Bonanno, G.A., Eds.; Guilford Press: New York, NY, USA, 2001; pp. 286–310. [Google Scholar]
- Salovey, P.; Hsee, C.K.; Mayer, J.D. Emotional Intelligence and the Self-Regulation of Affect. In Century Psychology Series. Handbook of Mental Control; Wegner, D.M., Pennebaker, J.W., Eds.; Prentice-Hall, Inc.: Englewood Cliffs, NJ, USA, 1993; pp. 258–277. [Google Scholar]
- Goleman, D. Emotional Intelligence: Why It Can Matter More than IQ; Bantam Books: New York, NY, USA, 1995. [Google Scholar]
- Petrides, K.V.; Furnham, A. Trait emotional intelligence: Psychometric investigation with reference to established trait taxonomies. Eur. J. Personal. 2001, 15, 425–448. [Google Scholar] [CrossRef]
- Lazarus, R.S. From psychological stress to the emotions: A history of changing outlooks. Annu. Rev. Psychol. 1993, 44, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Tugade, M.M.; Fredrickson, B.L. Resilient individuals use positive emotions to bounce back from negative emotional experiences. J. Personal. Soc. Psychol. 2004, 86, 320–333. [Google Scholar] [CrossRef]
- Seligmana, M.; Ernstb, R.M.; Gillhamc, J.; Reivicha, K.; Linkins, M. Positive education: Positive psychology and classroom interventions. Oxf. Rev. Educ. 2009, 35, 293–311. [Google Scholar] [CrossRef]
- QUT Resourceful Adolescents Program (RAP-A). Available online: http://www.rap.qut.edu.au/programs/rap-a.jsp (accessed on 20 June 2017).
- Gilmore, L.; Campbell, M.; Shochet, I.; Garland, R.; Smyth, T.; Roberts, C.; West, D. Promoting resilience in children with intellectual disability: A randomized controlled trial in Australian schools. In Resilience Interventions for Youth in Diverse Populations; Prince-Embury, S., Saklofske, D.H., Eds.; Springer: New York, NY, USA, 2014; pp. 353–373. [Google Scholar]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.M.; Hall, L.E.; Haggerty, D.J.; Cooper, J.T.; Golden, C.J.; Dornheim, L. Development and validation of a measure of emotional intelligence. Personal. Individ. Differ. 1998, 25, 167–177. [Google Scholar] [CrossRef]
- Greenberg, M.T.; Kusché, C.A. Preventive intervention for school-age deaf children: The PATHS curriculum. J. Deaf Stud. Deaf Educ. 1998, 3, 49–63. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, G.; Feinn, R. Using Effect Size—Or Why the P Value Is Not Enough. J. Grad. Med. Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef] [PubMed]
- Claro, A.; Boulanger, M.-M.; Shaw, S.R. Targeting vulnerabilities to risky behavior: An intervention for promoting adaptive emotion regulation in adolescents. Contemp. Sch. Psychol. 2015, 19, 330–339. [Google Scholar] [CrossRef]
- Durlak, J.A.; Weissberg, R.P.; Dymnicki, A.B.; Taylor, R.D.; Schellinger, K.B. The impact of enhancing students’ social and emotional learning: A meta-analysis of school-based universal interventions. Child Dev. 2011, 82, 405–432. [Google Scholar] [CrossRef] [PubMed]
- Hodzic, S.; Scharfen, J.; Ripoll, P.; Holling, H.; Zenasni, F. How Efficient Are Emotional Intelligence Trainings: A Meta-Analysis. Emot. Rev. 2018, 10, 138–148. [Google Scholar] [CrossRef]
- Ugoani, J.N.N.; Akuezue, E.M. Imperatives of emotional intelligence on psychological wellbeing among adolescents. Am. J. Appl. Psychol. 2013, 1, 44–48. [Google Scholar]
- Pietzrak, W. Perception of the emotions of others by deaf schoolchildren. Dcfcktolopyz 1981, 4, 37–92. [Google Scholar]
- Al-Tal, S.; AL-Jawaldeh, F.; AL-Taj, H.; Maharmeh, L. Emotional Intelligence Levels of Students with Sensory Impairment. Int. Educ. Stud. 2017, 10, 145–153. [Google Scholar] [CrossRef]
- Izard, C.; Stark, K.; Trentacosta, C.; Schultz, D. Beyond Emotion Regulation: Emotion Utilization and Adaptive Functioning. Child Dev. Perspect. 2008, 2, 156–163. [Google Scholar] [CrossRef]
- Ruiz-Aranda, D.; Castillo, R.; Salguero, J.M.; Cabello, R.; Fernández-Berrocal, P.; Balluerka, N. Short and midterm effects of emotional intelligence training on adolescent mental health. J. Adolesc. Health 2012, 51, 462–467. [Google Scholar] [CrossRef]
- Nelis, D.; Quoidbach, J.; Mikolajczak, M.; Hansenne, M. Increasing emotional intelligence: (How) is it possible? Personal. Individ. Differ. 2009, 47, 36–41. [Google Scholar] [CrossRef]


{kind=link}
| EI Domain | Scoring Range | Control Group | Intervention Group | p-Value |
|---|---|---|---|---|
| Mean ± SD | Mean ± SD | |||
| Emotion regulation | 0–50 | 32.92 ± 5.67 | 32.15 ± 4.32 | NS * |
| Emotion Appraisal and Expression | 0–65 | 38.38 ± 5.80 | 38.06 ± 4.40 | NS |
| Emotion Utilization | 0–50 | 31.08 ± 5.27 | 31.65 ± 4.04 | NS |
| Total Emotional Intelligence score | 0–165 | 105.64 ± 14.51 | 105.00 ± 9.37 | NS |
| EI Domain | Scoring Range | Control Group | Intervention Group | p-Value | Effect Size |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | ||||
| Emotion regulation | 0–50 | 32.30 ± 4.16 | 37.48 ± 5.18 | <0.001 | 1.2 |
| Emotion Appraisal and Expression | 0–65 | 38.77 ± 3.94 | 44.16 ± 5.10 | <0.001 | 1.3 |
| Emotion Utilization | 0–50 | 32.69 ± 3.50 | 35.30 ± 4.22 | <0.001 | 0.7 |
| Total Emotional Intelligence score | 0–165 | 106.90 ± 9.27 | 120.79 ± 12.52 | <0.001 | 1.5 |
| EI Domain | Scoring Range | Control Group | Intervention Group | p-Value | Effect Size |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | ||||
| Emotion regulation | 0–50 | 33.51 ± 4.55 | 37.10 ± 3.44 | <0.001 | 0.8 |
| Emotion Appraisal and Expression | 0–65 | 38.56 ± 3.16 | 44.02 ± 3.75 | <0.001 | 1.7 |
| Emotion Utilization | 0–50 | 30.87 ± 3.58 | 33.75 ± 4.13 | <0.001 | 0.8 |
| Total Emotional Intelligence score | 0–165 | 105.15 ± 8.26 | 118.56 ± 8.33 | <0.001 | 1.6 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adibsereshki, N.; Hatamizadeh, N.; Sajedi, F.; Kazemnejad, A. The Effectiveness of a Resilience Intervention Program on Emotional Intelligence of Adolescent Students with Hearing Loss. Children 2019, 6, 48. https://doi.org/10.3390/children6030048
Adibsereshki N, Hatamizadeh N, Sajedi F, Kazemnejad A. The Effectiveness of a Resilience Intervention Program on Emotional Intelligence of Adolescent Students with Hearing Loss. Children. 2019; 6(3):48. https://doi.org/10.3390/children6030048
Chicago/Turabian StyleAdibsereshki, Narges, Nikta Hatamizadeh, Firoozeh Sajedi, and Anoshirvan Kazemnejad. 2019. "The Effectiveness of a Resilience Intervention Program on Emotional Intelligence of Adolescent Students with Hearing Loss" Children 6, no. 3: 48. https://doi.org/10.3390/children6030048