The Percentage of Free PSA and Urinary Markers Distinguish Prostate Cancer from Benign Hyperplasia and Contribute to a More Accurate Indication for Prostate Biopsy

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patients, Inflammation, Urine Collection and RNA Isolation
2.2. Reverse Transcription and Quantitative Polymerase Chain Reaction
2.3. Dilution of LNCaP Cells and Leukocytes
2.4. Statistical Analysis
3. Results
3.1. Urine KLK3 Strongly Correlates with Prostate Cancer Relevant Transcripts
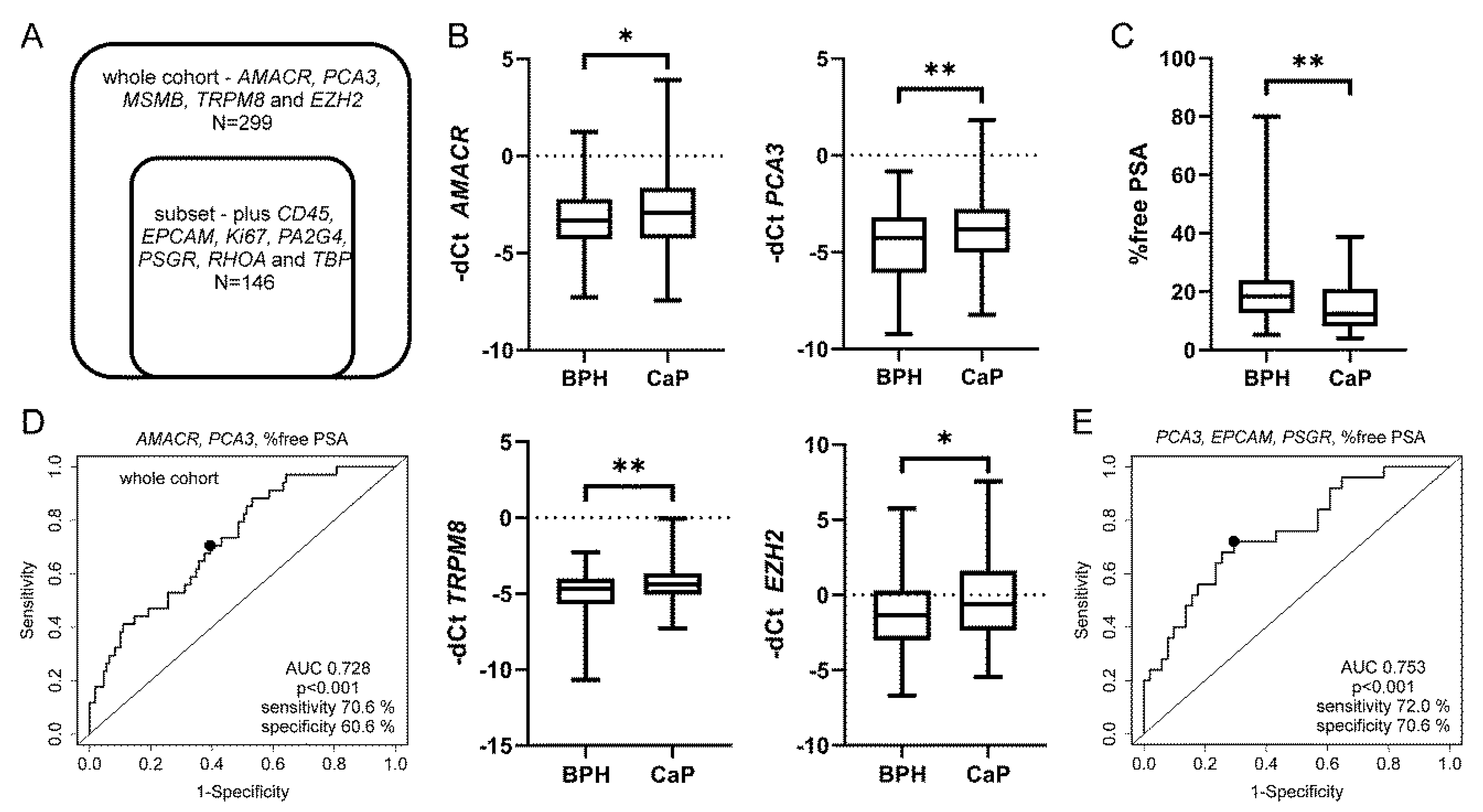
3.2. Urine PCA3, AMACR and Percentage of Free PSA Discriminate CaP from BPH
3.3. The Best Combined Model was Achieved for EPCAM, PSGR, PCA3 and Percentage of Free PSA in the Subset of Patients
3.4. Prostate Inflammation in BPH Increases Urine PCA3 but Does Not Affect Prostate Biopsy Decision Making
3.5. The qRT-PCR Assay Detects Relevant Numbers of Leukocytes and Cancer Cells in Urine
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pereira-Azevedo, N.; Verbeek, J.F.M.; Nieboer, D.; Bangma, C.H.; Roobol, M.J. Head-to-head comparison of prostate cancer risk calculators predicting biopsy outcome. Transl. Androl. Urol. 2018, 7, 18–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raja, N.; Russell, C.M.; George, A.K. Urinary markers aiding in the detection and risk stratification of prostate cancer. Transl. Androl. Urol. 2018, 7, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Cucchiara, V.; Cooperberg, M.R.; Dall’Era, M.; Lin, D.W.; Montorsi, F.; Schalken, J.A.; Evans, C.P. Genomic Markers in Prostate Cancer Decision Making. Eur. Urol. 2018, 73, 572–582. [Google Scholar] [CrossRef]
- Kearns, J.T.; Lin, D.W. Improving the Specificity of PSA Screening with Serum and Urine Markers. Curr. Urol. Rep. 2018, 19, 80. [Google Scholar] [CrossRef] [PubMed]
- Stephan, C.; Ralla, B.; Jung, K. Prostate-specific antigen and other serum and urine markers in prostate cancer. Biochim. Biophys. Acta Rev. Cancer 2014, 1846, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, A.; Mahon, J.; Boland, A.; Beale, S.; Dwan, K.; Fleeman, N.; Hockenhull, J.; Dundar, Y. The clinical effectiveness and cost-effectiveness of the PROGENSA(R) prostate cancer antigen 3 assay and the Prostate Health Index in the diagnosis of prostate cancer: A systematic review and economic evaluation. Health Technol. Assess. 2015, 19, 1–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parekh, D.J.; Punnen, S.; Sjoberg, D.D.; Asroff, S.W.; Bailen, J.L.; Cochran, J.S.; Concepcion, R.; David, R.D.; Deck, K.B.; Dumbadze, I.; et al. A multi-institutional prospective trial in the USA confirms that the 4Kscore accurately identifies men with high-grade prostate cancer. Eur. Urol. 2015, 68, 464–470. [Google Scholar] [CrossRef]
- Vickers, A.J.; Eastham, J.A.; Scardino, P.T.; Lilja, H. The Memorial Sloan Kettering Cancer Center Recommendations for Prostate Cancer Screening. Urology 2016, 91, 12–18. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Perlis, N.; Al-Kasab, T.; Ahmad, A.; Goldberg, E.; Fadak, K.; Sayyid, R.; Finelli, A.; Kulkarni, G.; Hamilton, R.; Zlotta, A.; et al. Defining a Cohort that May Not Require Repeat Prostate Biopsy Based on PCA3 Score and Magnetic Resonance Imaging: The Dual Negative Effect. J. Urol. 2018, 199, 1182–1187. [Google Scholar] [CrossRef]
- Smith, B.; Agarwal, P.; Bhowmick, N.A. MicroRNA applications for prostate, ovarian and breast cancer in the era of precision medicine. Endocr. Relat. Cancer 2017, 24, R157–R172. [Google Scholar] [CrossRef] [PubMed]
- Helsmoortel, H.; Everaert, C.; Lumen, N.; Ost, P.; Vandesompele, J. Detecting long non-coding RNA biomarkers in prostate cancer liquid biopsies: Hype or hope? Non-Coding RNA Res. 2018, 3, 64–74. [Google Scholar] [CrossRef]
- Larsen, L.K.; Jakobsen, J.S.; Abdul-Al, A.; Guldberg, P. Noninvasive Detection of High Grade Prostate Cancer by DNA Methylation Analysis of Urine Cells Captured by Microfiltration. J. Urol. 2018, 200, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Kral, M.; Grepl, M.; Hruska, F.; Hradil, D.; Rajmon, P.; Student, V.; Knillova, J.; Bouchal, J. Effect of prostatic tissue inflammation on prostate cancer markers in urine. Eur. Urol. Suppl. 2015, 14, e1285. [Google Scholar] [CrossRef]
- De Luca, S.; Passera, R.; Fiori, C.; Bollito, E.; Cappia, S.; Mario Scarpa, R.; Sottile, A.; Rondone, D.F.; Porpiglia, F. Prostate health index and prostate cancer gene 3 score but not percent-free Prostate Specific Antigen have a predictive role in differentiating histological prostatitis from PCa and other nonneoplastic lesions (BPH and HG-PIN) at repeat biopsy. Urol. Oncol. 2015, 33, 424.e17–424.e23. [Google Scholar] [CrossRef] [PubMed]
- Smelov, V.; Novikov, A.; Brown, L.J.; Eklund, C.; Strokova, L.; Ouburg, S.; Morre, S.A.; Dillner, J. False-positive prostate cancer markers in a man with symptomatic urethral Chlamydia trachomatis infection. Int. J. STD AIDS 2013, 24, 501–502. [Google Scholar] [CrossRef]
- Sequeiros, T.; Bastaros, J.M.; Sanchez, M.; Rigau, M.; Montes, M.; Placer, J.; Planas, J.; de Torres, I.; Pegtel, D.M.; Doll, A.; et al. Urinary biomarkers for the detection of prostate cancer in patients with high-grade prostatic intraepithelial neoplasia. Prostate 2015, 75, 1102–1113. [Google Scholar] [CrossRef]
- Jamaspishvili, T.; Kral, M.; Khomeriki, I.; Vyhnankova, V.; Mgebrishvili, G.; Student, V.; Kolar, Z.; Bouchal, J. Quadriplex model enhances urine-based detection of prostate cancer. Prostate Cancer Prostatic Dis. 2011, 14, 354–360. [Google Scholar] [CrossRef] [Green Version]
- Fujita, K.; Pavlovich, C.P.; Netto, G.J.; Konishi, Y.; Isaacs, W.B.; Ali, S.; De Marzo, A.; Meeker, A.K. Specific detection of prostate cancer cells in urine by multiplex immunofluorescence cytology. Hum. Pathol. 2009, 40, 924–933. [Google Scholar] [CrossRef] [Green Version]
- Joosse, S.A.; Gorges, T.M.; Pantel, K. Biology, detection and clinical implications of circulating tumor cells. EMBO Mol. Med. 2015, 7, 1–11. [Google Scholar] [CrossRef]
- Cao, C.; Wang, Q.; Li, Q.; Zhao, Q.; Wang, J.Q.; Liu, Y. Development and Preliminary Clinical Application of Circulating Tumor Cell Detection System for Prostate Cancer. J. Biomed. Nanotechnol. 2019, 15, 612–620. [Google Scholar] [CrossRef]
- Zhang, Y.; Linn, D.; Liu, Z.; Melamed, J.; Tavora, F.; Young, C.Y. EBP1, an Erb3—Binding protein, is decreased in prostate cancer and implicated in hormone resistance. Mol. Cancer Ther. 2008, 7, 3176–3186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hessels, D.; Klein Gunnewiek, J.M.T.; van Oort, I.; Karthaus, H.F.M.; van Leenders, G.J.L.; van Balken, B.; Kiemeney, L.A.; Witjes, J.A.; Schalken, J.A. DD3(PCA3)-based molecular urine analysis for the diagnosis of prostate cancer. Eur. Urol. 2003, 44, 8–16. [Google Scholar] [CrossRef]
- Kucerova, R.; Bienova, M.; Kral, M.; Bouchal, J.; Trtkova, K.S.; Burdova, A.; Student, V.; Kolar, Z. Androgenetic alopecia and polymorphism of the androgen receptor gene (SNP rs6152) in patients with benign prostate hyperplasia or prostate cancer. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.L.; Gaido, L. Laboratory diagnosis of urinary tract infections in adult patients. Clin. Infect. Dis. 2004, 38, 1150–1158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dos Santos, J.C.; Weber, L.P.; Perez, L.R.R. Evaluation of urinalysis parameters to predict urinary-tract infection. Braz. J. Infect. Dis. 2007, 11, 479–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musher, D.M.; Thorsteinsson, S.B.; Airola, V.M., II. Quantitative urinalysis. Diagnosing urinary tract infection in men. JAMA 1976, 236, 2069–2072. [Google Scholar] [CrossRef] [PubMed]
- Ploussard, G.; Haese, A.; van Poppel, H.; Marberger, M.; Stenzl, A.; Mulders, P.F.A.; Huland, H.; Bastien, L.; Abbou, C.-C.; Remzi, M.; et al. The prostate cancer gene 3 (PCA3) urine test in men with previous negative biopsies: Does free-to-total prostate-specific antigen ratio influence the performance of the PCA3 score in predicting positive biopsies? BJU Int. 2010, 106, 1143–1147. [Google Scholar] [CrossRef]
- Auprich, M.; Augustin, H.; Budäus, L.; Kluth, L.; Mannweiler, S.; Shariat, S.F.; Fisch, M.; Graefen, M.; Pummer, K.; Chun, F.K.-H. A comparative performance analysis of total prostate-specifi c antigen, percentage free prostate-specific antigen, prostate-specifi c antigen velocity and urinary prostate cancer gene 3 in the fi rst, second and third repeat prostate biopsy. BJU Int. 2012, 109, 1627–1635. [Google Scholar] [CrossRef]
- Leyten, G.H.J.M.; Hessels, D.; Jannink, S.A.; Smit, F.P.; de Jong, H.; Cornel, E.B.; de Reijke, T.M.; Vergunst, H.; Kil, P.; Knipscheer, B.C.; et al. Prospective multicentre evaluation of PCA3 and TMPRSS2-ERG gene fusions as diagnostic and prognostic urinary biomarkers for prostate cancer. Eur. Urol. 2014, 65, 534–542. [Google Scholar] [CrossRef]
- Van Neste, L.; Hendriks, R.J.; Dijkstra, S.; Trooskens, G.; Cornel, E.B.; Jannink, S.A.; de Jong, H.; Hessels, D.; Smit, F.P.; Melchers, W.J.G.; et al. Detection of High-grade Prostate Cancer Using a Urinary Molecular Biomarker-Based Risk Score. Eur. Urol. 2016, 70, 740–748. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, R.J.; van der Leest, M.M.G.; Dijkstra, S.; Barentsz, J.O.; Van Criekinge, W.; Hulsbergen-van de Kaa, C.A.; Schalken, J.K.; Mulders, P.F.A.; van Oort, I.M. A urinary biomarker-based risk score correlates with multiparametric MRI for prostate cancer detection. Prostate 2017, 77, 1401–1407. [Google Scholar] [CrossRef]
- McKiernan, J.; Donovan, M.J.; Margolis, E.; Partin, A.; Carter, B.; Brown, G.; Torkler, P.; Noerholm, M.; Skog, J.; Shore, N.; et al. A Prospective Adaptive Utility Trial to Validate Performance of a Novel Urine Exosome Gene Expression Assay to Predict High-grade Prostate Cancer in Patients with Prostate-specific Antigen 2-10ng/ml at Initial Biopsy. Eur. Urol. 2018, 74, 731–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomlins, S.A.; Day, J.R.; Lonigro, R.J.; Hovelson, D.H.; Siddiqui, J.; Kunju, L.P.; Dunn, R.L.; Meyer, S.; Hodge, P.; Groskopf, J.; et al. Urine TMPRSS2:ERG Plus PCA3 for Individualized Prostate Cancer Risk Assessment. Eur. Urol. 2016, 70, 45–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanda, M.G.; Feng, Z.; Howard, D.H.; Tomlins, S.A.; Sokoll, L.J.; Chan, D.W.; Regan, M.M.; Groskopf, J.; Chipman, J.; Patil, D.H.; et al. Association Between Combined TMPRSS2:ERG and PCA3 RNA Urinary Testing and Detection of Aggressive Prostate Cancer. JAMA Oncol. 2017, 3, 1085–1093. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Li, Y.; Li, X.; Jiang, M. Urinary Biomarker Panel to Improvement in Predicting Prostate Biopsy Result in Chinese Men with PSA 4-10 nj/mL. Biomed. Res. Int. 2017, 2017, 1–9. [Google Scholar]
- Deras, I.L.; Aubin, S.M.J.; Blase, A.; Day, J.R.; Koo, S.; Partin, A.W.; Ellis, W.J.; Marks, L.S.; Fradet, Y.; Rittenhouse, H.; et al. PCA3: A molecular urine assay for predicting prostate biopsy outcome. J. Urol. 2008, 179, 1587–1592. [Google Scholar] [CrossRef]
- De Luca, S.; Passera, R.; Milillo, A.; Coda, R.; Randone, D.F. Histological chronic prostatitis and high-grade prostate intra-epithelial neoplasia do not influence urinary prostate cancer gene 3 score. BJU Int. 2012, 110, 778–782. [Google Scholar] [CrossRef]
- Vlaeminck-Guillem, V.; Bandel, M.; Cottancin, M.; Rodriguez-Lafrasse, C.; Bohbot, J.-M.; Sednaoui, P. Chronic prostatitis does not influence urinary PCA3 score. Prostate 2012, 72, 549–554. [Google Scholar] [CrossRef]
- Schaeffer, E.M. Re: Chronic prostatitis does not influence urinary PCA3 score. J. Urol. 2012, 188, 2242. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Whole Cohort (n = 299) | Subset (n = 146) | ||
|---|---|---|---|---|
| BPH | CaP | BPH | CaP | |
| No. Patients | 178 | 121 | 78 | 68 |
| Age 1 | ||||
| <55 | 17 | 18 | 7 | 7 |
| 55–65 | 80 | 46 | 31 | 26 |
| >65 | 81 | 57 | 40 | 35 |
| Serum PSA (ng/mL) | ||||
| <2.5 | - | 10 | - | 6 |
| 2.5–10 | 147 | 111 | 63 | 62 |
| >10 | 31 | - | 15 | - |
| % free PSA 2 | ||||
| 0–10 | 18 | 12 | 11 | 9 |
| 11–20 | 49 | 16 | 20 | 12 |
| 21–100 | 48 | 8 | 24 | 5 |
| Inflammation 3 | ||||
| yes | 62 | - | 34 | - |
| no | 83 | - | 43 | - |
| n.a. | 33 | - | 1 | - |
| Gleason score | ||||
| <7 | - | 39 | - | 18 |
| 7 | - | 70 | - | 41 |
| >7 | - | 12 | - | 9 |
| Cancer stages 4 | ||||
| T1-pT2b | - | 38 | - | 18 |
| pT2c | - | 64 | - | 39 |
| pT3a-b | - | 19 | - | 11 |
| Risk groups 5 | ||||
| low | - | 26 | - | 10 |
| intermediate | - | 70 | - | 42 |
| high | - | 25 | - | 16 |
| KLK3 | AMACR | PCA3 | TRPM8 | MSMB | EZH2 | CD45 | EPCAM | Ki67 | RHOA | PA2G4 | PSGR | TBP | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| KLK3 | 1.000 | 0.720 | 0.791 | 0.863 | 0.895 | 0.292 | −0.092 | 0.489 | 0.154 | 0.192 | 0.433 | 0.826 | 0.169 |
| AMACR | 1.000 | 0.685 | 0.663 | 0.680 | 0.562 | 0.186 | 0.507 | 0.350 | 0.463 | 0.665 | 0.647 | 0.431 | |
| PCA3 | 1.000 | 0.770 | 0.682 | 0.274 | −0.027 | 0.426 | 0.191 | 0.240 | 0.411 | 0.747 | 0.225 | ||
| TRPM8 | 1.000 | 0.827 | 0.317 | 0.007 | 0.582 | 0.256 | 0.324 | 0.506 | 0.746 | 0.318 | |||
| MSMB | 1.000 | 0.403 | 0.050 | 0.462 | 0.184 | 0.266 | 0.474 | 0.711 | 0.215 | ||||
| EZH2 | 1.000 | 0.775 | 0.259 | 0.530 | 0.738 | 0.669 | 0.039 | 0.685 | |||||
| CD45 | 1.000 | 0.157 | 0.491 | 0.809 | 0.588 | −0.126 | 0.718 | ||||||
| EPCAM | 1.000 | 0.500 | 0.425 | 0.496 | 0.368 | 0.457 | |||||||
| Ki67 | 1.000 | 0.586 | 0.624 | 0.075 | 0.626 | ||||||||
| RHOA | 1.000 | 0.819 | 0.105 | 0.926 | |||||||||
| PA2G4 | 1.000 | 0.384 | 0.827 | ||||||||||
| PSGR | 1.000 | 0.126 | |||||||||||
| TBP | 1.000 |
| Univariate Logistic Analysis | ROC Analysis | ||||
| Variable | β | OR (95% CI) | p-Value | AUC (95% CI) | p-Value |
| AMACR | 0.168 | 1.183 (1.031–1.357) | 0.017 | 0.569 (0.502–0.635) | 0.023 |
| PCA3 | 0.233 | 1.263 (1.09–1.463) | 0.002 | 0.602 (0.533–0.667) | 0.002 |
| TRPM8 | 0.341 | 1.406 (1.143–1.73) | 0.001 | 0.599 (0.532–0.664) | 0.003 |
| MSMB | 0.07 | 1.072 (0.883–1.303) | 0.482 | 0.526 (0.458–0.594) | 0.223 |
| EZH2 | 0.127 | 1.136 (1.037–1.244) | 0.006 | 0.587 (0.519–0.653) | 0.007 |
| EPCAM | 0.141 | 1.152 (0.991–1.338) | 0.065 | 0.585 (0.488–0.674) | 0.042 |
| PSGR | 0.127 | 1.135 (0.888–1.451) | 0.311 | 0.532 (0.44–0.633) | 0.255 |
| % free PSA | −0.075 | 0.928 (0.879–0.98) | 0.007 | 0.666 (0.559−0.763) | 0.001 |
| Multivariate Logistic Analysis | ROC Analysis | ||||
| Whole Cohort | β | OR (95% CI) | p-Value | AUC (95% CI) | p-Value |
| age | 0.043 | 1.044 (0.97–1.123) | 0.256 | 0.728 (0.633–0.816) | <0.001 |
| AMACR | 0.244 | 1.277 (0.943–1.729) | 0.114 | ||
| PCA3 | 0.283 | 1.327 (1.01–1.742) | 0.042 | ||
| % free PSA | −0.082 | 0.921 (0.871–0.975) | 0.004 | ||
| Subset | β | OR (95% CI) | p-Value | AUC (95% CI) | p-Value |
| PCA3 | 0.439 | 1.551 (1.092–2.205) | 0.014 | 0.753 (0.642–0.862) | <0.001 |
| EPCAM | 0.207 | 1.23 (0.935–1.619) | 0.139 | ||
| PSGR | −0.151 | 0.86 (0.578–1.278) | 0.454 | ||
| % free PSA | −0.064 | 0.938 (0.877–1.004) | 0.064 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huskova, Z.; Knillova, J.; Kolar, Z.; Vrbkova, J.; Kral, M.; Bouchal, J. The Percentage of Free PSA and Urinary Markers Distinguish Prostate Cancer from Benign Hyperplasia and Contribute to a More Accurate Indication for Prostate Biopsy. Biomedicines 2020, 8, 173. https://doi.org/10.3390/biomedicines8060173
Huskova Z, Knillova J, Kolar Z, Vrbkova J, Kral M, Bouchal J. The Percentage of Free PSA and Urinary Markers Distinguish Prostate Cancer from Benign Hyperplasia and Contribute to a More Accurate Indication for Prostate Biopsy. Biomedicines. 2020; 8(6):173. https://doi.org/10.3390/biomedicines8060173
Chicago/Turabian StyleHuskova, Zlata, Jana Knillova, Zdenek Kolar, Jana Vrbkova, Milan Kral, and Jan Bouchal. 2020. "The Percentage of Free PSA and Urinary Markers Distinguish Prostate Cancer from Benign Hyperplasia and Contribute to a More Accurate Indication for Prostate Biopsy" Biomedicines 8, no. 6: 173. https://doi.org/10.3390/biomedicines8060173