

Long-Term Response to Tyrosine Kinase Inhibitors for Metastatic Renal Cell Carcinoma

 , ,
, ,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Schedule Treatment
2.2. Outcome Assessment and Statistical Analysis
3. Results
3.1. Patient’s Features According to Duration of Response
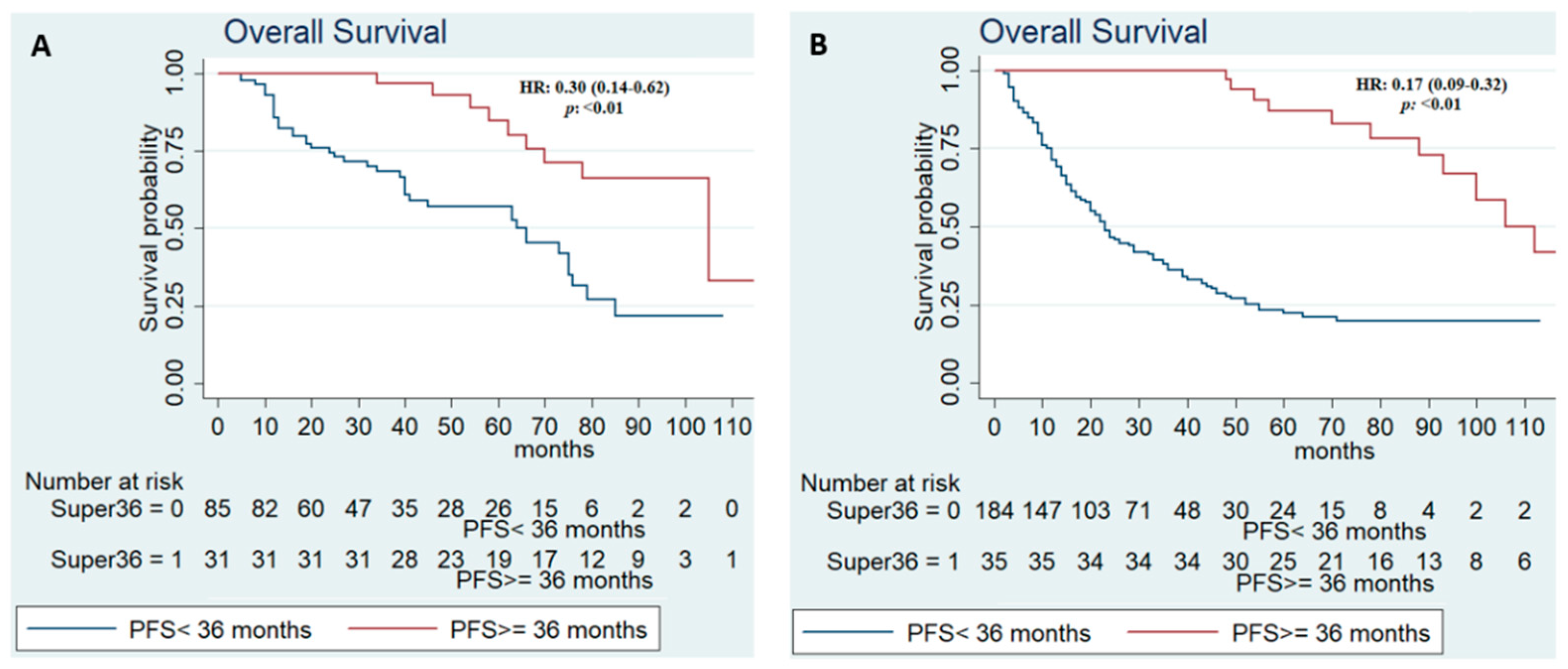
3.2. Patients Features According to Duration of Response and IMDC Score Risk
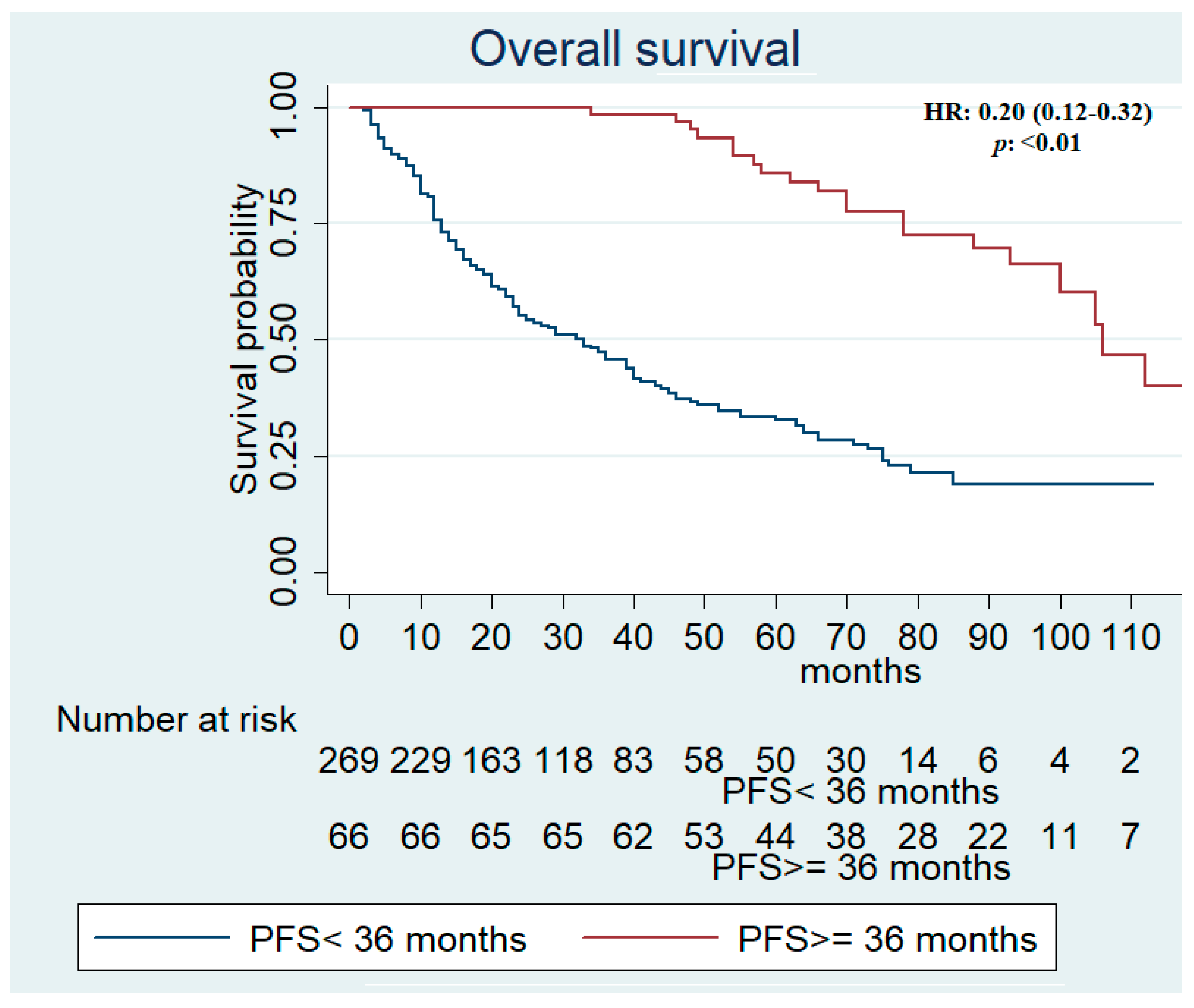
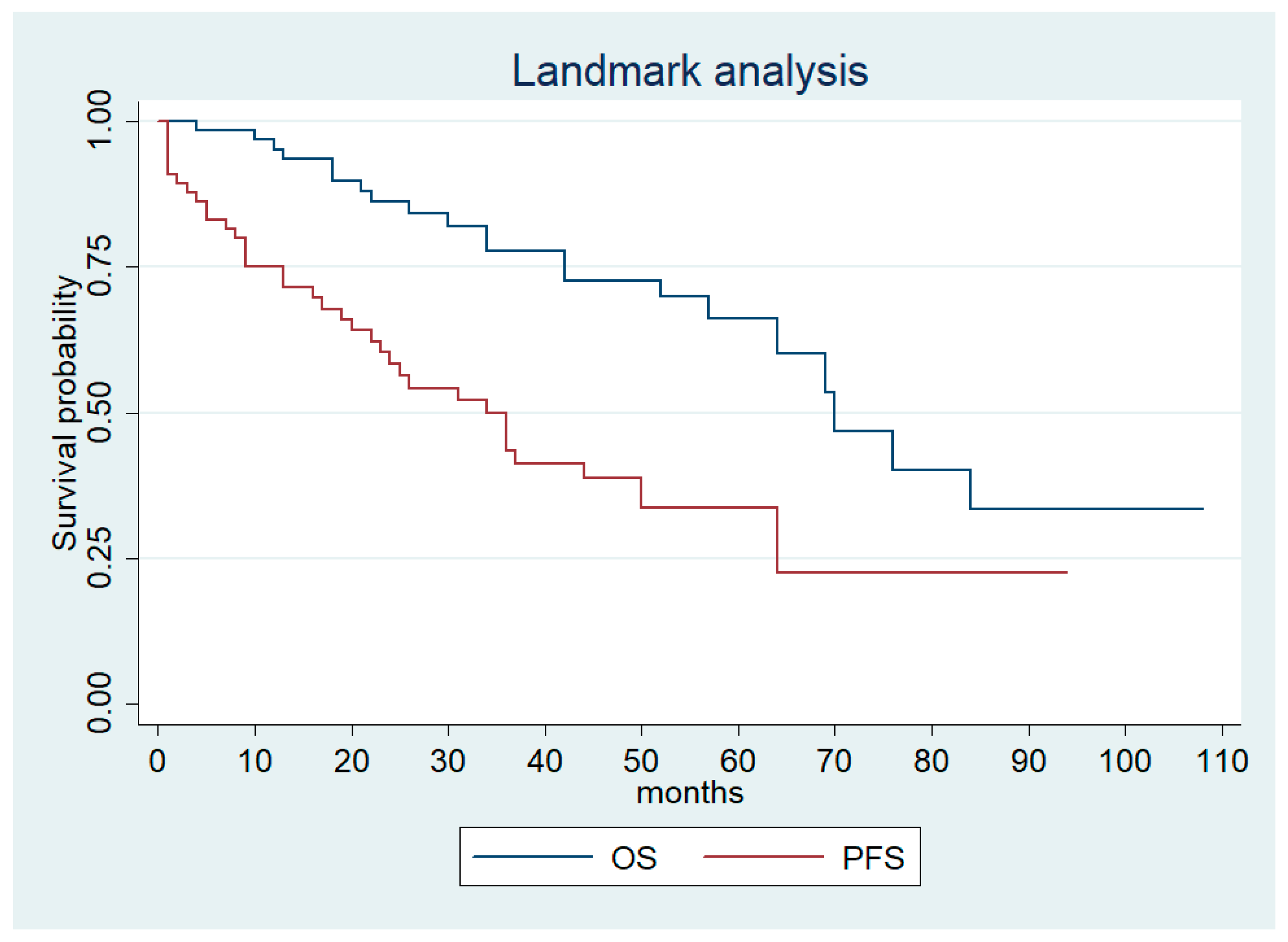
3.3. Response Rate and Outcome Efficacy
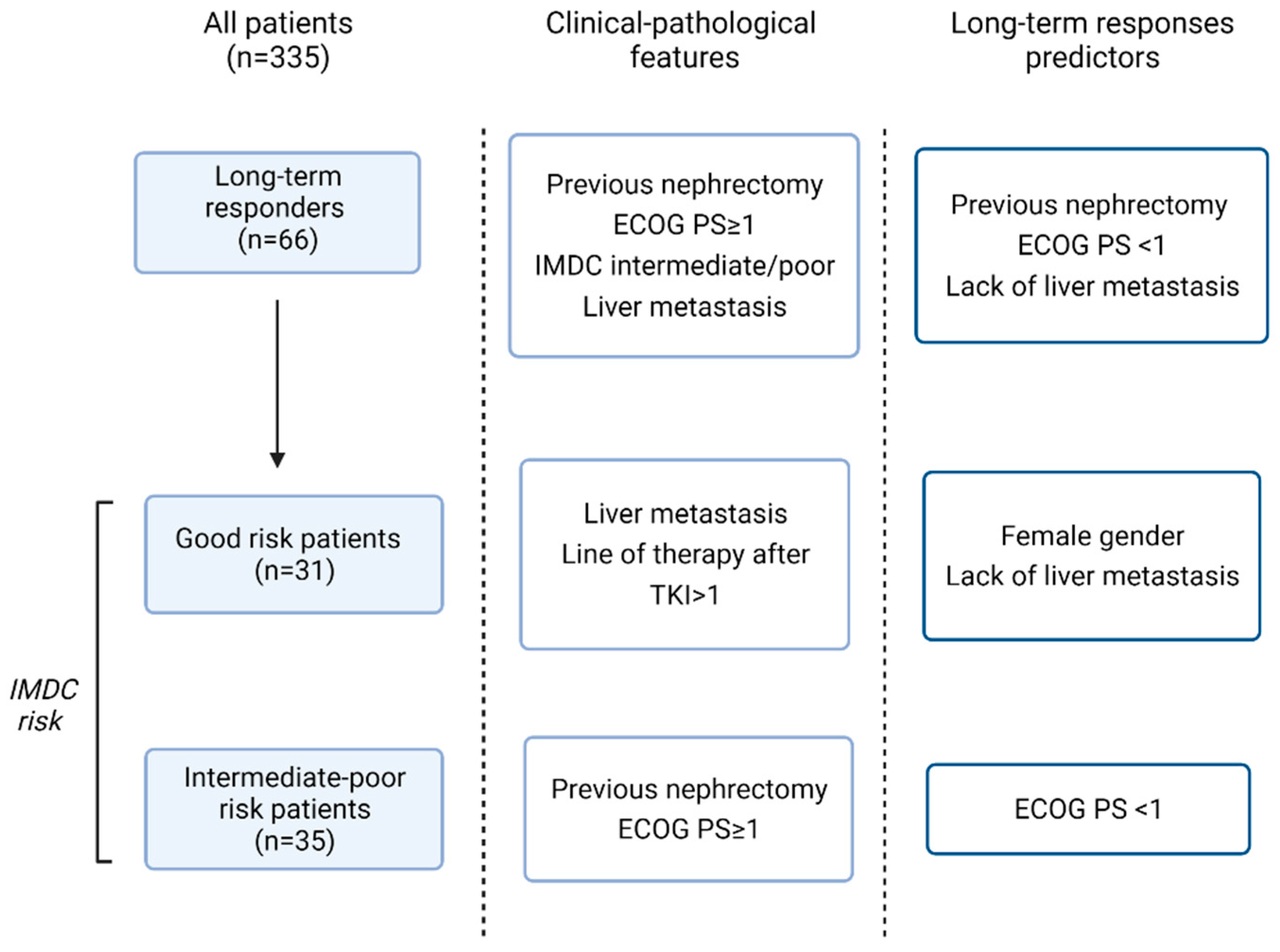
3.4. Long-Term Response Predictors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hsieh, J.J.; Purdue, M.P.; Signoretti, S.; Swanton, C.; Albiges, L.; Schmidinger, M.; Heng, D.Y.; Larkin, J.; Ficarra, V. Renal cell carcinoma. Nat. Rev. Dis. Primers 2017, 3, 17009. [Google Scholar] [CrossRef]
- Bedke, J.; Albiges, L.; Capitanio, U.; Giles, R.H.; Hora, M.; Lam, T.B.; Ljungberg, B.; Marconi, L.; Klatte, T.; Volpe, A.; et al. The 2021 Updated European Association of Urology Guidelines on Renal Cell Carcinoma: Immune Checkpoint Inhibitor–based Combination Therapies for Treatment-naive Metastatic Clear-cell Renal Cell Carcinoma Are Standard of Care. Eur. Urol. 2021, 80, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Powles, T.; Burotto, M.; Escudier, B.; Bourlon, M.T.; Shah, A.Y.; Suárez, C.; Hamzaj, A.; Porta, C.; Hocking, C.M.; et al. Nivolumab plus cabozantinib versus sunitinib in first-line treatment for advanced renal cell carcinoma (CheckMate 9ER): Long-term follow-up results from an open-label, randomised, phase 3 trial. Lancet Oncol. 2022, 23, 888–898. [Google Scholar] [CrossRef]
- Powles, T.; Plimack, E.R.; Soulières, D.; Waddell, T.; Stus, V.; Gafanov, R.; Nosov, D.; Pouliot, F.; Melichar, B.; Vynnychenko, I.; et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): Extended follow-up from a randomised, open-label, phase 3 trial. Lancet Oncol. 2020, 21, 1563–1573. [Google Scholar] [CrossRef]
- Tannir, N.M.; McDermott, D.F.; Escudier, B.; Hammers, H.J.; Aren, O.R.; Plimack, E.R.; Barthelemy, P.; Neiman, V.; George, S.; Porta, C.; et al. Overall survival and independent review of response in CheckMate 214 with 42-month follow-up: First-line nivolumab + ipilimumab (N+I) versus sunitinib (S) in patients (pts) with advanced renal cell carcinoma (aRCC). J. Clin. Oncol. 2020, 38, 609. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Arén Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Oudard, S.; Negrier, S.; Szczylik, C.; Pili, R.; Bjarnason, G.A.; et al. Overall survival and updated results for sunitinib compared with interferon alfa in patients with metastatic renal cell carcinoma. J. Clin. Oncol. 2009, 27, 3584–3590. [Google Scholar] [CrossRef]
- Motzer, R.J.; Hutson, T.E.; Cella, D.; Reeves, J.; Hawkins, R.; Guo, J.; Nathan, P.; Staehler, M.; de Souza, P.; Merchan, J.R.; et al. Pazopanib versus Sunitinib in Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2013, 369, 722–731. [Google Scholar] [CrossRef]
- Schwartz, L.H.; Litière, S.; De Vries, E.; Ford, R.; Gwyther, S.; Mandrekar, S.; Shankar, L.; Bogaerts, J.; Chen, A.; Dancey, J.; et al. RECIST 1.1—Update and clarification: From the RECIST committee. Eur. J. Cancer 2016, 62, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Motzer, R.J.; Hutson, T.E.; Tomczak, P.; Michaelson, M.D.; Bukowski, R.M.; Rixe, O.; Oudard, S.; Negrier, S.; Szczylik, C.; Kim, S.T.; et al. Sunitinib versus Interferon Alfa in Metastatic Renal-Cell Carcinoma. N. Engl. J. Med. 2007, 356, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Schmidinger, M.; Pichler, R.; Loidl, W.; Bauernhofer, T.; Kretz, M.; Tinchon, C.; Niedersüß-Beke, D.; Pfleger, G.; Wiesinger, C.G.; Vogl, U.; et al. Real-World Evidence Data on Metastatic Renal-Cell Carcinoma Treatment in Austria: The RELACS Study. Clin. Genitourin. Cancer 2019, 17, e957–e967. [Google Scholar] [CrossRef]
- Isaacsson Velho, P.; Nardo, M.; de Azevedo Souza, M.C.L.; Bonadio, R.R.C.C.; Marta, G.N.; Muniz, D.Q.B.; Bastos, D.A.; Dzik, C. Analysis of Efficacy and Toxicity Profile of First-Line Sunitinib or Pazopanib in Metastatic Clear Cell Renal Cell Carcinoma in the Brazilian Population. J. Glob. Oncol. 2018, 4, JGO-18. [Google Scholar] [CrossRef]
- Lalani, A.K.A.; Li, H.; Heng, D.Y.C.; Wood, L.; Kalirai, A.; Bjarnason, G.A.; Sim, H.W.; Kollmannsberger, C.K.; Kapoor, A.; Hotte, S.J.; et al. First-line sunitinib or pazopanib in metastatic renal cell carcinoma: The Canadian experience. J. Can. Urol. Assoc. 2017, 11, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Morales, J.M.; Swierkowski, M.; Wells, J.C.; Fraccon, A.P.; Pasini, F.; Donskov, F.; Bjarnason, G.A.; Lee, J.L.; Sim, H.W.; Sliwczynsk, A.; et al. First-line sunitinib versus pazopanib in metastatic renal cell carcinoma: Results from the International Metastatic Renal Cell Carcinoma Database Consortium. Eur. J. Cancer 2016, 65, 102–108. [Google Scholar] [CrossRef]
- Pal, S.K.; Ghate, S.R.; Li, N.; Swallow, E.; Peeples, M.; Zichlin, M.L.; Perez, J.R.; Agarwal, N.; Vogelzang, N.J. Real-World Survival Outcomes and Prognostic Factors Among Patients Receiving First Targeted Therapy for Advanced Renal Cell Carcinoma: A SEER–Medicare Database Analysis. Clin. Genitourin. Cancer 2017, 15, e573–e582. [Google Scholar] [CrossRef]
- Gul, Z.G.; Liaw, C.W.; Mehrazin, R. Gender Differences in Incidence, Diagnosis, Treatments, and Outcomes in Clinically Localized Bladder and Renal Cancer. Urology 2021, 151, 176–181. [Google Scholar] [CrossRef]
- Molina, A.M.; Jia, X.; Feldman, D.R.; Hsieh, J.J.; Ginsberg, M.S.; Velasco, S.; Patil, S.; Motzer, R.J. Long-term response to sunitinib therapy for metastatic renal cell carcinoma. Clin. Genitourin. Cancer 2013, 11, 297–302. [Google Scholar] [CrossRef]
- Mustafa, E.; Bivas, B.; Pongwut, D.; Lingwu, C.; Wong, Y.F.; Hashem, T.; Lim, C.S.; Karabulut, B.; Chung, H.J.; Chikatapu, C.; et al. Prospective observational study on Pazopanib in patients treated for advanced or metastatic renal cell carcinoma in countries in Asia Pacific, North Africa, and Middle East regions: PARACHUTE study. BMC Cancer 2021, 21, 1021. [Google Scholar] [CrossRef]
- Heng, D.Y.C.; Rini, B.I.; Garcia, J.; Wood, L.; Bukowski, R.M. Prolonged complete responses and near-complete responses to sunitinib in metastatic renal cell carcinoma. Clin. Genitourin. Cancer 2007, 5, 446–451. [Google Scholar] [CrossRef]
- Albiges, L.; Oudard, S.; Negrier, S.; Caty, A.; Gravis, G.; Joly, F.; Duclos, B.; Geoffrois, L.; Rolland, F.; Guillot, A.; et al. Complete remission with tyrosine kinase inhibitors in renal cell carcinoma. J. Clin. Oncol. 2012, 30, 482–487. [Google Scholar] [CrossRef]
- Motzer, R.J.; Escudier, B.; Gannon, A.; Figlin, R.A. Sunitinib: Ten Years of Successful Clinical Use and Study in Advanced Renal Cell Carcinoma. Oncologist 2017, 22, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Cella, D.; Beaumont, J.L. Pazopanib in the treatment of advanced renal cell carcinoma. Ther. Adv. Urol. 2016, 8, 61–69. [Google Scholar] [CrossRef] [PubMed]
- eUpdate—Renal Cell Carcinoma Treatment Recommendations|ESMO. Available online: https://www.esmo.org/guidelines/guidelines-by-topic/genitourinary-cancers/renal-cell-carcinoma/eupdate-renal-cell-carcinoma-treatment-recommendations-4 (accessed on 31 July 2022).
- Izzedine, H.; Mathian, A.; Champiat, S.; Picard, C.; Mateus, C.; Routier, E.; Varga, A.; Malka, D.; Leary, A.; Michels, J.; et al. Renal toxicities associated with pembrolizumab. Clin. Kidney J. 2019, 12, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | PFS ≥ 36 Months | PFS < 36 Months | p | |
|---|---|---|---|---|
| N = 335 | N = 66 (19.7%) | N = 269 (80.3%) | ||
| Age | 0.9 | |||
| Median (range) | 66 (37–89) | 67 (37–85) | 66 (37–89) | |
| Gender,n (%) | 0.1 | |||
| Male | 240 (71.6) | 43 (65.1) | 197 (73.2) | |
| Histology,n (%) | 0.4 | |||
| Clear-cell RCC | 294 (87.8) | 59 (89.4) | 235 (87.4%) | |
| Previous nephrectomy,n (%) | <0.01 | |||
| Yes | 286 (85.4%) | 63 (95.4) | 223 (82.9) | |
| ECOG,n (%) | <0.01 | |||
| ≥1 | 170 (50.7) | 22 (33.3) | 148 (55.0) | |
| Sarcomatoid feature | 0.1 | |||
| Yes | 14 (4.2) | 0 | 14 (5.2) | |
| IMDC score,n (%) | 0.02 | |||
| Intermediate-poor | 219 (65.4) | 35 (53.0) | 184 (68.4) | |
| Metastatic sites,n (%) | ||||
| Lung | 218 (65.1) | 40 (60.6) | 178 (66.2) | 0.2 |
| Liver | 51 (15.2) | 4 (6.1) | 47 (17.5) | 0.02 |
| Nodal | 117 (34.9) | 21 (31.8) | 96 (35.7) | 0.2 |
| Bone | 105 (31.3) | 18 (27.3) | 87 (32.3) | 0.3 |
| Brain | 14 (4.2) | 1 (1.5) | 13 (4.8) | 0.1 |
| First-Line Therapy,n (%) | 0.4 | |||
| Sunitinib | 200 (59.7) | 38 (57.5) | 162 (60.2) | |
| Pazopanib | 135 (40.3) | 28 (42.5) | 107 (39.8) | |
| Line of therapy after TKI,n (%) | 0.1 | |||
| >1 | 102 (30.4) | 15 (22.7) | 87 (32.3) |
| All | PFS ≥ 36 Month | PFS < 36 Months | p | |
|---|---|---|---|---|
| N = 116 | N = 31 (26.7%) | N = 85 (73.3%) | ||
| Age | 0.3 | |||
| Median (range) | 69 (37–86) | 71 (44–85) | 69 (37–86) | |
| Gender,n (%) | 0.1 | |||
| Male | 83 (71.5) | 18 (58.1) | 75 (76.5) | |
| Histology,n (%) | 0.7 | |||
| Clear-cell RCC | 102 (87.9) | 28 (90.3) | 74 (87.1%) | |
| Previous nephrectomy,n (%) | 0.9 | |||
| Yes | 110 (94.8%) | 30 (96.8) | 80 (94.1) | |
| ECOG,n (%) | 0.2 | |||
| ≥1 | 46 (39.7) | 9 (29.0) | 37 (43.5) | |
| Sarcomatoid feature | 1 | |||
| Yes | 1 (0.9) | 0 | 1 (1.2) | |
| Metastatic sites,n (%) | ||||
| Lung | 80 (69.0) | 20 (64.5) | 60 (70.6) | 0.6 |
| Liver | 18 (15.5) | 1 (3.2) | 17 (20.0) | 0.04 |
| Nodal | 32 (27.6) | 10 (32.3) | 22 (25.9) | 0.2 |
| Bone | 28 (24.1) | 8 (25.8) | 20 (23.5) | 0.8 |
| Brain | 2 (1.7) | 1 (3.2) | 1 (1.2) | 0.5 |
| First-Line Therapy,n (%) | 0.3 | |||
| Sunitinib | 66 (56.9) | 15(48.4) | 51 (60) | |
| Pazopanib | 50 (43.1) | 16 (51.6) | 34 (40) | |
| Line of therapy after TKI,n (%) | 0.03 | |||
| >1 | 33 (28.4) | 4 (12.9) | 29 (34.1) |
| All | PFS ≥ 36 Months | PFS < 36 Months | p | |
|---|---|---|---|---|
| N = 219 | N = 35 (16.0%) | N = 184 (84.0%) | ||
| Age | 0.5 | |||
| Median (range) | 65 (37–89) | 63 (37–78) | 65 (37–89) | |
| Gender,n (%) | 1 | |||
| Male | 157 (71.7) | 25 (71.4) | 132 (71.7) | |
| Histology,n (%) | 1 | |||
| Clear-cell RCC | 192 (87.7%) | 31 (88.6) | 161 (87.5) | |
| Previous nephrectomy,n (%) | 0.02 | |||
| Yes | 176 (80.4%) | 33 (94.3) | 143 (77.7) | |
| ECOG,n (%) | <0.01 | |||
| ≥1 | 124 (56.6) | 13 (37.1) | 11 (60.3) | |
| Sarcomatoid feature | 0.2 | |||
| Yes | 13 (5.9) | 0 | 13 (7.1) | |
| Metastatic sites,n (%) | 0.4 | |||
| Lung | 138 (63.0) | 20 (57.1) | 118 (64.1) | 0.3 |
| Liver | 33 (15.1) | 3 (8.6) | 30 (16.3) | 0.3 |
| Nodal | 85 (38.8) | 11 (31.4) | 74 (40.2) | 0.4 |
| Bone | 77 (35.2) | 10 (28.6) | 67 (36.4) | 0.2 |
| Brain | 12 (5.5) | 0 | 12 (6.5) | |
| First-Line Therapy,n (%) | 0.6 | |||
| Sunitinib | 134 (61.2) | 23 (65.7) | 111 (60.3) | |
| Pazopanib | 85 (38.8) | 12 (34.3) | 73 (39.7) | |
| Line of therapy after TKI,n (%) | 1 | |||
| >1 | 69 (31.5) | 11 (31.4) | 58 (31.5) |
| Univariate Analysis | Odds Ratio | CI 95% | p |
|---|---|---|---|
| Age | |||
| >70 | 0.92 | 0.53–1.60 | 0.8 |
| Gender | |||
| Male | 0.68 | 0.38–1.21 | 0.2 |
| Histology | |||
| Clear-cell RCC | 1.22 | 0.51–2.89 | 0.6 |
| Previous nephrectomy | |||
| Yes | 4.33 | 1.30–14.39 | 0.02 |
| ECOG PS | |||
| ≥1 | 0.43 | 0.26–0.72 | <0.01 |
| Sarcomatoid feature | |||
| Yes | 1 | ||
| IMDC score | |||
| Intermediate-poor | 0.52 | 0.30–0.90 | 0.02 |
| Metastatic sites,n (%) | |||
| Lung | 0.79 | 0.45–1.37 | 0.4 |
| Liver | 0.3 | 0.10–0.88 | 0.02 |
| Nodal | 0.84 | 0.47–1.49 | 0.5 |
| Bone | 0.78 | 0.43–1.43 | 0.4 |
| Others | 1.46 | 0.82–1.59 | 0.2 |
| Multivariate analysis | Odds Ratio | CI 95% | p |
| Previous nephrectomy | |||
| Yes | 3.42 | 1.00–11.63 | 0.05 |
| ECOG | |||
| ≥1 | 0.5 | 0.30–0.85 | 0.01 |
| IMDC score | |||
| Intermediate-poor | 0.64 | 0.36–1.14 | 0.1 |
| Metastatic sites,n (%) | |||
| Liver | 0.32 | 0.11–0.93 | 0.04 |
| Univariate Analysis | Odds Ratio | CI 95% | p |
|---|---|---|---|
| Age | |||
| >70 | 1.5 | 0.66–3.43 | 0.3 |
| Gender | |||
| Male | 0.43 | 0.18–1.02 | 0.05 |
| Histology | |||
| Clear-cell RCC | 1.39 | 0.36–5.34 | 0.6 |
| Previous nephrectomy | |||
| Yes | 1.87 | 0.21–16.71 | 0.6 |
| ECOG | |||
| ≥1 | 0.54 | 0.22–1.29 | 0.2 |
| Sarcomatoid feature | |||
| Yes | 1 | ||
| Metastatic sites,n (%) | |||
| Lung | 0.75 | 0.32–1.81 | 0.5 |
| Liver | 0.13 | 0.02–1.05 | 0.05 |
| Nodal | 1.37 | 0.56–3.34 | 0.5 |
| Bone | 1.13 | 0.44–2.92 | 0.8 |
| Others | 1.19 | 0.50–2.85 | 0.7 |
| Multivariate analysis | Odds Ratio | CI 95% | p |
| Gender | |||
| Male | 0.38 | 0.15–0.95 | 0.04 |
| Metastatic sites,n (%) | |||
| Liver | 0.32 | 0.11–0.93 | 0.04 |
| Univariate Analysis | Odds Ratio | CI 95% | p |
|---|---|---|---|
| Age | |||
| >70 | 0.53 | 0.23–1.19 | 0.1 |
| Gender | |||
| Male | 0.98 | 0.44–2.19 | 0.9 |
| Histology | |||
| Clear-cell RCC | 1.11 | 0.36–3.42 | 0.9 |
| Previous nephrectomy | |||
| Yes | 4.73 | 1.01–20.55 | 0.04 |
| ECOG | |||
| ≥1 | 0.39 | 0.18–0.82 | 0.01 |
| Sarcomatoid feature | |||
| Yes | 1 | ||
| Metastatic sites, n (%) | |||
| Lung | 0.74 | 0.36–1.55 | 0.4 |
| Liver | 0.48 | 0.14–1.67 | 0.2 |
| Nodal | 0.68 | 0.31–1.47 | 0.3 |
| Bone | 0.7 | 0.32–1.54 | 0.4 |
| Others | 1.81 | 0.82–3.95 | 0.1 |
| Multivariate analysis | Odds Ratio | CI 95% | p |
| Previous nephrectomy | |||
| Yes | 3.98 | 0.90–17.56 | 0.1 |
| ECOG | |||
| ≥1 | 0.44 | 0.21–0.94 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catalano, M.; De Giorgi, U.; Maruzzo, M.; Bimbatti, D.; Buti, S.; Mazzaschi, G.; Procopio, G.; Santoni, M.; Galli, L.; Conca, R.; et al. Long-Term Response to Tyrosine Kinase Inhibitors for Metastatic Renal Cell Carcinoma. Biomedicines 2022, 10, 2444. https://doi.org/10.3390/biomedicines10102444
Catalano M, De Giorgi U, Maruzzo M, Bimbatti D, Buti S, Mazzaschi G, Procopio G, Santoni M, Galli L, Conca R, et al. Long-Term Response to Tyrosine Kinase Inhibitors for Metastatic Renal Cell Carcinoma. Biomedicines. 2022; 10(10):2444. https://doi.org/10.3390/biomedicines10102444
Chicago/Turabian StyleCatalano, Martina, Ugo De Giorgi, Marco Maruzzo, Davide Bimbatti, Sebastiano Buti, Giulia Mazzaschi, Giuseppe Procopio, Matteo Santoni, Luca Galli, Raffaele Conca, and et al. 2022. "Long-Term Response to Tyrosine Kinase Inhibitors for Metastatic Renal Cell Carcinoma" Biomedicines 10, no. 10: 2444. https://doi.org/10.3390/biomedicines10102444
APA StyleCatalano, M., De Giorgi, U., Maruzzo, M., Bimbatti, D., Buti, S., Mazzaschi, G., Procopio, G., Santoni, M., Galli, L., Conca, R., Doni, L., Antonuzzo, L., & Roviello, G. (2022). Long-Term Response to Tyrosine Kinase Inhibitors for Metastatic Renal Cell Carcinoma. Biomedicines, 10(10), 2444. https://doi.org/10.3390/biomedicines10102444