

Mental Healthcare through Cognitive Emotional Regulation Strategies among Prisoners


Abstract
:1. Introduction
The Present Study
2. Method
2.1. Design and Setting
2.2. Participant
2.3. Measures
2.3.1. Cognitive Emotional Regulation Questionnaires
2.3.2. Number of Incarcerations
2.4. Analysis Procedures
3. Results
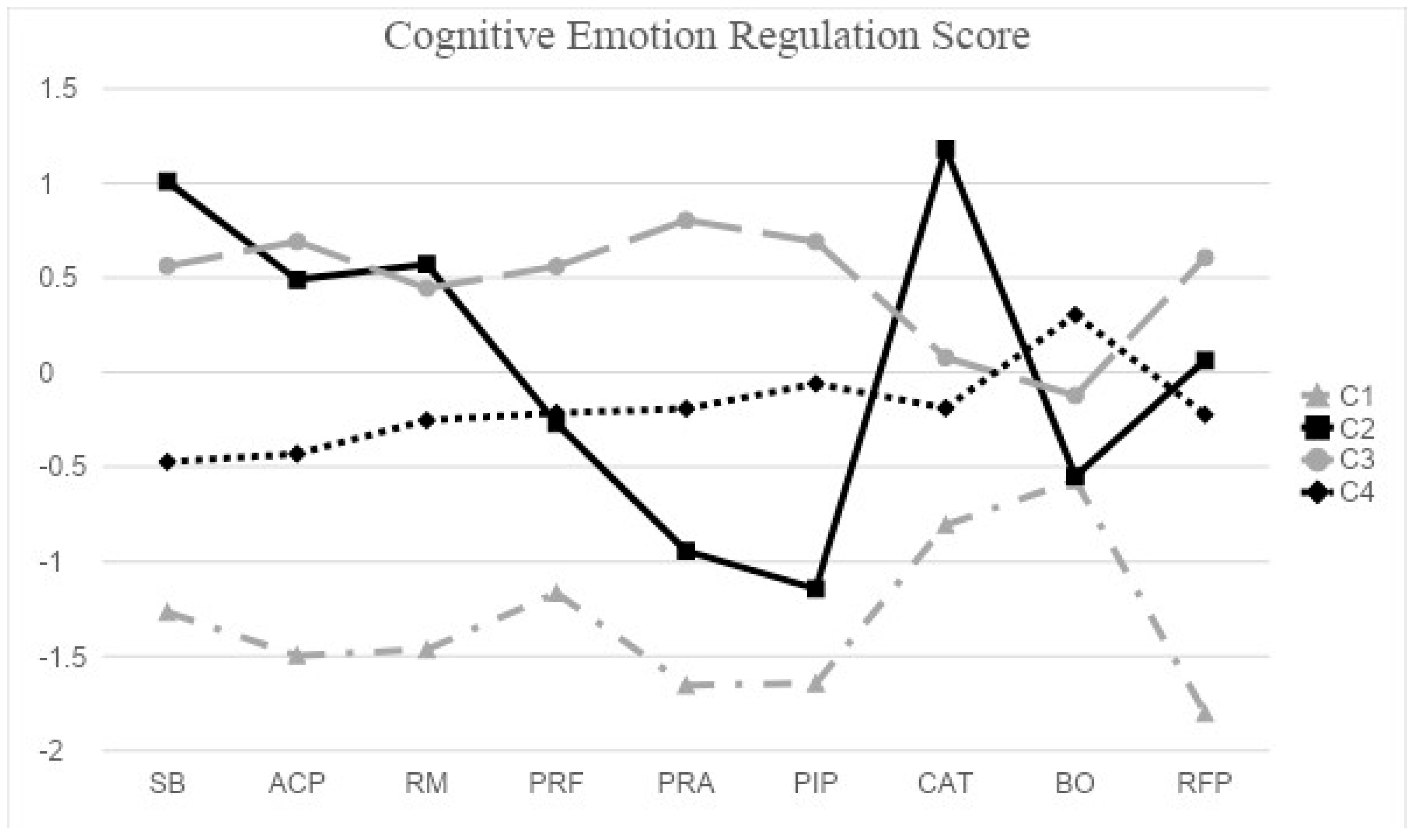
3.1. Identifying Latent Classes
3.2. Multinomial Logistic Regression Analysis
3.3. Number of Incarcerations Comparisons across Classes
4. Discussion
5. Implications and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sykes, G. The pains of imprisonment. In The Society of Captives: A Study of a Maximum Security Prison; Princeton University Press: Princeton, NJ, USA, 1958; pp. 63–78. [Google Scholar]
- Mandracchia, J.T.; Morgan, R.D.; Garos, S.; Garland, J.T. Prisoner Thinking Patterns: An Empirical Investigation. Crim. Justice Behav. 2007, 34, 1029–1043. [Google Scholar] [CrossRef]
- Katie, R.; Alexi, J. Research Roundup: Incarceration Can Cause Lasting Damage to Mental Health; Prison Policy Initiative: Northampton, MA, USA, 2021. [Google Scholar]
- Wang, L. Chronic Punishment: The Unmet Health Needs of People in State Prisons; Prison Policy Initiative: Northampton, MA, USA, 2022. [Google Scholar]
- Morgan, E.R.; Rivara, F.; Ta, M.; Crossman, D.; Jones, K.; Rowhani-Rahbar, A. Incarceration and subsequent risk of suicide: A statewide cohort study. Suicide Life-Threat. Behav. 2022, 52, 467–477. [Google Scholar] [CrossRef]
- Stringer, H. Improving mental health for inmates. Monit. Psychol. 2019, 50, 46. Available online: https://www.apa.org/monitor/2019/03/mental-heath-inmates (accessed on 10 December 2023).
- Bronson, J.; Berzofsky, M. Indicators of Mental Health Problems Reported by Prisoners and Jail Inmates, 2011–2012; U.S. Department of Justics Office of Justics, Programs Bureau of Justice Statistics: Washington, DC, USA, 2017.
- Alexi, J.; Sawyer, W. Arrest, Release, Repeat: How Police and Jails Are Misused to Respond to Social Problems; Prison Policy Initiative: Northampton, MA, USA, 2019. [Google Scholar]
- Wallace, D.; Wang, X. Does in-prison physical and mental health impact recidivism? SSM Pop. Health 2020, 11, 100569. [Google Scholar] [CrossRef]
- Reingle Gonzalez, J.M.; Connell, N.M. Mental health of prisoners: Identifying barriers to mental health treatment and medication continuity. Am. J. Public Health 2014, 104, 2328–2333. [Google Scholar] [CrossRef]
- Seo, J.H.; Kim, K.; Lee, K.; Kim, G. A study on linguistic and psychological characteristics and personality profiling in the writings of murders. J. Korean Data Anal. Soc. 2012, 14, 1355–1371. [Google Scholar]
- Hare, R.D. Hare Psychopathy Checklist-Revised, 2nd ed.; Multi-Health Systems: Toronto, ON, Canada, 2003. [Google Scholar]
- Hare, R.D.; Neumann, C.S. The PCL-R assessment of psychopathy: Development, structural properties, and new directions. In Handbook of Psychopathy; Patrick, C.J., Ed.; Guilford Press: New York, NY, USA, 2006; pp. 58–88. [Google Scholar]
- Williams, K.M.; Paulhus, D.L.; Hare, R.D. Capturing the four-factor structure of psychopathy in college students via self-report. J. Pers. Assess. 2007, 88, 205–219. [Google Scholar] [CrossRef]
- Hare, R.D. Psychopathy, affect and behavior. In Psychopathy: Theory, Research and Implications for Society; Cooke, D.J., Forth, A.E., Hare, R.D., Eds.; Kluwer: Dordrecht, The Netherlands, 1998; pp. 105–137. [Google Scholar]
- Garofalo, C.; Neumann, C.S. Psychopathy and emotion regulation: Taking stock and moving forward. In Routledge International Handbook of Psychopathy and Crime; DeLisi, M., Ed.; Routledge: Abingdon, UK, 2018; pp. 58–79. [Google Scholar]
- Coid, J.; Yang, M.; Ullrich, S.; Roberts, A.; Hare, R.D. Prevalence and correlates of psychopathic traits in the household population of Great Britain. Int. J. Law Psychiatry 2009, 32, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Hare, R.D.; Neumann, C.S. Psychopathy: Assessment and forensic implications. Can. J. Psychiatry 2009, 54, 791–802. [Google Scholar] [CrossRef] [PubMed]
- Olver, M.E.; Neumann, C.S.; Wong, S.C.P.; Hare, R.D. The structural and predictive properties of the Psychopathy Checklist–Revised in Canadian Aboriginal and non-Aboriginal offenders. Psychol. Assess. 2013, 25, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Garofalo, C.; Neumann, C.S.; Velotti, P. Psychopathy and aggression: The role of emotion dysregulation. J. Interpers. Violence 2021, 36, NP12640–NP12664. [Google Scholar] [CrossRef] [PubMed]
- Preston, O.C.; Anestis, J.C. The indirect relationships between psychopathic traits and proactive and reactive aggression through empathy and emotion dysregulation. J. Psychopathol. Behav. Assess. 2020, 42, 409–423. [Google Scholar] [CrossRef]
- Garnefski, N.; Kraaij, V.; Spinhoven, P. Negative life events, cognitive emotion regulation and emotional problems. Pers. Individ. Differ. 2001, 30, 1311–1327. [Google Scholar] [CrossRef]
- Weiss, N.H.; Forkus, S.R.; Contractor, A.A.; Dixon-Gordon, K.L. The interplay of negative and positive emotion dysregulation on mental health outcomes among trauma-exposed community individuals. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Ahn, H.N.; Lee, N.; Joo, H. Validation of the cognitive emotion regulation questionnaire in a Korean population. Korean J. Couns. 2013, 14, 1773–1794. [Google Scholar] [CrossRef]
- Garnefski, N.; Kraaij, V. The cognitive emotion regulation questionnaire. Eur. J. Psychol. Assess. 2007, 23, 141–149. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Lubke, G.H.; Muthén, B. Investigating population heterogeneity with factor mixture models. Psychol. Methods 2005, 10, 21–39. [Google Scholar] [CrossRef]
- Vermunt, J.K. Latent class modeling with covariates: Two improved three-step approaches. Political Anal. 2017, 18, 450–469. [Google Scholar] [CrossRef]
- Wang, J.; Wang, X. Structural Equation Modeling: Applications Using Mplus, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Struct. Equ. Model. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- McLachlan, G.J.; Peel, D. Finite Mixture Models; Wiley: Hoboken, NJ, USA, 2004. [Google Scholar]
- Schwartz, G. Estimating the dimension of a model. Ann. Stat. 1978, 6, 461–464. [Google Scholar] [CrossRef]
- Jung, S.; Shin, M.; Lee, Y.R. An application of latent class analysis to classifying change trajectory of school achievement improvement of general high school and testing determinants of the classification. J. Educ. Eval. Res. 2015, 28, 1277–1299. [Google Scholar]
- Garnefski, N.; Kraaij, V. Relationships between cognitive emotion regulation strategies and depressive symptoms: A comparative study of five specific samples. Pers. Individ. Differ. 2006, 40, 1659–1669. [Google Scholar] [CrossRef]
- Zhou, J.; Witt, K.; Cao, X.; Chen, C.; Wang, X. Predicting reoffending using the Structured Assessment of Violence Risk in Youth (SAVRY): A 5-year follow-up study of male juvenile offenders in Hunan Province, China. PLoS ONE 2017, 12, e0169251. [Google Scholar] [CrossRef] [PubMed]
- Ehring, T.; Tuschen-Caffier, B.; Schnulle, J.; Fisher, S.; Gross, J.J. Emotion regulation and vulnerability to depression: Spontaneous versus instructed use of emotion suppression and reappraisal. Emotion 2010, 10, 563. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.; Worrall, A. Life as a woman: The gendered pains of indeterminate imprisonment. Prison. Serv. J. 2000, 132, 27–37. [Google Scholar] [CrossRef]
- Lipsey, M.W.; Cullen, F.T. The effectiveness of correctional rehabilitation: A review of systematic reviews. Annu. Rev. Law Soc. Sci. 2007, 3, 297–320. [Google Scholar] [CrossRef]
- Okeke, A.O.; Obiora, A.; Ezeokaana, J.O.; Abamara, N.C. Age, gender, stress and self-blame as predictors of suicidal-ideation among prison inmates in South East Nigeria. Soc. Sci. Res. 2022, 6, 1. [Google Scholar]
- Carl, J.R.; Soskin, D.P.; Kerns, C.; Barlow, D.H. Positive emotion regulation in emotional disorders: A theoretical review. Clin. Psychol. Rev. 2013, 33, 343–360. [Google Scholar] [CrossRef]
- Pearson, F.S.; Lipton, D.S.; Cleland, C.M.; Yee, D.S. The effects of behavioral/cognitive-behavioral programs on recidivism. Crime Delinq. 2022, 48, 476–496. [Google Scholar] [CrossRef]
- Antonowicz, D.H.; Ross, R.R. Essential components of successful rehabilitation programs for offenders. Int. J. Offender. Ther. Comp. Criminol. 1994, 38, 97–104. [Google Scholar] [CrossRef]
- Gendreau, P. Offender rehabilitation: What we know and what needs to be done. Crim. Justice Behav. 1996, 23, 144–161. [Google Scholar] [CrossRef]
- Docherty, M.; Lieman, A.; Gorden, B.L. Improvement in emotion regulation while detained predicts lower juvenile recidivism. Youth Violence Juv. Justice 2021, 20, 164–183. [Google Scholar] [CrossRef]

{kind=link}
| Demographic Information | Categories | N | % |
|---|---|---|---|
| Criminals | Homicide | 149 | 29.8 |
| Violent Offenses | 77 | 15.4 | |
| Sexual Violence Offenses | 150 | 30.0 | |
| Property Offenses | 86 | 17.2 | |
| Drug-Related Crimes | 20 | 4.0 | |
| Others | 18 | 3.6 | |
| Years of Education | Below Primary School | 12 | 2.4 |
| Primary School | 73 | 14.6 | |
| Middle School | 133 | 26.6 | |
| High School | 221 | 44.2 | |
| Above College | 60 | 12 | |
| Job Status | Full-time Jobs | 285 | 57.0 |
| Part-time Jobs | 145 | 29.0 | |
| Unemployed | 70 | 14.0 | |
| Total | 500 | ||
| Mean | SD | ||
| Age | 46.69 | 11.59 | |
| # of incarcerations | 2.39 | 2.20 | |
| Depression | PHQ9 | 30.64 | 2.68 |
| CER Strategy | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|
| Self-blame | 0.80 | ||||||||
| Acceptance | 0.55 ** | 0.64 | |||||||
| Rumination | 0.47 ** | 0.41 ** | 0.66 | ||||||
| Positive refocusing | 0.28 ** | 0.33 ** | 0.19 ** | 0.75 | |||||
| Positive reappraisal | 0.26 ** | 0.47 ** | 0.29 ** | 0.48 ** | 0.74 | ||||
| Putting into perspectives | 0.23 ** | 0.40 ** | 0.23 ** | 0.38 ** | 0.64 ** | 0.59 | |||
| Catastrophizing | 0.41 ** | 0.19 ** | 0.58 ** | −0.02 | −0.05 | −0.08 | 0.78 | ||
| Blaming others | −0.27 ** | −0.10 * | 0.11 * | −0.06 | 0.09 * | 0.13 ** | 0.17 ** | 0.74 | |
| Refocus on planning | 0.32 ** | 0.45 ** | 0.36 * | 0.40 ** | 0.58 ** | 0.43 ** | 0.03 | 0.05 | 0.77 |
| Mean | 13.80 | 11.07 | 13.10 | 13.74 | 13.99 | 13.75 | 10.76 | 9.77 | 15.87 |
| SD | 3.78 | 2.55 | 3.20 | 3.47 | 3.55 | 3.04 | 3.99 | 3.40 | 3.05 |
| Fit Index | 2 Classes | 3 Classes | 4 Classes | 5 Classes |
|---|---|---|---|---|
| BIC | 12319.27 | 12100.90 | 11937.32 | 11865.87 |
| BLRT | 625.19 ** | 280.52 ** | 225.72 ** | 133.59 ** |
| Class sizes | 143/357 | 22/242/236 | 36/45/188/231 | 18/105/224/47/106 |
| Entropy | 0.78 | 0.81 | 0.84 | 0.81 |
| Demographic Information | Categories | Class 1 | Class 2 | Class 3 | Class 4 |
|---|---|---|---|---|---|
| Strong Blamer | Negative Self-Blamer | Distorted Positivity | Moderate Blamer | ||
| Frequency (%) | |||||
| Criminals | Homicide | 11 (30.6) | 23 (51.1) | 51 (27.1) | 64 (27.7) |
| Violent Offenses | 4 (11.1) | 6 (13.3) | 33 (17.6) | 34 (14.7) | |
| Sexual Violence Offenses | 16 (44.4) | 12 (26.7) | 42 (22.3) | 80 (34.6) | |
| Property Offenses | 3 (8.3) | 2 (4.4) | 38 (20.2) | 43 (18.6) | |
| Drug-Related Crimes | - | 1 (2.2) | 14 (7.4) | 5 (2.2) | |
| Others | 2 (5.6) | 1 (2.2) | 10 (5.3) | 5 (2.2) | |
| Educational Years | Below Primary School | - | 1 (2.2) | 7 (3.7) | 4 (1.7) |
| Primary School | 8 (22.2) | 9 (20.0) | 23 (12.2) | 33 (14.3) | |
| Middle School | 9 (25.0) | 11 (24.4) | 37 (19.7) | 76 (32.9) | |
| High School | 17 (47.2) | 19 (42.2) | 93 (49.5) | 92 (39.8) | |
| Above College | 2 (5.6) | 5 (11.1) | 27 (14.4) | 26 (11.3) | |
| Job Status | Full-time Jobs | 21 (58.3) | 28 (62.2) | 111 (59.0) | 125 (54.1) |
| Part-time Jobs | 9 (25.0) | 9 (20.0) | 53 (28.2) | 67 (29.0) | |
| No Jobs | 6 (16.7) | 8 (17.8) | 24 (12.8) | 39 (16.9) | |
| Total | 36 | 45 | 188 | 231 | |
| Mean (SD) | |||||
| Age | 43.32 (12.46) | 51.16 (11.30) | 47.74 (10.46) | 45.44 (12.12) | |
| # of recidivism | 2.22 (1.82) | 1.71 (1.58) | 2.49 (2.28) | 2.46 (2.27) | |
| Depression | PHQ9 | 29.94 (2.62) | 31.49 (2.46) | 30.35 (2.63) | 30.83 (2.72) |
| Anxiety | STAI-S | 37.75 (6.59) | 40.56 (6.53) | 42.97 (6.04) | 40.37 (6.87) |
| STAI-T | 38.17 (7.63) | 40.11 (6.03) | 43.95 (5.70) | 41.12 (6.38) | |
| Class Comparison | Estimate | S.E. | p-Value | Odds Ratio |
|---|---|---|---|---|
| Depression → C1 | −0.22 | 0.09 | 0.01 | 0.80 |
| Depression → C3 | −0.16 | 0.06 | 0.01 | 0.85 |
| Depression → C4 | −0.08 | 0.06 | 0.10 | 0.91 |
| Class Comparison | Estimate | S.E. | p-Value |
|---|---|---|---|
| C1 vs. C2 | 0.50 | 0.38 | 0.18 |
| C1 vs. C3 | −0.27 | 0.34 | 0.43 |
| C1 vs. C4 | −0.24 | 0.34 | 0.48 |
| C2 vs. C3 | −0.78 | 0.29 | 0.01 |
| C2 vs. C4 | −0.74 | 0.28 | 0.01 |
| C3 vs. C4 | 0.03 | 0.23 | 0.88 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.; Kim, M.; Park, J. Mental Healthcare through Cognitive Emotional Regulation Strategies among Prisoners. Healthcare 2024, 12, 6. https://doi.org/10.3390/healthcare12010006
Choi Y, Kim M, Park J. Mental Healthcare through Cognitive Emotional Regulation Strategies among Prisoners. Healthcare. 2024; 12(1):6. https://doi.org/10.3390/healthcare12010006
Chicago/Turabian StyleChoi, Younyoung, Mirim Kim, and Jeongsoo Park. 2024. "Mental Healthcare through Cognitive Emotional Regulation Strategies among Prisoners" Healthcare 12, no. 1: 6. https://doi.org/10.3390/healthcare12010006
APA StyleChoi, Y., Kim, M., & Park, J. (2024). Mental Healthcare through Cognitive Emotional Regulation Strategies among Prisoners. Healthcare, 12(1), 6. https://doi.org/10.3390/healthcare12010006