
Prevalence of Malnutrition in Hospitalized Patients in Lebanon Using Nutrition Risk Screening (NRS-2002) and Global Leadership Initiative on Malnutrition (GLIM) Criteria and Its Association with Length of Stay
 , ,
, ,
Abstract
:1. Introduction
Context of the Study
2. Materials and Methods
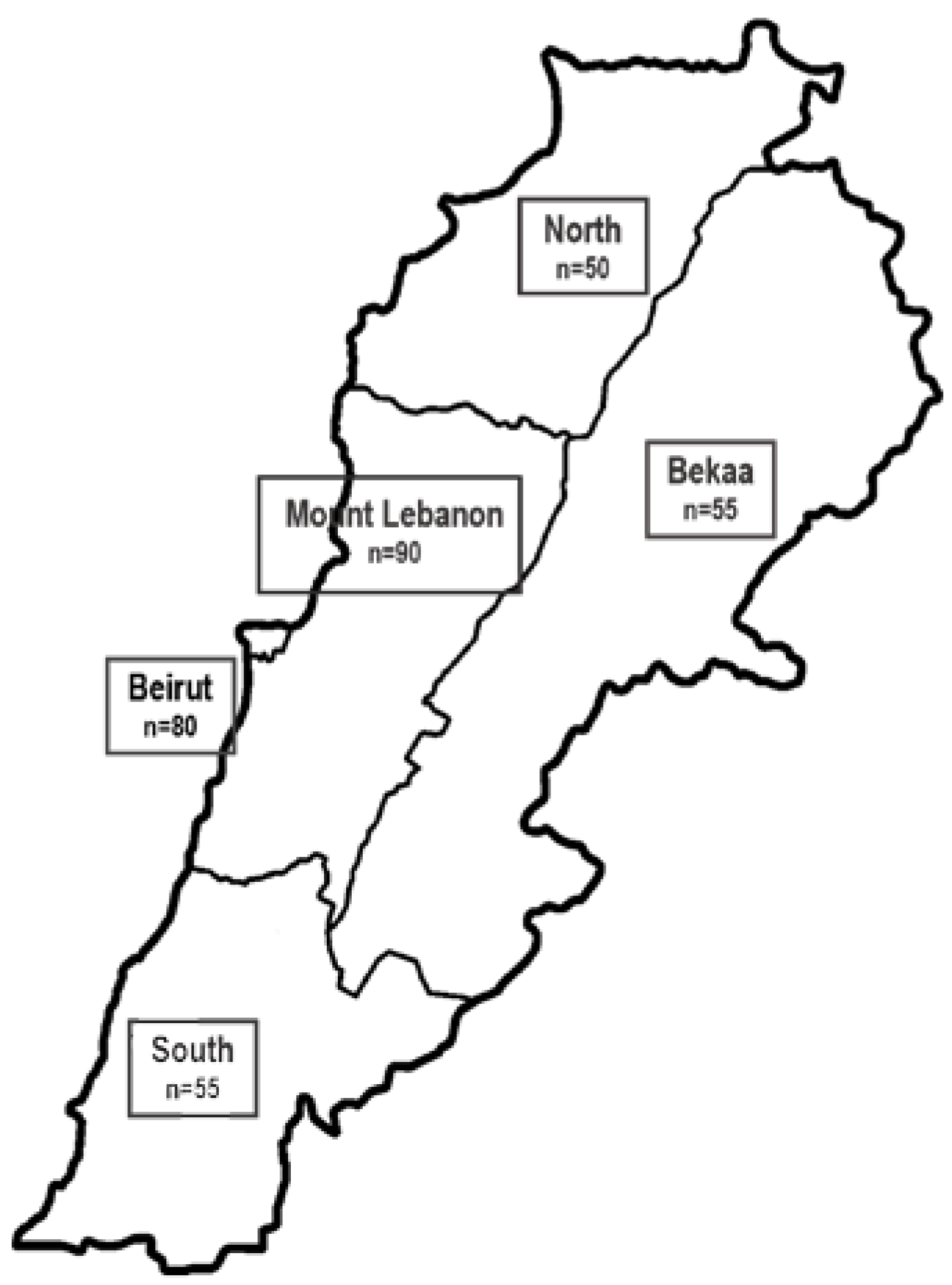
2.1. Design and Sample Size
2.2. Data Collection
2.3. Nutritional Status
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Basic Characteristic
3.2. Prevalence of Malnutrition
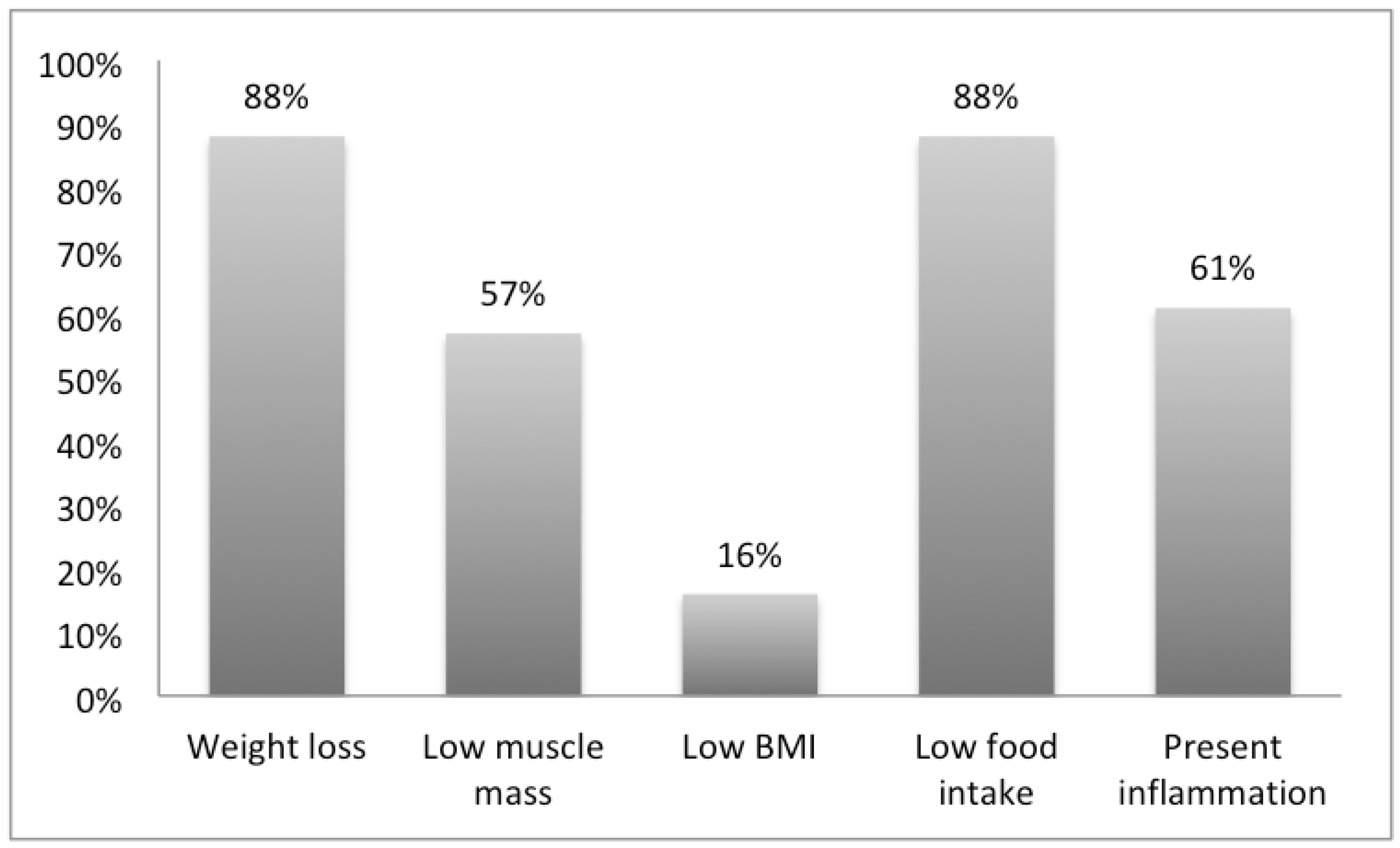
3.3. Frequency of the Different GLIM Criteria
3.4. Association of Malnutrition, Muscle Mass and Length of Hospital Stay
3.5. Multiple Logistic Regression of Length of Hospital Stay
3.6. Association of Malnutrition with Hospital Readmission
4. Discussion
Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barker, L.A.; Gout, B.; Crowe, T. Hospital malnutrition: Prevalence, identification and impact on patients and the healthcare system. Int. J. Environ. Res. Public Health 2011, 8, 514–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, K.; Pichard, C.; Lochs, H.; Pirlich, M. Prognostic impact of disease-related malnutrition. Clin. Nutr. 2008, 27, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Corkins, M.; Guenter, P.; DiMaria-Ghalili, R.A.; Jensen, G.; Malone, A.; Miller, S.; Patel, V.; Plogsted, S.; Resnick, H.; American Society for Parenteral and Enteral Nutrition. A.S.P.E.N. data brief 2014: Use of enteral and parenteral nutrition in hospitalized patients with a diagnosis of malnutrition: United States, 2010. Nutr. Clin. Pract. 2014, 29, 698–700. [Google Scholar] [CrossRef] [PubMed]
- Czapla, M.; Juárez-Vela, R.; Łokieć, K.; Wleklik, M.; Karniej, P.; Smereka, J. The Association between Nutritional Status and Length of Hospital Stay among Patients with Hypertension. Int. J. Environ. Res. Public Health 2022, 19, 5827. [Google Scholar] [CrossRef]
- Vong, T.; Yanek, L.R.; Wang, L.; Yu, H.; Fan, C.; Zhou, E.; Oh, S.J.; Szvarca, D.; Kim, A.; Potter, J.J.; et al. Malnutrition Increases Hospital Length of Stay and Mortality among Adult Inpatients with COVID-19. Nutrients 2022, 14, 1310. [Google Scholar] [CrossRef]
- Khalatbari-Soltani, S.; Marques-Vidal, P. The economic cost of hospital malnutrition in Europe; a narrative review. Clin. Nutr. ESPEN 2015, 10, e89–e94. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Reig, M.; Aranda-Reneo, I.; Peña-Longobardo, L.M.; Oliva-Moreno, J.; Barcons-Vilardell, N.; Hoogendijk, E.O.; Abizanda, P. Use of health resources and healthcare costs associated with nutritional risk: The FRADEA study. Clin. Nutr. 2017, 37, 1299–1305. [Google Scholar] [CrossRef]
- Meijers, J.M.; Schols, J.M.; Soeters, P.B.; Halfens, R.J. Defining malnutrition: Mission or mission impossible? Nutrition 2010, 26, 432–440. [Google Scholar] [CrossRef]
- Steiber, A.; Hegazi, R.; Herrera, M.; Zamor, M.L.; Chimanya, K.; Pekcan, A.G.; Redondo-Samin, D.C.D.; Correia, M.I.T.; Ojwang, A.A. Spotlight on Global Malnutrition: A Continuing Challenge in the 21st Century. J. Acad. Nutr. Diet. 2015, 115, 1335–1341. [Google Scholar] [CrossRef]
- Cárdenas, D.; Bermúdez, C.E.; Echeverri, S.; Pérez, A.; Puentes, M.; López, L.; Correia, M.I.; Ochoa, J.B.; Ferreira, A.M.; Texeira, M.A.; et al. Cartagena Declaration. The International Declaration on the Right to Nutritional Care and the Fight against Malnutrition. Nutr. Hosp. 2019, 36, 974–980. [Google Scholar]
- Cederholm, T.; Jensen, G. To create a consensus on malnutrition diagnostic criteria: A report from the Global Leadership Initiative on Malnutrition (GLIM) meeting at the ESPEN Congress 2016. Clin. Nutr. 2017, 36, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Klek, S.; Krznaric, Z.; Gundogdu, R.H.; Chourdakis, M.; Kekstas, G.; Jakobson, T.; Paluszkiewicz, P.; Bender, D.V.; Uyar, M.; Demirag, K.; et al. Prevalence of malnutrition in various political, economic, and geographic settings. JPEN J. Parenter. Enter. Nutr. 2015, 39, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Sorensen, J.; Kondrup, J.; Prokopowicz, J.; Schiesser, M.; Krähenbühl, L.; Meier, R.; Liberda, M. EuroOOPS: An international, multicentre study to implement nutritional risk screening and evaluate clinical outcome. Clin. Nutr. 2008, 27, 340–349. [Google Scholar] [CrossRef] [PubMed]
- El Zoghbi, M.; Boulos, C.; Awada, S.; Rachidi, S.; Al-Hajje, A.; Bawab, W.; Saleh, N.; Salameh, P. Prevalence of malnutrition and its correlates in older adults living in long stay institutions situated in Beirut, Lebanon. J. Res. Health Sci. 2014, 14, 11–17. [Google Scholar]
- Mitri, R.; Boulos, C.; Adib, S. Determinants of the nutritional status of older adults in urban Lebanon. Geriatr. Gerontol. Int. 2017, 17, 424–432. [Google Scholar] [CrossRef]
- Central Adminsitration of Stastitistic in Lebanon. Minsitry of Social Affairs. 2015. Available online: http://www.cas.gov.lb/index.php/demographic-and-social-en (accessed on 22 December 2022).
- Lebanon Econmic Monitor, in World Bank. 2022. Available online: https://www.worldbank.org/en/country/lebanon/publication/lebanon-economic-monitor (accessed on 22 December 2022).
- National Health Statistics Report in Lebanon. Minsitry of Public Health. 2012. Available online: https://www.usj.edu.lb/intranet/annonce/files/pdf/175_pdf_1.pdf (accessed on 22 December 2022).
- Lim, S.L.; Ong, K.C.B.; Chan, Y.H.; Loke, W.C.; Ferguson, M.; Daniels, L. Malnutrition and its impact on cost of hospitalization, length of stay, readmission and 3-year mortality. Clin. Nutr. 2012, 31, 345–350. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Kondrup, J.; Rasmussen, H.H.; Hamberg, O.; Stanga, Z. Nutritional risk screening (NRS 2002): A new method based on an analysis of controlled clinical trials. Clin. Nutr. 2003, 22, 321–336. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.J.; et al. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community. Clin. Nutr. 2019, 38, 207–217. [Google Scholar] [CrossRef] [Green Version]
- Prado, C.M.; Landi, F.; Chew, S.T.; Atherton, P.J.; Molinger, J.; Ruck, T.; Gonzalez, M.C. Advances in muscle health and nutrition: A toolkit for healthcare professionals. Clin. Nutr. 2022, 41, 2244–2263. [Google Scholar] [CrossRef]
- Choueiry, G.; Fattouh, N.; Hallit, R.; Kazour, F.; Hallit, S.; Salameh, P. Nutritional Status of Lebanese Hospitalized Patients With Chronic Disease: A Cross-Sectional Study. Hosp. Pharm. 2021, 56, 102–108. [Google Scholar] [CrossRef]
- Balci, C.; Bolayir, B.; Eşme, M.; Arik, G.; Kuyumcu, M.E.; Yeşil, Y.; Varan, H.D.; Kara, Ö.; Güngör, A.E.; Doğu, B.B.; et al. Comparison of the Efficacy of the Global Leadership Initiative on Malnutrition Criteria, Subjective Global Assessment, and Nutrition Risk Screening 2002 in Diagnosing Malnutrition and Predicting 5-Year Mortality in Patients Hospitalized for Acute Illnesses. JPEN J. Parenter. Enter. Nutr. 2021, 45, 1172–1180. [Google Scholar] [CrossRef]
- Bellanti, J.A.; Zeligs, B.; Kulszycki, L. Nutrition and development of pulmonary defense mechanisms. Pediatr. Pulmonol. Suppl. 1997, 16, 170–171. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Wan, Z.; Zhu, Y.; Zhang, L.; Zhang, L.; Wan, H. Prevalence of malnutrition comparing NRS2002, MUST, and PG-SGA with the GLIM criteria in adults with cancer: A multi-center study. Nutrition 2021, 83, 111072. [Google Scholar] [CrossRef]
- Bellanti, F.; Buglio, A.L.; Quiete, S.; Pellegrino, G.; Dobrakowski, M.; Kasperczyk, A.; Kasperczyk, S.; Vendemiale, G. Comparison of Three Nutritional Screening Tools with the New Glim Criteria for Malnutrition and Association with Sarcopenia in Hospitalized Older Patients. J. Clin. Med. 2020, 9, 1898. [Google Scholar] [CrossRef]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. ESPEN guidelines for nutrition screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Kiss, N.; Steer, B.; de van der Schueren, M.; Loeliger, J.; Alizadehsani, R.; Edbrooke, L.; Deftereos, I.; Laing, E.; Khosravi, A. Comparison of the prevalence of 21 GLIM phenotypic and etiologic criteria combinations and association with 30-day outcomes in people with cancer: A retrospective observational study. Clin. Nutr. 2022, 41, 1102–1111. [Google Scholar] [CrossRef] [PubMed]
- Barone, M. Is the use of the BMI alone sufficient to diagnose malnutrition in both male and female adults? Clin. Nutr. 2018, 37, 1771. [Google Scholar] [CrossRef] [PubMed]
- Allard, J.P.; Keller, H.; Jeejeebhoy, K.N.; Laporte, M.; Duerksen, D.R.; Gramlich, L.; Payette, H.; Bernier, P.; Vesnaver, E.; Davidson, B.; et al. Malnutrition at Hospital Admission-Contributors and Effect on Length of Stay: A Prospective Cohort Study From the Canadian Malnutrition Task Force. JPEN J. Parenter. Enter. Nutr. 2016, 40, 487–497. [Google Scholar] [CrossRef]
- Fry, D.E.; Pine, M.; Jones, B.L.; Meimban, R.J. Patient characteristics and the occurrence of never events. Arch. Surg. 2010, 145, 148–151. [Google Scholar] [CrossRef] [Green Version]
- Keller, H.; de van der Schueren, M.A.; GLIMConsortium Jensen, G.L.; Barazzoni, R.; Compher, C.; Correia, M.I.; Gonzalez, M.C.; Jager-Wittenaar, H.; Pirlich, M.; Steiber, A. Global Leadership Initiative on Malnutrition (GLIM): Guidance on Validation of the Operational Criteria for the Diagnosis of Protein-Energy Malnutrition in Adults. JPEN J. Parenter. Enter. Nutr. 2020, 44, 992–1003. [Google Scholar] [CrossRef]
- Mendes, J.; Azevedo, A.; Amaral, T. Handgrip strength at admission and time to discharge in medical and surgical inpatients. JPEN J. Parenter. Enter. Nutr. 2014, 38, 481–488. [Google Scholar] [CrossRef]
- McNicholl, T.; Curtis, L.; Dubin, J.A.; Mourtzakis, M.; Nasser, R.; Laporte, M.; Keller, H. Handgrip strength predicts length of stay and quality of life in and out of hospital. Clin. Nutr. 2020, 39, 2501–2509. [Google Scholar] [CrossRef]
- Soriano-Moreno, D.R.; Dolores-Maldonado, G.; Benites-Bullón, A.; Ccami-Bernal, F.; Fernandez-Guzman, D.; Esparza-Varas, A.L.; Caira-Chuquineyra, B.; Taype-Rondan, A. Recommendations for nutritional assessment across clinical practice guidelines: A scoping review. Clin. Nutr. ESPEN 2022, 49, 201–207. [Google Scholar] [CrossRef]
- United Nations Decade of Action on Nutrition 2016-2025. Food and Agriculture Origanization. Available online: http://www.fao.org/3/a-i6129e.pdf (accessed on 22 December 2022).
- Holmes, R.A. Role of dietitians in reducing malnutrition in hospital. CMAJ 2019, 191, E139. [Google Scholar] [CrossRef] [Green Version]
- Simmance, N.; Cortinovis, T.; Green, C.; Lunardi, K.; McPhee, M.; Steer, B.; Wai, J.; Martin, T.; Porter, J. Introducing novel advanced practice roles into the health workforce: Dietitians leading in gastrostomy management. Nutr. Diet. 2019, 76, 14–20. [Google Scholar] [CrossRef]
- Cook, F.; Rodriguez, J.; McCaul, L. Malnutrition, nutrition support and dietary intervention: The role of the dietitian supporting patients with head and neck cancer. Br. Dent. J. 2022, 233, 757–764. [Google Scholar] [CrossRef]
- Khan, M.; Hui, K.; McCauley, S. What Is a Registered Dietitian Nutritionist’s Role in Addressing Malnutrition? J. Acad. Nutr. Diet. 2018, 118, 1804. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Phenotypic Criteria | Etiologic Criteria | |||
|---|---|---|---|---|
| Severity level | Moderate | Severe | ||
| Weight loss | >5–10% within past 6 months or 10–20% beyond 6 months | >10% within past 6 months or >20% beyond 6 months | Reduced food intake | <50% of estimated needs in >1 week or any reduction for >2 weeks |
| Low BMI | <20 kg/m2 if <70 years, <22 kg/m2 if ≥70 years | <18.5 if <70 years, <20 if <70 years | Any chronic GI condition that adversely impacts food assimilation or absorption | |
| Reduced muscle mass 2 | MUAC 1 < 23 cm | MUAC < 20 cm | Inflammation | Elevated C-reactive protein (CRP) levels |
| Characteristic | N (%) |
|---|---|
| Age | |
| <70 years old | 226 (65.9%) |
| ≥70 years old | 117 (34.11%) |
| Gender | |
| Male | 188 (54.81%) |
| Female | 155 (45.19%) |
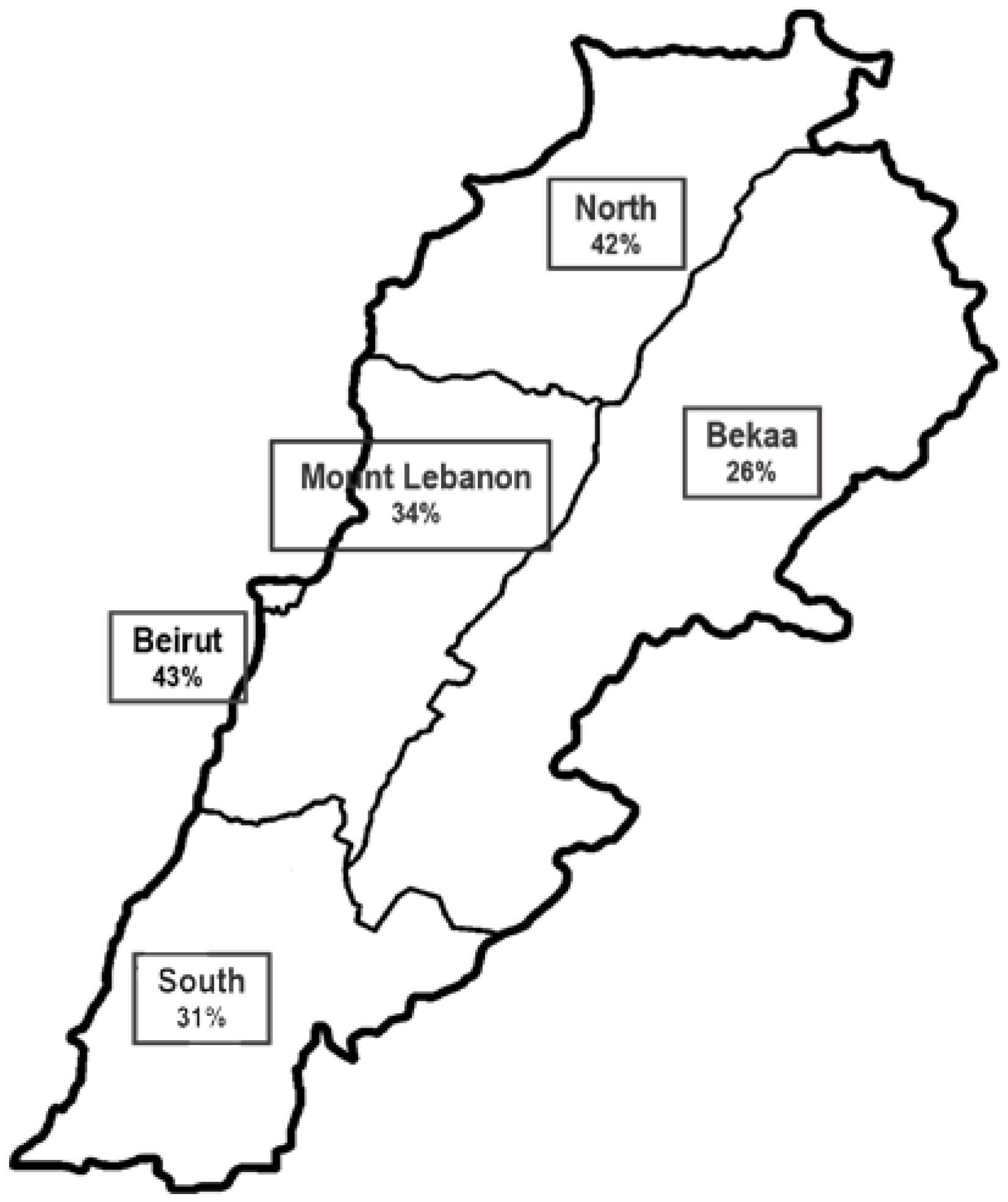
| District | |
| Beirut | 81 (23.62%) |
| North | 50 (14.58%) |
| South | 58 (16.91%) |
| Mount Lebanon | 100 (29.15%) |
| Bekaa Valley | 54 (15.74%) |
| Present illness | |
| Oncology | 25 (7.29%) |
| Cardiovascular disease | 53 (15.45%) |
| Infectious disease | 95 (27.70%) |
| Gastrointestinal disease | 40 (11.66%) |
| Surgical procedure | 113 (32.4%) |
| Other | 17 (4.96%) |
| Underlying disease | |
| None | 87 (25.36%) |
| Diabetes and cardiovascular diseases | 192 (55.98%) |
| Cancer | 44 (12.83%) |
| Neurological disorders | 8 (2.33%) |
| Gastrointestinal diseases | 12 (3.50%) |
| Home medications | |
| None | 110 (32.07%) |
| One medication | 46 (13.41%) |
| Two medications | 46 (13.41%) |
| Three or more medications | 141 (41.11%) |
| Previous hospital admission within 3 months | |
| Yes | 48 (13.99%) |
| No | 295 (86.01%) |
| Prevalence Rate | N (%) |
|---|---|
| NRS-2002 | |
| Mild risk (<3) | 236 (68.8%) |
| At risk (≥3) | 107 (31.2%) |
| GLIM | |
| Normal nutritional status | 221 (64.43%) |
| Malnourished | 122 (35.57%) |
| Moderate malnutrition | 73 (21.28%) |
| Severe malnutrition | 49 (14.29%) |
| Nutritional Status | Low | Normal |
|---|---|---|
| Nutritional status according to GLIM criteria 1 | 90.9% | 9.1% |
| Handgrip strength (HGS) | 74.4% | 25.6% |
| Mid-upper arm muscle circumference (MUAC) | 84.4% | 15.6% |
| Odds Ratio (OR) | 95% CI for OR | p-Value | |
|---|---|---|---|
| Underlying disease a | |||
| Diabetes and cardiovascular diseases | 0.97 | 0.31; 3.06 | 0.963 |
| Cancer | 1.50 | 0.31; 7.11 | 0.608 |
| Other (neurological disorders and gastrointestinal diseases) | 0.56 | 0.11; 2.87 | 0.489 |
| Home medications b | |||
| 1–2 | 1.67 | 0.56; 5.03 | 0.356 |
| ≥3 | 1.08 | 0.32; 3.67 | 0.894 |
| Present illness c | |||
| Oncology | 5.00 | 0.86; 29.05 | 0.073 |
| Cardiovascular disease | 4.85 | 0.92; 25.68 | 0.063 |
| Infectious disease | 0.87 | 0.13; 5.78 | 0.889 |
| Gastrointestinal disease | 1.16 | 0.22; 5.97 | 0.854 |
| Other | 3.18 | 0.39; 25.58 | 0.276 |
| Malnutrition diagnosis d | |||
| Present | 60.72 | 23.97; 153.78 | <0.001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ouaijan, K.; Hwalla, N.; Kandala, N.-B.; Mpinga, E.K. Prevalence of Malnutrition in Hospitalized Patients in Lebanon Using Nutrition Risk Screening (NRS-2002) and Global Leadership Initiative on Malnutrition (GLIM) Criteria and Its Association with Length of Stay. Healthcare 2023, 11, 730. https://doi.org/10.3390/healthcare11050730
Ouaijan K, Hwalla N, Kandala N-B, Mpinga EK. Prevalence of Malnutrition in Hospitalized Patients in Lebanon Using Nutrition Risk Screening (NRS-2002) and Global Leadership Initiative on Malnutrition (GLIM) Criteria and Its Association with Length of Stay. Healthcare. 2023; 11(5):730. https://doi.org/10.3390/healthcare11050730
Chicago/Turabian StyleOuaijan, Krystel, Nahla Hwalla, Ngianga-Bakwin Kandala, and Emmanuel Kabengele Mpinga. 2023. "Prevalence of Malnutrition in Hospitalized Patients in Lebanon Using Nutrition Risk Screening (NRS-2002) and Global Leadership Initiative on Malnutrition (GLIM) Criteria and Its Association with Length of Stay" Healthcare 11, no. 5: 730. https://doi.org/10.3390/healthcare11050730