Abstract
Background: Pharmacists in community settings are recognized as highly accessible healthcare practitioners and demonstrate a crucial role in the primary prevention of cardiovascular disease. Evidence indicates that community pharmacists can make a significant impact on controlling cardiovascular disease risk factors, particularly on hypertension. Objectives: We aimed to assess the knowledge of community pharmacists in Saudi Arabia regarding cardiovascular disease risk factors. Methods: A cross-sectional study involving community pharmacists was conducted. The knowledge of cardiovascular disease risk factors was assessed with the Heart Disease Fact Questionnaire (HDFQ). A web link for an anonymous questionnaire was shared with the licensed community pharmacists in Saudi Arabia using the “Seha” platform of the Ministry of Health. Data analysis was performed with R version 4.0.5. Results: Three hundred seventy-four community pharmacists responded to the questionnaire. Many community pharmacists (94.4%) had satisfactory awareness of cardiovascular disease risk factors. The odds of having satisfactory HDFQ knowledge for community pharmacists seeing more than 20 individuals with diabetes per month were 20 times (AOR = 19.9, 95% CI: 1.73–260, and p = 0.019) more compared to those seeing fewer than 10 individuals with diabetes per month. The age of the community pharmacists and the average number of individuals with diabetes seen per month were found to be factors associated with satisfactory HDFQ knowledge. Conclusion: The practicing pharmacists had a substantial understanding of cardiovascular disease risk factors. In line with counseling and education, the implementation of community pharmacy models for improving the knowledge of pharmacists, particularly the young pharmacists, is needed to effectively assist patients with cardiovascular disease.
1. Introduction
Cardiovascular disease is the leading cause of mortality globally, accounting for an estimated 30% of all deaths [1]. The burden of cardiovascular disease increases due to the modern lifestyle that changed eating habits from organic to processed unhealthy food, as well as smoking and alcohol consumption [2]. In developing economies, epidemiological data on the incidence of cardiovascular disease risk factors are scarce. Cardiovascular disease can be prevented through the effective control and management of cardiovascular disease risk factors. Evidence suggests that the primary prevention of cardiovascular disease represents a cost-effective strategy and eventually reduces the burden of cardiovascular disease in the population [3]. There has been no attempt to derive a robust prevalence estimate of cardiovascular disease in Saudi Arabia, but the prevalence of chronic heart disease is 5.5% [4] and estimated to be higher in the future [5]. Moreover, many cardiac patients in Saudi Arabia possess the following risk factors: dyslipidemia, hypertension, and obesity [6]. The prevalence of dyslipidemia is between 20 and 40% [7], and of obesity, 24.7% [8]. Likewise, a recent study showed that about 31.4% of Saudis are hypertensive [6].
Patients often face difficulties in approaching primary care physicians, whereas healthcare costs are continuously increasing, which necessitates the greater integration of pharmacy professionals as providers of health services and members of the healthcare team [1,9,10,11,12]. Pharmacists working in community pharmacies are recognized as highly accessible healthcare professionals, and their role for the management of cardiovascular disease and associated risk factors is well-documented [13,14]. Further, the role of community pharmacists includes educating patients about diseases and counseling patients regarding medicines and medicines-related problems [15]. Community pharmacists improve the health of patients by reducing drug-related harms and advocating better medicine adherence, therefore preventing unnecessary hospital admissions [16].
An authoritative report in Saudi Arabia forecasted a three-fold increase in the economic burden of cardiovascular disease, from USD 3.5 billion to USD 9.8 billion, by 2035 [17]. A sedentary lifestyle and the consumption of unhealthy food are prevalent in Saudi Arabia. Likewise, recent data provide evidence that there is a rising trend of cardiovascular disease deaths across Saudi Arabia [4]. With the rising prevalence of cardiovascular disease risk factors and incidence of cardiovascular disease along with rising health care costs in Saudi Arabia, community pharmacists working in Saudi Arabia may indeed have a role in tackling the challenges pertinent to this public health issue. There is a scarcity of literature on the knowledge of cardiovascular disease among community pharmacists in Saudi Arabia. Therefore, we aimed to assess the knowledge of community pharmacists in Saudi Arabia regarding cardiovascular disease risk factors. In addition, we also determined the relationship between the knowledge of diagnostic cut-offs for common cardiovascular disease risk factors and Heart Disease Fact Questionnaire (HDFQ) score.
2. Material and Methods
2.1. Study Design and Setting
A cross-sectional study was conducted from May 2020 to March 2021. There are 8683 community pharmacies in Saudi Arabia [18]. The Ministry of Health (MOH) manages all the community pharmacies in the kingdom.
2.2. Data Collection
A 48-item questionnaire was adapted from the previous study, and permission was also sought from the study authors [19]. A web link for the validated English questionnaire was distributed to the licensed pharmacists working in the community pharmacies throughout Saudi Arabia. To avoid selection bias, all community pharmacists employed in 8683 community pharmacies received an invitation to participate in this study. A web link for the questionnaire was disseminated to the community pharmacists working in Saudi Arabia by using the “Seha” platform. Seha is an electronic platform that serves the health sector in Saudi Arabia by providing MOH-approved electronic services and aims to automate and unify procedures and services. Moreover, it provides electronic integration with the relevant authorities and a secure medium for the transmission of data and information [20].
The questionnaire consisted of four parts. The first part was for personal and demographic data and contained 9 questions. The second part tested the knowledge of community pharmacists about cardiovascular disease risk factors (e.g., smoking and diabetes are risk factors for developing heart disease, and high blood sugar puts a strain on the heart) using the widely validated Heart Disease Fact Questionnaire (HDFQ), a 25-item tool for assessing the knowledge of risk factors for heart disease [21,22]. The HDFQ has frequently been used in various study populations, with reliable test–retest reliability, internal consistency, and satisfactory discriminant validity [21]. The responses were true, false, or do not know. The final scores were summed up, and a total score >20 demonstrated good knowledge. The scores were also indicated in percentages. Participants with scores of less than 50% and between 50–69% showed low and moderate levels of knowledge, respectively. Participants with an HDFQ score greater than 70% demonstrated a good level of knowledge. Questions that <70% of the participants answered correctly were deemed unsatisfactory. The third part assessed the knowledge of diagnostic cut-off points for cardiovascular disease risk factors and consisted of eight questions. The questionnaire also had a brief statement describing the nature and purpose of this study and a consent part ensuring the anonymity and voluntary participation of the community pharmacists. The questionnaire was also validated among a pilot sample of community pharmacists. Completing the questionnaire took an average of 18 min. We also sent a reminder every month, via employees managing the “Seha” platform, for completing the questionnaire.
2.3. Sample Size and Statistical Analysis
Given an estimated community pharmacist population of 8419 [23] and based on a 95% confidence level and a 5% margin of error, we estimated an ideal sample size of 368 participants for this survey. Data analysis was performed with R version 4.0.5. Descriptive statistics was applied to report the general characteristics of the participants, correct responses of the HDFQ questionnaire, and knowledge of diagnostic cut-offs for common cardiovascular disease risk factors. Testing for normality of continuous variables was performed using the Shapiro–Wilk test. A binary logistic regression was conducted to identify factors associated with satisfactory HDFQ knowledge. A linear regression was also applied to evaluate the relationship between the knowledge of diagnostic cut-offs for common cardiovascular disease risk factors and HDFQ score. A p-value of <0.05 was taken as the level of significance between responses.
2.4. Ethical Considerations
This study was conducted according to the principles of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board of King Saud Medical City, prior to the initiation of this study (reference number: H1RI-06-Apr20-05). Agreeing or responding to the study questionnaire was considered as implied consent for participation.
3. Results
The general characteristics of the respondents are presented in Table 1. All community pharmacies received the study invitation, but only 374 community pharmacists participated in this study. About two-thirds (67%) of the respondents’ ages ranged between 25 and 34 years old. The majority (91%) of the respondents were males. About a quarter of the respondents had a Bachelor of Pharmacy qualification (73%) and less than ten years of practice as community pharmacists (75%). Sixty-two percent of the pharmacists had seen more than twenty, on average, hypertensive patients, as well as smokers, each month. Two hundred and sixty-four pharmacists (71%) claimed that they had seen over twenty patients with diabetes per month.

Table 1.
General characteristics of respondents.
The results of the correct responses of the HDFQ questionnaire are given in Table 2. In 16 questions, more than 90% of the respondents correctly answered the questions. Only one-third of the pharmacists correctly responded to “men with diabetes have a higher risk of heart disease than women with diabetes.”
Table 2.
Correct responses of HDFQ questionnaire.
About half of the respondents correctly identified the diagnostic cut-off points for hypertension (49.2%), diabetes (46.0%), and truncal obesity in females (48%). About the knowledge of truncal obesity in males and hypercholesterolemia, 58% and 41% correctly identified the diagnostic cut-off points, respectively (Table 3). As shown in Figure 1, there was a proportional relationship between the overall HDFQ score and knowledge of diagnostic cut-offs (p < 0.001).
Table 3.
Knowledge of diagnostic cut-offs for common cardiovascular disease risk factors.
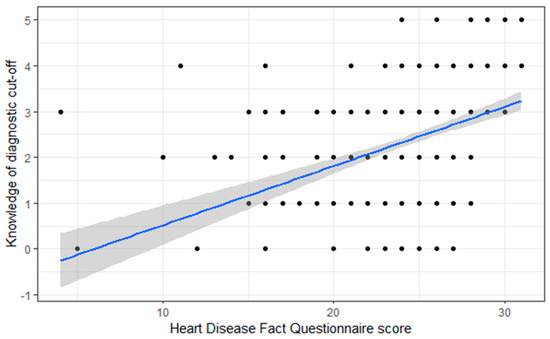
Figure 1.
Relation between HDFQ score and knowledge of diagnostic cut-offs.
The majority (94.4%) of the pharmacists had satisfactory awareness of cardiovascular disease risk factors. The age of the respondents and average number of individuals with diabetes seen per month were found to be factors associated with satisfactory HDFQ knowledge. Accordingly, the odds of having satisfactory HDFQ knowledge for pharmacists aged 25 to 34 and 35 to 44 years old were nearly 14-fold (AOR = 13.9, 95% CI: 1.19–175, and p = 0.040) and 13-fold (AOR = 13.0, 95% CI: 1.19–79.1, and p = 0.003) more, respectively, compared to patients aged 18 to 24 years old.
The odds of having satisfactory HDFQ knowledge for community pharmacists seeing more than 20 individuals with diabetes per month were 20 times (AOR = 19.9, 95% CI: 1.73–260, and p = 0.019) more compared to those seeing fewer than 10 individuals with diabetes per month (Table 4).
Table 4.
Association between HDFQ score category and socio-demographic characteristics.
4. Discussion
This study found that many pharmacists had satisfactory awareness of cardiovascular disease risk factors. Studies have demonstrated that patients have relatively lower knowledge of heart disease risks compared to healthcare professionals. A previous study reported a prevalence of 19.9% for knowledge of heart disease risks among Spanish speakers with diabetes [22]. Another study conducted in Ethiopia also reported almost half of cardiovascular disease patients had suboptimal knowledge regarding cardiovascular risk factors [24].
The findings from this study showed that the pharmacists had good knowledge on the biological and behavioral risk factors of cardiovascular disease. Additionally, the pharmacists were also majorly involved in cardiovascular disease primary prevention by lifestyle counseling and risk factors screening. Since the community pharmacists demonstrated a high level of knowledge, this finding could provide a foundation for feasibility research on the effectiveness of community pharmacy professionals in the screening of cardiovascular disease risk factors in Saudi Arabia.
This study further showed that the community pharmacists displayed good knowledge of both the behavioral and biological risk factors for cardiovascular disease. Nonetheless, in comparative terms, the knowledge of diabetes mellitus and hypercholesterolemia was lower, as only few community pharmacists correctly responded to the questions about the cut-offs for diabetes mellitus and hypercholesterolemia compared to those for hypertension. The reason for this might be due to the invasive nature of screening for diabetes mellitus (by glucometer) and hypercholesterolemia (by blood sample) that could demotivate community pharmacists as well as patients. Similarly, the finding related to diabetes was consistent with the previous report [19]. We also found a proportional relationship between the overall HDFQ score and knowledge of diagnostic cut-offs. This reflects that pharmacists with better knowledge regarding diagnostic cut-offs possess more knowledge regarding cardiovascular disease risk factors. This finding is consistent with a study performed in Nigeria [19] that reported 95.5% of the participants correctly identified cardiovascular disease risk factors.
The age of the respondents and average number of individuals with diabetes seen per month were found to be factors associated with satisfactory HDFQ knowledge. Compared to those aged less than 25 years, the older participants (25 to 45) had relatively higher odds of satisfactory knowledge of cardiovascular disease risk factors. A plausible explanation for this result may be related to work experience, as younger participants are usually new to the practice. Pharmacists providing services to more than 20 individuals with diabetes per month had higher odds of satisfactory knowledge of cardiovascular disease risk factors in comparison to those who provided services to fewer than 10 individuals with diabetes per month.
Health behavior knowledge is a crucial factor in the health belief model. The findings from this study may offer a foundation for future feasibility models focusing on the effectiveness of community pharmacists in cardiovascular disease risk screening in Saudi Arabia. It has been well-studied that the presence of cardiovascular disease risk factors is associated with higher death risk [25,26,27,28]. This risk can be managed with lifestyle and dietary counseling, which lowers the risk factors [29]. Pharmacists are, therefore, best suited to deliver this counseling because of being front-line service providers to the public. Community pharmacists could participate in the provision of education to patients via educational brochures and brief verbal discussions with each patient regarding cardiovascular disease risk factors. However, there is no specific model for the provision of education by community pharmacists in Saudi Arabia.
There are some limitations with this study. We used the HDFQ tool to assess the knowledge of pharmacists; however, this tool was initially designed for the lay public. The results reported here may be subjected to bias. A recall bias also may be introduced, as some questions relied on self-reporting.
5. Conclusions
The practicing pharmacists had a substantial understanding of cardiovascular disease risk factors. In line with counseling and education, the implementation of community pharmacy models for improving the knowledge of pharmacists, particularly the young pharmacists, is needed to effectively assist patients with cardiovascular disease. Pharmacists have updated courses or seminars, so that the variable of whether “they see or not” patients with a certain pathology results in being more up-to-date or more accurate in a diagnosis.
Author Contributions
Conceptualization, F.M.S., S.A. and I.A.A.-Z.; methodology, F.M.S., S.A. and I.A.A.-Z.; software, S.A. and F.M.S.; validation, S.A. and F.M.S.; formal analysis, S.A. and F.M.S.; data curation, M.S.A., T.A.A., A.Z.A. and A.Y.; writing—original draft preparation, S.A. and F.M.S.; writing—review and editing, M.S.A., T.A.A., A.Y., S.A., A.Z.A. and F.M.S.; supervision, S.A.; project administration, F.M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of King Saud Medical City prior to the initiation of this study (reference number: H1RI-06-Apr20-05).
Informed Consent Statement
Agreeing or responding to the study questionnaire was considered as implied consent for participation.
Data Availability Statement
The data used to analyze this survey will be provided by the corresponding author upon request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Prevention of Cardiovascular Disease: Guidelines for Assessment and Management of Total Cardiovascular Risk; World Health Organization: Geneva, Switzerland, 2007; Available online: https://apps.who.int/iris/handle/10665/43685 (accessed on 15 November 2022).
- Yusuf, S.; Reddy, S.; Ounpuu, S.; Anand, S. Global burden of cardiovascular diseases: Part II: Variations in cardiovascular disease by specific ethnic groups and geographic regions and prevention strategies. Circulation 2001, 104, 2855–2864. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Primary prevention of cardiovascular disease through population-wide motivational strategies: Insights from using smartphones in stroke prevention. BMJ Glob. Health 2016, 2, e000306. [Google Scholar] [CrossRef] [PubMed]
- Aljefree, N.; Ahmed, F. Prevalence of Cardiovascular Disease and Associated Risk Factors among Adult Population in the Gulf Region: A Systematic Review. Adv. Public Health 2015, 2015, 235101. [Google Scholar] [CrossRef]
- Al-Nozha, M.M.; Arafah, M.R.; Al-Mazrou, Y.Y.; Al-Maatouq, M.A.; Khan, N.B.; Khalil, M.Z.; Al-Khadra, A.H.; Al-Marzouki, K.; Abdullah, M.A.; Al-Harthi, S.S.; et al. Coronary artery disease in Saudi Arabia. Saudi Med. J. 2004, 25, 1165–1171. [Google Scholar] [PubMed]
- Ahmed, A.M.; Hersi, A.; Mashhoud, W.; Arafah, M.R.; Abreu, P.C.; Al Rowaily, M.A.; Al-Mallah, M.H. Cardiovascular risk factors burden in Saudi Arabia: The Africa Middle East Cardiovascular Epidemiological (ACE) study. J. Saudi Heart Assoc. 2017, 29, 235–243. [Google Scholar] [CrossRef]
- Al-Kaabba, A.F.; Al-Hamdan, N.A.; El Tahir, A.; Abdalla, A.M.; Saeed, A.A.; Hamza, M.A. Prevalence and Correlates of Dyslipidemia among Adults in Saudi Arabia: Results from a National Survey. Open J. Endocr. Metab. Dis. 2012, 02, 89–97. [Google Scholar] [CrossRef]
- Althumiri, N.A.; Basyouni, M.H.; AlMousa, N.; AlJuwaysim, M.F.; Almubark, R.A.; BinDhim, N.F.; Alkhamaali, Z.; Alqahtani, S.A. Obesity in Saudi Arabia in 2020: Prevalence, Distribution, and Its Current Association with Various Health Conditions. Healthcare 2021, 9, 311. [Google Scholar] [CrossRef]
- Joint British Societies’ consensus recommendations for the prevention of cardiovascular disease (JBS3). Heart 2014, 100 (Suppl. S2), ii1–ii67. [CrossRef]
- Blenkinsopp, A.; Anderson, C.; Armstrong, M. Systematic review of the effectiveness of community pharmacy-based interventions to reduce risk behaviours and risk factors for coronary heart disease. J. Public Health Med. 2003, 25, 144–153. [Google Scholar] [CrossRef]
- Morgado, M.; Rolo, S.; Castelo-Branco, M. Pharmacist intervention program to enhance hypertension control: A randomised controlled trial. Int. J. Clin. Pharm. 2011, 33, 132–140. [Google Scholar] [CrossRef]
- Perk, J.; De Backer, G.; Gohlke, H.; Graham, I.; Reiner, Z.; Verschuren, M.; Albus, C.; Benlian, P.; Boysen, G.; Cifkova, R.; et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts). Eur. Heart J. 2012, 33, 1635–1701. [Google Scholar] [CrossRef] [PubMed]
- George, J.; McNamara, K.; Stewart, K. The roles of community pharmacists in cardiovascular disease prevention and management. Australas Med. J. 2011, 4, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Santschi, V.; Chiolero, A.; Paradis, G.; Colosimo, A.L.; Burnand, B. Pharmacist interventions to improve cardiovascular disease risk factors in diabetes: A systematic review and meta-analysis of randomized controlled trials. Diabetes Care 2012, 35, 2706–2717. [Google Scholar] [CrossRef]
- Nazar, H.; Nazar, Z.; Portlock, J.; Todd, A.; Slight, S.P. A systematic review of the role of community pharmacies in improving the transition from secondary to primary care. Br. J. Clin. Pharmacol. 2015, 80, 936–948. [Google Scholar] [CrossRef]
- Mossialos, E.; Courtin, E.; Naci, H.; Benrimoj, S.; Bouvy, M.; Farris, K.; Noyce, P.; Sketris, I. From “retailers” to health care providers: Transforming the role of community pharmacists in chronic disease management. Health Policy 2015, 119, 628–639. [Google Scholar] [CrossRef]
- Jeddah Economic Gateway. Available online: https://jeg.org.sa/?q=printpdf/news/3978/details (accessed on 15 November 2022).
- Ministry of Health. Statistical Yearbook. Available online: https://www.moh.gov.sa/Ministry/Statistics/book/Documents/book-Statistics-2018.pdf (accessed on 15 November 2022).
- Amadi, C.E.; Lawal, F.O.; Mbakwem, A.C.; Ajuluchukwu, J.N.; Oke, D.A. Knowledge of cardiovascular disease risk factors and practice of primary prevention of cardiovascular disease by Community Pharmacists in Nigeria: A cross-sectional study. Int. J. Clin. Pharm. 2018, 40, 1587–1595. [Google Scholar] [CrossRef]
- SEHA. 2020. Available online: https://www.seha.sa/ (accessed on 15 November 2022).
- Wagner, J.; Lacey, K.; Chyun, D.; Abbott, G. Development of a questionnaire to measure heart disease risk knowledge in people with diabetes: The Heart Disease Fact Questionnaire. Patient Educ. Couns. 2005, 58, 82–87. [Google Scholar] [CrossRef]
- Wagner, J.; Abbott, G.; Lacey, K. Knowledge of heart disease risk among spanish speakers with diabetes: The role of interpreters in the medical encounter. Ethn. Dis. 2005, 15, 679–684. [Google Scholar] [PubMed]
- AlRuthia, Y.; Alsenaidy, M.A.; Alrabiah, H.K.; AlMuhaisen, A.; Alshehri, M. The status of licensed pharmacy workforce in Saudi Arabia: A 2030 economic vision perspective. Hum. Resour. Health 2018, 16, 28. [Google Scholar] [CrossRef]
- Negesa, L.B.; Magarey, J.; Rasmussen, P.; Hendriks, J.M.L. Patients’ knowledge on cardiovascular risk factors and associated lifestyle behaviour in Ethiopia in 2018: A cross-sectional study. PLoS ONE 2020, 15, e0234198. [Google Scholar] [CrossRef]
- Daviglus, M.L.; Pirzada, A.; Liu, K.; Yan, L.L.; Garside, D.B.; Dyer, A.R.; Hoff, J.A.; Kondos, G.T.; Greenland, P.; Stamler, J. Comparison of low risk and higher risk profiles in middle age to frequency and quantity of coronary artery calcium years later. Am. J. Cardiol. 2004, 94, 367–369. [Google Scholar] [CrossRef]
- Miura, K.; Daviglus, M.L.; Dyer, A.R.; Liu, K.; Garside, D.B.; Stamler, J.; Greenland, P. Relationship of blood pressure to 25-year mortality due to coronary heart disease, cardiovascular diseases, and all causes in young adult men: The Chicago Heart Association Detection Project in Industry. Arch. Intern. Med. 2001, 161, 1501–1508. [Google Scholar] [CrossRef] [PubMed]
- Rosengren, A.; Dotevall, A.; Eriksson, H.; Wilhelmsen, L. Optimal risk factors in the population: Prognosis, prevalence, and secular trends; data from Göteborg population studies. Eur. Heart J. 2001, 22, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Stamler, J.; Stamler, R.; Neaton, J.D.; Wentworth, D.; Daviglus, M.L.; Garside, D.; Dyer, A.R.; Liu, K.; Greenland, P. Low risk-factor profile and long-term cardiovascular and noncardiovascular mortality and life expectancy: Findings for 5 large cohorts of young adult and middle-aged men and women. JAMA 1999, 282, 2012–2018. [Google Scholar] [CrossRef] [PubMed]
- Stampfer, M.J.; Hu, F.B.; Manson, J.E.; Rimm, E.B.; Willett, W.C. Primary Prevention of Coronary Heart Disease in Women through Diet and Lifestyle. N. Engl. J. Med. 2000, 343, 16–22. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).