
Effect of COVID-19 Lockdowns on Eye Emergency Department, Increasing Prevalence of Uveitis and Optic Neuritis in the COVID-19 Era

Abstract
:1. Introduction
2. Materials and Methods
2.1. Methods
2.2. Statistical Methods
3. Results
3.1. Number of Patients
3.2. Time to Discharge
3.3. Trauma
3.4. Anterior Segment Diseases
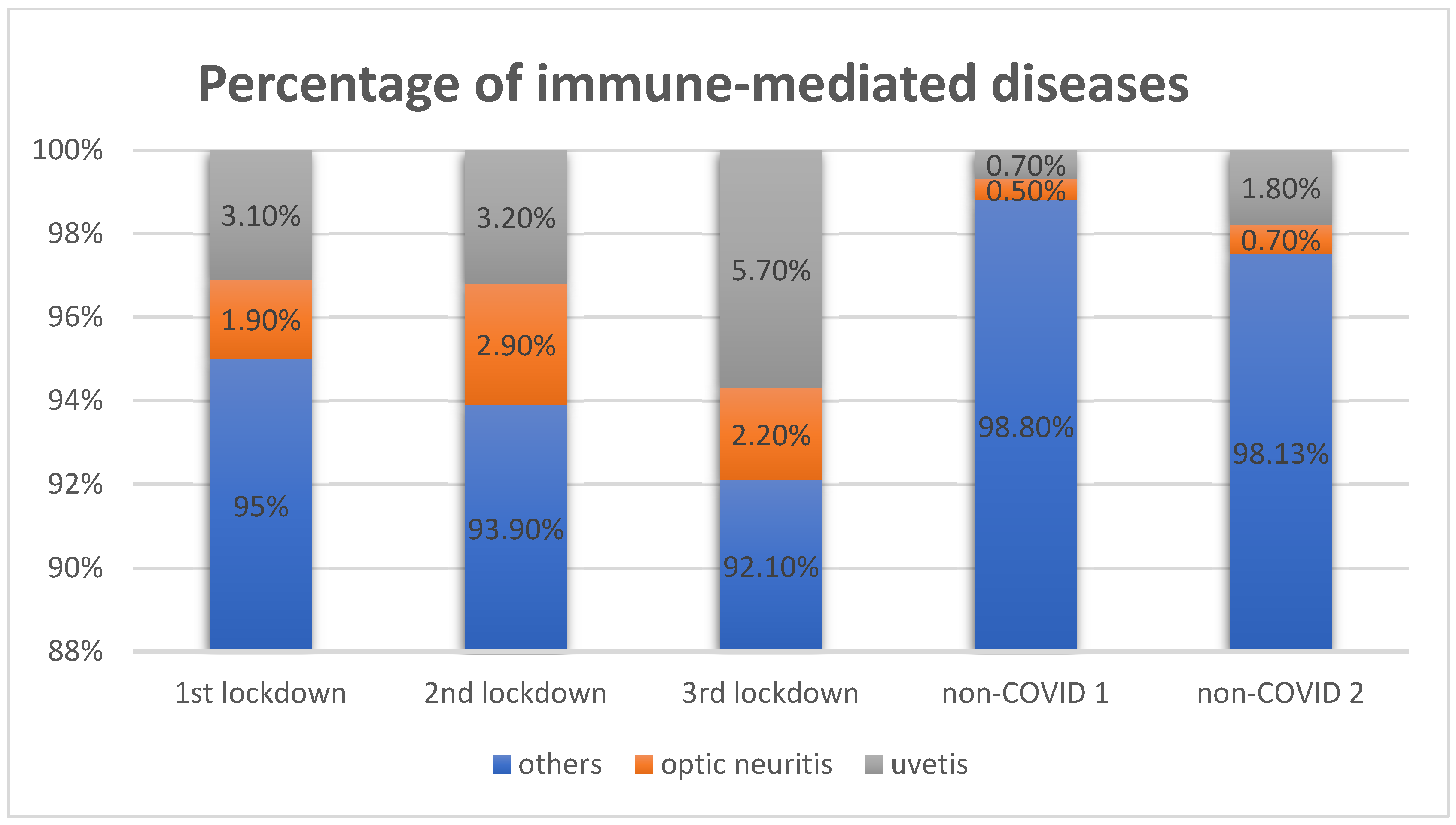
3.5. Posterior Segment and Immune-Mediated Diseases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.worldometers.info/coronavirus/ (accessed on 21 June 2022).
- Maab, H.; Mustafa, F.; Shabbir, S.J. Cardiovascular impact of COVID-19: An array of presentations: Cardiovascular impact of COVID-19. Acta Bio-Med. Atenei Parm. 2021, 92, e2021021. [Google Scholar] [CrossRef]
- Smith, E.; Hill, M.; Anderson, C.; Sim, M.; Miles, A.; Reid, D.; Mills, B. Lived Experience of Emergency Health Care Utilization during the COVID-19 Pandemic: A Qualitative Study. Prehospital Disaster Med. 2021, 36, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Kite, T.A.; Ladwiniec, A.; Owens, C.G.; Chase, A.; Shaukat, A.; Mozid, A.M.; O’Kane, P.; Routledge, H.; Perera, D.; Jain, A.K.; et al. Outcomes following PCI in CABG candidates during the COVID-19 pandemic: The prospective multicentre UK-ReVasc registry. Catheter. Cardiovasc. Interv. 2021, 99, 305–313. [Google Scholar] [CrossRef]
- Mafham, M.M.; Spata, E.; Goldacre, R.; Gair, D.; Curnow, P.; Bray, M.; Hollings, S.; Roebuck, C.; Gale, C.P.; A Mamas, M.; et al. COVID-19 pandemic and admission rates for and management of acute coronary syndromes in England. Lancet 2020, 396, 381–389. [Google Scholar] [CrossRef]
- Rudilosso, S.; Laredo, C.; Vera, V.; Vargas, M.; Renú, A.; Llull, L.; Obach, V.; Amaro, S.; Urra, X.; Torres, F.; et al. Acute Stroke Care Is at Risk in the Era of COVID-19: Experience at a Comprehensive Stroke Center in Barcelona. Stroke 2020, 51, 1991–1995. [Google Scholar] [CrossRef]
- Diegoli, H.; Magalhães, P.S.; Martins, S.C.; Moro, C.H.; França, P.H.; Safanelli, J.; Nagel, V.; Venancio, V.G.; Liberato, R.B.; Longo, A.L. Decrease in Hospital Admissions for Transient Ischemic Attack, Mild, and Moderate Stroke During the COVID-19 Era. Stroke 2020, 51, 2315–2321. [Google Scholar] [CrossRef]
- Park, D. II States limiting elective procedures in Hospitals, Resuming Surgery in All Settings. Available online: https://www.aao.org/practice-management/article/states-begin-easing-elective-procedure-restriction (accessed on 2 September 2021).
- Assi, M.; Abbas, S.; Nori, P.; Doll, M.; Godbout, E.; Bearman, G.; Stevens, M.P. Infection Prevention and Antimicrobial Stewardship Program Collaboration During the COVID-19 Pandemic: A Window of Opportunity. Curr. Infect. Dis. Rep. 2021, 23, 15. [Google Scholar] [CrossRef]
- Li, J.-P.O.; Thomas, A.A.; Kilduff, C.L.; Logeswaran, A.; Ramessur, R.; Jaselsky, A.; Sim, D.A.; Hay, G.R.; Thomas, P.B. Safety of video-based telemedicine compared to in-person triage in emergency ophthalmology during COVID-19. eClinicalMedicine 2021, 34, 100818. [Google Scholar] [CrossRef]
- Guo, Z.; Ma, N.; Wu, Y.; Yuan, H.; Luo, W.; Zeng, L.; Jie, H.; Li, S. The safety and feasibility of the screening for retinopathy of prematurity assisted by telemedicine network during COVID-19 pandemic in Wuhan, China. BMC Ophthalmol. 2021, 21, 258. [Google Scholar] [CrossRef]
- Sommer, A.C.; Blumenthal, E.Z. Telemedicine in ophthalmology in view of the emerging COVID-19 outbreak. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 2341–2352. [Google Scholar] [CrossRef]
- Fonda, S.J.; Bursell, S.-E.; Lewis, D.G.; Clary, D.; Shahon, D.; Horton, M.B. The Indian Health Service Primary Care-Based Teleophthalmology Program for Diabetic Eye Disease Surveillance and Management. Telemed. E-Health 2020, 26, 1466–1474. [Google Scholar] [CrossRef] [Green Version]
- Labiris, G.; Panagiotopoulou, E.-K.; Kozobolis, V.P. A systematic review of teleophthalmological studies in Europe. Int. J. Ophthalmol. 2018, 11, 314–325. [Google Scholar] [CrossRef]
- Malfatti, G.; Racano, E.; Site, R.D.; Gios, L.; Micocci, S.; Dianti, M.; Molini, P.B.; Allegrini, F.; Ravagni, M.; Moz, M.; et al. Enabling teleophthalmology during the COVID-19 pandemic in the Province of Trento, Italy: Design and implementation of a mHealth solution. PLoS ONE 2021, 16, e0257250. [Google Scholar] [CrossRef]
- Berkenstock, M.K.; Liberman, P.; McDonnell, P.J.; Chaon, B.C. Changes in patient visits and diagnoses in a large academic center during the COVID-19 pandemic. BMC Ophthalmol. 2021, 21, 139. [Google Scholar] [CrossRef]
- Mazzuca, D.; Borselli, M.; Gratteri, S.; Zampogna, G.; Feola, A.; Della Corte, M.; Guarna, F.; Scorcia, V.; Giannaccare, G. Applications and Current Medico-Legal Challenges of Telemedicine in Ophthalmology. Int. J. Environ. Res. Public Health 2022, 19, 5614. [Google Scholar] [CrossRef]
- Sharma, P.; Bhaskaran, K. Distancing? But still I-Care: Tele-Ophthalmology during COVID-19 era. Indian J. Ophthalmol. 2020, 68, 1243–1244. [Google Scholar] [CrossRef]
- Hong, N.; Yu, W.; Xia, J.; Shen, Y.; Yap, M.; Han, W. Evaluation of ocular symptoms and tropism of SARS-CoV-2 in patients confirmed with COVID-19. Acta Ophthalmol. 2020, 98, e649–e655. [Google Scholar] [CrossRef]
- Liu, Y.; Sawalha, A.H.; Lu, Q. COVID-19 and autoimmune diseases. Curr. Opin. Rheumatol. 2020, 33, 155–162. [Google Scholar] [CrossRef]
- Poyser, A.; Deol, S.S.; Osman, L.; Kuht, H.J.; Sivagnanasithiyar, T.; Manrique, R.; O Okafor, L.; DeSilva, I.; Sharpe, D.; Savant, V.; et al. Impact of COVID-19 pandemic and lockdown on eye emergencies. Eur. J. Ophthalmol. 2020, 31, 2894–2900. [Google Scholar] [CrossRef]
- Wickham, L.; Hay, G.; Hamilton, R.; Wooding, J.; Tossounis, H.; Da Cruz, L.; Siriwardena, D.; Strouthidis, N. The impact of COVID policies on acute ophthalmology services—Experiences from Moorfields Eye Hospital NHS Foundation Trust. Eye 2020, 34, 1189–1192. [Google Scholar] [CrossRef]
- Armarnik, S.; Kinori, M.; Elkader, A.A.; Meirovitch, S.B.; Kapelushnik, N.; Madgar, S.; Goldberg, H.; Sagiv, O.; Wygnanski-Jaffe, T.; Priel, A. COVID-19′s Influence on Ocular Emergency Visits at a Tertiary Referral Center and Its Relationship to Emergency Indications by the American Academy of Ophthalmology. J. Ophthalmol. 2021, 2021, 6682646. [Google Scholar] [CrossRef]
- Galindo-Ferreiro, A.; Sanchez-Tocino, H.; Varela-Conde, Y.; Diez-Montero, C.; Belani-Raju, M.; García-Sanz, R.; Diego-Alonso, M.; Llorente-Gonzalez, I.; Pazó-Jaudenes, C.; Schellini, S. Ocular emergencies presenting to an emergency department in Central Spain from 2013 to 2018. Eur. J. Ophthalmol. 2019, 31, 748–753. [Google Scholar] [CrossRef]
- Chen, L.; Deng, C.; Chen, X.; Zhang, X.; Chen, B.; Yu, H.; Qin, Y.; Xiao, K.; Zhang, H.; Sun, X. Ocular manifestations and clinical characteristics of 535 cases of COVID-19 in Wuhan, China: A cross-sectional study. Acta Ophthalmol. 2020, 98, e951–e959. [Google Scholar] [CrossRef]
- Güemes-Villahoz, N.; Burgos-Blasco, B.; García-Feijoó, J.; Sáenz-Francés, F.; Arriola-Villalobos, P.; Martinez-De-La-Casa, J.M.; Benítez-Del-Castillo, J.M.; De La Muela, M.H. Conjunctivitis in COVID-19 patients: Frequency and clinical presentation. Graefes Arch. Clin. Exp. Ophthalmol. 2020, 258, 2501–2507. [Google Scholar] [CrossRef]
- Samia-Aly, E.; Moussa, G.; Ch’Ng, S.W. The impact of COVID-19 on traumatic eye emergencies needing surgery. Eye 2021, 36, 899–900. [Google Scholar] [CrossRef]
- Patel, M.K.; Bergeri, I.; Bresee, J.S.; Cowling, B.J.; Crowcroft, N.S.; Fahmy, K.; Hirve, S.; Kang, G.; Katz, M.A.; Lanata, C.F.; et al. Evaluation of post-introduction COVID-19 vaccine effectiveness: Summary of interim guidance of the World Health Organization. Vaccine 2021, 39, 4013–4024. [Google Scholar] [CrossRef]
- Jasani, K.M.; Ivanova, T.; Sabatino, F.; Patton, N.; Dhawahir-Scala, F.; Chew, G.; Charles, S.; David, P.; Davies, A.; Jalil, A. Changing clinical patterns of Rhegmatogeneous Retinal Detachments during the COVID19 pandemic lockdown in the North West of the UK. Eur. J. Ophthalmol. 2020, 31, 2876–2880. [Google Scholar] [CrossRef]
- Zhao, M.; Li, J.; She, H.; Liu, N. The risk factors of the progression of rhegmatogenous retinal detachment on patients with the fourteen-day quarantine in the early period of COVID-19 outbreak. BMC Ophthalmol. 2021, 21, 215. [Google Scholar] [CrossRef]
- Shroff, D.; Narula, R.; Atri, N.; Chakravarti, A.; Gandhi, A.; Sapra, N.; Bhatia, G.; Pawar, S.; Narain, S. Endogenous fungal endophthalmitis following intensive corticosteroid therapy in severe COVID-19 disease. Indian J. Ophthalmol. 2021, 69, 1909–1914. [Google Scholar] [CrossRef]
- Sullivan, B.N.; Fischer, T. Age-Associated Neurological Complications of COVID-19: A Systematic Review and Meta-Analysis. Front. Aging Neurosci. 2021, 13, 653694. [Google Scholar] [CrossRef] [PubMed]
- Reichard, R.R.; Kashani, K.B.; Boire, N.A.; Constantopoulos, E.; Guo, Y.; Lucchinetti, C.F. Neuropathology of COVID-19: A spectrum of vascular and acute disseminated encephalomyelitis (ADEM)-like pathology. Acta Neuropathol. 2020, 140, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Benito-Pascual, B.; A Gegúndez, J.; Díaz-Valle, D.; Arriola-Villalobos, P.; Carreño, E.; Culebras, E.; Rodríguez-Avial, I.; Benitez-Del-Castillo, J.M. Panuveitis and Optic Neuritis as a Possible Initial Presentation of the Novel Coronavirus Disease 2019 (COVID-19). Ocul. Immunol. Inflamm. 2020, 28, 922–925. [Google Scholar] [CrossRef] [PubMed]
- Dalakas, M.C. Guillain-Barre syndrome: The first documented COVID-19-triggered autoimmune neurologic disease: More to come with myositis in the offing. Neurol. Neuroimmunol. Neuroinflamm. 2020, 7, e781. [Google Scholar] [CrossRef]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. An outbreak of severe Kawasaki-Like disease at the Italian epicentre of the SARS-CoV-2 epidemic: An observational cohort study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef]
- Picod, A.; Dinkelacker, V.; Savatovsky, J.; Trouiller, P.; Guéguen, A.; Engrand, N. SARS-CoV-2-associated encephalitis: Arguments for a post-infectious mechanism. Crit. Care 2020, 24, 658. [Google Scholar] [CrossRef]
- Burgos-Blasco, B.; Güemes-Villahoz, N.; Donate-Lopez, J.; Vidal-Villegas, B.; García-Feijóo, J. Optic nerve analysis in COVID-19 patients. J. Med. Virol. 2020, 93, 190–191. [Google Scholar] [CrossRef]


{kind=link}
| Whole Cohort | 1st Lockdown | 2nd Lockdown | 3rd Lockdown | Non-COVID 1 | Non-COVID 2 | p Value | |
|---|---|---|---|---|---|---|---|
| Number of patients (% of the whole cohort) | 2351 | 258 | 281 | 372 | 830 | 610 | * p < 0.001 |
| (100%) | (11%) | (12%) | (15.8%) | (35.3%) | (25.9%) | ||
| Sex: Malen (%) Female n (%) | 1146 | 92 (35.7%) | 126 (44.8%) | 175 (47%) | 411 (49.5%) | 342 (56.1%) | * p < 0.001 |
| 1205 | 166 (64.3%) | 155 (55.2%) | 197 (53%) | 419 (50.5%) | 268 (43.9%) | ** p = 0.014 | |
| Age: Median (Q1:Q3) | 52 | 49 | 56 | 53 | 51 | 54 | * p = 0.33 |
| 35–68 | 36–66 | 39–70 | 36–69 | 34–67 | 35–68 | ** p = 0.17 | |
| Chronic general disease n % of the group | 461 | 47 | 84 | 98 | 127 | 105 | * p < 0.0001 |
| 19.6% | 18.2% | 29.9% | 26.3% | 15.3% | 17.2% | ** p = 0.06 | |
| Ocular chronic disease present n % of the group | 758 | 85 | 104 | 126 | 259 | 184 | * p = 0.28 |
| 32.2% | 33% | 37% | 33.9% | 31.2% | 30.2% | ** p = 0.57 |
| 1st Lockdown | 2nd Lockdown | 3rd Lockdown | Non-COVID 1 | Non-COVID 2 | p Value | |
|---|---|---|---|---|---|---|
| Time spent in A&E until discharge, median (minutes) | 149 | 114 | 171 | 452 | 286 | * p < 0.001 ** p < 0.001 |
| Part of the day Night n (% of the group) | 32 (12.4%) | 23 (8.2%) | 32 (8.6%) | 104 (12.5%) | 44 (7.2%) | * p = 0.005 ** p = 0.18 |
| Admission to the hospital n (% of the group) | 12 (4.7%) | 7 (2.5%) | 11 (3%) | 18 (2.2%) | 12 (2%) | * p = 0.19 ** p = 0.33 |
| Clinical Diagnosis | Incidence per Month in COVID Lockdowns | Incidence per Month in Non-COVID Era | Part of the Whole Group COVID [%] | Part of the Whole Group Non-COVID [%] | p Value |
|---|---|---|---|---|---|
| Conjunctivitis | 23 | 138 | 7.6% | 19.1% | p = 0.0006 |
| Keratitis | 20 | 33 | 6.6% | 4.5% | p = 0.0079 |
| Dry eye | 10 | 37 | 3.2% | 5.1% | p = 0.728 |
| Hordeolum | 13 | 36 | 4.3% | 5% | p = 0.5688 |
| Subconjunctival hemorrhage | 13 | 36 | 4.2% | 4.9% | p = 0.5688 |
| COVID | Non-COVID | COVID- Part of the Whole Group [%] | Non-COVID Part of the Whole Group [%] | p Value | |
|---|---|---|---|---|---|
| Retinal detachment and tear | 46 | 48 | 5.1% | 3.3% | p = 0.254 |
| Macular disorders | 32 | 41 | 3.5% | 2.9% | p = 0.991 |
| Retinal vessel abnormalities | 10 | 19 | 1.1% | 1.3% | p = 0.296 |
| Vitreous detachment | 44 | 80 | 4.8% | 5.6% | p = 0.276 |
| Glaucoma | 37 | 48 | 4.1% | 3.3% | p = 0.959 |
| Optic neuritis | 21 | 8 | 2.3% | 0.6% | p = 0.0013 |
| Diagnosis | 1st Lockdown n = 258 | 2nd Lockdown n = 281 | 3rd Lockdown n = 372 | Non-COVID 1 n = 830 | Non-COVID 2 n = 610 | p Value |
|---|---|---|---|---|---|---|
| Uvetis | 8 | 9 | 21 | 6 | 11 | p < 0.0001 |
| Optic neuritis | 5 | 8 | 8 | 4 | 4 | p < 0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Przybek-Skrzypecka, J.; Szewczuk, A.; Kamińska, A.; Skrzypecki, J.; Pyziak-Skupień, A.; Szaflik, J.P. Effect of COVID-19 Lockdowns on Eye Emergency Department, Increasing Prevalence of Uveitis and Optic Neuritis in the COVID-19 Era. Healthcare 2022, 10, 1422. https://doi.org/10.3390/healthcare10081422
Przybek-Skrzypecka J, Szewczuk A, Kamińska A, Skrzypecki J, Pyziak-Skupień A, Szaflik JP. Effect of COVID-19 Lockdowns on Eye Emergency Department, Increasing Prevalence of Uveitis and Optic Neuritis in the COVID-19 Era. Healthcare. 2022; 10(8):1422. https://doi.org/10.3390/healthcare10081422
Chicago/Turabian StylePrzybek-Skrzypecka, Joanna, Alina Szewczuk, Anna Kamińska, Janusz Skrzypecki, Aleksandra Pyziak-Skupień, and Jacek Paweł Szaflik. 2022. "Effect of COVID-19 Lockdowns on Eye Emergency Department, Increasing Prevalence of Uveitis and Optic Neuritis in the COVID-19 Era" Healthcare 10, no. 8: 1422. https://doi.org/10.3390/healthcare10081422