

Medication Adherence in Hypertensive Individuals in Panama 2019: A National Cross-Sectional Study

 ,
, 

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Materials
2.2. Data Collection
2.3. Outcome Assessment
2.4. Exposure Variables
2.4.1. Sociodemographic Variables
2.4.2. Condition-Related Variables
2.4.3. Patient-Related Variables
2.5. Statistical Analysis
3. Results
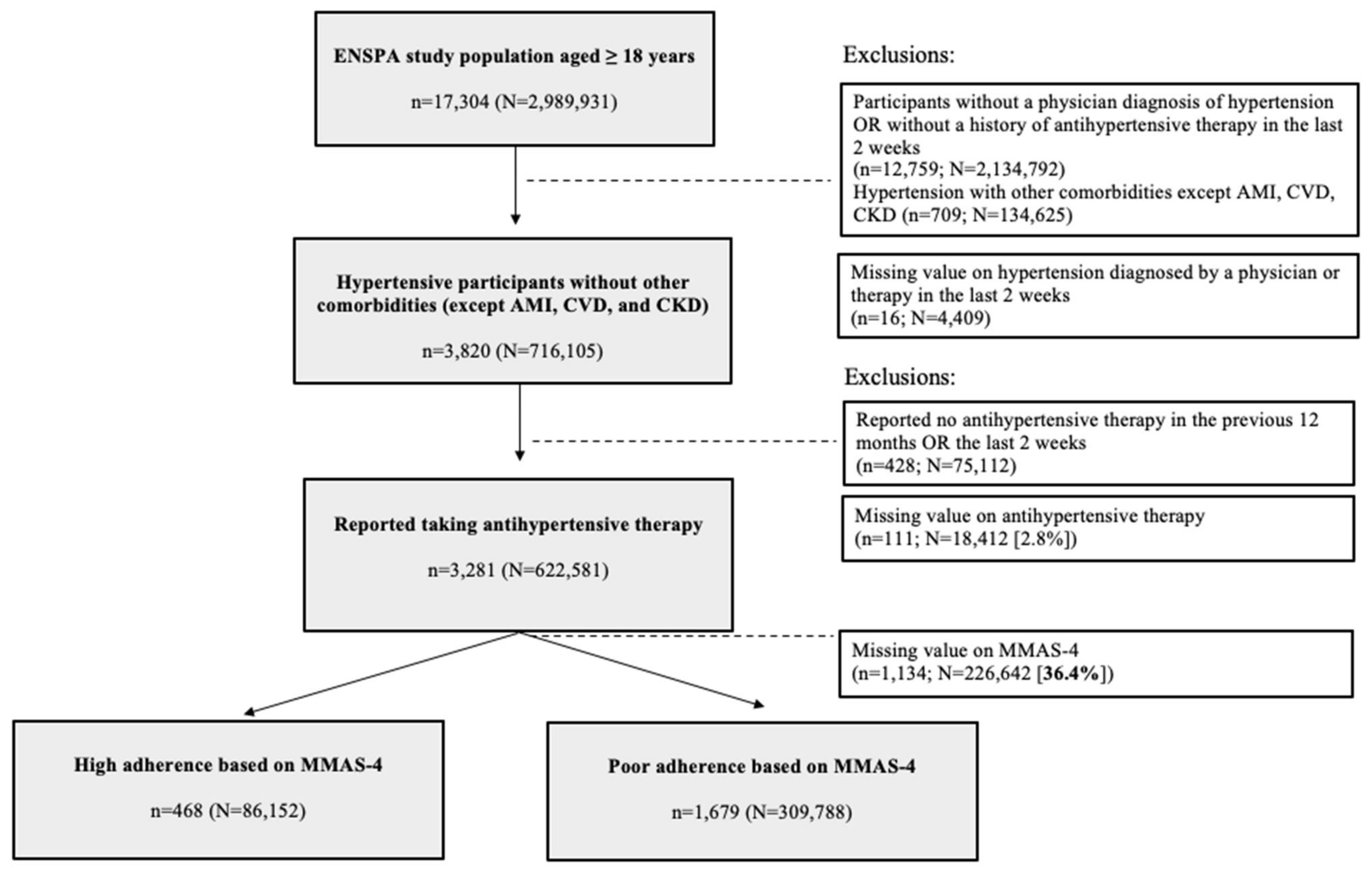
3.1. Participation Flowchart
3.2. Baseline Characteristics
3.3. Predictors of Low-Moderate Medication Adherence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension The Task Force for the Management of Arterial Hypertension of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH). Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Zhou, B.; Carrillo-Larco, R.M.; Danaei, G.; Riley, L.M.; Paciorek, C.J.; Stevens, G.A.; Gregg, E.W.; Bennett, J.E.; Solomon, B.; Singleton, R.K.; et al. Worldwide Trends in Hypertension Prevalence and Progress in Treatment and Control from 1990 to 2019: A Pooled Analysis of 1201 Population-Representative Studies with 104 Million Participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Mills, K.T.; Stefanescu, A.; He, J. The Global Epidemiology of Hypertension. Nat. Rev. Nephrol. 2020, 16, 223–237. [Google Scholar] [CrossRef]
- Lee, G.K.Y.; Wang, H.H.X.; Liu, K.Q.L.; Cheung, Y.; Morisky, D.E.; Wong, M.C.S. Determinants of Medication Adherence to Antihypertensive Medications among a Chinese Population Using Morisky Medication Adherence Scale. PLoS ONE 2013, 8, e62775. [Google Scholar] [CrossRef]
- World Health Organization. A Global Brief on Hypertension: Silent Killer, Global Public Health Crisis; World Health Organization: Geneva, Switzerland, 2013; Available online: https://www.who.int/publications/i/item/a-global-brief-on-hypertension-silent-killer-global-public-health-crisis-world-health-day-2013 (accessed on 20 August 2022).
- Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Kubik, M.; Li, L.; et al. Screening for Hypertension in Adults: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA J. Am. Med. Assoc. 2021, 325, 1650–1656. [Google Scholar] [CrossRef]
- Krousel-Wood, M.; Thomas, S.; Muntner, P.; Morisky, D. Medication Adherence: A Key Factor in Achieving Blood Pressure Control and Good Clinical Outcomes in Hypertensive Patients. Curr. Opin. Cardiol. 2004, 19, 357–362. [Google Scholar] [CrossRef]
- Carvalho, A.S.; Santos, P. Medication Adherence In Patients With Arterial Hypertension: The Relationship With Healthcare Systems’ Organizational Factors. Patient Prefer. Adherence 2019, 13, 1761–1774. [Google Scholar] [CrossRef]
- Cutler, R.L.; Fernandez-Llimos, F.; Frommer, M.; Benrimoj, C.; Garcia-Cardenas, V. Economic Impact of Medication Non-Adherence by Disease Groups: A Systematic Review. BMJ Open 2018, 8, e016982. [Google Scholar] [CrossRef]
- World Health Organization. Adherence to Long-Term Therapies-Evidence for Action; World Health Organization: Geneva, Switzerland, 2003; Available online: https://apps.who.int/iris/handle/10665/42682 (accessed on 20 August 2022).
- Burnier, M. Medication Adherence and Persistence as the Cornerstone of Effective Antihypertensive Therapy Terminology and Measurement of Medication-Taking Behavior Medication-Taking Behavior Encompasses Both Medication Adherence and Persistence, Terms for Which Distinct Defi. J. Hypertens. 2006, 19, 1190–1196. [Google Scholar] [CrossRef]
- Mc Donald Posso, A.J.; Motta Borrel, J.A.; Fontes, F.; Cruz Gonzalez, C.E.; Pachón Burgos, A.A.; Ortega, A.C. High Blood Pressure in Panama: Prevalence, Sociodemographic and Biologic Profile, Treatment, and Control (STROBE). Medicine 2014, 93, e101. [Google Scholar] [CrossRef] [PubMed]
- Instituto Conmemorativo Gorgas de Estudios de la Salud Sistema de Información Geográfico de Enfermedades Cardiovasculares. Available online: http://www.gorgas.gob.pa/SiGCARDIOVASCULARES/Datos.htm (accessed on 20 August 2022).
- Conte, E.; Morales, Y.; Niño, C.; Zamorano, C.; Benavidez, M.; Donato, M.; Llorach, C.; Gómez, B.; Toro, J. La Adherencia a Los Medicamentos En Pacientes Hipertensos y En Muestra de La Población General Characterization of Medication Adherence in a Sample of the General Population and Another of Hypertensive Patients in Panama. Ofil 2020, 30, 313–323. [Google Scholar]
- Montenegro Mendoza, R.; Moreno Velasquez, I.; Fontes, F.; Quintana, H. Prevalence of Central Obesity According to Different Definitions in Normal Weight Adults of Two Cross-Sectional Studies in Panama. Lancet Reg. Health Am. 2022, 10, 100215. [Google Scholar] [CrossRef]
- del Río, A.I.; Velásquez, I.M.; Roa, R.; Montenegro Mendoza, R.; Quintana, H.K. Prevalence of Hypertension and Possible Risk Factors of Hypertension Unawareness among Individuals Aged 30–75 Years from Two Panamanian Provinces: Results from Population-Based Cross-Sectional Studies, 2010 and 2019. PLoS ONE 2022, (In press).
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and Predictive Validity of a Self-Reported Measure of Medication Adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef]
- Cinar, F.I.; Mumcu, Ş.; Kiliç, B.; Polat, Ü.; Bal Özkaptan, B. Assessment of Medication Adherence and Related Factors in Hypertensive Patients: The Role of Beliefs About Medicines. Clin. Nurs. Res. 2021, 30, 985–993. [Google Scholar] [CrossRef]
- Algabbani, F.M.; Algabbani, A.M. Treatment Adherence among Patients with Hypertension: Findings from a Cross-Sectional Study. Clin. Hypertens. 2020, 26, 18. [Google Scholar] [CrossRef]
- Ramírez Pinzón, C.J. Adherencia a La Farmacoterapia En Pacientes Hipertensos Ambulatorios Que Asisten al Programa de Control de Hipertensión Arterial En El Hospital Jorge Cristo Sahium, Norte de Santander (Colombia). Cienc. Tecnol. Para Salud Vis. Ocul. 2015, 12, 27–35. [Google Scholar] [CrossRef]
- Fundación Farmaindustria. Encuesta Sobre Adherencia Terapéutica en España; Fundación Farmaindustria: Barcelona, Spain, 2015. Available online: https://www.farmaindustria.es/web/wp-content/uploads/sites/2/2016/12/Informe-Estudio-de-adherencia-anx.pdf (accessed on 20 August 2022).
- Formetin-Zayas, M.; Carbajales-León, E.B.; Medina-Fuentes, G.; Formetin-Zayas, D.M.; Formetin-Zayas, M. Adherencia Terapéutica En Pacientes Hipertensos de Un Consultorio Médico Perteneciente al Policlínico Universitario “Joaquín de Agüero y Agüero”. Rev. Inf. Cient. 2021, 100, 1–11. [Google Scholar]
- Luna Breceda, U.; Haro-Vázquez, S.d.R.; Uriostegui-Espíritu, L.C.; de Jesús Barajas-Gómez, T.; Rosas-Navarro, D.A. Nivel de Adherencia Terapéutica En Pacientes Con Hipertensión Arterial: Experiencia En Una Unidad de Medicina Familiar de Zapopan Jalisco, México. Aten. Fam. 2017, 24, 116–120. [Google Scholar] [CrossRef]
- Aid Kunert, J. Adherencia al Tratamiento Antihipertensivo En Pacientes Ambulatorios de Un Hospital Urbano. Rev. Virtual Soc. Parag. Medina Interna 2015, 2, 43–51. [Google Scholar] [CrossRef]
- Limaylla La Torre, M.L. Adherencia al Tratamiento Farmacológico en Pacientes Adultos Mayores Con Hipertensión Arterial del Centro de Atención Primaria III Huaycan–EsSalud; Universidad Nacional Mayor de San Marcos: Lima, Peru, 2016; Available online: https://cybertesis.unmsm.edu.pe/handle/20.500.12672/5273 (accessed on 20 August 2022).
- Valencia-Monsalvez, F.; Mendoza-Parra, S.; Luengo-Machuca, L. Evaluation of Morisky Medication Adherence Scale (MMAS-8) in Older Adults of a Primary Health Care Center in Chile. Rev. Peru Med. Exp. Salud Publica 2017, 34, 245–249. [Google Scholar] [CrossRef]
- Pan, J.; Wu, L.; Wang, H.; Lei, T.; Hu, B.; Xue, X.; Li, Q. Determinants of Hypertension Treatment Adherence among a Chinese Population Using the Therapeutic Adherence Scale for Hypertensive Patients. Medicine 2019, 98, e16116. [Google Scholar] [CrossRef]
- Uchmanowicz, B.; Jankowska, E.A.; Uchmanowicz, I.; Morisky, D.E. Self-Reported Medication Adherence Measured With Morisky Medication Adherence Scales and Its Determinants in Hypertensive Patients Aged ≥60 Years: A Systematic Review and Meta-Analysis. Front. Pharmacol. 2019, 10, 168. [Google Scholar] [CrossRef]
- Tola Gemeda, A.; Regassa, L.D.; Weldesenbet, A.B.; Merga, B.T.; Legesse, N.; Tusa, B.S. Adherence to Antihypertensive Medications and Associated Factors among Hypertensive Patients in Ethiopia: Systematic Review and Meta-Analysis. SAGE Open Med. 2020, 8, 205031212098245. [Google Scholar] [CrossRef]
- Hussein, A.; Awad, M.S.; Mahmoud, H.E.M. Patient Adherence to Antihypertensive Medications in Upper Egypt: A Cross-Sectional Study. Egypt. Heart J. 2020, 72, 29. [Google Scholar] [CrossRef]
- De Oliveira-Filho, A.D.; Morisky, D.E.; Neves, S.J.F.; Costa, F.A.; de Lyra, D.P. The 8-Item Morisky Medication Adherence Scale: Validation of a Brazilian-Portuguese Version in Hypertensive Adults. Res. Soc. Adm. Pharm. 2014, 10, 554–561. [Google Scholar] [CrossRef]
- Carmel, S. Health and Well-Being in Late Life: Gender Differences Worldwide. Front. Med. 2019, 6, 218. [Google Scholar] [CrossRef]
- Rosenberg, M.W.; Wilson, K. Gender, Poverty and Location: How Much Difference Do They Make in the Geography of Health Inequalities? Soc. Sci. Med. 2000, 51, 275–287. [Google Scholar] [CrossRef]
- Steiner, J.F.; Ho, P.M.; Beaty, B.L.; Dickinson, L.M.; Hanratty, R.; Zeng, C.; Tavel, H.M.; Havranek, E.P.; Davidson, A.J.; Magid, D.J.; et al. Sociodemographic and Clinical Characteristics Are Not Clinically Useful Predictors of Refill Adherence in Patients with Hypertension. Circ. Cardiovasc. Qual. Outcomes 2009, 2, 451–457. [Google Scholar] [CrossRef]
- Mahmoud, M.I.H. Compliance with Treatment of Patients with Hypertension in Almadinah Almunawwarah: A Community-Based Study. J. Taibah. Univ. Med. Sci. 2012, 7, 92–98. [Google Scholar] [CrossRef][Green Version]
- Berrington de Gonzalez, A.; Hartge, P.; Cerhan, J.R.; Flint, A.J.; Hannan, L.; MacInnis, R.J.; Moore, S.C.; Tobias, G.S.; Anton-Culver, H.; Beane Freeman, L.; et al. Body-Mass Index and Mortality among 1.46 Million White Adults. N. Engl. J. Med. 2010, 363, 2211–2219. [Google Scholar] [CrossRef] [PubMed]
- Gualdi-russo, E.; Rinaldo, N.; Masotti, S.; Bramanti, B.; Zaccagni, L. Sex Differences in Body Image Perception and Ideals: Analysis of Possible Determinants. Int. J. Environ. Res. Public Health 2022, 19, 2745. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Jang, M.H. The Influence of Body Image, Insight, and Mental Health Confidence on Medication Adherence in Young Adult Women with Mental Disorders. Int. J. Environ. Res. Public Health 2021, 18, 3866. [Google Scholar] [CrossRef]
- Ministerio de Salud de Panamá. Normas Técnico Administrativas de los Programas de Salud de Adulto y Adulto Mayor; Ministerio de Salud de Panamá: Panama City, Panama, 2018. Available online: https://www.minsa.gob.pa/sites/default/files/programas/programas_de_salud_de_adulto_y_adulto_mayor_resolucion_1.pdf (accessed on 20 August 2022).


{kind=link}
| National N = 622,581 % (95% CI) | Women N = 334,107 % (95% CI) | Men N = 288,474 % (95% CI) | |
|---|---|---|---|
| Sociodemographics | |||
| Age in years median (IQR) | 61 (49–72) | 59 (47–70) | 63 (52–73) |
| Ethnicity | |||
| Caucasian | 23.5 (20.8–26.6) | 23.0 (20.4–25.8) | 24.2 (19.2–30.0) |
| Afro-Panamanian | 18.4 (16.1–21.1) | 16.6 (14.3–19.1) | 20.6 (16.4–25.6) |
| Mestizo | 49.6 (46.6–52.7) | 52.5 (49.4–55.7) | 46.3 (40.9–51.8) |
| Indigenous | 4.7 (3.7–5.9) | 4.7 (3.6–6.2) | 4.7 (3.1–7.0) |
| Asians and others | 3.7 (2.7–5.0) | 3.2 (2.2–4.6) | 4.2 (2.6–6.9) |
| Regions | |||
| Urban | 73.2 (70.8–75.4) | 73.5 (71.1–75.8) | 72.8 (68.4–76.7) |
| Rural | 25.5 (23.3–27.8) | 25.6 (23.4–28.0) | 25.3 (21.5–29.6) |
| Indigenous | 1.4 (1.0–1.8) | 0.9 (0.6–1.3) | 1.9 (1.3–2.9) |
| Education | |||
| Higher education | 19.3 (16.6–22.2) | 16.9 (14.6–19.4) | 22.1 (17.2–27.9) |
| Secondary education | 43.3 (40.3–46.4) | 43.2 (40.1–46.4) | 43.5 (38.0–49.1) |
| Primary education | 33.0 (30.3–35.7) | 34.8 (32.9–38.8) | 29.7 (25.2–34.5) |
| No education | 4.4 (3.6–5.5) | 4.1 (3.3–5.2) | 4.8 (3.3–6.9) |
| Condition-related | |||
| Current smoker | 4.2 (3.0–5.8) | 2.4 (1.5–3.7) | 6.2 (4.0–9.6) |
| BMI categories | |||
| Normal (18.5–24.9 kg/m2) | 20.3 (17.7–23.2) | 25.6 (13.2–18.0) | 25.4 (20.7–30.7) |
| Overweight (25–29.9 kg/m2) | 35.4 (32.4–38.6) | 32.2 (29.2–35.4) | 38.1 (32.7–43.7) |
| Obese (≥30.0 kg/m2) | 44.2 (41.0–47.5) | 50.7 (47.3–54.0) | 35.4 (29.8–41.5) |
| Alcohol consumption | |||
| Non-drinker | 88.0 (85.7–90.0) | 93.0 (91.1–94.6) | 82.2 (77.7–86.0) |
| Moderate drinker | 4.9 (3.6–6.5) | 3.0 (1.9–4.5) | 7.1 (4.8–10.3) |
| Excessive drinker | 7.1 (5.6–9.0) | 8.3 (6.2–10.9) | 5.3 (3.3–8.3) |
| Patient-related | |||
| Self-reported comorbidities | |||
| CKD, CVD and/or AMI | 4.2 (3.0–5.9) | 2.6 (1.7–3.8) | 6.2 (3.9–9.6) |
| Anxiety and/or depression | 3.0 (2.1–4.4) | 3.9 (2.7–5.4) | 2.1 (0.8–5.1) |
| Time from hypertension diagnosis | |||
| Antihypertensive medication intake two weeks before the interview | 35.0 (32.0–38.1) | 33.6 (30.7–36.7) | 36.7 (31.3–42.4) |
| Less than a year before the interview | 9.3 (7.7–11.1) | 9.0 (7.4–10.8) | 9.6 (7.0–13.2) |
| 1–5 years before the interview | 19.5 (17.2–21.9) | 19.5 (17.2–22.1) | 19.4 (15.5–24.0) |
| ≥6 years before the interview | 36.2 (33.4–39.1) | 37.9 (34.9–41.0) | 34.3 (29.4–39.5) |
| Health checkups frequency | |||
| None | 14.7 (12.6–17.2) | 11.5 (9.2–14.4) | 20.5 (16.4–25.3) |
| 1–2 yearly | 57.6 (54.5–60.6) | 55.9 (52.1–59.6) | 60.4 (55.1–65.4) |
| ≥3 yearly | 27.7 (25.1–30.4) | 29.1 (26.4–32.0) | 26.1 (21.6–31.1) |
| National N = 622,581 % (95% CI) | Urban N = 455,434 % (95% CI) | Rural N = 158,649 % (95% CI) | Indigenous N = 8498 % (95% CI) | |
|---|---|---|---|---|
| The 4-items MMAS | ||||
| Replied yes to query “Do you ever forget to take your medicine?” | 33.6 (30.1–37.4) | 32.9 (28.3–37.7) | 35.3 (30.6–40.4) | 43.3 (25.5–63.1) |
| Replied yes to query “Are you careless at time about taking your medicine?” | 51.1 (47.3–54.9) | 52.3 (47.4–57.2) | 48.8 (43.7–53.9) | 31.5 (17.1–50.8) |
| Replied yes to query “When you feel better, do you sometimes stop taking your medicines?” | 24.0 (20.9–26.8) | 21.9 (18.4–25.8) | 25.8 (21.5–30.6) | 69.9 (52.2–83.2) |
| Replied yes to query “Sometimes, if you feel worse when you take the medicine, do you stop taking it?” | 41.6 (38.0–45.2) | 40.4 (35.9–45.0) | 45.8 (40.8–50.9) | 27.8 (16.1–43.5) |
| Low-moderate adherence MMAS: at least a “yes” reply to any of the four queries | 78.2 (74.7–81.0) | 77.8 (73.2–81.8) | 79.0 (74.6–82.8) | 87.4 (65.5–96.2) |
| National N = 622,580 % (95% CI) | Women N = 334,108 % (95% CI) | Men N = 288,474 % (95% CI) | |
|---|---|---|---|
| Sociodemographics | |||
| Sex | |||
| Men | 74.4 (67.5–80.4) | NA | NA |
| Women | 81.4 (78.4–84.0) | NA | NA |
| Education | |||
| Higher education | 75.3 (64.8–83.4) | 84.4 (76.8–89.8) | 67.2 (48.6–81.6) |
| Secondary education | 81.8 (76.3–86.2) | 83.1 (78.4–86.9) | 80.0 (68.1–88.2) |
| Primary education | 76.0 (70.3–81.0) | 79.0 (73.6–83.6) | 72.2 (60.8–81.3) |
| No formal education | 77.2 (65.8–85.6) | 76.7 (63.6–86.2) | 77.8 (55.6–90.7) |
| Condition-related | |||
| Current smoker | 92.0 (75.8–97.7) | 85.0 (56.0–96.2) | 98.5 (89.4–99.8) |
| BMI categories | |||
| Normal (18.5–24.9 kg/m2) | 76.7 (66.6–84.5) | 76.9 (66.3–85.0) | 76.5 (60.1–87.6) |
| Overweight (25–29.9 kg/m2) | 77.1 (71.3–82.1) | 81.0 (75.5–85.6) | 72.9 (62.2–81.5) |
| Obese (≥30.0 kg/m2) | 82.3 (77.0–86.7) | 84.6 (80.2–88.2) | 78.2 (64.3–87.6) |
| Alcohol consumption | |||
| Non-drinker | 77.6 (73.9–80.9) | 81.1 (78.0–83.9) | 72.6 (64.7–79.3) |
| Moderate drinker | 86.8 (69.8–94.9) | 88.2 (56.6–97.7) | 85.9 (61.7–95.8) |
| Excessive drinker | 79.7 (62.6–90.2) | 81.1 (64.5–91.0) | 79.1 (54.6–92.2) |
| Patient-related | |||
| CKD, CVD, and/or AMI | 61.8 (40.0–79.7) | 88.7 (70.8–96.2) | 52.0 (28.0–75.2) |
| Anxiety and/or depression | 88.6 (73.4–95.6) | 89.7 (73.7–96.4) | 84.2 (26.8–98.7) |
| Time from hypertension diagnosis | |||
| Antihypertensive medication intake at least two weeks before the interview | 86.2 (80.4–90.5) | 83.7 (76.7–88.8) | 89.2 (78.3–94.9) |
| Less than a year before the interview | 74.4 (62.5–83.6) | 79.4 (68.2–87.4) | 69.6 (48.4–84.8) |
| 1–5 years before the interview | 73.4 (64.9–80.5) | 79.1 (72.6–84.4) | 66.4 (50.1–79.5) |
| ≥6 years before the interview | 77.3 (71.8–81.9) | 81.6 (77.1–85.5) | 71.5 (60.5–80.5) |
| Health checkups frequency | |||
| None | 80.9 (68.0–89.4) | 84.8 (73.9–91.7) | 77.2 (53.7–90.8) |
| 1–2 yearly | 79.6 (75.3–83.3) | 80.6 (76.4–84.3) | 78.4 (70.1–84.9) |
| ≥3 yearly | 74.9 (68.0–80.8) | 81.6 (76.6–85.7) | 65.9 (52.1–77.4) |
| Women | Men | |||
|---|---|---|---|---|
| Sociodemographic | Crude OR (95% CI) | Adjusted * OR (95% CI) | Crude OR (95% CI) | Adjusted * OR (95% CI) |
| Age in years | 0.99 (0.98–1.00) | 0.99 (0.98–1.00) | 0.99 (0.96–1.01) | 1.00 (0.97–1.03) |
| Regions | ||||
| Urban | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| Rural | 0.67 (0.47–0.97) | 0.66 (0.42–1.03) | 1.80 (0.97–3.36) | 1.77 (0.78–3.98) |
| Indigenous | 1.66 (0.35–8.01) | 5.15 (1.40–18.98) | 2.55 (0.45–14.51) | 2.49 (0.22–27.91) |
| Education | ||||
| Higher education | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| Secondary education | 0.91 (0.51–1.62) | 0.90 (0.48–1.70) | 1.95 (0.73–5.23) | 2.94 (1.03–8.36) |
| Primary education | 0.70 (0.39–1.24) | 0.76 (0.38–1.56) | 1.27 (0.50–3.18) | 1.43 (0.49–4.13) |
| No education | 0.61 (0.28–1.36) | 0.77 (0.28–2.14) | 1.71 (0.48–6.06) | 0.97 (0.19–5.05) |
| Condition-related | ||||
| Current smoker | 1.31 (0.30–5.63) | 1.81 (0.33–9.85) | 24.24 (3.11–118.72) | 16.74 (1.83–152.70) |
| BMI categories | ||||
| Normal (18.5–24.9 kg/m2) | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| Overweight (25–29.9 kg/m2) | 1.28 (0.69–2.38) | 1.35 (0.73–2.50) | 0.83 (0.33–2.05) | 0.75 (0.32–1.78) |
| Obese (≥30.0 kg/m2) | 1.65 (0.90–3.03) | 1.49 (0.80–2.77) | 1.10 (0.39–3.06) | 1.52 (0.59–3.93) |
| Alcohol consumption | ||||
| Non-drinker | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| Moderate drinker | 1.75 (0.31–9.74) | 1.11 (0.20–6.06) | 2.29 (0.60–8.79) | 2.23 (0.44–11.43) |
| Excessive drinker | 1.00 (0.42–2.40) | 0.56 (0.23–1.39) | 1.42 (0.43–4.66) | 0.93 (0.29–2.97) |
| Patient-related | ||||
| CKD, CVD and/or AMI | 1.82 (0.57–5.86) | 1.73 (0.41–7.41) | 0.33 (0.11–0.95) | 0.44 (0.15–1.34) |
| Anxiety and/or depression | 2.04 (0.66–6.30) | 4.89 (1.36–17.49) | 0.78 (0.08–7.85) | 0.78 (0.08–7.85) |
| Time from hypertension diagnosis | ||||
| Antihypertensive medication intake at least two weeks before the interview | 1.15 (0.68–1.94) | 1.34 (0.61–2.94) | 3.27 (1.26–8.49) | 4.35 (1.11–17.11) |
| Less than a year before the interview | 0.87 (0.45–1.65) | 1.33 (0.66–2.68) | 0.91 (0.33–2.50) | 1.14 (0.37–3.52) |
| 1–5 years before the interview | 0.85 (0.54–1.34) | 1.06 (0.50–2.23) | 0.79 (0.34–1.81) | 1.12 (0.35–3.62) |
| ≥6 years before the interview | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
| Health checkups frequency | ||||
| None | 1.26 (0.60–2.65) | 1.50 (0.68–3.32) | 1.75 (0.52–5.83) | 2.97 (0.63–13.88) |
| 1–2 yearly | 0.82 (0.53–1.28) | 0.82 (0.53–1.28) | 1.88 (0.91–3.86) | 1.61 (0.78–3.32) |
| ≥3 yearly | 1 (reference) | 1 (reference) | 1 (reference) | 1 (reference) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guerra, C.; Conte, E.; Del Rio, A.I.; Motta, J.; Moreno Velásquez, I.; Quintana, H.K. Medication Adherence in Hypertensive Individuals in Panama 2019: A National Cross-Sectional Study. Healthcare 2022, 10, 2244. https://doi.org/10.3390/healthcare10112244
Guerra C, Conte E, Del Rio AI, Motta J, Moreno Velásquez I, Quintana HK. Medication Adherence in Hypertensive Individuals in Panama 2019: A National Cross-Sectional Study. Healthcare. 2022; 10(11):2244. https://doi.org/10.3390/healthcare10112244
Chicago/Turabian StyleGuerra, Carlos, Eric Conte, Angela Isabel Del Rio, Jorge Motta, Ilais Moreno Velásquez, and Hedley Knewjen Quintana. 2022. "Medication Adherence in Hypertensive Individuals in Panama 2019: A National Cross-Sectional Study" Healthcare 10, no. 11: 2244. https://doi.org/10.3390/healthcare10112244
APA StyleGuerra, C., Conte, E., Del Rio, A. I., Motta, J., Moreno Velásquez, I., & Quintana, H. K. (2022). Medication Adherence in Hypertensive Individuals in Panama 2019: A National Cross-Sectional Study. Healthcare, 10(11), 2244. https://doi.org/10.3390/healthcare10112244