Person-Centred Care Including Deprescribing for Older People

 ,
,
Abstract
1. Introduction
2. Person-Centred Care for Older People
2.1. How to Provide Person-Centred Care (PCC)
2.2. What Is the Role of the Clinician
2.3. How Can We Apply Person-Centred Care (PCC) to Deprescribing
3. Deprescribing Case Studies
3.1. Intermediate Care
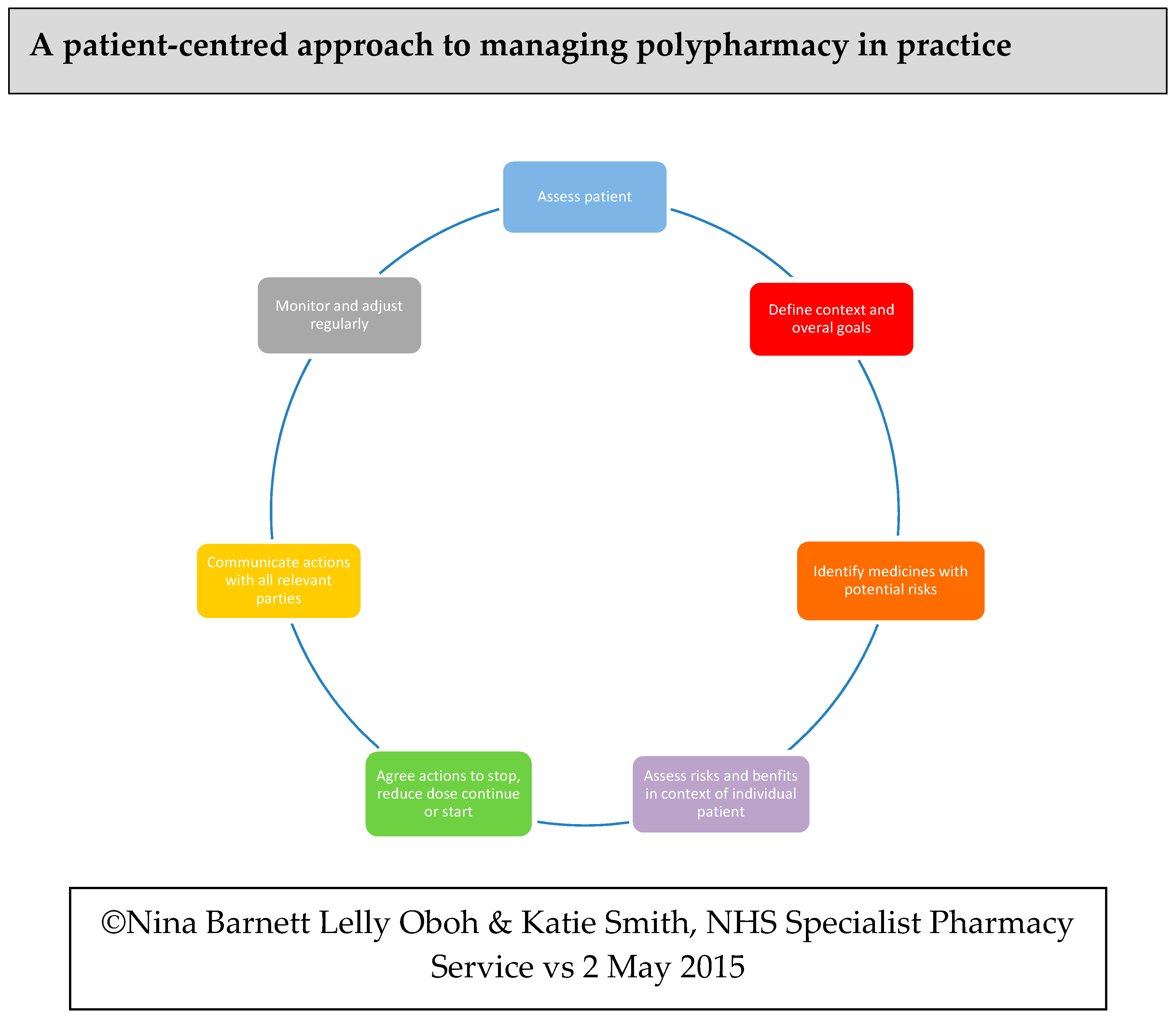
3.1.1. Steps 1 and 2: Assess Patient; Define Context and Overall Goals
- Nitrofurantoin 50 mg at night
- Lansoprazole 30 mg twice a day
- Perindopril 4 mg in the morning
- Furosemide 40 mg in the morning, 20 mg at lunchtime
- Pregabalin 25 mg at night
- Bisoprolol 2.5 mg in the morning
- Carbocisteine 750 mg twice a day
- Amitriptyline 10 mg at night
- Aspirin 75 mg in the morning
- Ropinirole 1 mg at night
- Montelukast 10 mg at night
- Clenil modulate 100 mcg 1 puff twice a day
- Salbutamol 100 mcg inhaler 1 to 2 puffs when required
- Paracetamol 1 g 4-6 hourly when required
- Forceval one in the morning
- Buprenorphine patch 10 mcg once a week on a Tuesday (this had been increased from 5 mcg during the hospital admission)
- Ispaghula husk one sachet twice a day
- Lidocaine 5% patch 1 once a day to both knees
3.1.2. Steps 3 and 4: Identify Medicines with Potential Risks; Assess Risks and Benefits in Context of Individual Patient
- Nitrofurantoin
- Lansoprazole
- Furosemide
- Pregabalin
- Amitriptyline
- Inhalers
- Montelukast
- Carbocisteine
- Forceval
- Lidocaine
3.1.3. Steps 5, 6, and 7: Agree Actions to Stop, Reduce Dose, Continue, or Start; Communicate Actions with All Relevant Parties; Monitor and Adjust Regularly
- Lansoprazole reduced from 30 mg twice a day to 15 mg twice a day
- Pregabalin stopped
- Montelukast stopped
- Carbocisteine stopped
- Forceval stopped
- Lidocaine patch stopped
- Alendronic acid 70 mg weekly restarted
- Colecalciferol 800 units daily restarted.
- Stopping nitrofurantoin
- Changing furosemide dose to once a day
- Stopping amitriptyline
- Discontinuing beclomethasone and salbutamol inhalers.
3.2. Care Home
3.2.1. Steps 1 and 2: Assess Patient; Define Context and Overall Goals
- Donepezil 10 mg once daily at night
- Oxycodone MR (Longtec®) 5 mg in the morning, 10 mg at night
- Paracetamol 1 g four times daily
- Pregabalin 75 mg in morning
- Furosemide 40 mg in the morning
- Clopidogrel 75 mg once daily
- Omeprazole 20 mg once daily
- Atorvastatin 10 mg at night
- Ferrous fumarate 305 mg once daily
- Diclofenac gel 1% apply three times daily when required for knee pain
- Macrogol sachet one sachet twice daily when required
3.2.2. Steps 3 and 4: Identify Medicines with Potential Risks; Assess Risks and Benefits in Context of Individual Patient
- Alzheimer’s treatment
- Pain management
- Diuretic treatment
- CVA prevention–medication interaction between clopidogrel and omeprazole
- Anticholinergic effect of cognition (AEC) scale and anticholinergic burden (ACB)
- Ferrous fumarate
- Use of statins
- Constipation
3.2.3. Steps 5, 6 and 7: Agree Actions to Stop, Reduce Dose, Continue or Start; Communicate Actions with all Relevant Parties; Monitor and Adjust Regularly
- Alzheimer’s management: donepezil continued
- Falls risk and anticholinergic burden reduced by discontinuation of furosemide
- Reduction in pregabalin dose from 75 mg to 50 mg once a day for one month, to be further tapered to 25 mg once a day, and then stopped after a further month if pain was controlled
- Longtec, paracetamol, and diclofenac gel continued with unchanged dose to manage pain
- Ferrous fumarate stopped
- Cardiovascular risk reduced by changing the choice of the proton pump inhibitor from omeprazole to lansoprazole
- Atorvastatin dose not increased
- Constipation managed with when required macrogol.
4. Summary
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Duerden, M.; Avery, T.; Payne, R. Polypharmacy and Medicines Optimization Making It Safe and Sound; The Kings Fund: London, UK, 2013. [Google Scholar]
- Reeve, E.; Thompson, W.; Farrell, B. Deprescribing: A narrative review of the evidence and practical recommendations for recognizing opportunities and taking action. Eur. J. Intern. Med. 2017, 38, 3–11. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Multimorbidity: Clinical Assessment and Management. NG56. September 2016. Available online: https://www.nice.org.uk/guidance/ng56 (accessed on 20 March 2019).
- Describing deprescribing. Drug Ther. Bull. 2014, 52, 25. [CrossRef] [PubMed]
- Wastesson, J.W.; Morin, L.; Tan, E.C.K.; Johnell, K. An update on the clinical consequences of polypharmacy in older adults: A narrative review. Expert Opin. Drug. Saf. 2018, 17, 1185–1196. [Google Scholar] [CrossRef] [PubMed]
- Hardy, J.; Hilmer, S. Deprescribing in the Last Year of Life. J. Pharm. Pract. Res. 2011, 41, 146–151. [Google Scholar] [CrossRef]
- Payne, R.; Duerden, M. Medicines optimisation in the care home setting. Prescriber 2015, 26, 20–24. [Google Scholar] [CrossRef][Green Version]
- McGrath, K.; Hajjar, E.R.; Kumar, C.; Hwang, C.; Salzman, B. Deprescribing: A simple method for reducing polypharmacy. J. Fam. Pract. 2017, 66, 436–445. [Google Scholar] [PubMed]
- Ziere, G.; Dieleman, J.; Hofman, A.; Pols, H.; van der Cammen, T.; Stricker, B. Polypharmacy and falls in the middle age and elderly population. Br. J. Clin. Pharmacol. 2006, 61, 218–223. [Google Scholar] [CrossRef]
- Marvin, V.; Ward, E.; Poots, A.; Heard, K.; Rajagopalan, A.; Jubraj, B. Deprescribing medicines in the acute setting to reduce the risk of falls. Eur. J. Hosp. Pharm. Sci. Pract. 2017, 24, 10–15. [Google Scholar] [CrossRef]
- Morandi, A.; Belelli, G.; Vasilevskis, E.; Turco, R.; Guerini, F.; Torpilliesi, T.; Speciale, S.; Emiliani, V.; Gentile, S.; Schnelle, J.; et al. Predictors of rehospitalization among elderly patients admitted to a rehabilitation hospital: The role of polypharmacy, functional status, and length of stay. J. Am. Med. Dir. Assoc. 2013, 14, 761–767. [Google Scholar] [CrossRef]
- Thompson, W.; Farrell, B. Deprescribing: What is it and what does the evidence tell us? Can. J. Hosp. Pharm. 2013, 66, 201–202. [Google Scholar] [CrossRef]
- Johansson, T.; Abuzahra, M.; Keller, S.; Mann, E.; Faller, B.; Sommerauer, C.; Höck, J.; Löffler, C.; Köchling, A.; Schuler, J.; et al. Impact of strategies to reduce polypharmacy on clinically relevant endpoints: A systematic review and meta-analysis. Br. J. Clin. Pharm. 2016, 82, 532–548. [Google Scholar] [CrossRef] [PubMed]
- Barnett, N.; Garfinkel, D. Deprescribing one year on: Challenging the first iatrogenic epidemic. Eur. J. Hosp. Pharm. 2018, 25, 63–64. [Google Scholar] [CrossRef] [PubMed]
- Frailty, polypharmacy and deprescribing. Drug Ther. Bull. 2016, 54, 69–72. [CrossRef] [PubMed]
- Reeve, E.; Shakib, S.; Hendrix, I.; Roberts, M.; Wiese, M. Review of deprescribing processes and development of an evidence-based, patient-centred deprescribing process. Br. J. Clin. Pharm. 2014, 78, 738–747. [Google Scholar] [CrossRef] [PubMed]
- Jansen, J.; Naganathan, V.; Carter, S.; McLachlan, A.; Nickel, B.; Irwig, L.; Bonner, C.; Doust, J.; Colvin, J.; Heaney, A.; et al. Too much medicine in older people? Deprescribing through shared decision making. BMJ 2016, 353. [Google Scholar] [CrossRef] [PubMed]
- Straand, J.; Sandvik, H. Stopping long-term drug therapy in general practice. How well do physicians and patients agree? Fam. Pract. 2001, 18, 597–601. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Linsky, A.; Simon, S.; Bokhour, B. Patient perceptions of proactive medication discontinuation. Patient Educ. Couns. 2015, 98, 220–225. [Google Scholar] [CrossRef]
- Turner, J.; Edwards, S.; Stanners, M.; Shakib, S.; Bell, J. What factors are important for deprescribing in Australian long-term care facilities? Perspectives of residents and health professionals. BMJ Open 2016, 6, e00978. [Google Scholar] [CrossRef]
- Royal Pharmaceutical Society. Medicines Optimisation: Helping Patients to Make the Most of Medicines; Royal Pharmaceutical Society: London, UK, 2013. [Google Scholar]
- Clyne, W.; Blenkinsopp, A.; Seal, R. A Guide to Medication Review; University National Prescribing Centre Plus & Medicines Partnership: Keele, UK, 2008. [Google Scholar]
- Santana, M.; Manalili, K.; Jolley, R.; Zelinsky, S.; Quan, H.; Lu, M. How to practice person-centred care: A conceptual framework. Health Expect. 2018, 21, 429–440. [Google Scholar] [CrossRef]
- Balint, E. The possibilities of patient-centered medicine. J. R. Coll. Gen. Pract. 1969, 17, 269–276. [Google Scholar]
- Gafni, A.; Charles, C.; Whelan, T. The physician–patient encounter: The physician as a perfect agent for the patient versus the informed treatment decision-making model. Soc. Sci. Med. 1998, 47, 347–354. [Google Scholar] [CrossRef]
- Farrell, C. Patient and Public Involvement in Health: The Evidence for Policy Implementation; Department of Health: London, UK, 2004.
- Barnett, N.; Oboh, L.; Smith, K. Patient-centred management of polypharmacy: A process for practice. Eur. J. Hosp. Pharm. 2016, 23, 113–117. [Google Scholar] [CrossRef] [PubMed]
- O’Mahony, D.; Sullivan, D.; Byrne, S.; O’Connor, M.; Ryan, C.; Gallagher, P. STOPP/START criteria for potentially inappropriate prescribing in older people: Version 2. Age Ageing 2015, 44, 489. [Google Scholar] [CrossRef] [PubMed]
- Beers, M.H.; Ouslander, J.G.; Rollingher, I.; Reuben, D.B.; Brooks, J.; Beck, J.C. Explicit criteria for determining inappropriate medication use in nursing home residents. UCLA division of geriatric medicine. Arch. Intern. Med. 1991, 151, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- By the 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults. J. Am. Geriatr. Soc. 2019, 67, 674–694. [Google Scholar] [CrossRef] [PubMed]
- Barnett, N. The new medicine service and beyond—Taking concordance to the next level. Pharm. J. 2011, 287, 653. [Google Scholar]
- Jackson, C.; Eliasson, L.; Barber, N.; Weinman, J. Applying COM-B to medication adherence. A suggested framework for research and interventions. Eur. Health Psych. 2014, 16, 7–17. [Google Scholar]
- Anderson, K.; Stowasser, D.; Freeman, C.; Scott, I. Prescriber barriers and enablers to minimising potentially inappropriate medications in adults: A systematic review and thematic synthesis. BMJ Open 2014, 4, e006544. [Google Scholar] [CrossRef]
- Anticholinergic Burden (ACB) scale. Available online: https://www.acbcalc.com (accessed on 24 April 2019).
- Anticholinergic Effect on Cognition (AEC) scale. Available online: https://medichec.com (accessed on 24 April 2019).
- Joint Formulary Committee. British National Formulary 76: September 2018; Pharmaceutical Press: London, UK, 2018. [Google Scholar]
- Cohen, N.; Dishi, V.V.; Zaidenstein, R.; Soback, S.; Weissgarten, J.; Averbukh, Z.; Gips, M.; Blatt, A.; Berman, S.; Modai, D.; et al. Effects of Various Modalities of Oral Furosemide Administration in Mild or Severe Congestive Heart Failure. J. Cardiovasc. Pharmacol. Ther. 1996, 1, 271–278. [Google Scholar] [CrossRef]
- Elliott, H.L.; Campbell, B.C.; Lawrence, J.R. Diuretic dose schedules: Is twice daily more effective? Br. J. Clin. Pharmacol. 1981, 12, 250–251. [Google Scholar] [CrossRef]
- Anisman, S.; Erickson, S.; Morden, N. How to prescribe loop diuretics in oedema. BMJ 2019, 364, l359. [Google Scholar] [CrossRef] [PubMed]
- Summary of Product Characteristics for Donepezil via Electronic Medicines Compendium. Available online: https://medicines.org.uk (accessed on 18 April 2019).
- National Institute for Health and Care Excellence. Dementia: Assessment, management and support for people living with dementia and their carers NG97. 2018. Available online: https://www.nice.org.uk/guidance/ng97 (accessed on 18 April 2019).
- European Society of Cardiology/European Society of Hypertension. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Clinical Knowledge Summaries Stroke and TIA. 2017. Available online: https://cks.nice.org.uk/stroke-and-tia (accessed on 18 April 2019).
- National Institute for Health and Care Excellence. Clinical Knowledge Summaries Constipation. 2017. Available online: https://cks.nice.org.uk/constipation (accessed on 24 April 2019).



{kind=link}
{kind=link}
| Medication Class | Questions to Consider | Comments |
|---|---|---|
| Symptom control |
|
|
| Risk reduction |
|
|
|
| For an Individual to Undertake a Behaviour They Must: | Problems May Include |
|---|---|
| 1. Be Capable of doing it |
|
| 2. Have Opportunity to do it |
|
| 3. Be Motivated to do it |
|
| Month (2018) | July | August | September |
|---|---|---|---|
| BP (mmHg) | 100/60 | 98/60 | 110/70 |
| Pulse (bpm) | 71 | 67 | 76 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smith, H.; Miller, K.; Barnett, N.; Oboh, L.; Jones, E.; Darcy, C.; McKee, H.; Agnew, J.; Crawford, P. Person-Centred Care Including Deprescribing for Older People. Pharmacy 2019, 7, 101. https://doi.org/10.3390/pharmacy7030101
Smith H, Miller K, Barnett N, Oboh L, Jones E, Darcy C, McKee H, Agnew J, Crawford P. Person-Centred Care Including Deprescribing for Older People. Pharmacy. 2019; 7(3):101. https://doi.org/10.3390/pharmacy7030101
Chicago/Turabian StyleSmith, Heather, Karen Miller, Nina Barnett, Lelly Oboh, Emyr Jones, Carmel Darcy, Hilary McKee, Jayne Agnew, and Paula Crawford. 2019. "Person-Centred Care Including Deprescribing for Older People" Pharmacy 7, no. 3: 101. https://doi.org/10.3390/pharmacy7030101
APA StyleSmith, H., Miller, K., Barnett, N., Oboh, L., Jones, E., Darcy, C., McKee, H., Agnew, J., & Crawford, P. (2019). Person-Centred Care Including Deprescribing for Older People. Pharmacy, 7(3), 101. https://doi.org/10.3390/pharmacy7030101