Communications Skills in the Pharmacy Profession: A Cross Sectional Survey of UK Registered Pharmacists and Pharmacy Educators


Abstract
:1. Introduction
1.1. Research Questions
- (1)
- What is the self-assessment of UK practicing pharmacists regarding their consultation skills and their views on behavioural change consultations?
- (2)
- What is the prevalence and nature of communication training and behavioural change consultation approaches in UK undergraduate pharmacy curricula?
1.2. Aims and Objectives
2. Materials and Methods
2.1. Survey to UK Pharmacists
2.2. Survey to Schools of Pharmacy
3. Results
3.1. Survey To Practicing Pharmacists
3.1.1. Pharmacists’ Consultation Skills Taught at Undergraduate Level
3.1.2. Pharmacists’ Consultation Skills Taught at Postgraduate Level/Continuous Professional Development
3.1.3. Training on Consultation and Communication Skills
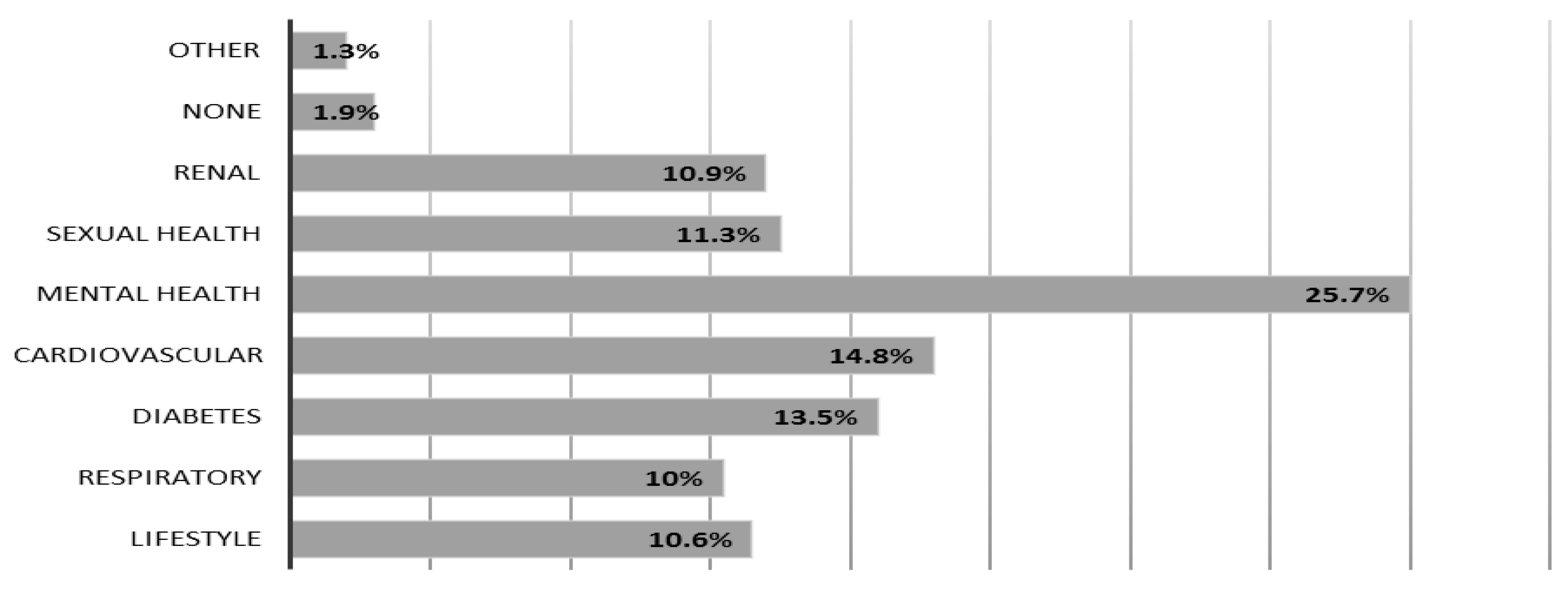
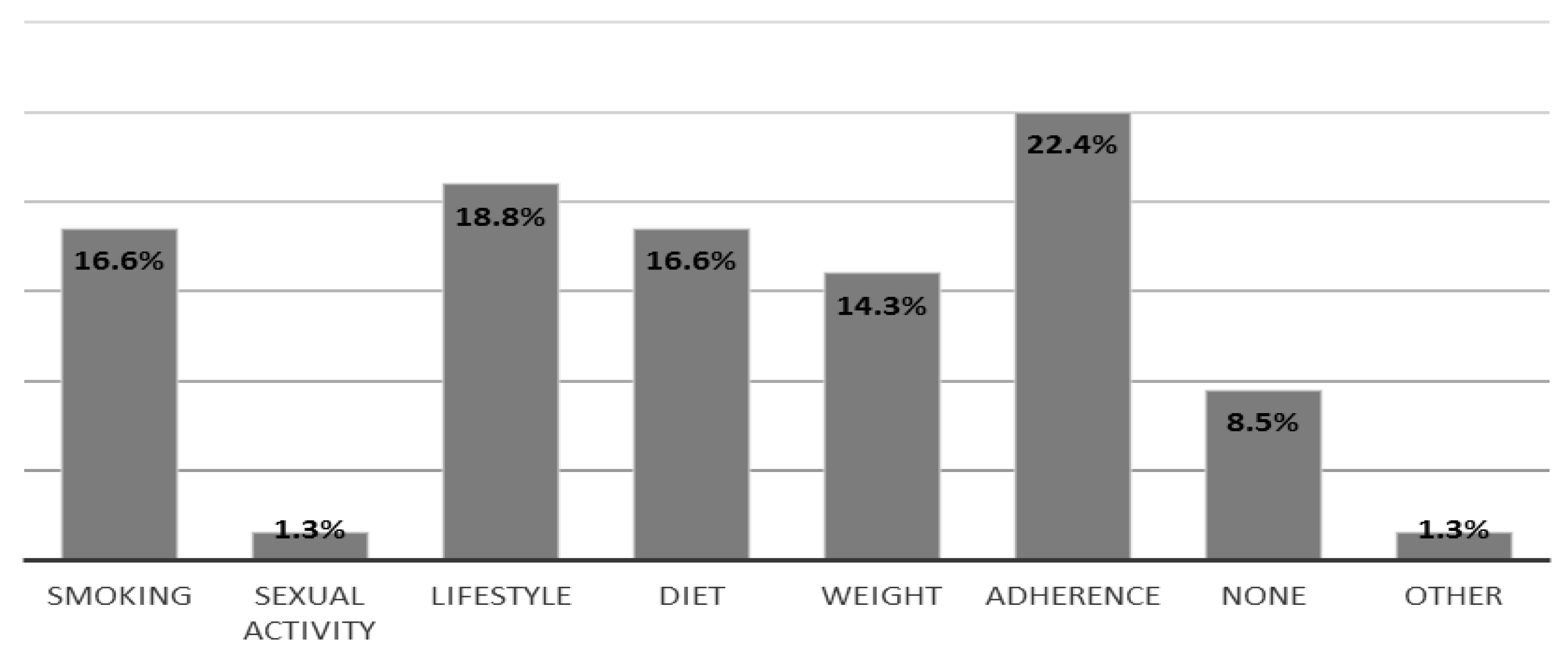
3.1.4. Pharmacists’ Knowledge and Application of Behavioural Interventions
3.2. Survey to Schools of Pharmacy
3.2.1. Methods of Teaching Communication and Consultation Skills
3.2.2. Health Behaviour Change Teaching
3.2.3. Teaching of Communication/Consultation Skills
3.2.4. MI in an MPharm Curriculum
3.2.5. Collaboration with Other Schools/Departments
3.2.6. Assessment of Motivational Interviewing
4. Discussion
Practice Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Patient Experience in Adult NHS Services: Improving the Experience of Care for People Using Adult NHS Services; Clinical Guideline [CG138]; National Institute for Clinical Excellence: London, UK, 2017.
- Bramhall, E. Effective communication skills in nursing practice. Nurs. Stand. 2014, 53. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.C.; Chutka, D.S. Assessing effective physician-patient communication skills: “Are you listening to me, doc?”. Korean J. Med. Educ. 2016, 28, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Initial Education and Training of Pharmacy Technicians: Draft Evidence Framework. Available online: https://www.pharmacyregulation.org/news/gphc-launches-new-education-and-training-standards-pharmacy-technicians (accessed on 11 December 2018).
- Consultation Skills for Pharmacy Practice: Taking a Patient Centred Approach; HSMO: St. Louis, MO, USA, 2014.
- Person-Centred Care Made Simple Quick Guide; The Health Foundation: London, UK, 2016; ISBN 978-1-906461-56-0.
- Consultation Skills for Pharmacy Practice. Available online: https://www.cppe.ac.uk/ (accessed on 11 December 2018).
- Counselling, Concordance and Communication–Innovative Education for Pharmacists, 2nd ed.; FIP: The Hague, The Netherlands, 2012; Available online: https://fip.org/files/fip/HaMIS/fip_ipsf_pce_2nd_2012.pdf (accessed on 11 December 2018).
- Simmons, L.A.; Wolever, R.Q. Integrative Health Coaching and Motivational Interviewing: Synergistic Approaches to Behavior Change in Healthcare. Glob. Adv. Health Med. 2013, 2, 28–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, W.R.; Rollnick, S. Ten things that Motivational Interviewing is not. Behav. Cognit. Psychother. 2009, 37, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Miller, W.R. Motivational interviewing in service to health promotion. The art of health promotion: Practical information to make programs more effective. Am. J. Heal Promot. 2004, 18, 1–10. [Google Scholar]
- Bisonó, A.M.; Manuel, J.K.; Forcehimes, A.A. Promoting Treatment Adherence through Motivational Interviewing; 05-O’Donohue-(V-5).qxd; SAGE Publications: Thousand Oaks, CA, USA, 2006; p. 71. [Google Scholar]
- Possidente, C.J.; Bucci, K.K.; Mcclain, W.J. Motivational interviewing: A tool to improve medication adherence? Am. J. Health-Syst. Pharm. 2005, 62, 1311–1314. [Google Scholar] [PubMed]
- Miller, W.R.; Rollnick, S. What’s New Since MIF-2; International Conference on Motivational! Interviewing (ICMI): Stockholm, Sweden, 2010; Available online: http://www.fhi.se/Documents/ICMI/Dokumentation/JuneF6/MillerFandFRollnickFjune6FpreF conferenceFworkshop.pdf (accessed on 11 December 2018).
- Smith, D.E.; Heckemeyer, C.M.; Kratt, P.P. Motivational interviewing to improve adherence to a behavioral weight-control program for older obese women with NIDDM: A pilot study. Diabetes Care 1997, 20, 52–54. [Google Scholar] [CrossRef]
- Kemp, R.; Kirov, G.; Everitt, B.; Hayward, P. Randomised controlled trial of compliance therapy. Br. J. Psychiatry 1998, 172, 413–419. [Google Scholar] [CrossRef]
- Daley, D.C.; Salloum, I.M.; Zuckoff, A. Increasing treatment adherence among outpatients with depression and cocaine dependence: Results of a pilot study. Br. J. Psychiatry 1998, 155, 1611–1613. [Google Scholar] [CrossRef]
- Dilorio, C.; Resnicow, K.; McDonnell, M. Using motivational interviewing to promote adherence to antiretroviral medications: A pilot study. J. Assoc. Nurs. AIDS Care 2003, 14, 52–62. [Google Scholar] [CrossRef]
- Schmaling, K.B.; Blume, A.W.; Afari, N. A randomized controlled pilot study of motivational interviewing to change attitudes about adherence to medications for asthma. J. Clin. Psychol. Med. Settings 2001, 8, 167–172. [Google Scholar] [CrossRef]
- Pringle, J.L.; Boyer, A.; Conklin, M.H.; McCullough, J.W.; Aldridge, A. The Pennsylvania Project: Pharmacist intervention improved medication adherence and reduced health care costs. Health Aff. 2014, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed]
- Future Pharmacists Standards for the Initial Education and Training of Pharmacists; General Pharmaceutical Council: London, UK, 2011.
- Miller, W.R.; Rollnick, S. Motivational Interviewing: Helping People Change, 3rd ed.; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Klonek, F.E.; Kauffeld, F. Providing engineers with OARS and EARS effects of a skills-based vocational training in motivational interviewing for engineers in higher education. High. Educ. Skills Work-Based Learn. 2015, 5, 117–134. [Google Scholar] [CrossRef]
- Motivational Interviewing: The Basics, OARS. (Adapted from Handouts by David Rosengren and from Miller & Rollnick, Motivational Interviewing, 2nd Edition, 2002). Available online: http://homelesshub.ca/resource/motivational-interviewing-open-questions-affirmation-reflective-listening-and-summary (accessed on 11 December 2018).
- Matulich, B. How to Do Motivational Interviewing 2013. Available online: https://www.youtube.com/watch?v=s3MCJZ7OGRk (accessed on 11 December 2018).
- Herie, M. CAMH Addiction Programs Clinical Day 2011: Five Essential Strategies in Motivating Clients to Change. 2011. Available online: https://www.youtube.com/watch?v=k4ZCfUTr4FM (accessed on 11 December 2018).
- Al Odhayani, A.; Ratnapalan, S. Teaching communication skills. Can. Fam. Phys. 2011, 57, 1216–1218. [Google Scholar]
- Oliver, D. Teaching medical learners to appreciate “difficult” patients. Can. Fam. Phys. 2011, 57, 506–508. [Google Scholar]
- Joyner, B.; Young, L. Teaching medical students using role play: Twelve tips for successful role plays. Med. Teach. 2006, 28, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Lavanya, S.H.; Kalpana, L.; Veena, R.M.; Bharath Kumar, V.D. Role-play as an educational tool in medication communication skills: Students’ perspectives. Ind. J. Pharm. 2016, 48 (Suppl. 1), S33–S36. [Google Scholar] [CrossRef]
- Nestel, D.; Tierney, T. Role-play for medical students learning about communication: Guidelines for maximising benefits. BMC Med. Educ. 2007, 7. [Google Scholar] [CrossRef]
- Bosse, H.M.; Nickel, M.; Huwendiek, S.; Jünger, J.; Schultz, J.H.; Nikendei, C. Peer role-play and standardised patients in communication training: A comparative study on the student perspective on acceptability, realism, and perceived effect. BMC Med. Educ. 2010, 10. [Google Scholar] [CrossRef]
- Schlegel, C.; Woermann, U.; Shaha, M.; Rethans, J.J.; van der Vleuten, C. Effects of communication training on real practice performance: A role-play module versus a standardized patient module. J. Nurs. Educ. 2016, 51, 16–22. [Google Scholar] [CrossRef]
- Buchel, T.L.; Edwards, F.D. Characteristics of effective clinical teachers. Fam. Med. 2005, 37, 30–35. [Google Scholar] [PubMed]
- What makes a good educational supervisor? Educ. Prim. Care 2010, 21, 230–235. [CrossRef]
- Training Professionals in Motivational Interviewing; The Health Foundation: London, UK, 2011.
- D’Antonio, N. Including Motivational Interviewing Skills in the PharmD Curriculum. Am. J. Pharm. Educ. 2010, 74, 152. [Google Scholar]
- Berger, B.A.; Bertram, C.T. Motivational Interviewing and Specialty Pharmacy. J. Manag. Care Spec. Pharm. 2015, 21, 13–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svensberg, K.; Björnsdottir, I.; Wallman, A.; Sporrong, S.K. Nordic Pharmacy Schools’ Experience in Communication Skills Training. Am. J. Pharm. Educ. 2017, 81, 6005. [Google Scholar] [CrossRef] [PubMed]
- Qidwai, W. Paternalistic model of medical practice. J. Coll. Phys. Surg. Pak. 2003, 13, 296. [Google Scholar]
- Papageorgiou, A. ‘Models of the doctor-patient consultation’. In Clinical Communication in Medicine, 1st ed.; Brown, J., Noble, L.M., Papageorgiou, A., Kidd, J., Eds.; Wiley Blackwell: Oxford, UK, 2016; pp. 21–29. [Google Scholar]
- Clinical Communication in Medicine. Available online: https://books.google.co.uk/books?isbn=1118728246 (accessed on 11 December 2018).
- TOMORROW’S DOCTORS 1993–General Medical Council. Tomorrow’s Doctors: Recommendations on Undergraduate Medical Education; Education Committee of the General Medical Council: London, UK, 1993. [Google Scholar]
- TOMORROW’S DOCTORS 2003–General Medical Council. Tomorrow’s Doctors; General Medical Council: London, UK, 2003. [Google Scholar]
- TOMORROW’S DOCTORS 2009–General Medical Council. Tomorrow’s Doctors: Outcomes and Standards for Undergraduate Medical Education; General Medical Council: London, UK, 2009. [Google Scholar]
- PROMOTING EXCELLENCE–General Medical Council. Promoting Excellence: Standards for Medical Education and Training; General Medical Council: London, UK, 2016. [Google Scholar]
- GOOD MEDICAL PRACTICE 2014–General Medical Council. Good Medical Practice. 2014. Available online: https://www.gmc-uk.org/ethical-guidance/ethical-guidance-for-doctors/good-medical-practice (accessed on 29 May 2018).
- Smith, J.; Picton, C.; Dayan, M. Now or Never: Shaping Pharmacy for the Future: The Report of the Commission on Future Models of Care Delivered through Pharmacy; Royal Pharmaceutical Society: London, UK, 2013. [Google Scholar]
- Picton, C.; Wright, H. Medicines Optimisation: Helping Patients to Make the Most of Medicines Good Practice Guidance for Healthcare Professionals in England; Royal Pharmaceutical Society: London, UK, 2013. [Google Scholar]
- Al-Nagar, A.; Constantine, D.; Thayaparan, J.; De-La-Mare, N.; Desborough, J. Views and experiences of community pharmacists about consultation skills training: A national survey. Intern. J. Pharm Pract. 2012, 20 (Suppl. 2), 3–30. [Google Scholar]
- Binaso, K.A. Medication Therapy Management Interventions in Outpatient Settings. J. Am. Pharm. Assoc. 2012, 52, 25–33. [Google Scholar]
- Hedegaard, U.; Kjeldsen, L.J.; Pottegård, A. Multifaceted intervention including motivational interviewing to support medication adherence after stroke/transient ischemic attack: A randomized trial. Cerebrovasc. Dis. Extra 2014, 4, 221–234. [Google Scholar] [CrossRef]
- Wallman, A.; Vaudan, C.; Sporrong, S.K. Communications Training in Pharmacy Education, 1995–2010. Am. J. Pharm. Educ. 2013, 77, 36. [Google Scholar] [CrossRef]
- Westra, H.A.; Aviram, A.; Doell, F.K. Extending Motivational Interviewing to the Treatment of Major Mental Health Problems: Current Directions and Evidence. Can. J. Psychiatry 2011, 56, 643–650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Report from the Independent Mental Health Taskforce to the NHS in England February 2016. Available online: https://www.england.nhs.uk/wp-content/uploads/2016/02/Mental-Health-Taskforce-FYFV-final.pdf (accessed on 11 December 2018).



{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Gender | |
| Male | 53 (50%) |
| Female | 52 (49.1%) |
| Prefer not to say | 1 (0.9%) |
| Qualified pharmacist (years) | |
| 0–5 | 34 (32.1%) |
| 6–10 | 27 (25.5%) |
| More than 10 | 45 (42.5%) |
| Type of community pharmacy | |
| Chain | 40 (39.6%) |
| Independent | 34 (33.75%) |
| Locum pharmacist | 13 (12.9%) |
| N/A | 14 (13.9%) |
| Years of pharmacy practice (years) | |
| 31+ | 5 (4.7%) |
| 25–30 | 11 (10.3%) |
| 20–24 | 14 (13.1%) |
| 15–19 | 8 (7.5%) |
| 10–14 | 14 (13.1%) |
| 5–9 | 21 (19.6%) |
| 0–4 | 34 (31.8%) |
| Branch of practice | |
| Hospital | 20 (18%) |
| GP surgery | 8 (7.2%) |
| Community Pharmacy | 67 (60.4%) |
| Other | 16 (14.4%) |
| Region of work | |
| East Midlands | 38 (35.5%) |
| West Midlands | 47 (43.9%) |
| London | 8 (7.5%) |
| Other | 14 (13.1%) |
| Qualification | |
| MPharm | 70 (57.9%) |
| BSc Pharm | 40 (33.1%) |
| Pharma D | 0 |
| Independent Prescriber | 11 (9.1%) |
| School of Pharmacy | MPharm Variations | Cohort Size (2016–2017) | In What Year Are Communication/Consultation Skills Included in Your Curriculum | Communication Course Includes Strategic Collaboration with Other Departments | Is Assessment for Behaviour Change Techniques (MI) Formative or Summative? |
|---|---|---|---|---|---|
| 1 | BOTH 4 Year and 5 Year MPharm | 76–100 | First Year, Second Year, Third Year, Fourth Year, Fifth Year | Medicine | Formative |
| 2 | 4 Year MPharm | 101–150 | First Year, Second Year, Third Year, Fourth Year | Medicine | Not applicable |
| 3 | 4 Year MPharm | 51–75 | First Year, Second Year, Third Year, Fourth Year | Medicine | Summative |
| 4 | 4 Year MPharm | 76–100 | First Year, Second Year, Third Year, Fourth Year | Not applicable | |
| 5 | 4 Year MPharm | 101–150 | First Year, Second Year, Third Year, Fourth Year | Medicine, Nursing, Social work/sociology | Summative |
| 6 | 4 Year MPharm | 101–150 | First Year, Second Year, Third Year, Fourth Year | None—no strategic collaborations | |
| 7 | BOTH 4 Year and 5 Year MPharm | 101–150 | First Year, Second Year, Third Year, Fourth Year, Fifth Year | Medicine, Nursing | Formative |
| 8 | 4 Year MPharm | 101–150 | First Year, Second Year, Third Year, Fourth Year | Psychology | Not applicable |
| 9 | BOTH 4 Year and 5 Year MPharm | 76–100 | First Year, Second Year, Third Year, Fourth Year | Psychology, Psychotherapy and counselling, Medicine, Nursing, Social work/sociology | Formative |
| 10 | 4 Year MPharm | 76–100 | First Year, Second Year, Third Year, Fourth Year | None—no strategic collaborations | Formative |
| 11 | 4 Year MPharm | 0–50 | First Year, Second Year, Third Year, Fourth Year | None—no strategic collaborations | Summative |
| 12 | 4 Year MPharm | 101–150 | First Year, Second Year, Third Year, Fourth Year | None—no strategic collaborations | Not applicable |
| 13 | BOTH 4 Year and 5 Year MPharm | 101–150 | First Year, Second Year, Third Year, Fourth Year, Fifth Year | None—no strategic collaborations | Summative |
| 14 | 4 Year MPharm | 76–100 | First Year | Formative | |
| 15 | 4 Year MPharm | 101–150 | Second Year, Third Year | Psychology | Not applicable |
| 16 | 4 year MPharm | 0–50 | First Year, Second Year, Third Year, Fourth Year | Medicine | Summative |
| 17 | 4 Year MPharm | 101–150 | First Year, Second Year, Third Year, Fourth Year | Nursing, Social work/sociology | Not applicable |
| 18 | BOTH 4 Year and 5 Year MPharm | 200+ | First Year, Second Year, Third Year, Fourth Year, Fifth Year | None—no strategic collaborations | Formative |
| ACRONYM | Elements of Behavioural Approaches |
|---|---|
| DARN-CAT [22] | Desire, Ability, Reason, Need—Commitment, Activation, Taking steps |
| EARS [23] | Elaborate, Affirm, Reflect, Summarise |
| OARS [24] | Open-ended questions, Affirmations, Reflections, Summaries |
| PACE [25] | Partnership, Autonomy/Acceptance, Compassion, Evocation |
| REACH [26] | Resist the ‘righting reflex’, Evoke, Affirm autonomy, Clarify goals, Highlight change talk |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jalal, Z.; Cox, A.; Goel, N.; Vaitha, N.; King, K.; Ward, J. Communications Skills in the Pharmacy Profession: A Cross Sectional Survey of UK Registered Pharmacists and Pharmacy Educators. Pharmacy 2018, 6, 132. https://doi.org/10.3390/pharmacy6040132
Jalal Z, Cox A, Goel N, Vaitha N, King K, Ward J. Communications Skills in the Pharmacy Profession: A Cross Sectional Survey of UK Registered Pharmacists and Pharmacy Educators. Pharmacy. 2018; 6(4):132. https://doi.org/10.3390/pharmacy6040132
Chicago/Turabian StyleJalal, Zahraa, Anthony Cox, Neera Goel, Nikita Vaitha, Kathryn King, and Jon Ward. 2018. "Communications Skills in the Pharmacy Profession: A Cross Sectional Survey of UK Registered Pharmacists and Pharmacy Educators" Pharmacy 6, no. 4: 132. https://doi.org/10.3390/pharmacy6040132