Training Needs of Manitoba Pharmacists to Increase Application of Assessment and Prescribing for Minor Ailments into Practice: A Qualitative and Quantitative Survey

Abstract
:1. Introduction
2. Methods
2.1. Survey Design
2.2. Recruitment and Data Collection
2.3. Statistical Analysis
3. Results
3.1. Demographics of Survey Respondents
3.2. Assessment and Prescribing Skills for Self-Limiting Conditions in the Practice Setting
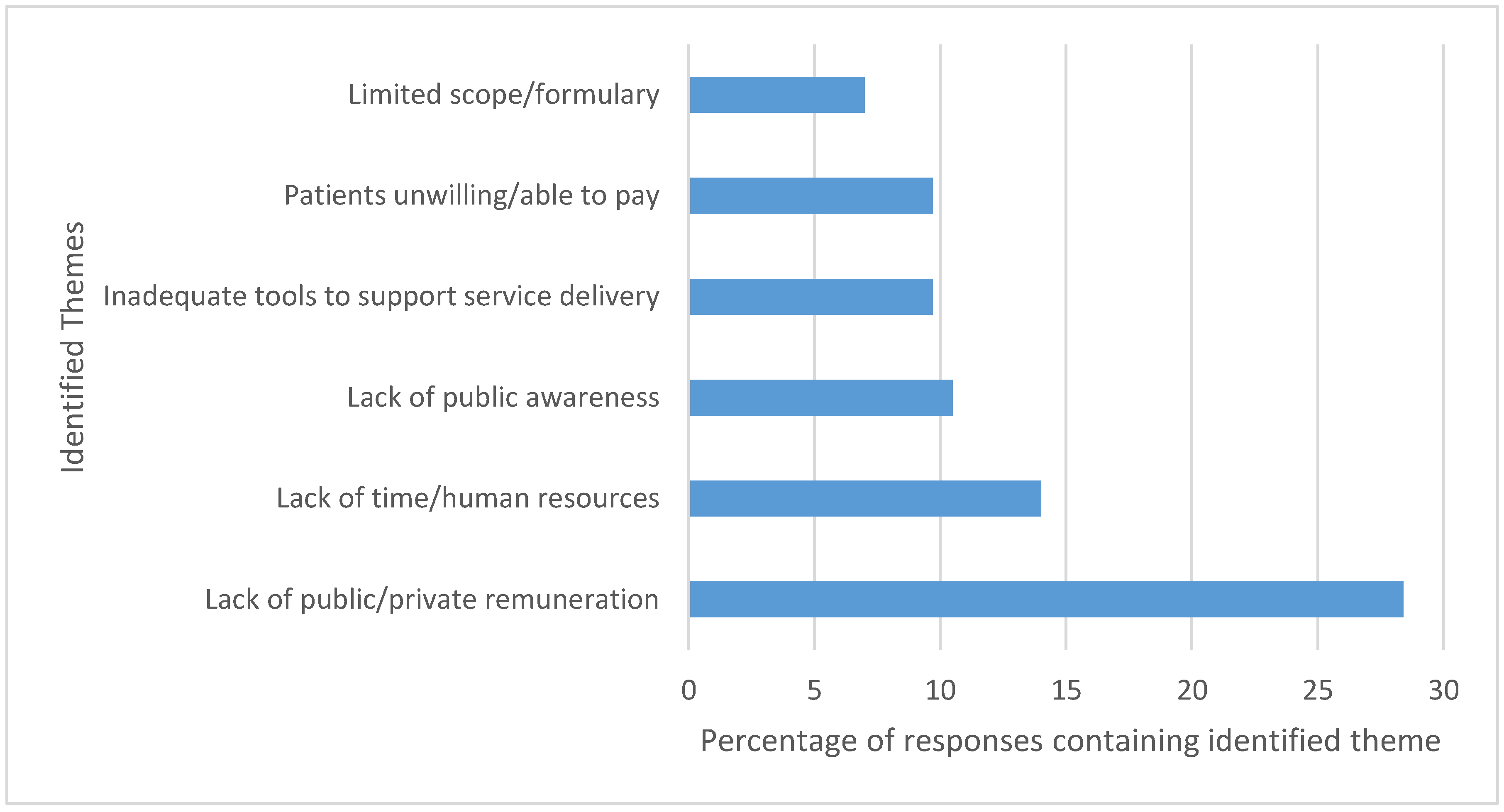
3.3. Perceived Barriers for Applying Assessment and Prescribing Skills
3.4. Preferences for Continuing Education
4. Discussion
Strengths & Limitation
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Habicht, D.; Ng, S.; Dunford, D.; Shearer, B.; Kuo, I.F. Incorporating assessment and prescribing for ambulatory ailments skills into practice: An environmental scan of continuing education for pharmacist prescribing in Canada. Can. Pharm. J. 2017, 150, 316–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- College of Pharmacists of Manitoba. A guide to pharmacy practice in Manitoba. 2018. Available online: http://www.cphm.ca/uploaded/web/Legislation/Pharmacy-Practice-Guide/Guide-to-Pharmacy-Practice-Final.pdf (accessed on 4 August 2018).
- Faruquee, C.F.; Guirguis, L.M. A scoping review of research on the prescribing practice of Canadian pharmacists. Can. Pharm. J. 2015, 148, 325–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canadian Pharmacists Association. A Review of Pharmacy Services in Canada and the Health Economic Evidence. 2016. Available online: https://www.pharmacists.ca/cpha-ca/assets/File/cpha-on-the-issues/Pharmacy%20Services%20Report%201.pdf (accessed on 4 August 2018).
- Grol, R.; Grimshaw, J. From best evidence to best practice: Effective implementation of change in patients’ care. Lancet 2003, 362, 1225–1230. [Google Scholar] [CrossRef]
- George, J.; Pfleger, D.; McCaig, D.; Bond, C.; Stewart, D. Independent prescribing by pharmacists: A study of the awareness, views and attitudes of Scottish community pharmacists. Pharm. World Sci. 2006, 28, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Pfleger, D.E.; McHattie, L.W.; Diack, H.L.; McCaig, D.J.; Stewart, D.C. Views, attitudes and self-assessed training needs of Scottish community pharmacists to public health practice and competence. Pharm. World Sci. 2008, 30, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Partin, M.R.; Powell, A.A.; Burgess, D.J.; Haggstrom, D.A.; Gravely, A.A.; Halek, K.; Bangerter, A.; Shaukat, A.; Nelson, D.B. Adding Postal Follow-Up to a Web-Based Survey of Primary Care and Gastroenterology Clinic Physician Chiefs Improved Response Rates but not Response Quality or Representativeness. Eval. Health Prof. 2015, 38, 382–403. [Google Scholar] [CrossRef] [PubMed]
- Gregory, P.A.M.; Teixeira, B.; Austin, Z. What does it take to change practice? Perspectives of pharmacists in Ontario. Can. Pharm. J. 2018, 151, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Houle, S.K.D.; Grindrod, K.A.; Chatterley, T.; Tsuyuki, R.T. Paying pharmacists for patient care: A systematic review of remunerated pharmacy clinical care services. Can. Pharm. J. 2014, 147, 209–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCullough, K.B.; Formea, C.M.; Berg, K.D.; Burzynski, J.A.; Cunningham, J.L.; Ou, N.N.; Rudis, M.I.; Stollings, J.L.; Nicholson, W.T. Assessment of the pharmacogenomics educational needs of pharmacists. Am. J. Pharm. Educ. 2011, 75, 51. [Google Scholar] [CrossRef] [PubMed]
- Kibicho, J.; Pinkerton, S.D.; Owczarzak, J. Community-Based Pharmacists’ Needs for HIV-Related Training and Experience. J. Pharm. Pract. 2014, 27, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Maio, V.; Belazi, D.; Goldfarb, N.I.; Phillips, A.L.; Crawford, A.G. Use and effectiveness of pharmacy continuing-education materials. Am. J. Health Syst. Pharm. 2003, 60, 1644–1649. [Google Scholar] [PubMed]
- Hasan, S. Continuing education needs assessment of pharmacists in the United Arab Emirates. Pharm. World Sci. 2009, 31, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Bascom, C.S.; Rosenthal, M.M.; Houle, S.K.D. Are pharmacists ready for a greater role in travel health? An evaluation of the knowledge and confidence in providing travel health advice of pharmacists practicing in a community pharmacy chain in Alberta, Canada. J. Travel Med. 2015, 22, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Amery, J.; Lapwood, S. A study into the educational needs of children’s hospice doctors: A descriptive quantitative and qualitative survey. Palliat. Med. 2004, 18, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Awad, N.I.; Bridgeman, M.B. Continuing-education program planning: Tips for assessing staff educational needs. Am. J. Health Syst. Pharm. 2014, 71, 1616–1619. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Johnson, T.P.; Wislar, J.S. Response rates and nonresponse errors in surveys. JAMA 2012, 307, 1805–1806. [Google Scholar] [CrossRef] [PubMed]
- Dillman, D. Mail and Internet Surverys: The Tailored Design Method, 2nd ed.; John Wiley & Sons: Hoboken, NJ, USA, 2007. [Google Scholar]
- Medway, R.L.; Fulton, J. When More Gets You Less: A Meta-Analysis of the Effect of Concurrent Web Options on Mail Survey Response Rates. Public Opin. Q. 2012, 76, 733–746. [Google Scholar] [CrossRef]
- Koo, M.; Skinner, H. Challenges of internet recruitment: A case study with disappointing results. J. Med. Int. Res. 2005, 7, e6. [Google Scholar] [CrossRef] [PubMed]
- Jain, C.L.; Wyatt, C.M.; Burke, R.; Sepkowitz, K.; Begier, E.M. Knowledge of the Centers for Disease Control and Prevention’s 2006 routine HIV testing recommendations among New York City internal medicine residents. AIDS Patient Care STDS 2009, 23, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.; Schmalenberg, C.; Brewer, B.B.; Verran, J.A.; Keller-Unger, J. Accurate assessment of clinical nurses’ work environments: Response rate needed. Res. Nurs. Health 2009, 32, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Torghele, K.; Buyum, A.; Dubruiel, N.; Augustine, J.; Houlihan, C.; Alperin, M.; Miner, K.R. Logic Model Use in Developing a Survey Instrument for Program Evaluation: Emergency Preparedness Summits for Schools of Nursing in Georgia. Public Health Nurs. 2007, 24, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Petrovčič, A.; Petrič, G.; Lozar Manfreda, K. The effect of email invitation elements on response rate in a web survey within an online community. Comput. Hum. Behav. 2016, 56, 320–329. [Google Scholar] [CrossRef]
- Zillmann, D.; Schmitz, A.; Skopek, J.; Blossfeld, H.-P. Survey topic and unit nonresponse. Qual. Quant. 2014, 48, 2069–2088. [Google Scholar] [CrossRef]
- De Valck, K.D.; Langerak, F.; Verhoef, P.C.; Verlegh, P.W.J. Satisfaction with Virtual Communities of Interest: Effect on Members’ Visit Frequency*. Br. J. Manag. 2007, 18, 241–256. [Google Scholar] [CrossRef]
- Isenor, J.E.; Minard, L.V.; Stewart, S.A.; Curran, J.A.; Deal, H.; Rodrigues, G.; Sketris, I.S. Identification of the relationship between barriers and facilitators of pharmacist prescribing and self-reported prescribing activity using the theoretical domains framework. Res. Soc. Adm. Pharm. 2017. [Google Scholar] [CrossRef] [PubMed]
- Guirguis, L.M.; Hughes, C.A.; Makowsky, M.J.; Sadowski, C.A.; Schindel, T.J.; Yuksel, N.; Faruquee, C.F. Development and validation of a survey instrument to measure factors that influence pharmacist adoption of prescribing in Alberta, Canada. Pharm. Pract. 2018, 16, 1068. [Google Scholar] [CrossRef] [PubMed]
- Tsuyuki, R.T.; Beahm, N.P.; Okada, H.; Al Hamarneh, Y.N. Pharmacists as accessible primary health care providers: Review of the evidence. Can. Pharm. J. 2018, 151, 4–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosar, L.; Hu, N.; Lix, L.M.; Shevchuk, Y.; Teare, G.F.; Champagne, A.; Blackburn, D.F. Uptake of the Medication Assessment Program in Saskatchewan: Tracking claims during the first year. Can. Pharm. J. 2018, 151, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Weglicki, R.S.; Reynolds, J.; Rivers, P.H. Continuing professional development needs of nursing and allied health professionals with responsibility for prescribing. Nurse Educ. Today 2015, 35, 227–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenthal, M.M.; Holmes, E.R. The Professional Culture of Community Pharmacy and the Provision of MTM Services. Pharmacy 2018, 6. [Google Scholar] [CrossRef] [PubMed]
- Henkel, P.J.; Marvanova, M. Maintaining Vitality: Pharmacists’ Continuing Professional Education Decision-Making in the Upper Midwest. Pharmacy 2018, 6. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Overall (n = 162) | Self-Study Completed (n = 115) | Self-Study in Progress (n = 9) | Self-study not Started but Plan to Initiate (n = 23) | No Plans to Start Self-Study (n = 15) | |
|---|---|---|---|---|---|
| Number of years practicing as pharmacist | |||||
| <6 years | 36 (22.2%) | 29 (25.2%) | 1 (11.1%) | 5 (21.7%) | 1 (6.7%) |
| 6–15 years | 52 (32.1%) | 33 (28.7%) | 2 (22.2%) | 7 (30.4%) | 10 (66.7%) |
| >15 years | 74 (45.7%) | 53 (46.1%) | 6 (66.7%) | 11 (47.8%) | 4 (26.7%) |
| Employment status | |||||
| Full time | 122 (75.3%) | 94 (81.7%) | 5 (55.6%) | 14 (60.9%) | 9 (60.0%) |
| Part time | 27 (16.7%) | 16 (13.9%) | 3 (33.3%) | 4 (17.4%) | 4 (26.7%) |
| Casual or on leave | 12 (7.4%) | 4 (3.4%) | 1 (11.1%) | 5 (21.7%) | 2 (13.3%) |
| Primary area of employment | |||||
| Retail/community | 147 (90.7%) | 111 (96.5%) | 6 (66.7%) | 20 (87.0%) | 10 (66.7%) |
| Hospital | 8 (4.9%) | 1 (0.9%) | 1 (11.1%) | 1 (4.3%) | 5 (33.3%) |
| Government or academia | 3 (1.9%) | 2 (1.8%) | 1 (11.1%) | 0 | 0 |
| Other | 3 (1.9%) | 1 (0.9%) | 1 (11.1%) | 1 (4.3%) | 0 |
| Location of employment by health region | |||||
| Winnipeg (Churchill) | 85 (52.5%) | 55 (47.8%) | 6 (66.7%) | 12 (52.2%) | 1 (6.7%) |
| Interlake Eastern | 16 (9.9%) | 12 (10.4%) | 1 (11.1%) | 3 (13.0%) | 0 |
| Northern | 5 (3.1%) | 3 (2.6%) | 0 | 1 (4.3%) | 1 (6.7%) |
| Prairie Mountain Health | 25 (15.4%) | 19 (16.5%) | 1 (11.1%) | 4 (17.4%) | 1 (6.7%) |
| Southern Health-Sante Sud | 22 (13.6%) | 20 (17.4%) | 0 | 2 (8.7%) | 12 (80.0%) |
| Self-Study Completed (n = 115) | Self-Study in Progress/Plan to Initiate (n = 32) | No Plans to Start Self-Study (n = 15) | |
|---|---|---|---|
| Encountered barriers in applying assessment and prescribing skills for minor ailments | |||
| Yes | 96 (83.5%) | -- | -- |
| No | 19 (16.5%) | -- | -- |
| Anticipated encountering barriers in applying assessment and prescribing skills for minor ailments | |||
| Yes | -- | 20 (62.5%) | -- |
| No | -- | 12 (37.5%) | -- |
| Identified barriers to taking on expanded role of applying assessment and prescribing skills for minor ailments | |||
| Yes | -- | -- | 14 (93.3%) |
| No | -- | -- | 1 (0.06%) |
| Specific barriers identified (n, %) | |||
| Lack of sufficient revenue attached to expanded role | 68 (26.2%) | 14 (29.8%) | 10 (66.7%) |
| Lack of training in expanded role | 11 (4.2%) | 1 (2.1%) | -- |
| Lack of confidence in skills | 25 (9.6%) | 4 (8.5%) | 0 |
| Clinical uncertainty | 12 (4.6%) | 0 | 1 (6.7%) |
| Lack of time at work | 61 (23.5%) | 15 (31.9%) | 8 (53.3%) |
| Lack of performance feedback | 2 (0.8%) | 2 (4.3%) | -- |
| Lack of motivation to take on new responsibilities | 10 (3.8%) | 3 (6.4%) | 7 (46.7%) |
| Lack of support from management | 14 (5.4%) | 4 (8.5%) | 4 (26.7%) |
| Lack of patients presenting with minor ailments | 31 (11.9%) | 2 (4.3%) | -- |
| Lack of satisfaction with current training and certification program | -- | -- | 2 (13.3%) |
| Irrelevant to practice | -- | -- | 4 (26.7%) |
| Other | 26 (10.0%) | 2 (4.3%) | 2 (13.3%) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shearer, B.; Ng, S.; Dunford, D.; Kuo, I.F. Training Needs of Manitoba Pharmacists to Increase Application of Assessment and Prescribing for Minor Ailments into Practice: A Qualitative and Quantitative Survey. Pharmacy 2018, 6, 82. https://doi.org/10.3390/pharmacy6030082
Shearer B, Ng S, Dunford D, Kuo IF. Training Needs of Manitoba Pharmacists to Increase Application of Assessment and Prescribing for Minor Ailments into Practice: A Qualitative and Quantitative Survey. Pharmacy. 2018; 6(3):82. https://doi.org/10.3390/pharmacy6030082
Chicago/Turabian StyleShearer, Brenna, Sheila Ng, Drena Dunford, and I Fan Kuo. 2018. "Training Needs of Manitoba Pharmacists to Increase Application of Assessment and Prescribing for Minor Ailments into Practice: A Qualitative and Quantitative Survey" Pharmacy 6, no. 3: 82. https://doi.org/10.3390/pharmacy6030082