
Comparative Study of Lesions Obtained through Radiofrequency between the Irrigated Ablation Catheter with a Flexible Tip and the Non-Irrigated Catheter in Ex Vivo Porcine Hearts
 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
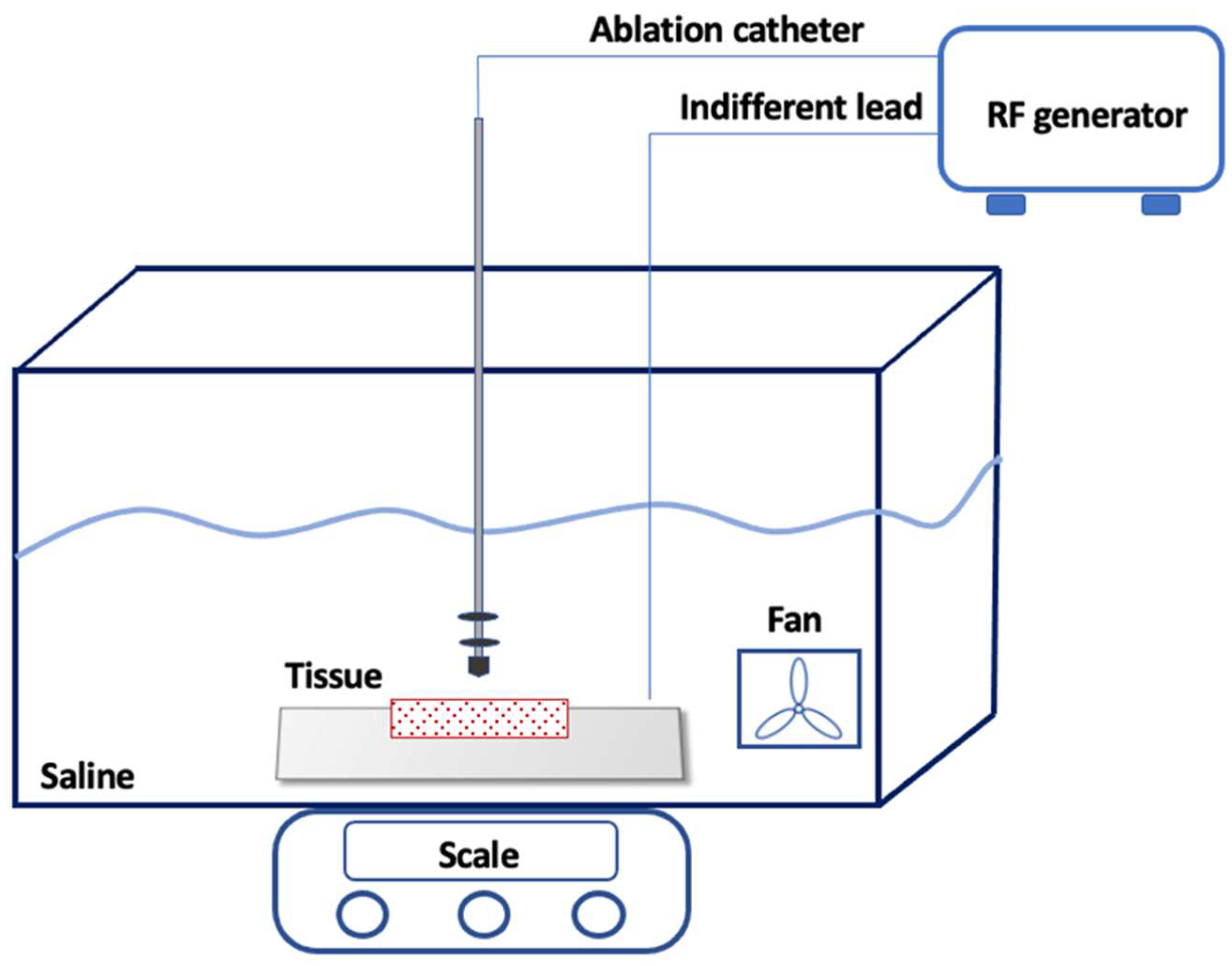
2.1. Experiment Setup
2.2. Ablation Catheters and the Radiofrequency Energy System
2.3. Ablation Protocol
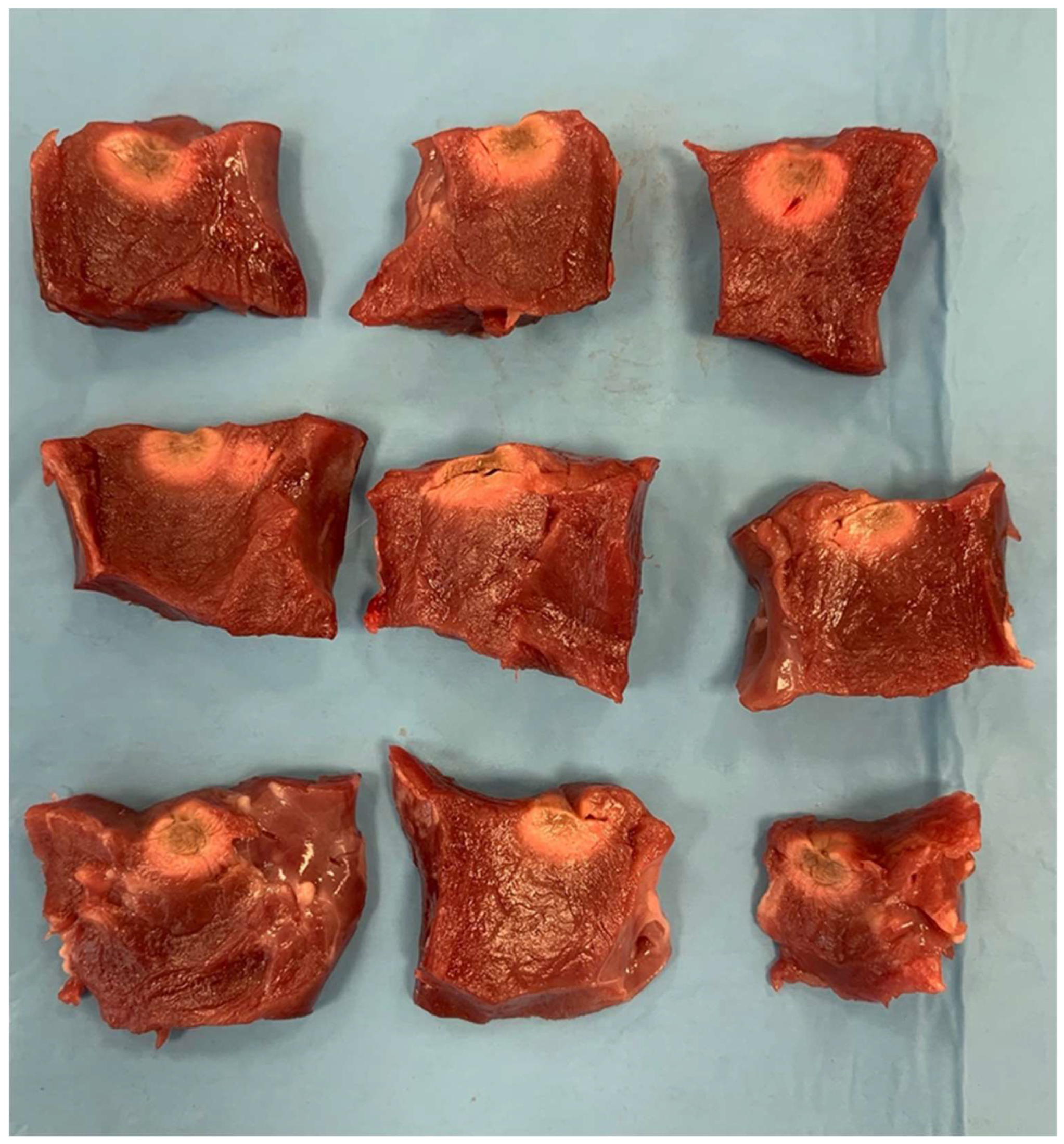
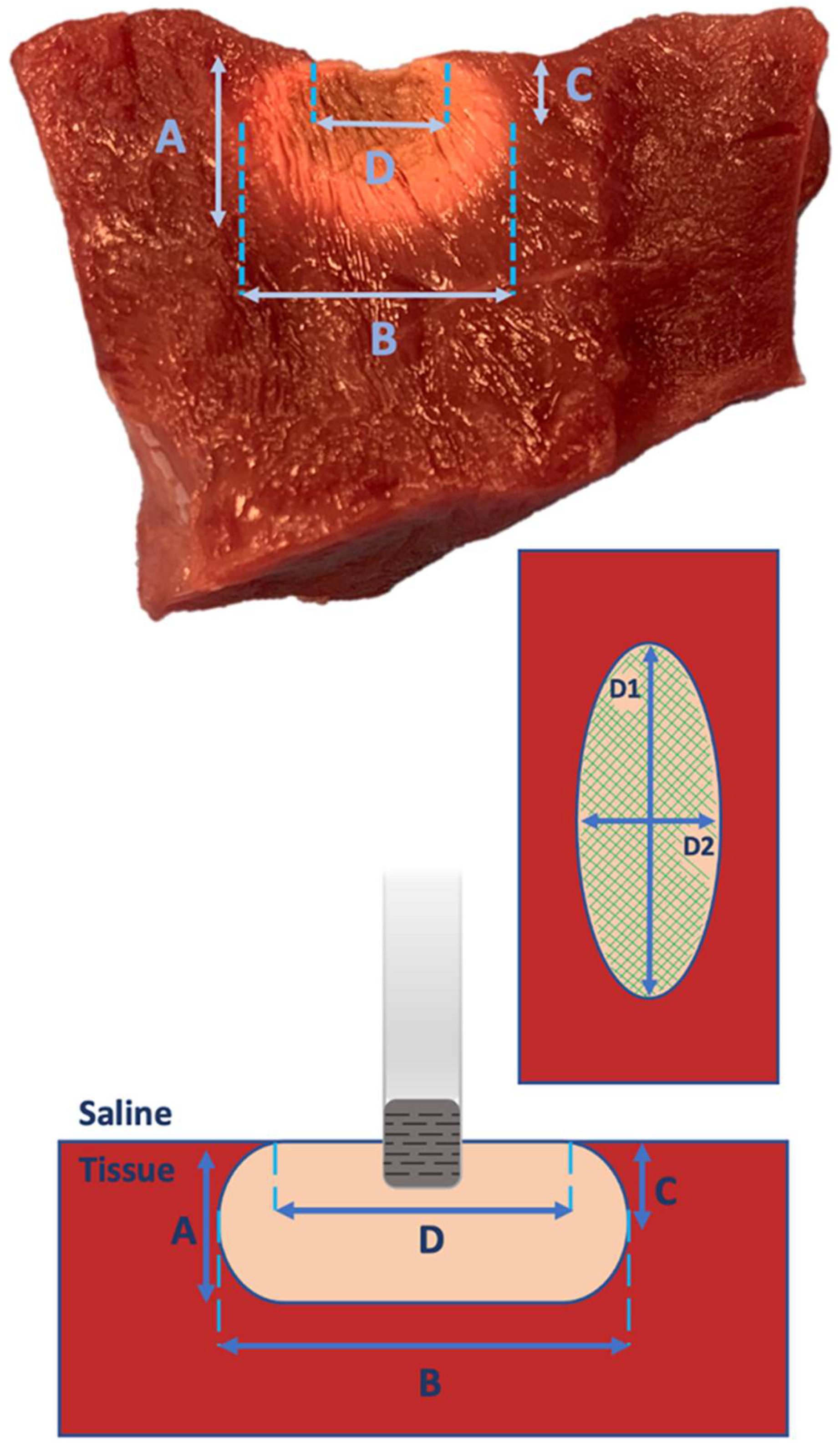
2.4. Lesion Measurements and Characterization
2.5. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A. Clinical Perspectives
Appendix A.1. Competency in Medical Knowledge
Appendix A.2. Translational Outlook
References
- Haines, D. Biophysics of ablation: Application to technology. J. Cardiovasc. Electrophysiol. 2004, 15 (Suppl. S10), S2–S11. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.T.; Olson, M.; Zheng, L.; Barham, W.; Moss, J.D.; Sauer, W.H. Effect of Irrigant Characteristics on Lesion Formation after Radiofrequency Energy Delivery Using Ablation Catheters with Actively Cooled Tips. J. Cardiovasc. Electrophysiol. 2015, 26, 792–798. [Google Scholar] [CrossRef] [PubMed]
- Leshem, E.; Zilberman, I.; Barkagan, M.; Shapira-Daniels, A.; Sroubek, J.; Govari, A.; Buxton, A.E.; Anter, E. Temperature-Controlled Radiofrequency Ablation Using Irrigated Catheters: Maximizing Ventricular Lesion Dimensions While Reducing Steam-Pop Formation. JACC Clin. Electrophysiol. 2020, 6, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Malagù, M.; Vitali, F.; Marchini, F.; Fiorio, A.; Sirugo, P.; Mele, D.; Brieda, A.; Balla, C.; Bertini, M. Ablation of Atrioventricular Nodal Re-Entrant Tachycardia Combining Irrigated Flexible-Tip Catheters and Three-Dimensional Electroanatomic Mapping: Long-Term Outcomes. J. Cardiovasc. Dev. Dis. 2021, 8, 61. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.T.; Gerstenfeld, E.P.; Tzou, W.S.; Jurgens, P.T.; Zheng, L.; Schuller, J.; Zipse, M.; Sauer, W.H. Radiofrequency Ablation Using an Open Irrigated Electrode Cooled with Half-Normal Saline. JACC Clin. Electrophysiol. 2017, 3, 1103–1110. [Google Scholar] [CrossRef] [PubMed]
- Calzolari, V.; De Mattia, L.; Basso, F.; Crosato, M.; Scalon, A.; Squasi, P.A.M.; Del Favero, S.; Cernetti, C. Ablation catheter orientation: In vitro effects on lesion size and in vivo analysis during PVI for atrial fibrillation. Pacing Clin. Electrophysiol. 2020, 43, 1554–1563. [Google Scholar] [CrossRef] [PubMed]
- Calzolari, V.; De Mattia, L.; Indiani, S.; Crosato, M.; Furlanetto, A.; Licciardello, C.; Squasi, P.A.M.; Olivari, Z. In Vitro Validation of the Lesion Size Index to Predict Lesion Width and Depth after Irrigated Radiofrequency Ablation in a Porcine Model. JACC Clin. Electrophysiol. 2017, 3, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Winterfield, J.R.; Jensen, J.; Gilbert, T.; Marchlinski, F.; Natale, A.; Packer, D.; Reddy, V.; Mahapatra, S.; Wilber, D.J. Lesion Size and Safety Comparison Between the Novel Flex Tip on the FlexAbility Ablation Catheter and the Solid Tips on the ThermoCool and ThermoCool SF Ablation Catheters. J. Cardiovasc. Electrophysiol. 2016, 27, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Dorwarth, U.; Fiek, M.; Remp, T.; Reithmann, C.; Dugas, M.; Steinbeck, G.; Hoffmann, E. Radiofrequency catheter ablation: Different cooled and noncooled electrode systems induce specific lesion geometries and adverse effects profiles. Pacing Clin. Electrophysiol. 2003, 26, 1438–1445. [Google Scholar] [CrossRef] [PubMed]
- Weiss, C.; Antz, M.; Eick, O.; Eshagzaiy, K.; Meinertz, T.; Willems, S. Radiofrequency catheter ablation using cooled electrodes: Impact of irrigation flow rate and catheter contact pressure on lesion dimensions. Pacing Clin. Electrophysiol. 2002, 25, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Houmsse, M.; Daoud, E.G. Biophysics and clinical utility of irrigated-tip radiofrequency catheter ablation. Expert. Rev. Med. Devices 2012, 9, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Field, M.E.; Wilber, D.J.; Mahapatra, S.; Byrd, I.; Kim, D.; Winterfield, J.R. Use and design of irrigated catheters for ablation including monitoring and active endpoints. In Ablation VT: A Practical Guide; Mahapatra, S., Marchlinski, F.E., Natale, A., Shivkumar, K., Eds.; Cardiotext Publishing: Hopkins, MN, USA, 2014; pp. 135–145. [Google Scholar]
- Hamaya, R.; Miyazaki, S.; Kajiyama, T.; Watanabe, T.; Kusa, S.; Nakamura, H.; Hachiya, H.; Iesaka, Y. Efficacy and safety comparison between different types of novel design enhanced open-irrigated ablation catheters in creating cavo-tricuspid isthmus block. J. Cardiol. 2018, 71, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Chrispin, J.; Misra, S.; Marine, J.E.; Rickard, J.; Barth, A.; Kolandaivelu, A.; Ashikaga, H.; Tandri, H.; Spragg, D.D.; Crosson, J.; et al. Current management and clinical outcomes for catheter ablation of atrioventricular nodal re-entrant tachycardia. Europace 2018, 20, e51–e59. [Google Scholar] [CrossRef] [PubMed]
- Bertini, M.; Brieda, A.; Balla, C.; Pollastrelli, A.; Smarrazzo, V.; Vitali, F.; Malagù, M.; Ferrari, R. Efficacy and safety of catheter ablation of atrioventricular nodal re-entrant tachycardia by means of flexible-tip irrigated catheters. J. Interv. Card. Electrophysiol. 2020, 58, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, J.Á.; Anderson, R.H.; Macías, Y.; Nevado-Medina, J.; Porta-Sánchez, A.; Rubio, J.M.; Sánchez-Quintana, D. Variable Arrangement of the Atrioventricular Conduction Axis within the Triangle of Koch: Implications for Permanent His Bundle Pacing. Clin. Electrophysiol. 2020, 6, 362–377. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 20 W | Irrigated Catheter | Non-Irrigated Catheter | p |
|---|---|---|---|
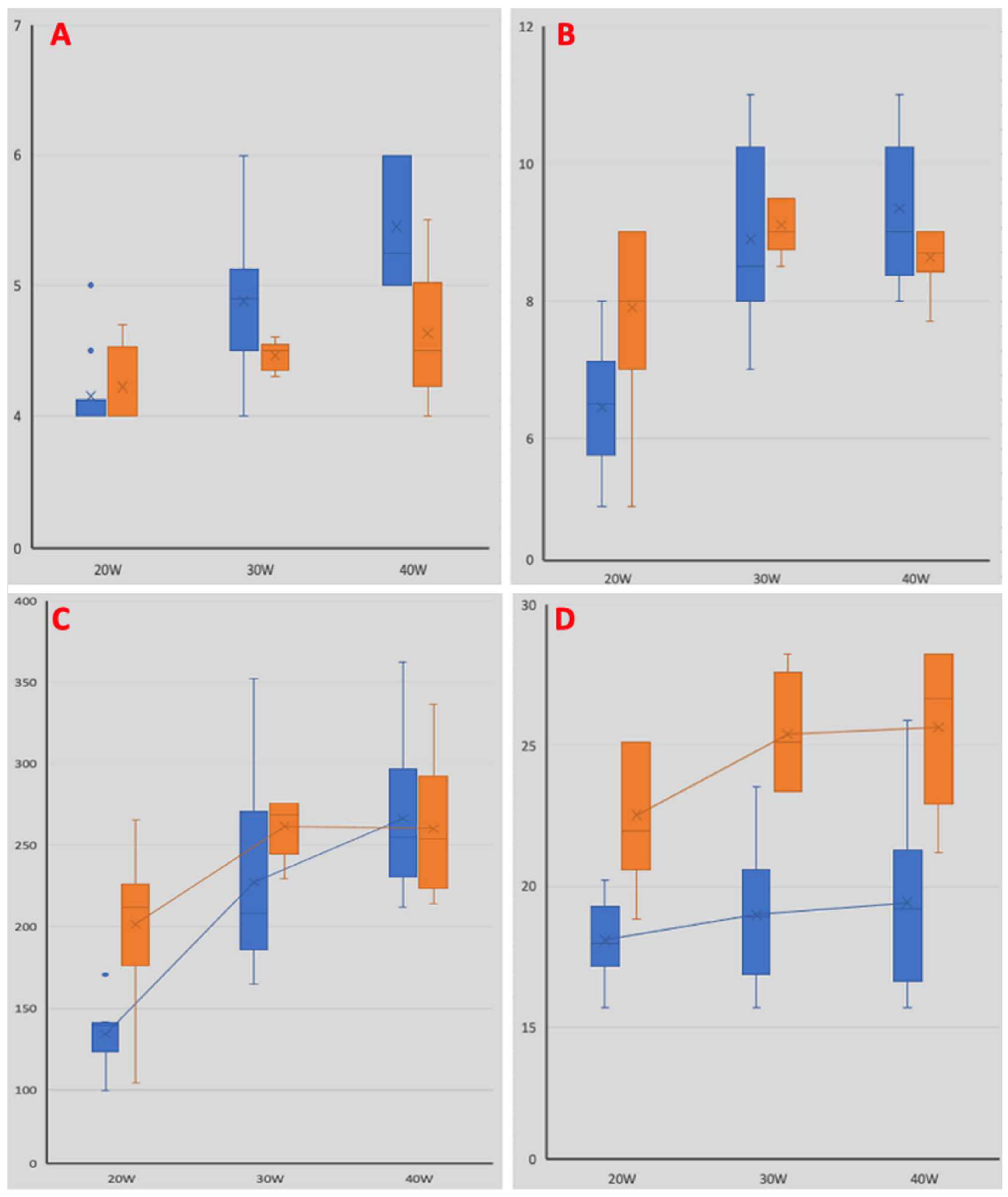
| Superficial length [mm] | 5.3 ± 0.3 | 7.7 ± 0.8 | 0.02 |
| Superficial width [mm] | 4.4 ± 0.3 | 3.8 ± 0.4 | 0.001 |
| Maximum depth [mm] | 4.2 ± 0.3 | 4.2 ± 0.3 | 0.43 |
| Maximum length at any depth [mm] | 6.5 ± 1 | 7.9 ± 1.2 | 0.012 |
| Depth at max length [mm] | 2.1 ± 0.4 | 2.3 ± 0.4 | 0.72 |
| Superficial area [mm2] | 18 ± 1.5 | 23 ± 2.5 | 0.001 |
| Lesion volume [µL] | 134 ± 18 | 201 ± 42 | 0.002 |
| 30 W | Irrigated Catheter | Non-Irrigated Catheter | p |
|---|---|---|---|
| Superficial length [mm] | 5.5 ± 0.4 | 8.5 ± 0.3 | 0.03 |
| Superficial width [mm] | 4.4 ± 0.5 | 3.9 ± 0.2 | 0.019 |
| Maximum depth [mm] | 4.9 ± 0.5 | 4.5 ± 0.1 | 0.08 |
| Maximum length at any depth [mm] | 8.9 ± 1.3 | 9.1 ± 0.4 | 0.45 |
| Depth at max length [mm] | 2.1 ± 0.5 | 2.2 ± 0.4 | 0.98 |
| Superficial area [mm2] | 19 ± 2.4 | 25 ± 4.6 | 0.005 |
| Lesion volume [µL] | 227 ± 58 | 131 ± 32 | 0.86 |
| 40 W | Irrigated Catheter | Non-Irrigated Catheter | p |
|---|---|---|---|
| Superficial length [mm] | 5.5 ± 0.4 | 8.6 ± 0.4 | 0.02 |
| Superficial width [mm] | 4.5 ± 0.5 | 3.8 ± 0.3 | 0.003 |
| Maximum depth [mm] | 5.5 ± 0.5 | 4.6 ± 0.5 | 0.007 |
| Maximum length at any depth [mm] | 9.4 ± 1.1 | 8.6 ± 0.4 | 0.14 |
| Depth at max length [mm] | 2.5 ± 0.4 | 2.4 ± 0.4 | 1 |
| Superficial area [mm2] | 19 ± 3.2 | 26 ± 2.6 | 0.001 |
| Lesion volume [µL] | 266 ± 43 | 260 ± 39 | 0.73 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vitali, F.; De Raffele, M.; Malagù, M.; Balla, C.; Azzolini, G.; Gibiino, F.; Boccadoro, A.; Micillo, M.; Bertini, M. Comparative Study of Lesions Obtained through Radiofrequency between the Irrigated Ablation Catheter with a Flexible Tip and the Non-Irrigated Catheter in Ex Vivo Porcine Hearts. Biology 2024, 13, 132. https://doi.org/10.3390/biology13020132
Vitali F, De Raffele M, Malagù M, Balla C, Azzolini G, Gibiino F, Boccadoro A, Micillo M, Bertini M. Comparative Study of Lesions Obtained through Radiofrequency between the Irrigated Ablation Catheter with a Flexible Tip and the Non-Irrigated Catheter in Ex Vivo Porcine Hearts. Biology. 2024; 13(2):132. https://doi.org/10.3390/biology13020132
Chicago/Turabian StyleVitali, Francesco, Martina De Raffele, Michele Malagù, Cristina Balla, Giorgia Azzolini, Federico Gibiino, Alberto Boccadoro, Marco Micillo, and Matteo Bertini. 2024. "Comparative Study of Lesions Obtained through Radiofrequency between the Irrigated Ablation Catheter with a Flexible Tip and the Non-Irrigated Catheter in Ex Vivo Porcine Hearts" Biology 13, no. 2: 132. https://doi.org/10.3390/biology13020132