1. Introduction
Targeted therapies are amongst the major treatment options for cancer today. Immune checkpoint inhibitors (ICI) targeting programmed death-1/ligand-1 (PD-1/PD-L1) have transformed the management of different prognostically poor cancers [
1,
2,
3]. Interferences with the PD-1 axes can cause an activation of autoreactive T-cells, damaging host tissues, and different immune-related adverse events (irAEs) have previously been reported. The known irAEs may affect a variety of organs such as the bowel, thyroid, liver, pituitary gland, and musculoskeletal system. Potential cardiovascular and cardiotoxicity have also been described [
1,
4,
5]. PD-1/PD-L1 chemokine axes could play important roles in limiting T-cell-mediated autoimmune inflammation. Previous preclinical studies have suggested that activated T-cells produce large amounts of pro-atherogenic cytokines, potentially contributing to both the growth and destabilization of atherosclerotic plaques [
6]. Positron emission tomography (PET) with 2-[18F]fluorodeoxyglucose (FDG) is a validated tool to assess atherosclerotic inflammatory activity, including in cancer patients [
7,
8]. Recently, we described an elevated inflammation determined by increased FDG-uptake in the large arteries after immunotherapy in older patients (mean age: 71 ± 14 years) suffering from melanoma and treated with ICI, suggesting increased atherosclerotic inflammation [
9]. There is less published knowledge regarding how ICI affects arterial inflammation in younger patients; therefore, in this present study, we aimed to analyze the cardiovascular toxicity induced by ICI treatment in patients with lymphoma under 50 years of age with low cardiovascular risk.
2. Materials and Methods
Twelve lymphoma patients (seven females, five males, mean age: 35 ± 9 years) treated with PD-1 inhibitors who underwent FDG positron emission tomography–computer tomography (PET/CT) or positron emission tomography–magnetic resonance imaging (PET/MRI) scans performed for diagnostic purposes before and after treatment (time interval between pre- and post-scans: 9.6 ± 3.9 months) were retrospectively analyzed. The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the University of Vienna (approval no. 1367/2020). Baseline patient characteristics, as well their cardiovascular risk factors and previous cancer treatments, were recorded (
Table 1). Maximum FDG standardized uptake values (SUV
max) were corrected for FDG blood-pool activity (SUV
bloodpool) to calculate target-to-background ratios (TBRs), as previously described [
10].
We analyzed 117 arterial lesions of 6 arterial segments (ascending and descending aorta, aortic arch, abdominal aorta, and iliac arteries) in PET scans pre- and post-ICI treatment, and quantified segmental FDG accumulation according to the current guidelines [
10]. We classified arterial lesions by pre-existing active inflammation (cut-off: TBRpre ≥ 1.48). Segmental calcium density categorization as non-calcified (<130 Hounsfield Units-HU) or calcified (≥130 HU) was only possible in eight patients who received PET/CT before and after ICI treatment. Continuous variables were recorded as the mean ± standard deviation. The mean FDG uptake values (SUV
max and TBR
max) pre- and post-therapy were retrospectively assessed using the paired Student’s t-test. The change in TBR values (ΔTBR = TBR
post − TBR
pre) was subsequently calculated and compared using the ANOVA test. Two-sided
p-values of <0.05 were considered significant.
As surrogate markers for systemic immune activation, FDG uptake as SUV
max was measured in bone marrow and spleen before and after ICI therapy, as previous described [
9]. The hepatic activity also as SUV
max was additionally measured by manually placing three regions of interest (ROIs) in coronal, axial, and longitudinal projections of the organ parenchyma, and liver-to-spleen ratios (normally >1) were subsequently calculated [
11]. Patients with splenic and/or hepatic metastases were excluded from this analysis.
As an additional systemic inflammation marker, high-sensitivity C-reactive protein (hsCRP) levels before and after ICI therapy were also collected.
3. Results
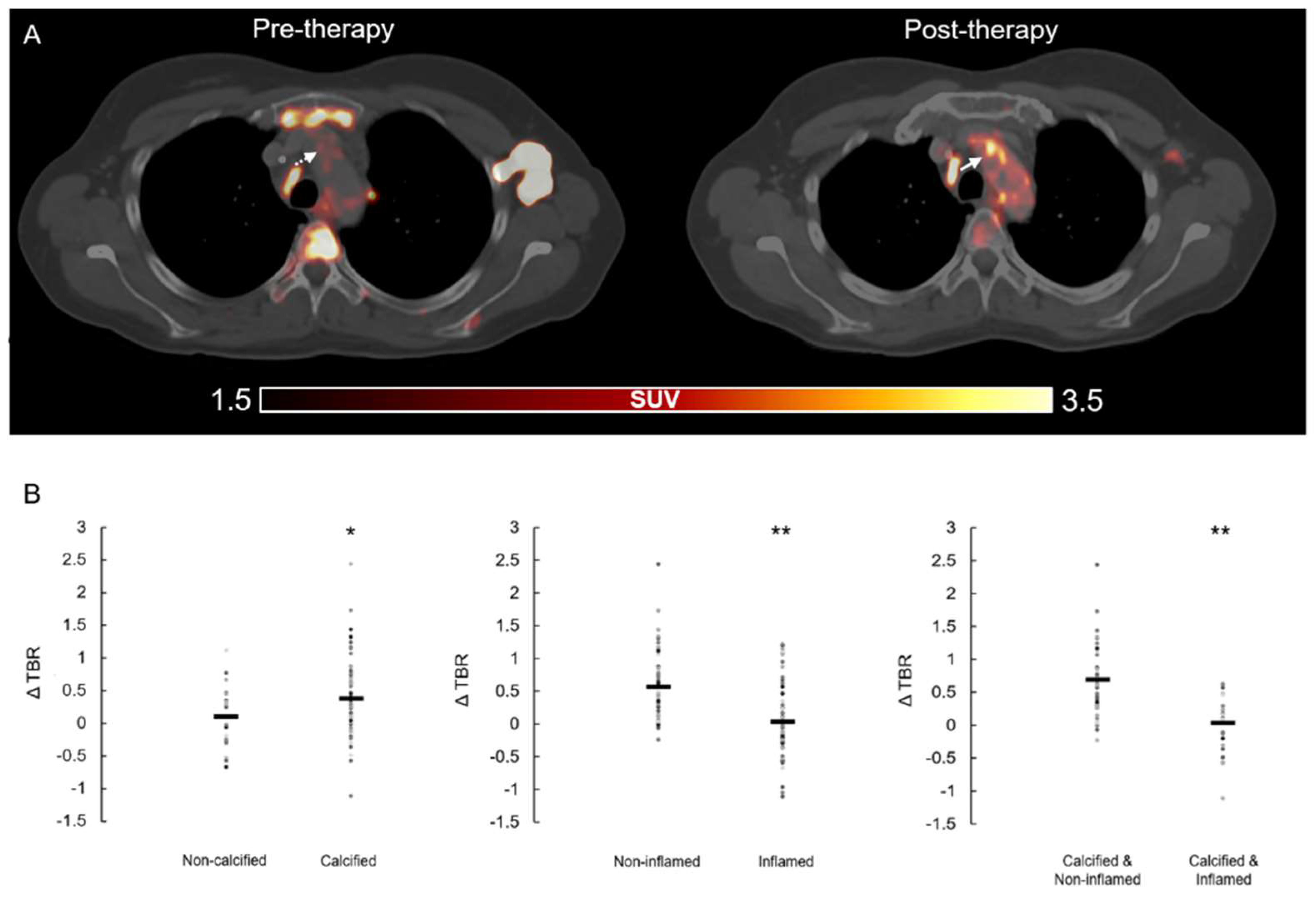
ICI immunotherapy resulted in significant increases in the inflammatory activity in all assessed arterial PET lesions (
n = 117, lesional TBR
pre = 1.50 ± 0.42 vs. lesional TBR
post = 1.79 ± 0.46,
p < 0.001) (
Figure 1A). A significant increase in lesional calcification after therapy was also found (HU
pre = 147 ± 59 vs. HU
post = 177 ± 65,
p < 0.001). Significant increases in TBR were found in lesions without pre-existing arterial inflammation (
n = 65, TBR
neg_pre = 1.20 ± 0.22 vs. TBR
neg_post = 1.71 ± 0.45,
p < 0.001), whereas lesions with pre-existing active inflammation remained largely unchanged (
n = 52, TBR
pos_pre = 1.85 ± 0.36 vs. TBR
pos_post = 1.87 ± 0.51,
p = 0.834). In contrast, in calcified lesions, TBR values were significantly elevated after therapy (
n = 73, TBR
calc_pre = 1.36 ± 0.38 vs. TBR
calc_post = 1.76 ± 0.42,
p < 0.001), whereas no significant change was observed in non-calcified PET lesions (
n = 14, TBR
non_calc_pre = 1.97 ± 0.35 vs. TBR
non_calc_post = 1.92 ± 0.25,
p= 0.683).
To derive a deeper insight into the relationship between pre-existing inflammation, calcification and increased inflammation after treatment, we generated four subgroups of arterial segments by calcification (yes/no) and pre-existing inflammation (yes/no). Calcified lesions without active inflammation showed a significant increase in inflammation after ICI, regardless of the severity of calcification (
n = 47, TBR
calc_neg_pre = 1.16 ± 0.18 vs. TBR
calc_neg_post = 1.74 ± 0.46,
p < 0.001). In contrast, no significant changes in inflammation were found in initially inflamed lesions, independent of pre-existing calcification (
Figure 1B).
FDG uptake measured in bone marrow, spleen, and liver did not show statistical differences before and after ICI (SUVmax_bonemarrow_pre = 1.97 ± 0.85 vs. SUVmax_bonemarrow_post = 1.86 ± 0.84, p = 0.075; SUVmax_spleen_pre = 3.77 ± 2.17 vs. SUVmax_spleen_post = 3.05 ± 1.02, p = 0.343; SUVmax_liver_pre = 3.49 ± 0.94 vs. SUVmax_liver_post = 3.18 ± 0.61, p = 0.197).
There were also no significant differences in the spleen-to-liver ratios measured in pre- and post-FDG PET scans (S/Lpre = 2.11 ± 0.44 vs. S/Lpost = 2.13 ± 0.50, p = 0.889). The inflammatory blood biomarker hsCRP markedly increased after therapy, but without statistical significance (hsCRPpre = 2.66 ± 4.61 vs. hsCRPpost = 6.96 ± 15.77; p = 0.393).
4. Discussion
The present study demonstrates a significant effect of ICI treatment on arterial inflammation in lymphoma patients under 50 years of age, without high cardiovascular risk. The underlying mechanism of inflammatory activation by ICI treatment, however, remains unclear. Pioneering studies have demonstrated that PD-L1 is expressed on endothelial cells and antigen-presenting cells (such as dendritic cells or macrophages) in the vasculature, whereas PD-1 is expressed on activated T-cells [
12,
13]. The protective immunity of vascular PD-L1 and T-cell PD-1 interaction downregulates the T-cell activation coupled with subsequent apoptosis or the suppression of cluster of differentiation 4 (CD4+) and CD8+ T-cell proliferation [
13]. Hence, inhibiting the PD-1 pathway could induce vascular inflammation by ICI treatment, which was observed in our findings. Nonetheless, we found that ICI therapy selectively activates low-active lesions, but not pre-active lesions. It could be speculated that PD-L1 blockade could compromise vascular integrity in early atherosclerosis by allowing activated PD-1
high T-cells to interact with the PD-L1
high endothelium/macrophages. Furthermore, the upregulation of vascular inflammation/metabolism was observed in arterial segments without present inflammation. Negligible activation in pre-activated segments by immunotherapy with ICI, probably because the deficient infiltration PD-1
high T-cells, induces pre-vascular inflammation, which disrupts the protective effect of the PD-L1 and PD-1 axes. We also hypothesize that previous anti-cancer therapies might induce the pre-vascular inflammation in respect to endothelial/macrophages activation, which hampers the pro-inflammation modulation of subsequent ICI treatment.
Taken together, this pre-existing unbalanced axis between PD-L1
high macrophages/endothelial cells and PD-1
high T-cells in inflamed arterial segments delivers a lower sensitivity to ICI therapy. In line with our hypothesis, this could be related to previous increases in effector-memory CD4+ T-cells in these inflamed arterial segments [
14]. In summary, the vascular PD-L1 and PD-1 axes could exert an atheroprotective mechanism to maintain peripheral immune tolerance, and an intercepted PD-1/PD-L1 axis between PD-1
high T-cells and PD-L1
high endothelium/macrophages could destruct vascular integrity [
12,
15]. PD-1 deficiency or inhibition of the T-cells could accelerate intimal infiltration of CD8+ T-cells without directly affecting the myeloid system, according with our findings regarding non-statistical significance changes in the uptake of spleen and bone marrow [
14].
The main limitations of this preliminary report are the very small patient population and the lack of follow-up data concerning the clinical outcome of the patients.
A long-term follow-up of the described subjects is currently ongoing. However, it is significant to consider that many of these patients have an advanced cancer disease and may not complete the follow-up as planned due to premature death.
Furthermore, we are also working on other larger patient cohorts including subjects affected by other malignancies. To provide further insights, prospective studies on oncological patients receiving ICI should be performed. In these next analysis, patients cardiovascular risk profile should be described in more detail, including through more specific blood tests and adequate follow-ups. Finally, a study should be conducted also in atherosclerosis preclinical models, in order to obtain more information in regard to the mechanism behind this treatment and to enlighten the potential toxic side effects of ICI treatment.
5. Conclusions
The consequences of ICI therapy on atherosclerosis are still incompletely understood.
The early identification of patients at risk of cardiovascular and cardiotoxicity from cancer target therapies, as well the early diagnosis of possible cardiovascular complications after ICI exposure, are crucial.
Our findings suggested that cancer ICI immunotherapy could be a critical regulator of atherosclerosis, with a possible increased risk of future cerebro- and/or cardiovascular events in younger patients with low cardiovascular risk and longer life expectancy.
Author Contributions
Conceptualization, R.C., M.H. and X.L. (Xiang Li); formal analysis, R.C., X.L. (Xia Lu) and X.L. (Xiang Li); investigation, C.K., P.B., X.L. (Xia Lu), V.P. and M.M.; writing—original draft preparation, R.C., M.H. and X.L. (Xiang Li); ethics documentation, R.C. and A.H.; supervision, M.H., X.L. (Xiang Li) and P.B.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the University of Vienna (Approval no. 1367/2020).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wang, D.Y.; Salem, J.E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal Toxic Effects Associated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varricchi, G.; Galdiero, M.R.; Marone, G.; Criscuolo, G.; Triassi, M.; Bonaduce, D.S.; Marone, G.; Tocchetti, C.G. Cardiotoxicity of immune checkpoint inhibitors. ESMO Open 2017, 2, e000247. [Google Scholar] [CrossRef] [Green Version]
- Titov, A.; Zmievskaya, E.; Ganeeva, I.; Valiullina, A.; Petukhov, A.; Rakhmatullina, A.; Miftakhova, R.; Fainshtein, M.; Rizvanov, A.; Bulatov, E. Adoptive Immunotherapy beyond CAR T-Cells. Cancers 2021, 13, 743. [Google Scholar] [CrossRef] [PubMed]
- Puzanov, I.; Diab, A.; Abdallah, K.; Bingham, C.O.; Brogdon, C.; Dadu, R.; Hamad, L.; Kim, S.; Lacouture, M.E.; LeBoeuf, N.R.; et al. Society for Immunotherapy of Cancer Toxicity Management Working Group. Managing toxicities associated with immune checkpoint inhibitors: Consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J. Immunother. Cancer 2017, 5, 1–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Escudier, M.; Cautela, J.; Malissen, N.; Ancedy, Y.; Orabona, M.; Pinto, J.; Monestier, S.; Grob, J.-J.; Scemama, U.; Jacquier, A.; et al. Clinical Features, Management, and Outcomes of Immune Checkpoint Inhibitor-Related Cardiotoxicity. Circulation 2017, 136, 2085–2087. [Google Scholar] [CrossRef] [PubMed]
- Lutgens, E.; Seijkens, T.T.P. Cancer patients receiving immune checkpoint inhibitor therapy are at an increased risk for atherosclerotic cardiovascular disease. J. Immunother. Cancer 2020, 8, e000300. [Google Scholar] [CrossRef] [PubMed]
- Rominger, A.; Saam, T.; Wolpers, S.; Cyran, C.C.; Schmidt, M.; Foerster, S.; Nikolaou, K.; Reiser, M.F.; Bartenstein, P.; Hacker, M. 18F-FDG PET/CT identifies patients at risk for future vascular events in an otherwise asymptomatic cohort with neoplastic disease. J. Nucl. Med. 2009, 50, 1611–1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Heber, D.; Cal-Gonzalez, J.; Karanikas, G.; Mayerhoefer, M.E.; Rasul, S.; Beitzke, D.; Zhang, X.; Agis, H.; Mitterhauser, M.; et al. Association between Osteogenesis and Inflammation during the Progression of Calcified Plaque Evaluated by 18F-Fluoride and 18F-FDG. J. Nucl. Med. 2017, 58, 968–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calabretta, R.; Hoeller, C.; Pichler, V.; Mitterhauser, M.; Karanikas, G.; Haug, A.; Li, X.; Hacker, M. Immune Checkpoint Inhibitor Therapy Induces Inflammatory Activity in Large Arteries. Circulation 2020, 142, 2396–2398. [Google Scholar] [CrossRef] [PubMed]
- Bucerius, J.; Hyafil, F.; Verberne, H.J.; Slart, R.H.; Lindner, O.; Sciagra, R.; Agostini, D.; Übleis, C.; Gimelli, A.; Hacker, M. Cardiovascular Committee of the European Association of Nuclear Medicine (EANM). Position paper of the Cardiovascular Committee of the European Association of Nuclear Medicine (EANM) on PET imaging of atherosclerosis. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 780–792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aide, N.; Hicks, R.J.; Le Tourneau, C.; Lheureux, S.; Fanti, S.; Lopci, E. FDG PET/CT for assessing tumour response to immunotherapy: Report on the EANM symposium on immune modulation and recent review of the literature. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 238–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veluswamy, P.; Wacker, M.; Scherner, M.; Wippermann, J. Delicate Role of PD-L1/PD-1 Axis in Blood Vessel Inflammatory Diseases: Current Insight and Future Significance. Int. J. Mol. Sci. 2020, 21, 8159. [Google Scholar] [CrossRef] [PubMed]
- Weyand, C.M.; Berry, G.J.; Goronzy, J.J. The immunoinhibitory PD-1/PD-L1 pathway in inflammatory blood vessel disease. J. Leukoc. Biol. 2018, 103, 565–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poels, K.; van Leent, M.M.T.; Boutros, C.; Tissot, H.; Roy, S.; Meerwaldt, A.E.; Toner, Y.C.A.; Reiche, M.E.; Kusters, P.J.H.; Malinova, T.; et al. Immune Checkpoint Inhibitor Therapy Aggravates T Cell-Driven Plaque Inflammation in Atherosclerosis. J. Am. Coll. Cardiol. CardioOnc. 2020, 2, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Grabie, N.; Gotsman, I.; DaCosta, R.; Pang, H.; Stavrakis, G.; Butte, M.J.; Keir, M.E.; Freeman, G.J.; Sharpe, A.H.; Lichtman, A.H. Endothelial programmed death-1 ligand 1 (PD-L1) regulates CD8+ T-cell mediated injury in the heart. Circulation 2007, 116, 2062–2071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}