Clinicopathologic Characteristics of Epstein–Barr Virus-Associated Gastric Cancer Over the Past Decade in Japan



 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
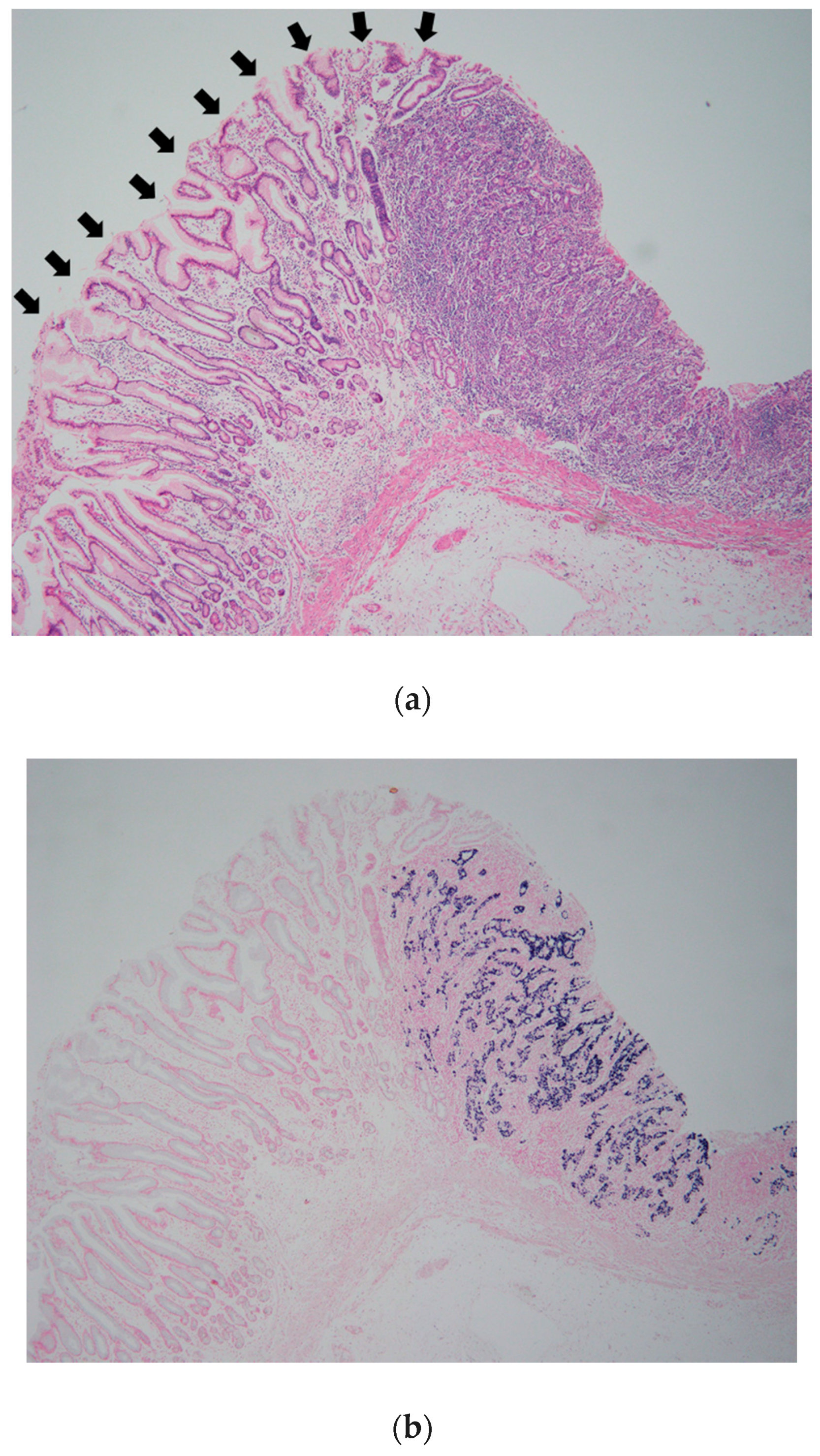
2.2. EBV-Encoded Small RNA 1 (EBER-1) in Situ Hybridization
2.3. Evaluation of Clinicopathologic Findings
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rickinson, A.B.; Kieff, E. Epstein-Barr virus. In Fields Virology, 5th ed.; Fields, B.N., Knipe, D.M., Howley, P.M., Eds.; Lippincott-Williams & Wilkins: Philadelphia, PA, USA, 2007; Volume 2, pp. 2655–2700. [Google Scholar]
- Zur Hausen, H.; Schulte-Holthausen, H.; Klein, G.; Henle, W.; Henle, G.; Clifford, P.; Santesson, L. EBV DNA in biopsies of Burkitt tumours and anaplastic carcinomas of the nasopharynx. Nature 1970, 228, 1056–1058. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Takada, K. Epstein-Barr virus and gastric carcinoma. Mol. Pathol. 2000, 53, 255–261. [Google Scholar] [CrossRef]
- Murphy, G.; Pfeiffer, R.; Camargo, M.C.; Rabkin, C.S. Meta-analysis shows that prevalence of Epstein-Barr virus-positive gastric cancer differs based on sex and anatomic location. Gastroenterology 2009, 137, 824–833. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [Green Version]
- Nishikawa, J.; Iizasa, H.; Yoshiyama, H.; Shimokuri, K.; Kobayashi, Y.; Sasaki, S.; Nakamura, M.; Yanai, H.; Sakai, K.; Suehiro, Y.; et al. Clinical importance of Epstein-Barr virus-associated gastric cancer. Cancers 2018, 10, 167. [Google Scholar] [CrossRef]
- Van Beek, J.; zur Hausen, A.; Klein Kranenbarg, E.; van de Velde, C.J.; Middeldorp, J.M.; van den Brule, A.J.; Meijer, C.J.; Bloemena, E. EBV-positive gastric adenocarcinomas: A distinct clinicopathologic entity with a low frequency of lymph node involvement. J. Clin. Oncol. 2004, 22, 664–670. [Google Scholar] [CrossRef]
- Camargo, M.C.; Kim, W.H.; Chiaravalli, A.M.; Kim, K.M.; Corvalan, A.H.; Matsuo, K.; Yu, J.; Sung, J.J.; Herrera-Goepfert, R.; Meneses-Gonzalez, F.; et al. Improved survival of gastric cancer with tumour Epstein-Barr virus positivity: An international pooled analysis. Gut 2014, 63, 236–243. [Google Scholar] [CrossRef]
- Tada, M.; Murakami, A.; Karita, M.; Yanai, H.; Okita, K. Endoscopic resection of early gastric cancer. Endoscopy 1993, 25, 445–450. [Google Scholar] [CrossRef]
- Tokunaga, M.; Land, C.E. Epstein-Barr virus involvement in gastric cancer: Biomarker for lymph node metastasis. Cancer Epidemiol. Biomarkers Prev. 1998, 7, 449–450. [Google Scholar]
- Park, J.H.; Kim, E.K.; Kim, Y.H.; Kim, J.H.; Bae, Y.S.; Lee, Y.C.; Cheong, J.H.; Noh, S.H.; Kim, H. Epstein-Barr virus positivity, not mismatch repair-deficiency, is a favorable risk factor for lymph node metastasis in submucosa-invasive early gastric cancer. Gastric Cancer. 2016, 19, 1041–1051. [Google Scholar] [CrossRef]
- Shibata, D.; Weiss, L.M. Epstein-Barr virus-associated gastric adenocarcinoma. Am. J. Pathol. 1992, 140, 769–774. [Google Scholar]
- Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer 2011, 14, 101–112. [Google Scholar] [CrossRef] [Green Version]
- Arikawa, J.; Tokunaga, M.; Tashiro, Y.; Tanaka, S.; Sato, E.; Haraguchi, K.; Yamamoto, A.; Toyohira, O.; Tsuchimochi, A. Epstein-Barr virus-positive multiple early gastric cancers and dysplastic lesions: A case report. Pathol. Int. 1997, 47, 730–734. [Google Scholar] [CrossRef]
- Kaizaki, Y.; Hosokawa, O.; Sakurai, S.; Fukayama, M. Epstein-Barr virus-associated gastric carcinoma in the remnant stomach: De novo and metachronous gastric remnant carcinoma. J. Gastroenterol. 2005, 40, 570–577. [Google Scholar] [CrossRef]
- Shibata, D.; Tokunaga, M.; Uemura, Y.; Sato, E.; Tanaka, S.; Weiss, L.M. Association of Epstein-Barr virus with undifferentiated gastric carcinomas with intense lymphoid infiltration. Lymphoepithelioma-like carcinoma. Am. J. Pathol. 1991, 139, 469–474. [Google Scholar]
- Oda, K.; Tamaru, J.; Takenouchi, T.; Mikata, A.; Nunomura, M.; Saitoh, N.; Sarashina, H.; Nakajima, N. Association of Epstein-Barr virus with gastric carcinoma with lymphoid stroma. Am. J. Pathol. 1993, 143, 1063–1071. [Google Scholar]
- Nakamura, S.; Ueki, T.; Yao, T.; Ueyama, T.; Tsuneyoshi, M. Epstein-Barr virus in gastric carcinoma with lymphoid stroma. Special reference to its detection by the polymerase chain reaction and in situ hybridization in 99 tumors, including a morphologic analysis. Cancer 1994, 73, 2239–2249. [Google Scholar] [CrossRef]
- Matsunou, H.; Konishi, F.; Hori, H.; Ikeda, T.; Sasaki, K.; Hirose, Y.; Yamamichi, N. Characteristics of Epstein-Barr virus-associated gastric carcinoma with lymphoid stroma in Japan. Cancer 1996, 77, 1998–2004. [Google Scholar] [CrossRef]
- Yanai, H.; Nishikawa, J.; Mizugaki, Y.; Shimizu, N.; Takada, K.; Matsusaki, K.; Toda, T.; Matsumoto, Y.; Tada, M.; Okita, K. Endoscopic and pathologic features of Epstein-Barr virus-associated gastric carcinoma. Gastrointest. Endosc. 1997, 45, 236–242. [Google Scholar] [CrossRef]
- Nishikawa, J.; Yanai, H.; Mizugaki, Y.; Takada, K.; Tada, M.; Okita, K. Case report: Hypoechoic submucosal nodules: A sign of Epstein-Barr virus-associated early gastric cancer. J. Gastroenterol. Hepatol. 1998, 13, 585–590. [Google Scholar] [CrossRef]
- Watanabe, H.; Enjoji, M.; Imai, T. Gastric carcinoma with lymphoid stroma. Its morphologic characteristics and prognostic correlations. Cancer 1976, 38, 232–243. [Google Scholar] [CrossRef]
- Kawazoe, A.; Kuwata, T.; Kuboki, Y.; Shitara, K.; Nagatsuma, A.K.; Aizawa, M.; Yoshino, T.; Doi, T.; Ohtsu, A.; Ochiai, A. Clinicopathological features of programmed death ligand 1 expression with tumor-infiltrating lymphocyte, mismatch repair, and Epstein-Barr virus status in a large cohort of gastric cancer patients. Gastric Cancer. 2017, 20, 407–415. [Google Scholar] [CrossRef]
- Böger, C.; Behrens, H.M.; Mathiak, M.; Krüger, S.; Kalthoff, H.; Röcken, C. PD-L1 is an independent prognostic predictor in gastric cancer of Western patients. Oncotarget. 2016, 7, 24269–24283. [Google Scholar] [CrossRef] [Green Version]
- Derks, S.; Liao, X.; Chiaravalli, A.M.; Xu, X.; Camargo, M.C.; Solcia, E.; Sessa, F.; Fleitas, T.; Freeman, G.J.; Rodig, S.J.; et al. Abundant PD-L1 expression in Epstein-Barr Virus-infected gastric cancers. Oncotarget. 2016, 7, 32925–32932. [Google Scholar] [CrossRef]
- Ma, C.; Patel, K.; Singhi, A.D.; Ren, B.; Zhu, B.; Shaikh, F.; Sun, W. Programmed Death-Ligand 1 Expression Is Common in Gastric Cancer Associated with Epstein-Barr Virus or Microsatellite Instability. Am. J. Surg. Pathol. 2016, 40, 1496–1506. [Google Scholar] [CrossRef]
- Saito, R.; Abe, H.; Kunita, A.; Yamashita, H.; Seto, Y.; Fukayama, M. Overexpression and gene amplification of PD-L1 in cancer cells and PD-L1+ immune cells in Epstein-Barr virus-associated gastric cancer: The prognostic implications. Mod Pathol. 2017, 30, 427–439. [Google Scholar] [CrossRef]
- Kang, Y.K.; Boku, N.; Satoh, T.; Ryu, M.H.; Chao, Y.; Kato, K.; Chung, H.C.; Chen, J.S.; Muro, K.; Kang, W.K.; et al. Nivolumab in patients with advanced gastric or gastro-oesophageal junction cancer refractory to, or intolerant of, at least two previous chemotherapy regimens (ONO-4538-12, ATTRACTION-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017, 390, 2461–2471. [Google Scholar] [CrossRef]
- Lawrence, M.S.; Stojanov, P.; Polak, P.; Kryukov, G.V.; Cibulskis, K.; Sivachenko, A.; Carter, S.L.; Stewart, C.; Mermel, C.H.; Roberts, S.A.; et al. Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature 2013, 499, 214–218. [Google Scholar] [CrossRef]
- Panda, A.; Mehnert, J.M.; Hirshfield, K.M.; Riedlinger, G.; Damare, S.; Saunders, T.; Kane, M.; Sokol, L.; Stein, M.N.; Poplin, E.; et al. Immune activation and benefit from avelumab in EBV-positive gastric cancer. J. Natl. Cancer Inst. 2018, 110, 316–320. [Google Scholar] [CrossRef]
- Ayers, M.; Lunceford, J.; Nebozhyn, M.; Murphy, E.; Loboda, A.; Kaufman, D.R.; Albright, A.; Cheng, J.D.; Kang, S.P.; Shankaran, V.; et al. IFN-γ-related mRNA profile predicts clinical response to PD-1 blockade. J. Clin. Investig. 2017, 127, 2930–2940. [Google Scholar] [CrossRef]
- Kim, S.T.; Cristescu, R.; Bass, A.J.; Kim, K.M.; Odegaard, J.I.; Kim, K.; Liu, X.Q.; Sher, X.; Jung, H.; Lee, M.; et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat. Med. 2018, 24, 1449–1458. [Google Scholar] [CrossRef]
- Osumi, H.; Kawachi, H.; Murai, K.; Kusafuka, K.; Inoue, S.; Kitamura, M.; Yoshio, T.; Kakusima, N.; Ishihara, R.; Ono, H.; et al. Risk stratification for lymph node metastasis using Epstein-Barr virus status in submucosal invasive (pT1) gastric cancer without lymphovascular invasion: A multicenter observational study. Gastric Cancer 2019. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Feature | Total | EBV Positive | EBV Negative | p Value |
|---|---|---|---|---|
| Sex | ||||
| Male | 735 (68.8%) | 61 (88.4%) | 674 (67.5%) | 0.022 |
| Female | 332 (31.2%) | 8 (11.6%) | 324 (32.5%) | |
| Age (yrs, mean) | 65.6 | 68.9 | <0.001 | |
| Location | ||||
| U | 228 (20.1%) | 30 (37.5%) | 198 (18.8%) | <0.001 |
| M | 520 (45.9%) | 40 (50.0%) | 480 (45.6%) | |
| L | 356 (31.4%) | 6 (7.5%) | 350 (33.3%) | |
| Remnant stomach | 28 (2.5%) | 4 (5.0%) | 24 (2.3%) | |
| Stage | ||||
| Early | 603 (58.6%) | 52 (65.0%) | 551 (52.4%) | 0.029 |
| Advanced | 529 (41.4%) | 28 (35.0%) | 501 (47.5%) | |
| Depth of invasion | ||||
| m | 318 (28.1%) | 19 (23.7%) | 299 (28.4%) | <0.001 |
| sm | 285 (25.2%) | 33 (41.3%) | 252 (24.0%) | |
| mp | 126 (11.1%) | 8 (10.0%) | 118 (11.2%) | |
| ss | 203 (17.9%) | 10 (12.5%) | 193 (18.3%) | |
| sei | 200 (17.7%) | 10 (12.5%) | 190 (18.1%) | |
| Macroscopic type | ||||
| Protruded | 192 (17.0%) | 11 (13.8%) | 181 (17.2%) | 0.428 |
| Depressed | 940 (83.0%) | 69 (86.2%) | 871 (82.8%) | |
| Pathologic type | ||||
| Differentiated | 610 (53.9%) | 37 (46.3%) | 573 (54.5%) | 0.155 |
| Undifferentiated | 522 (46.1%) | 43 (53.7%) | 479 (45.5%) | |
| Lymphatic invasion | ||||
| Presence | 536 (47.3%) | 25 (31.3%) | 511 (48.6%) | 0.003 |
| Absence | 596 (52.7%) | 55 (68.7%) | 541 (51.4%) | |
| Venous invasion | ||||
| Presence | 533 (47.1%) | 25 (31.3%) | 408 (38.8%) | 0.182 |
| Absence | 599 (52.9%) | 55 (68.7%) | 644 (61.2%) | |
| Lymph node metastasis | ||||
| Presence | 445 (41.6%) | 25 (37.3%) | 420 (42.1%) | 0.169 |
| Absence | 622 (58.4%) | 44 (63.7%) | 578 (57.9%) | |
| CLS | ||||
| Presence | 43 (3.8%) | 26 (32.5%) | 17 (1.6%) | <0.001 |
| Absence | 1089 (96.2%) | 54 (67.5%) | 1035 (98.4%) | |
| Multiple cancers | ||||
| Presence | 60 (5.6%) | 10 (14.5%) | 50 (5.0%) | <0.001 |
| Absence | 1007 (94.4%) | 59 (85.5%) | 948 (95.0%) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yanagi, A.; Nishikawa, J.; Shimokuri, K.; Shuto, T.; Takagi, T.; Takagi, F.; Kobayashi, Y.; Yamamoto, M.; Miura, O.; Yanai, H.; et al. Clinicopathologic Characteristics of Epstein–Barr Virus-Associated Gastric Cancer Over the Past Decade in Japan. Microorganisms 2019, 7, 305. https://doi.org/10.3390/microorganisms7090305
Yanagi A, Nishikawa J, Shimokuri K, Shuto T, Takagi T, Takagi F, Kobayashi Y, Yamamoto M, Miura O, Yanai H, et al. Clinicopathologic Characteristics of Epstein–Barr Virus-Associated Gastric Cancer Over the Past Decade in Japan. Microorganisms. 2019; 7(9):305. https://doi.org/10.3390/microorganisms7090305
Chicago/Turabian StyleYanagi, Ayaka, Jun Nishikawa, Kanami Shimokuri, Takuya Shuto, Tatsuya Takagi, Fumiya Takagi, Yuki Kobayashi, Misa Yamamoto, Osamu Miura, Hideo Yanai, and et al. 2019. "Clinicopathologic Characteristics of Epstein–Barr Virus-Associated Gastric Cancer Over the Past Decade in Japan" Microorganisms 7, no. 9: 305. https://doi.org/10.3390/microorganisms7090305
APA StyleYanagi, A., Nishikawa, J., Shimokuri, K., Shuto, T., Takagi, T., Takagi, F., Kobayashi, Y., Yamamoto, M., Miura, O., Yanai, H., Suehiro, Y., Yamasaki, T., Yoshiyama, H., & Sakaida, I. (2019). Clinicopathologic Characteristics of Epstein–Barr Virus-Associated Gastric Cancer Over the Past Decade in Japan. Microorganisms, 7(9), 305. https://doi.org/10.3390/microorganisms7090305