
Development of an Automatic Air-Driven 3D-Printed Spinal Posture Corrector

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Development of Posture Corrector Scheme
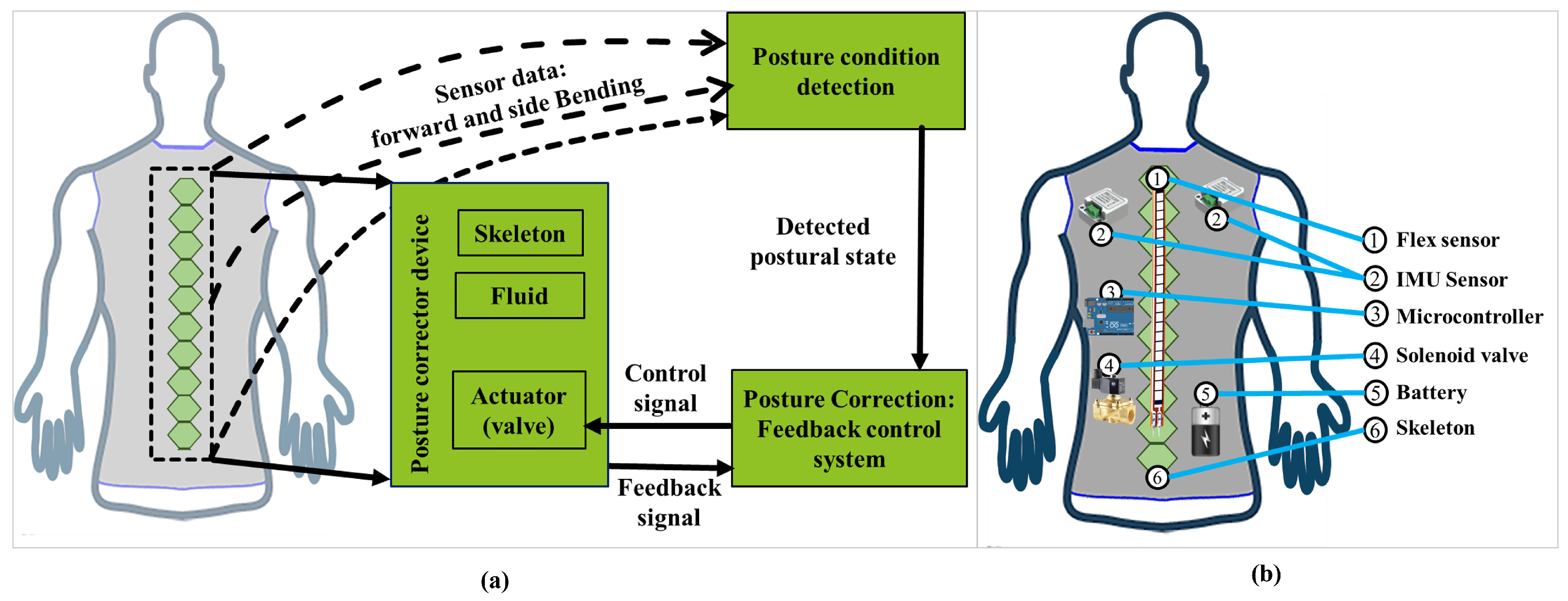
2.1. Overview of the Proposed Posture Corrector
2.2. Sensors
2.3. Design of Skeleton
2.4. Fluid-Driven Actuating Mechanism
2.5. Design of Controller for Posture Corrector
3. Experimental Results
4. Discussion
4.1. Force vs. Pressure
4.2. Force vs. Angular Deviation
4.3. Pressure vs. Angular Deviation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
Appendix A.1. Experimental Data

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ≈Applied Load by Body on Skeleton | With 1 N Load (kPa) | With 2 N Load (kPa) | With 3 N Load (kPa) | With 4 N Load (kPa) | With 5 N Load (kPa) | With 6 N Load (kPa) | With 7 N Load (kPa) |
|---|---|---|---|---|---|---|---|
| Trial no. 1 | 56.40 | 66.70 | 74.87 | 80.66 | 88.32 | 96.67 | 105.75 |
| 2 | 55.42 | 56.54 | 71.22 | 76.24 | 83.66 | 92.23 | 98.35 |
| 3 | 37.50 | 56.47 | 69.66 | 79.32 | 88.18 | 82.22 | 100.17 |
| 4 | 39.50 | 63.72 | 67.34 | 72.26 | 78.29 | 96.58 | 103.85 |
| 5 | 51.70 | 64.43 | 73.71 | 77.61 | 86.10 | 90.24 | 101.60 |
| 6 | 46.13 | 57.83 | 61.47 | 79.98 | 82.93 | 94.59 | 97.95 |
| 7 | 40.55 | 61.15 | 59.56 | 77.29 | 87.29 | 84.41 | 98.73 |
| 8 | 41.88 | 52.13 | 63.86 | 77.81 | 81.55 | 89.70 | 96.65 |
| 9 | 44.02 | 60.88 | 68.56 | 75.35 | 77.84 | 85.18 | 104.16 |
| 10 | 42.23 | 52.43 | 65.53 | 78.46 | 86.24 | 87.23 | 106.82 |
| Average | 44.33 | 59.23 | 68.47 | 75.50 | 84.04 | 89.90 | 101.4 |
| ≈1 N Applied Load by Body on Skeleton | Angular Displacement | Angular Retraction | Deviation | Average |
| Trial no. 1 | 30.50 | 28.98 | 4.98 | 2.61% |
| 2 | 30.50 | 29.50 | 3.28 | |
| 3 | 30.50 | 30.20 | 0.98 | |
| 4 | 30.50 | 29.89 | 2.00 | |
| 5 | 30.50 | 29.62 | 2.89 | |
| 6 | 30.50 | 29.69 | 2.66 | |
| 7 | 30.50 | 29.85 | 2.13 | |
| 8 | 30.50 | 29.81 | 2.26 | |
| 9 | 30.50 | 29.73 | 2.52 | |
| 10 | 30.50 | 29.77 | 2.39 | |
| ≈2N Applied Load | Angular Displacement | Angular Retraction | Deviation | Average |
| Trial no. 1 | 30.50 | 27.75 | 9.03 | 5.59% |
| 2 | 30.50 | 28.92 | 5.18 | |
| 3 | 30.50 | 29.43 | 3.51 | |
| 4 | 30.50 | 28.56 | 6.37 | |
| 5 | 30.50 | 27.95 | 8.37 | |
| 6 | 30.50 | 28.81 | 5.55 | |
| 7 | 30.50 | 28.61 | 6.21 | |
| 8 | 30.50 | 29.71 | 2.60 | |
| 9 | 30.50 | 28.76 | 5.71 | |
| 10 | 30.50 | 29.48 | 3.34 |
| ≈3N Applied Load by Body on Skeleton | Angular Displacement | Angular Retraction | Deviation | Average |
| Trial no. 1 | 30.50 | 27.38 | 10.23 | 7.82% |
| 2 | 30.50 | 27.81 | 8.82 | |
| 3 | 30.50 | 27.87 | 8.62 | |
| 4 | 30.50 | 28.17 | 7.64 | |
| 5 | 30.50 | 27.75 | 9.02 | |
| 6 | 30.50 | 28.58 | 6.30 | |
| 7 | 30.50 | 29.11 | 4.57 | |
| 8 | 30.50 | 28.36 | 7.02 | |
| 9 | 30.50 | 27.95 | 8.36 | |
| 10 | 30.50 | 28.18 | 7.61 | |
| ≈4N Applied Load | Angular Displacement | Angular Retraction | Deviation | Average |
| Trial no. 1 | 30.50 | 26.33 | 13.67 | 10.96% |
| 2 | 30.50 | 27.67 | 9.28 | |
| 3 | 30.50 | 26.63 | 12.69 | |
| 4 | 30.50 | 28.21 | 7.50 | |
| 5 | 30.50 | 26.86 | 11.93 | |
| 6 | 30.50 | 26.63 | 12.69 | |
| 7 | 30.50 | 27.55 | 9.67 | |
| 8 | 30.50 | 26.92 | 11.74 | |
| 9 | 30.50 | 28.02 | 8.15 | |
| 10 | 30.50 | 26.77 | 12.23 | |
| ≈5N Applied Load | Angular Displacement | Angular Retraction | Deviation | Average |
| Trial no. 1 | 30.50 | 23.77 | 22.07 | 18.40% |
| 2 | 30.50 | 25.31 | 17.02 | |
| 3 | 30.50 | 23.94 | 21.51 | |
| 4 | 30.50 | 25.69 | 15.77 | |
| 5 | 30.50 | 24.85 | 18.52 | |
| 6 | 30.50 | 25.47 | 16.49 | |
| 7 | 30.50 | 24.27 | 20.43 | |
| 8 | 30.50 | 25.58 | 16.13 | |
| 9 | 30.50 | 25.69 | 15.77 | |
| 10 | 30.50 | 24.31 | 20.30 | |
| ≈6N Applied Load | Angular Displacement | Angular Retraction | Deviation | Average |
| Trial no. 1 | 30.50 | 21.33 | 30.07 | 26.12% |
| 2 | 30.50 | 22.18 | 27.28 | |
| 3 | 30.50 | 23.65 | 22.47 | |
| 4 | 30.50 | 21.37 | 29.93 | |
| 5 | 30.50 | 22.63 | 25.80 | |
| 6 | 30.50 | 21.57 | 29.28 | |
| 7 | 30.50 | 23.29 | 23.65 | |
| 8 | 30.50 | 22.94 | 24.79 | |
| 9 | 30.50 | 23.23 | 23.85 | |
| 10 | 30.50 | 23.15 | 24.10 | |
| ≈7N Applied Load | Angular Displacement | Angular Retraction | Deviation | Average |
| Trial no. 1 | 30.50 | 19.59 | 35.79 | 32.55% |
| 2 | 30.50 | 21.30 | 30.16 | |
| 3 | 30.50 | 20.53 | 32.69 | |
| 4 | 30.50 | 19.98 | 34.48 | |
| 5 | 30.50 | 20.21 | 33.74 | |
| 6 | 30.50 | 21.94 | 28.07 | |
| 7 | 30.50 | 20.95 | 31.31 | |
| 8 | 30.50 | 21.94 | 28.07 | |
| 9 | 30.50 | 19.85 | 34.92 | |
| 10 | 30.50 | 19.43 | 36.30 |


References
- Asadullah, G.M.; Sabyrov, N.; Kamal, M.A.S.; Ali, M.H. Design of a fluid-driven 3d printed spinal posture corrector. Mater. Today Proc. 2021, 44, 1555–1559. [Google Scholar] [CrossRef]
- Fathi, A. Prevalence rate of postural damages, disorders and anomalies among computer users. Phys. Treat. Specif. Phys. Ther. J. 2016, 1, 59–65. [Google Scholar] [CrossRef][Green Version]
- Hansraj, K.K. Assessment of stresses in the cervical spine caused by posture and position of the head. Surg. Technol. Int. 2014, 25, 277–279. [Google Scholar] [PubMed]
- Liao, D.-Y. Design of a secure, biofeedback, head-and-neck posture correction system. In Proceedings of the IEEE First International Conference on Connected Health: Applications, Systems and Engineering Technologies (CHASE), Washington, DC, USA, 27–29 June 2016; pp. 119–124. [Google Scholar]
- Lawanont, W.; Mongkolnam, P.; Nukoolkit, C. Smartphone posture monitoring system to prevent unhealthy neck postures. In Proceedings of the 12th International Joint Conference on Computer Science and Software Engineering (JCSSE), Songkhla, Thailand, 22–24 July 2015; pp. 331–336. [Google Scholar]
- Sardini, E. Wireless wearable t-shirt for posture monitoring during rehabilitation exercises. IEEE Trans. Instrum. Meas. 2014, 64, 439–448. [Google Scholar] [CrossRef]
- Ribeiro, P. Spine Cop: Posture Correction Monitor and Assistant. Sensors 2020, 20, 5376. [Google Scholar] [CrossRef] [PubMed]
- Yaman, O. Kyphosis and review of the literature. Turk. Neurosurg. 2014, 24, 455–465. [Google Scholar] [CrossRef]
- Finocchiaro, F.M. Treatment of kyphotic deformities in adults: Our experience. Eur. Spine J. 2012, 21, 100–107. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hermanis, A.; Nesenbergs, K. Grid shaped accelerometer network for surface shape recognition. In Proceedings of the 13th Biennial Baltic Electronics Conference, Tallinn, Estonia, 3–5 October 2012; pp. 203–206. [Google Scholar]
- Kumar, A.; Aravindan, M.C. Posturector-the posture corrector. Int. J. Innov. Sci. Res. Technol. 2017, 2, 70–74. [Google Scholar]
- Al-Rahayfeh, A.; Faezipour, M. Application of head flexion detection for enhancing eye gaze direction classification. In Proceedings of the 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 966–969. [Google Scholar]
- El-Sayed, B.; Farra, N.; Moacdieh, N.; Hajj, H.; Haidar, R.; Hajj, Z. A novel mobile wireless sensing system for realtime monitoring of posture and spine stress. In Proceedings of the 1st Middle East Conference on Biomedical Engineering, Sharjah, United Arab Emirates, 21–24 February 2011; pp. 428–431. [Google Scholar]
- Petropoulos, A.; Sikeridis, D.; Antonakopoulos, T. SPoMo: IMU-based real-time sitting posture monitoring. In Proceedings of the IEEE 7th International Conference on Consumer Electronics-Berlin (ICCE-Berlin), Berlin, Germany, 3–6 September 2017; pp. 5–9. [Google Scholar]
- Alsuwaidi, A. Wearable posture monitoring system with vibration feedback. arXiv 2018, arXiv:1810.00189. [Google Scholar]
- Tlili, F.; Haddad, R.; Ouakrim, Y.; Bouallegue, R.; Mezghani, N. A survey on sitting posture monitoring systems. In Proceedings of the 9th International Symposium on Signal, Image, Video and Communications (ISIVC), Rabat, Morocco, 27–30 November 2018; pp. 185–190. [Google Scholar]
- Maidin, N.A. A Prototype development of anti-hunchback device. J. Mech. Eng. 2018, 15, 192–209. [Google Scholar]
- Wong, W.Y. Smart garment for trunk posture monitoring: A preliminary study. Scoliosis 2008, 3, 7. [Google Scholar] [CrossRef] [PubMed]
- Paloschi, D. Validation and Assessment of a Posture Measurement System with Magneto-Inertial Measurement Units. Sensors 2021, 21, 6610. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L. The role of wearables in spinal posture analysis: A systematic review. BMC Musculoskelet. Disord. 2019, 20, 55. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Vogt, D.M.; Rus, D.; Wood, R.J. Fluid-driven origami-inspired artificial muscles. Proc. Natl. Acad. Sci. USA 2017, 114, 13132–13137. [Google Scholar] [CrossRef] [PubMed]
- Japan Demographics: What’s the Average Life Expectancy, Height, and Monthly Income? Available online: Https://livejapan.com/en/in-tokyo/in-pref-tokyo/in-shinjuku/article-a0000962 (accessed on 16 September 2020).
- Busscher, I. Comparative anatomical dimensions of the complete human and porcine spine. Eur. Spine J. 2010, 19, 1104–1114. [Google Scholar] [CrossRef] [PubMed]












| Parameters | Material Used |
|---|---|
| Skeleton | Flex material |
| Skeleton frame | Flex material |
| Frame cap | Flex material |
| Parameters | Height (mm) | Width (mm) |
|---|---|---|
| Skeleton (single block) | 40 | 50 |
| Skeleton frame (single block) | 40 | 70 |
| Frame cap (single block) | 40 | 60 |
| Full skeleton blocks | 560 | 50 |
| Full Skeleton frame | 560 | 70 |
| Full frame cap | 560 | 60 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asadullah, G.M.; Ali, M.H.; Hashikura, K.; Kamal, M.A.S.; Yamada, K. Development of an Automatic Air-Driven 3D-Printed Spinal Posture Corrector. Actuators 2022, 11, 184. https://doi.org/10.3390/act11070184
Asadullah GM, Ali MH, Hashikura K, Kamal MAS, Yamada K. Development of an Automatic Air-Driven 3D-Printed Spinal Posture Corrector. Actuators. 2022; 11(7):184. https://doi.org/10.3390/act11070184
Chicago/Turabian StyleAsadullah, G. M., Md. Hazrat Ali, Kotaro Hashikura, Md Abdus Samad Kamal, and Kou Yamada. 2022. "Development of an Automatic Air-Driven 3D-Printed Spinal Posture Corrector" Actuators 11, no. 7: 184. https://doi.org/10.3390/act11070184
APA StyleAsadullah, G. M., Ali, M. H., Hashikura, K., Kamal, M. A. S., & Yamada, K. (2022). Development of an Automatic Air-Driven 3D-Printed Spinal Posture Corrector. Actuators, 11(7), 184. https://doi.org/10.3390/act11070184