Can Genetics Predict Sports Injury? The Association of the Genes GDF5, AMPD1, COL5A1 and IGF2 on Soccer Player Injury Occurrence


Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Methods
2.1. Participants
2.2. Sample Collection
2.3. Data Analysis
3. Results
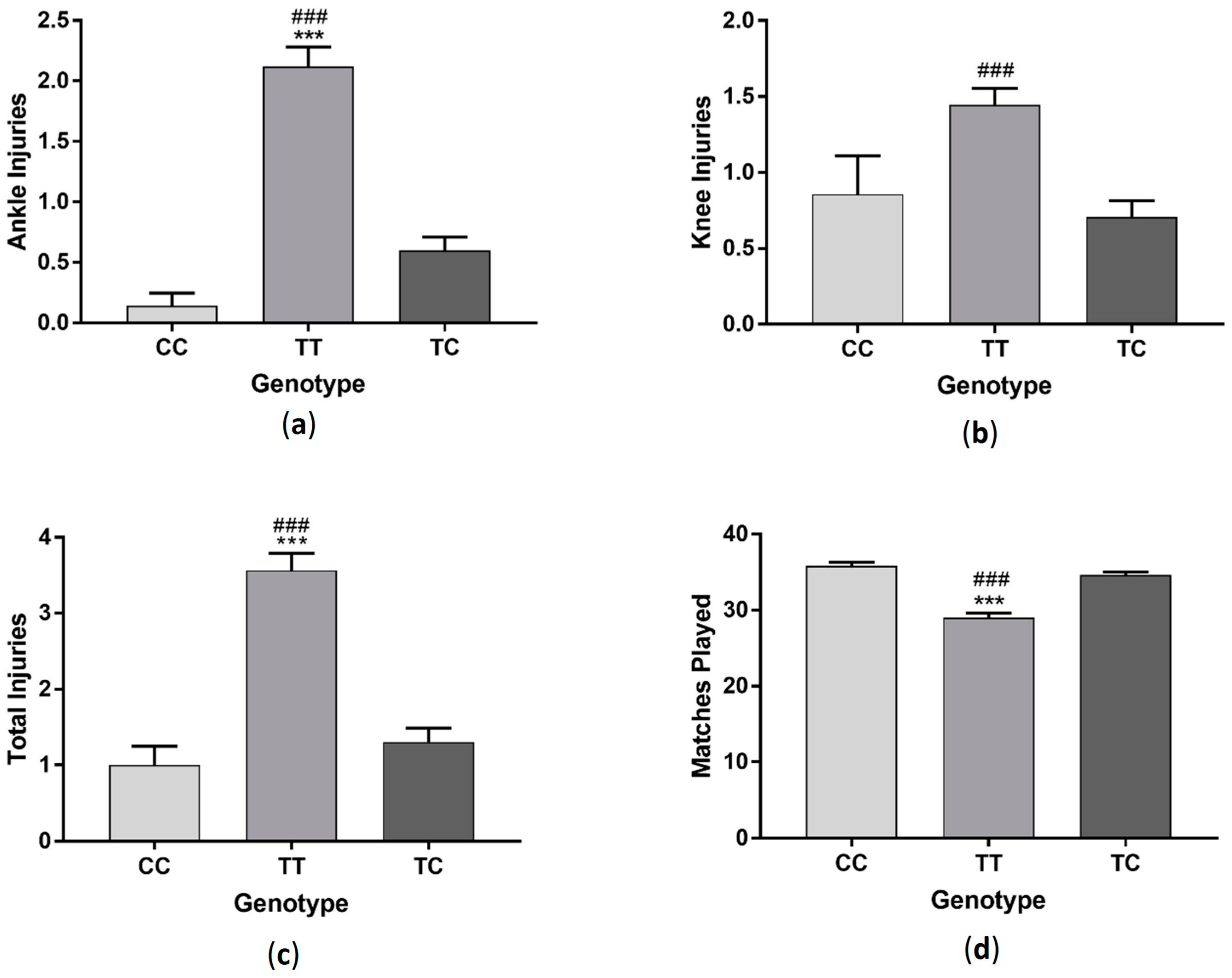
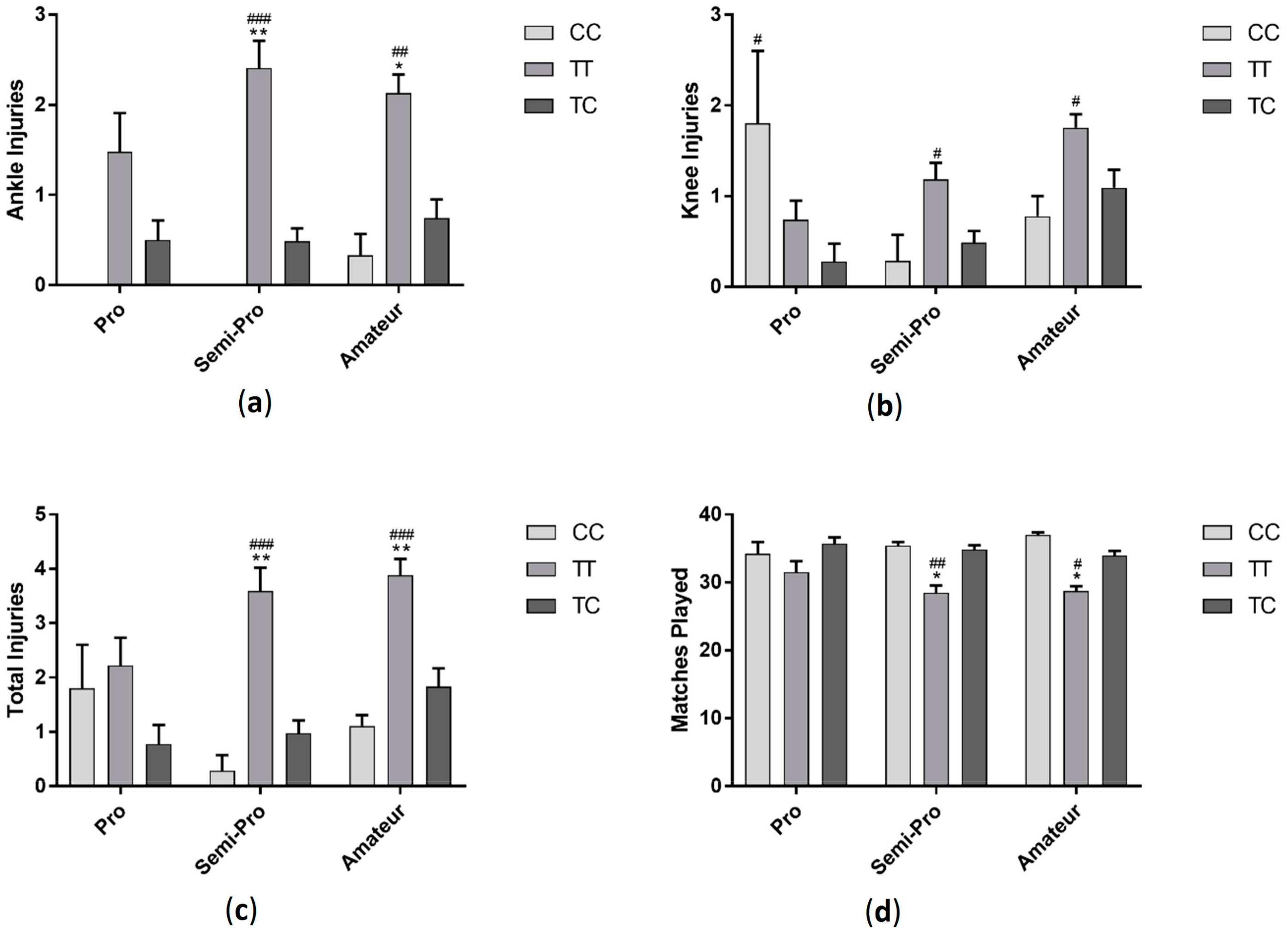
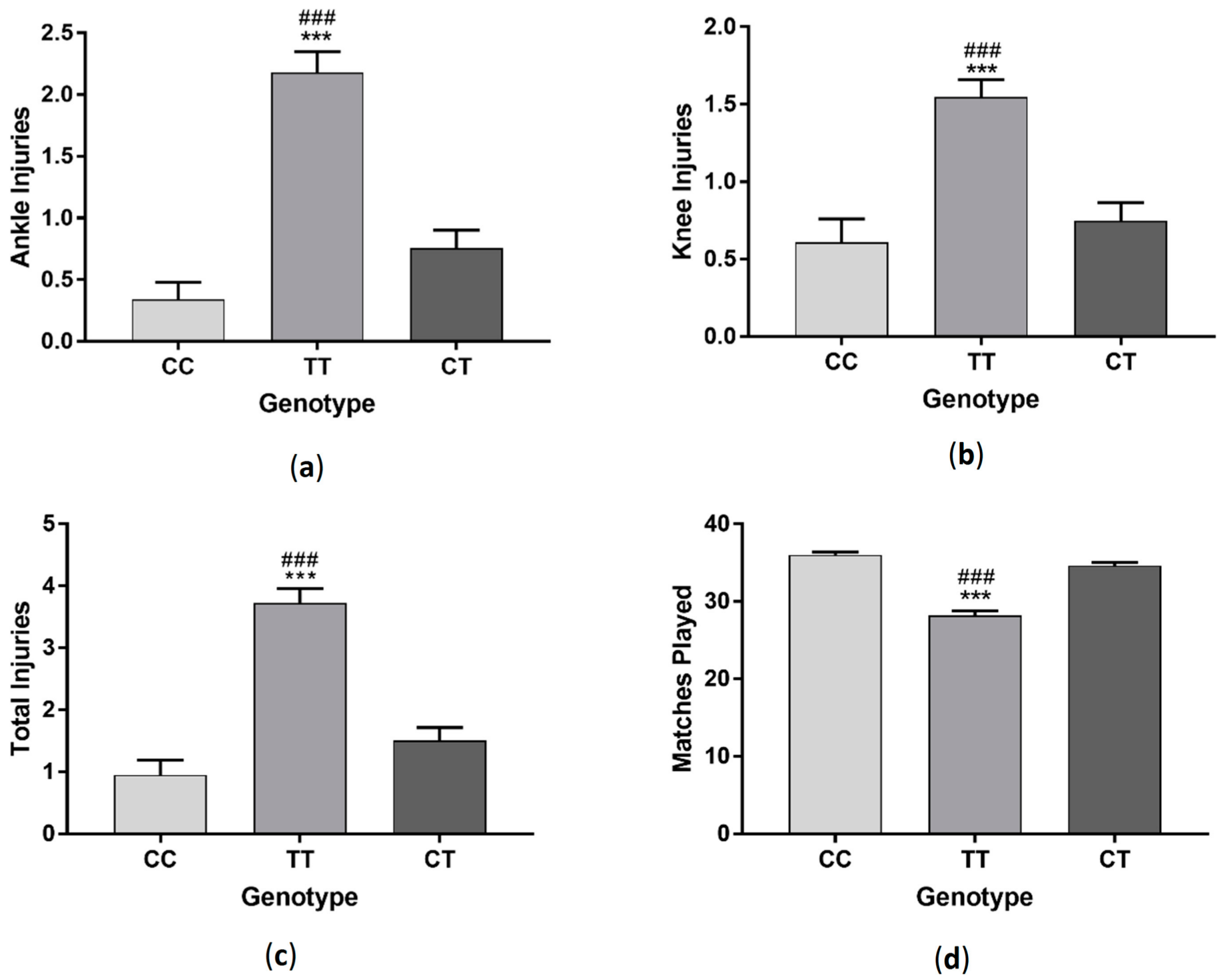
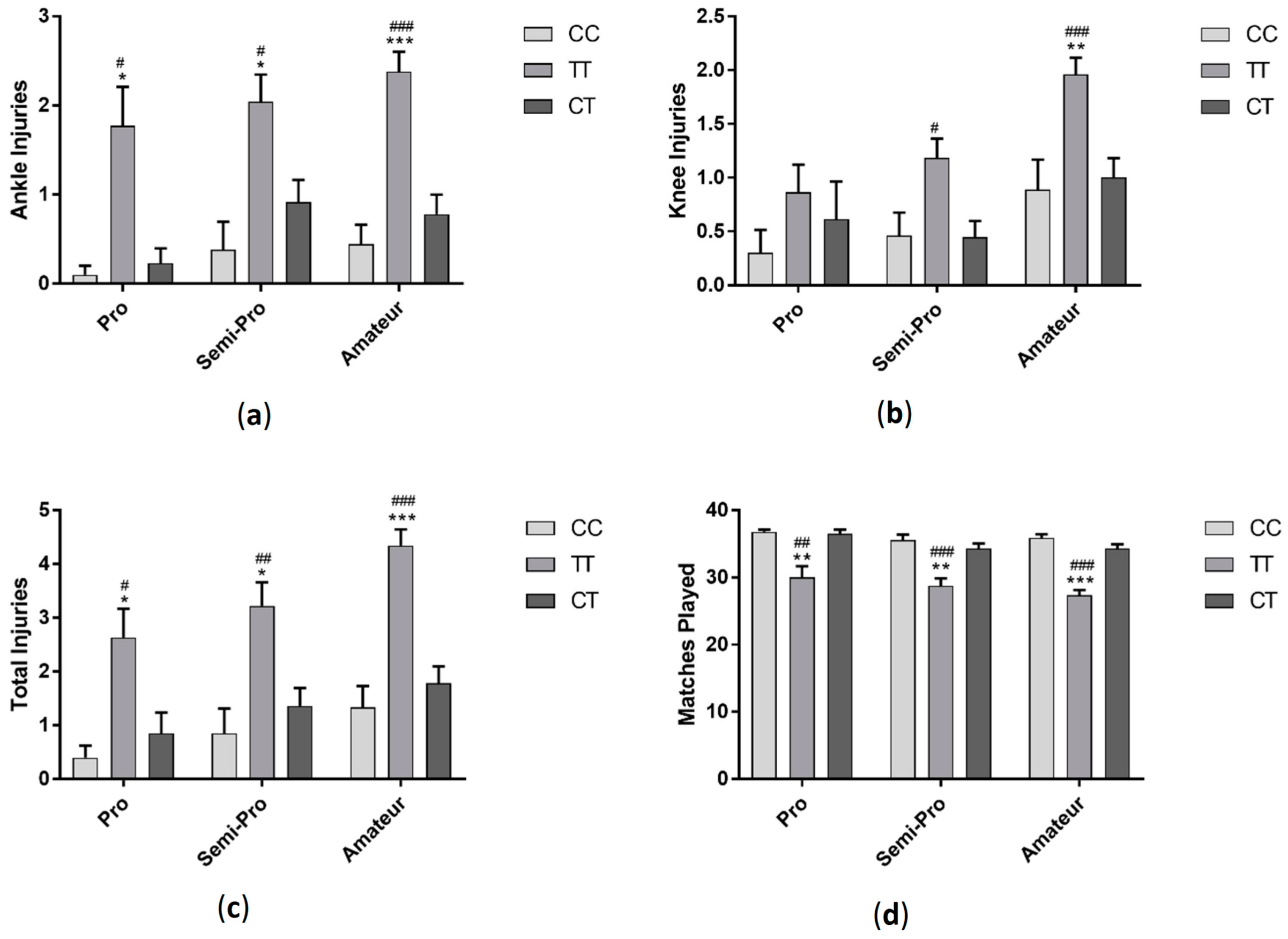
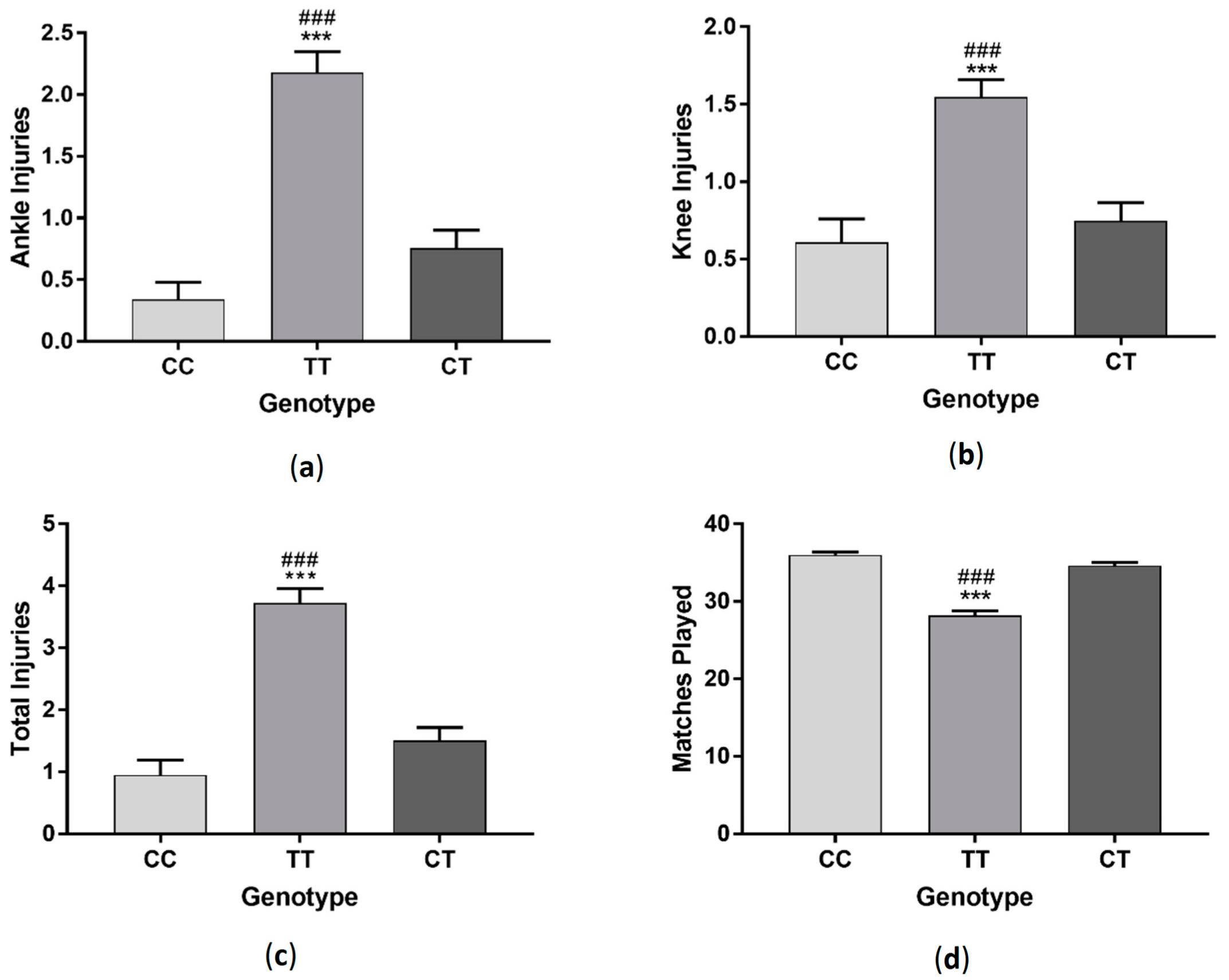
3.1. GDF5 Genotype Effect on Injury and Matches Played
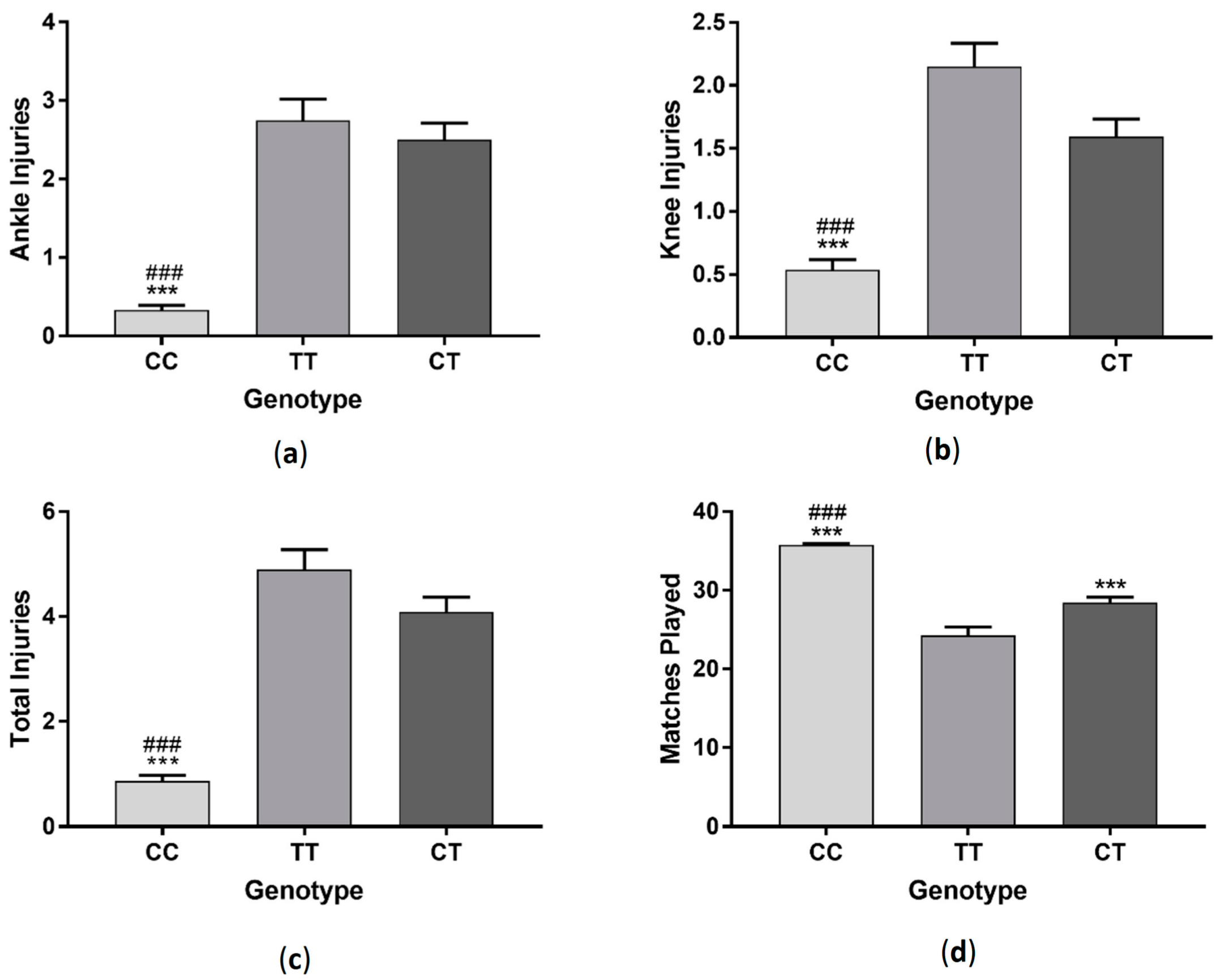
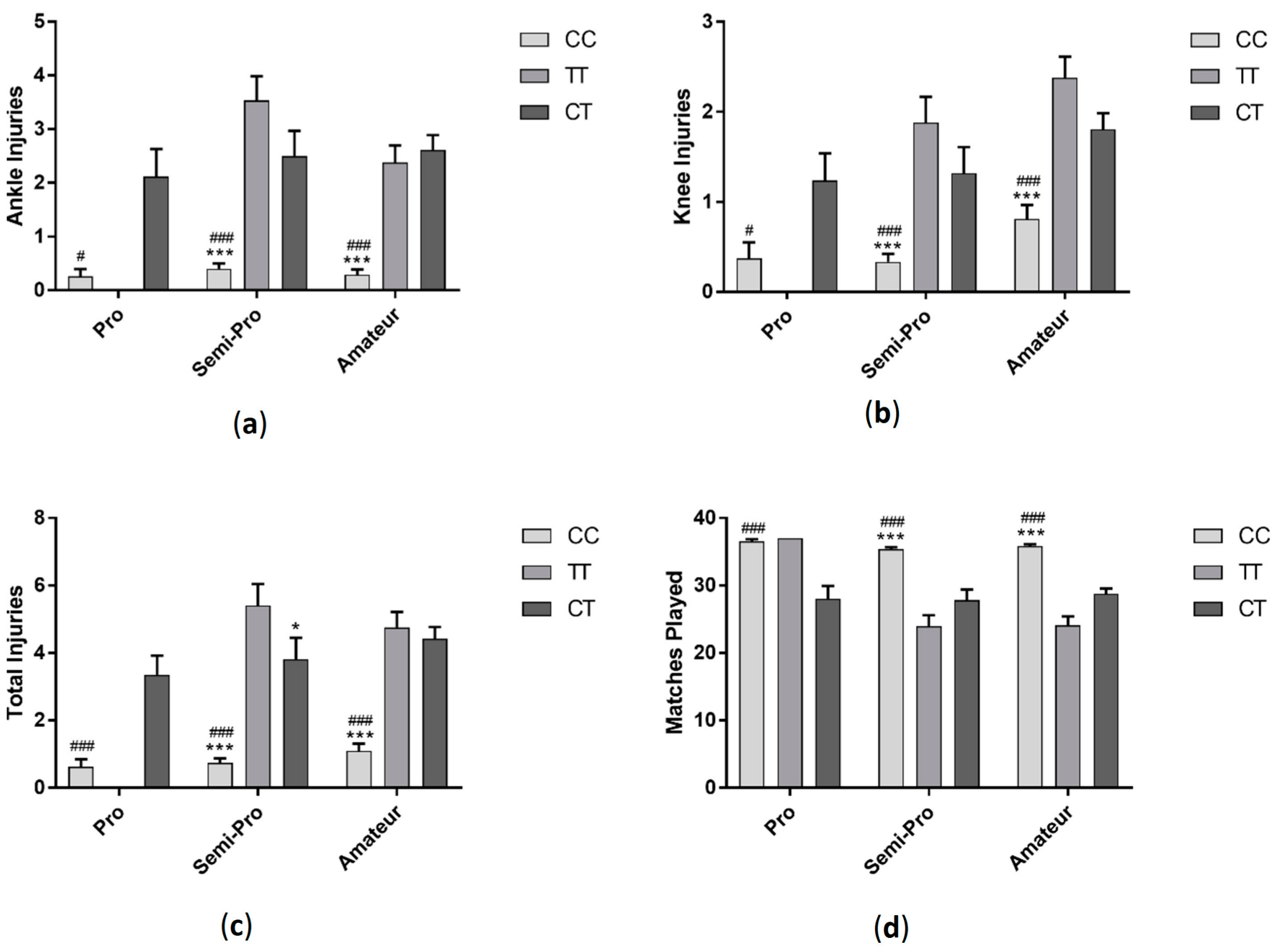
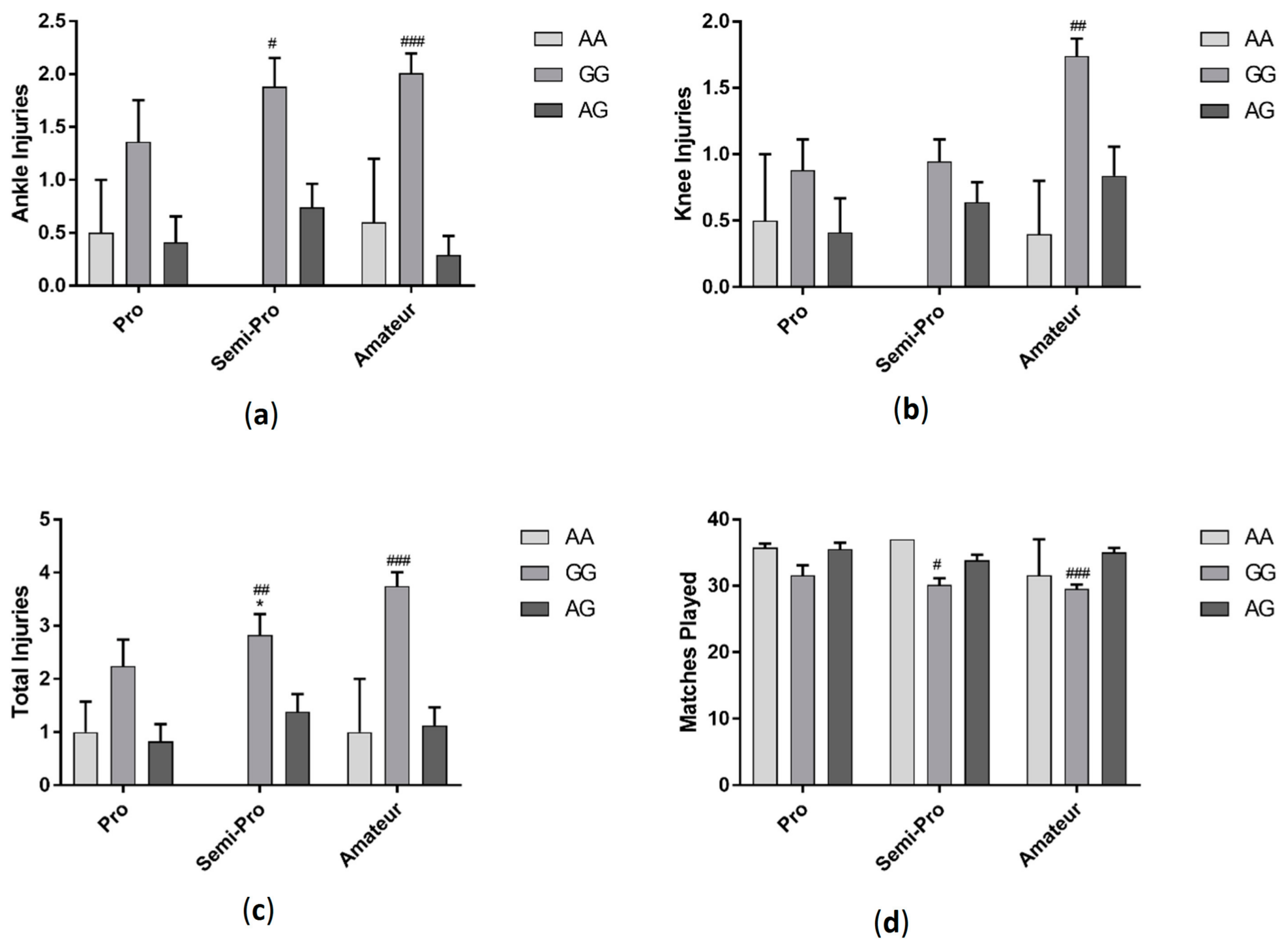
3.2. AMPD1 Genotype Effect on Injury and Matches Played
3.3. COL5A1 Genotype Effect on Injury and Matches Played
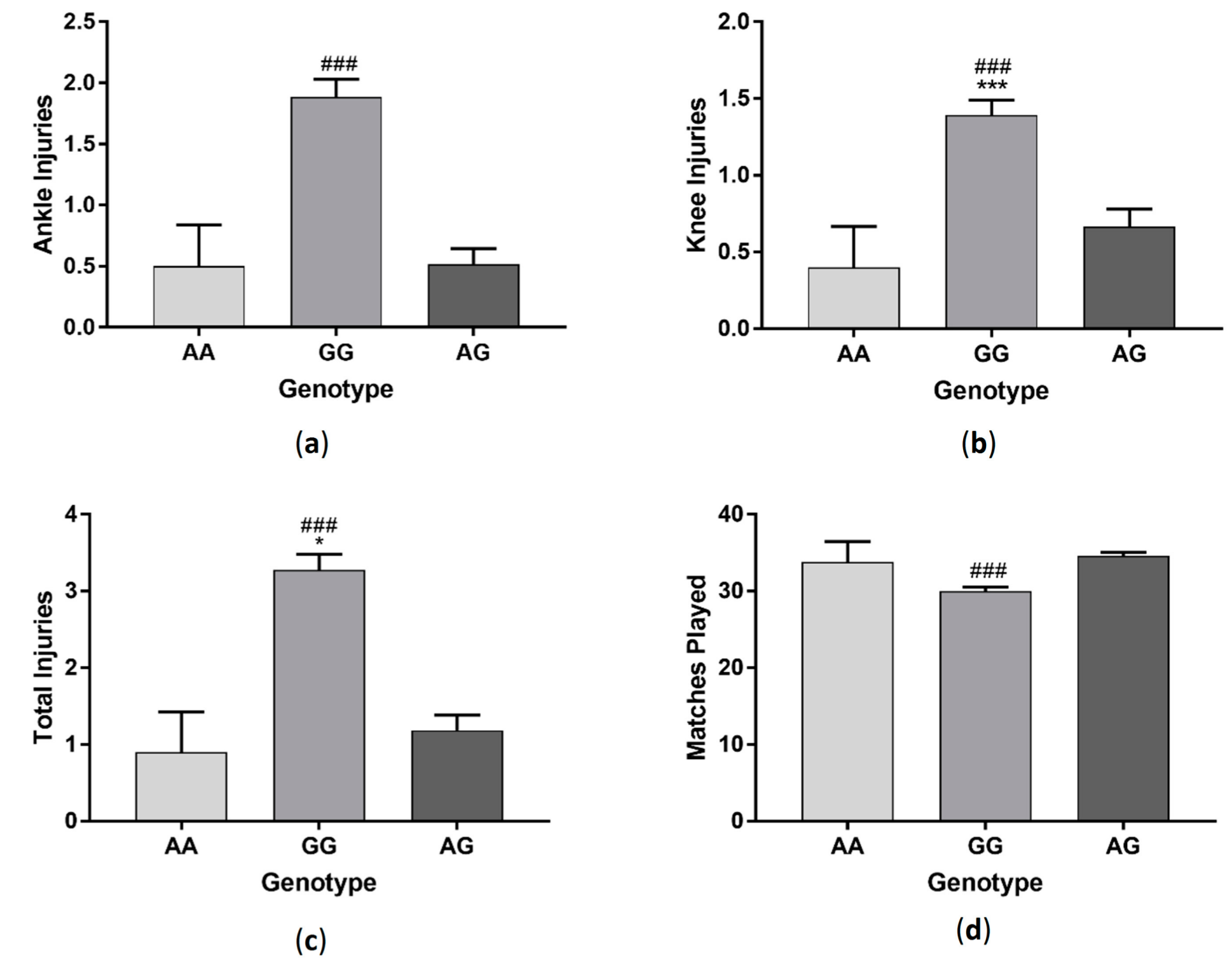
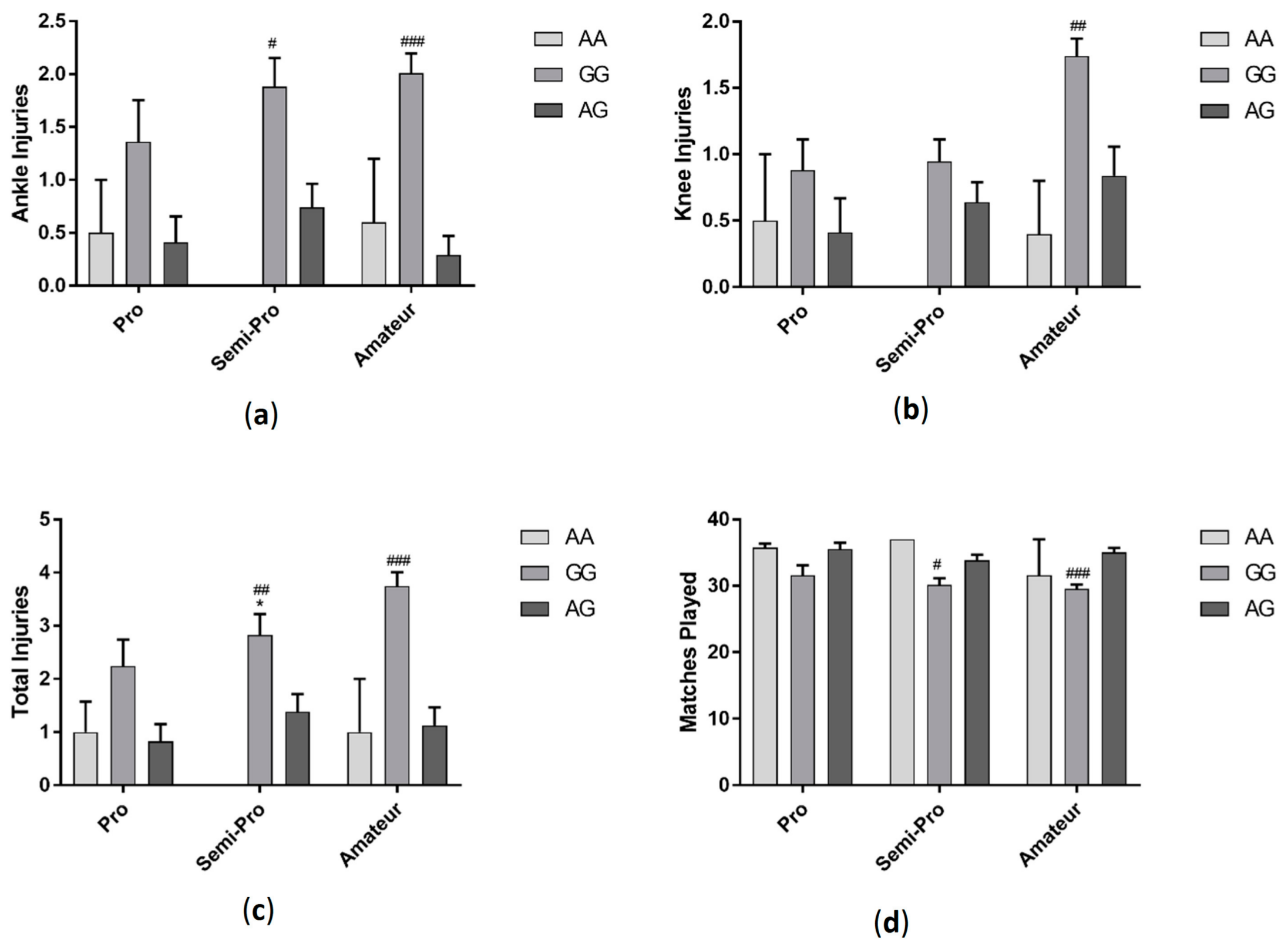
3.4. IGF2 Genotype Effect on Injury and Matches Played
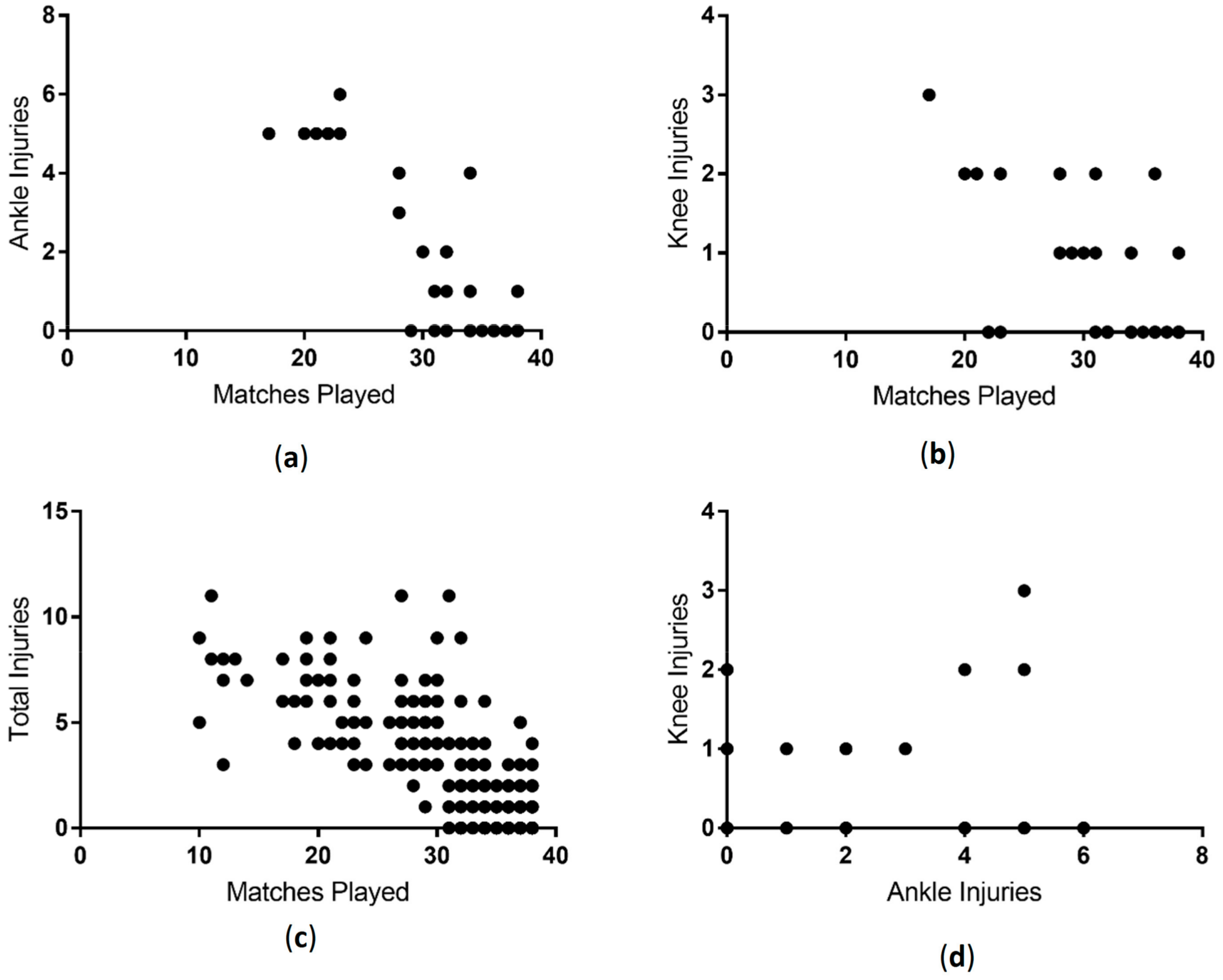
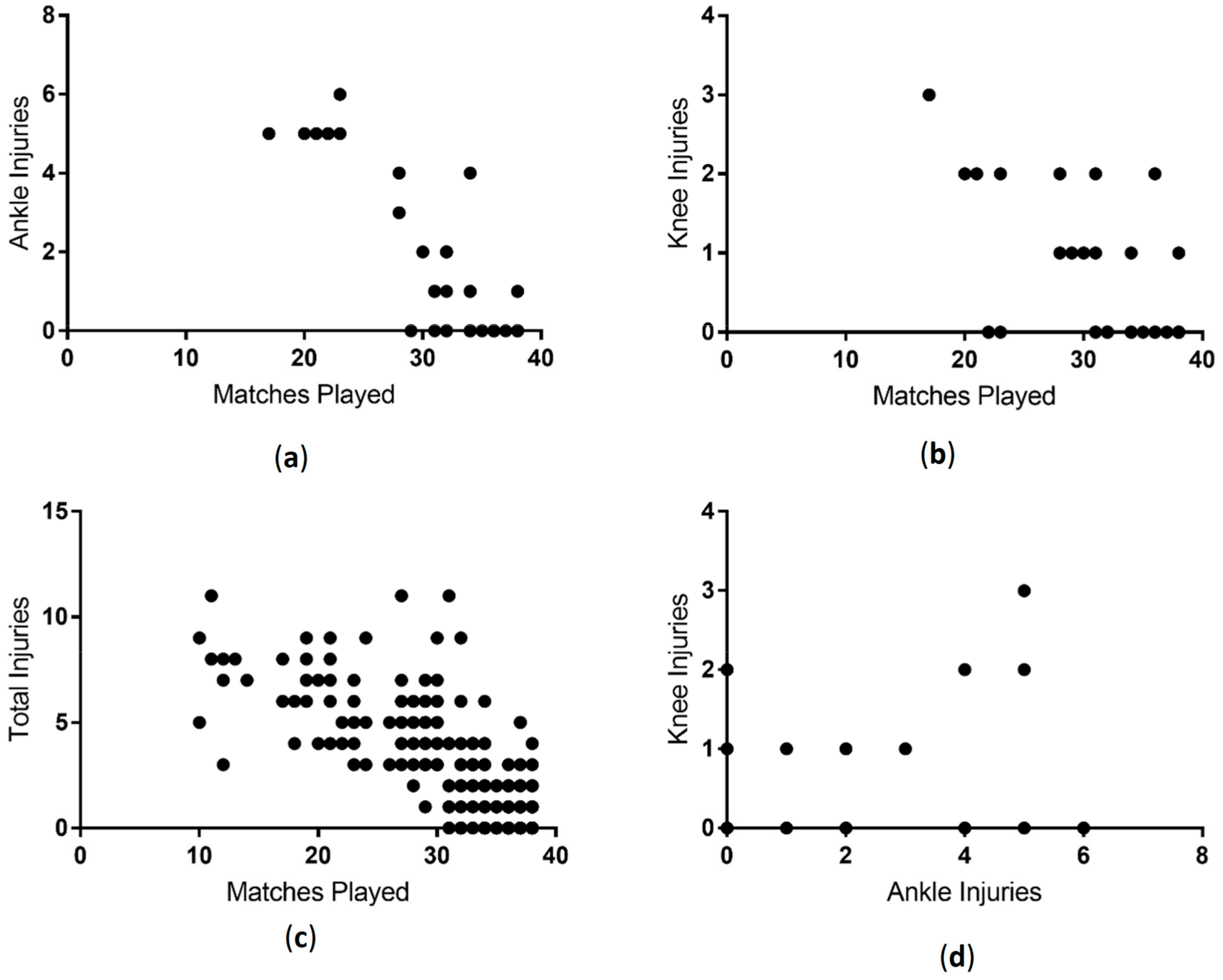
3.5. Correlation between Matches Played and Injuries
4. Discussion
5. Overall Limitations and Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- Agel, J.; Evans, T.A.; Dick, R.; Putukian, M.; Marshall, S.W. Descriptive epidemiology of collegiate men’s soccer injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2002–2003. J. Athl. Train. 2007, 42, 270–277. [Google Scholar] [PubMed]
- Hawkins, R.D.; Hulse, M.A.; Wilkinson, C.; Hodson, A.; Gibson, M. The association football medical research programme: An audit of injuries in professional football. Br. J. Sports Med. 2001, 35, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, Y.; Mabuchi, A.; Shi, D.; Kubo, T.; Takatori, Y.; Saito, S.; Fujioka, M.; Sudo, A.; Uchida, A.; Yamamoto, S. A functional polymorphism in the 5′ UTR of GDF5 is associated with susceptibility to osteoarthritis. Nat. Genet. 2007, 39, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Southam, L.; Rodriguez-Lopez, J.; Wilkins, J.M.; Pombo-Suarez, M.; Snelling, S.; Gomez-Reino, J.J.; Chapman, K.; Gonzalez, A.; Loughlin, J. An SNP in the 5′-UTR of GDF5 is associated with osteoarthritis susceptibility in Europeans and with in vivo differences in allelic expression in articular cartilage. Hum. Mol. Genet. 2007, 16, 2226–2232. [Google Scholar] [CrossRef] [PubMed]
- Evangelou, E.; Chapman, K.; Meulenbelt, I.; Karassa, F.B.; Loughlin, J.; Carr, A.; Doherty, M.; Doherty, S.; Gómez-Reino, J.J.; Gonzalez, A. Large-scale analysis of association between GDF5 and FRZB variants and osteoarthritis of the hip, knee, and hand. Arthritis Rheumatism 2009, 60, 1710–1721. [Google Scholar] [CrossRef] [PubMed]
- Sabina, R.L.; Swain, J.L.; Olanow, C.W.; Bradley, W.G.; Fishbein, W.N.; DiMauro, S.; Holmes, E.W. Myoadenylate deaminase deficiency. Functional and metabolic abnormalities associated with disruption of the purine nucleotide cycle. J. Clin. Investig. 1984, 73, 720–730. [Google Scholar] [CrossRef] [PubMed]
- Thomaes, T.; Thomis, M.; Onkelinx, S.; Fagard, R.; Matthijs, G.; Buys, R.; Schepers, D.; Cornelissen, V.; Vanhees, L. A genetic predisposition score for muscular endophenotypes predicts the increase in aerobic power after training: The CAREGENE study. BMC Genet. 2011, 12, 84. [Google Scholar] [CrossRef] [PubMed]
- Abrahams, Y.; Laguette, M.-J.; Prince, S.; Collins, M. Polymorphisms within the COL5A1 3′-UTR That Alters mRNA Structure and the MIR608 Gene are Associated with Achilles Tendinopathy. Ann. Hum. Genet. 2013, 77, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Devaney, J.M.; Hoffman, E.P.; Gordish-Dressman, H.; Kearns, A.; Zambraski, E.; Clarkson, P.M. IGF-II gene region polymorphisms related to exertional muscle damage. J. Appl. Physiol. 2007, 102, 1815–1823. [Google Scholar] [CrossRef] [PubMed]
- Jardine Lloyd Thompson (JLT). JLT Specialty Sports Injury Index|JLT. 2017. Available online: http://www.jltspecialty.com/Media-Centre/Press-Release/2017/January/JLT-Specialty-Sport-Injury-Index (accessed on 8 January 2018).
- Fernández-Cuevas, I.; Gómez Carmona, P.M.; Sillero Quintana, M.; Noya Salces, J.; Arnaiz-Lastras, J.; Pastor Barrón, A. Economic Costs Estimation of Soccer Injuries in First and Second Spanish Division Professional Teams. 2010. Available online: https://www.researchgate.net/publication/258726802_Economic_costs_estimation_of_soccer_injuries_in_first_and_second_spanish_division_professional_teams (accessed on 8 January 2018).
- Chen, B.; Li, B.; Qi, Y.J.; Tie, K.; Chen, L.B. Association study between growth differentiation factor 5 polymorphism and non-contact anterior cruciate ligament rupture in Chinese Han population. Int. J. Clin. Exp. Med. 2015, 8, 22484–22490. [Google Scholar] [PubMed]
- Posthumus, M.; Collins, M.; Cook, J.; Handley, C.J.; Ribbans, W.J.; Smith, R.K.; Schwellnus, M.P.; Raleigh, S.M. Components of the transforming growth factor-family and the pathogenesis of human Achilles tendon pathology—A genetic association study. Rheumatology 2010, 49, 2090–2097. [Google Scholar] [CrossRef] [PubMed]
- Date, H.; Furumatsu, T.; Sakoma, Y.; Yoshida, A.; Hayashi, Y.; Abe, N.; Ozaki, T. GDF-5/7 and bFGF activate integrin α2-mediated cellular migration in rabbit ligament fibroblasts. J. Orthop. Res. 2009, 28. [Google Scholar] [CrossRef] [PubMed]
- Collins, C. Resistance Training, Recovery and Genetics: AMPD1 the Gene for Recovery. J. Athl. Enhanc. 2017, 6. [Google Scholar] [CrossRef]
- Mokone, G.G.; Schwellnus, M.P.; Noakes, T.D.; Collins, M. The COL5A1 gene and Achilles tendon pathology. Scand. J. Med. Sci. Sports 2006, 16, 19–26. [Google Scholar] [CrossRef] [PubMed]
- September, A.V.; Cook, J.; Handley, C.J.; van der Merwe, L.; Schwellnus, M.P.; Collins, M. Variants within the COL5A1 gene are associated with Achilles tendinopathy in two populations. Br. J. Sports Med. 2009, 43, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Posthumus, M.; September, A.V.; O’Cuinneagain, D.; van der Merwe, W.; Schwellnus, M.P.; Collins, M. The COL5A1 Gene Is Associated with Increased Risk of Anterior Cruciate Ligament Ruptures in Female Participants. Am. J. Sports Med. 2009, 37, 2234–2240. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.C.; Miller, C.J.; Posthumus, M.; Schwellnus, M.P.; Collins, M. The COL5A1 gene, ultra-marathon running performance, and range of motion. Int. J. Sports Physiol. Perform. 2011, 6, 485–496. [Google Scholar] [CrossRef] [PubMed]
- Pruna, R.; Artells, R.; Ribas, J.; Montoro, B.; Cos, F.; Muñoz, C.; Rodas, G.; Maffulli, N. Single nucleotide polymorphisms associated with non-contact soft tissue injuries in elite professional soccer players: Influence on degree of injury and recovery time. BMC Musculoskelet. Disord. 2013, 14, 221. [Google Scholar] [CrossRef] [PubMed]
- Ben-Zaken, S.; Meckel, Y.; Nemet, D.; Eliakim, A. High prevalence of the IGF2 rs680 GG polymorphism among top-level sprinters and jumpers. Growth Horm. IGF Res. 2017, 37, 26–30. [Google Scholar] [CrossRef] [PubMed]



© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McCabe, K.; Collins, C. Can Genetics Predict Sports Injury? The Association of the Genes GDF5, AMPD1, COL5A1 and IGF2 on Soccer Player Injury Occurrence. Sports 2018, 6, 21. https://doi.org/10.3390/sports6010021
McCabe K, Collins C. Can Genetics Predict Sports Injury? The Association of the Genes GDF5, AMPD1, COL5A1 and IGF2 on Soccer Player Injury Occurrence. Sports. 2018; 6(1):21. https://doi.org/10.3390/sports6010021
Chicago/Turabian StyleMcCabe, Kiah, and Christopher Collins. 2018. "Can Genetics Predict Sports Injury? The Association of the Genes GDF5, AMPD1, COL5A1 and IGF2 on Soccer Player Injury Occurrence" Sports 6, no. 1: 21. https://doi.org/10.3390/sports6010021
APA StyleMcCabe, K., & Collins, C. (2018). Can Genetics Predict Sports Injury? The Association of the Genes GDF5, AMPD1, COL5A1 and IGF2 on Soccer Player Injury Occurrence. Sports, 6(1), 21. https://doi.org/10.3390/sports6010021