
Economic Analysis of Alternative Strategies for Detection of ALK Rearrangements in Non Small Cell Lung Cancer

Abstract
:1. Introduction
2. Methods Section
3. Results

{kind=link}
{kind=link}
| Variable | Value | Lower Limit | Upper Limit | Source |
|---|---|---|---|---|
| Cost of IHC per sample (USA) | $89 | $54 | $124 | Lab. survey |
| Cost of IHC per sample (Europe) | $67.88 | $33 | $112.73 | Lab. survey |
| Cost of FISH per sample (USA) | $330 | $300 | $360 | Lab. survey |
| Cost of FISH per sample (Europe) | $197.72 | $169.09 | $244.20 | Lab. survey |
| IHC reimbursement (USA) | $90.46 | - | - | Medicare [17] |
| FISH reimbursement (USAA) | $216.35 | $214.52 | $217.38 | Medicare [17] |
| ALK testing reimbursement (Europe) | $155.50 | $132 | $186 | - |
| Probability of ALK+ result by IHC | 4.0% | 3.4% | 10.1% | Paik [18], Cabillic [19], Ali [20], Sullivan [21] |
| Probability of ALK+ result by FISH | 4.2% | 3.8% | 6.4% | Paik [18], Cabillic [19], Ali [20], Sullivan [21] |
| Probability of ALK+ result by either IHC or FISH | 4.9% | 3.8% | 10.1% | Paik [18], Cabillic [19], Ali [20], Sullivan [21] |
| Probability of ALK+ result by IHC but ALK− by FISH | 0.7% | 0.0% | 3.7% | Paik [18], Cabillic [19], Ali [20], Sullivan [21] |
| Failure rate of ALK IHC | 1.2% | - | - | Zhou [22] |
| Failure rate of ALK FISH | 6.6% | - | - | Zhou [22] |
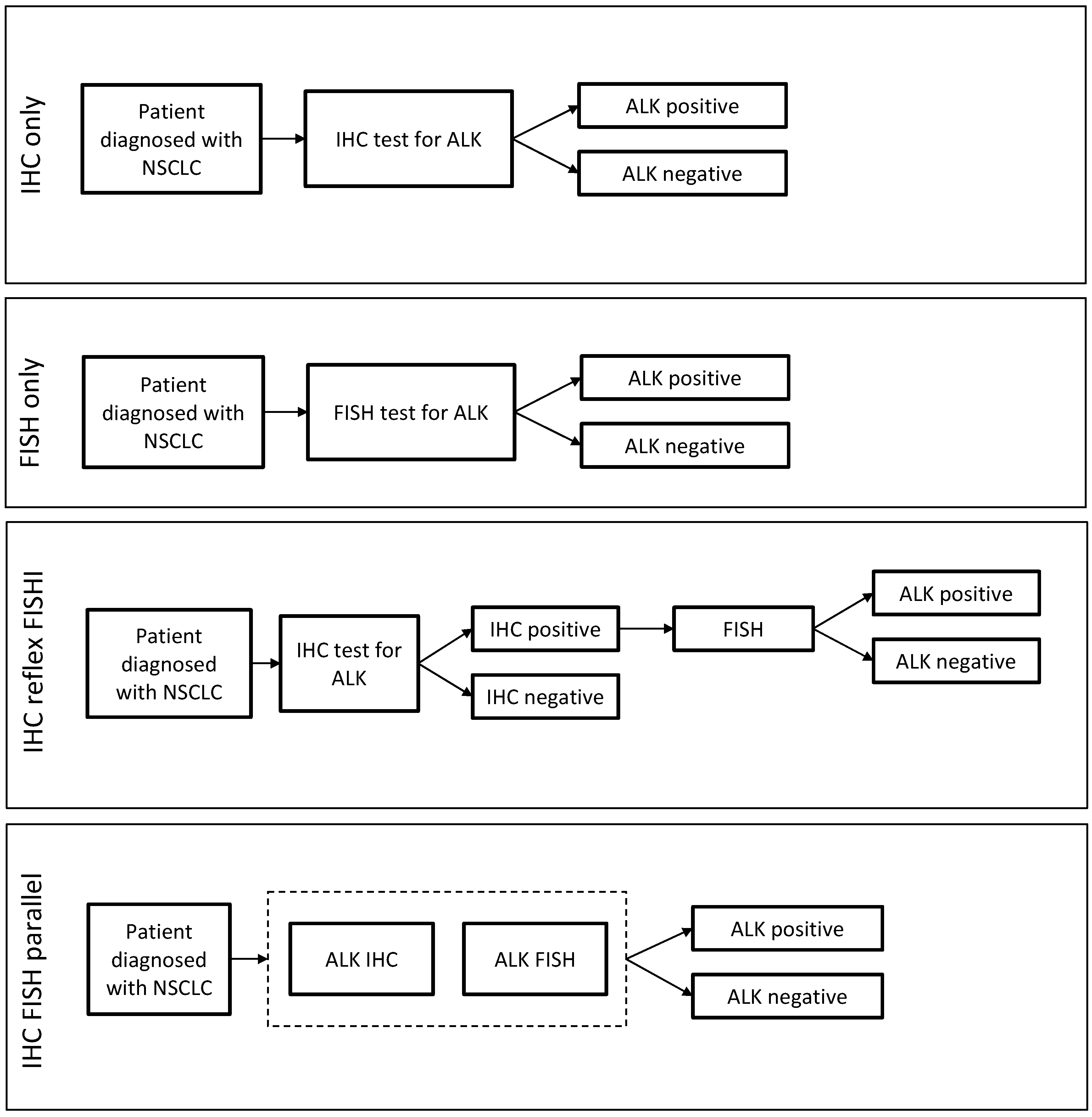
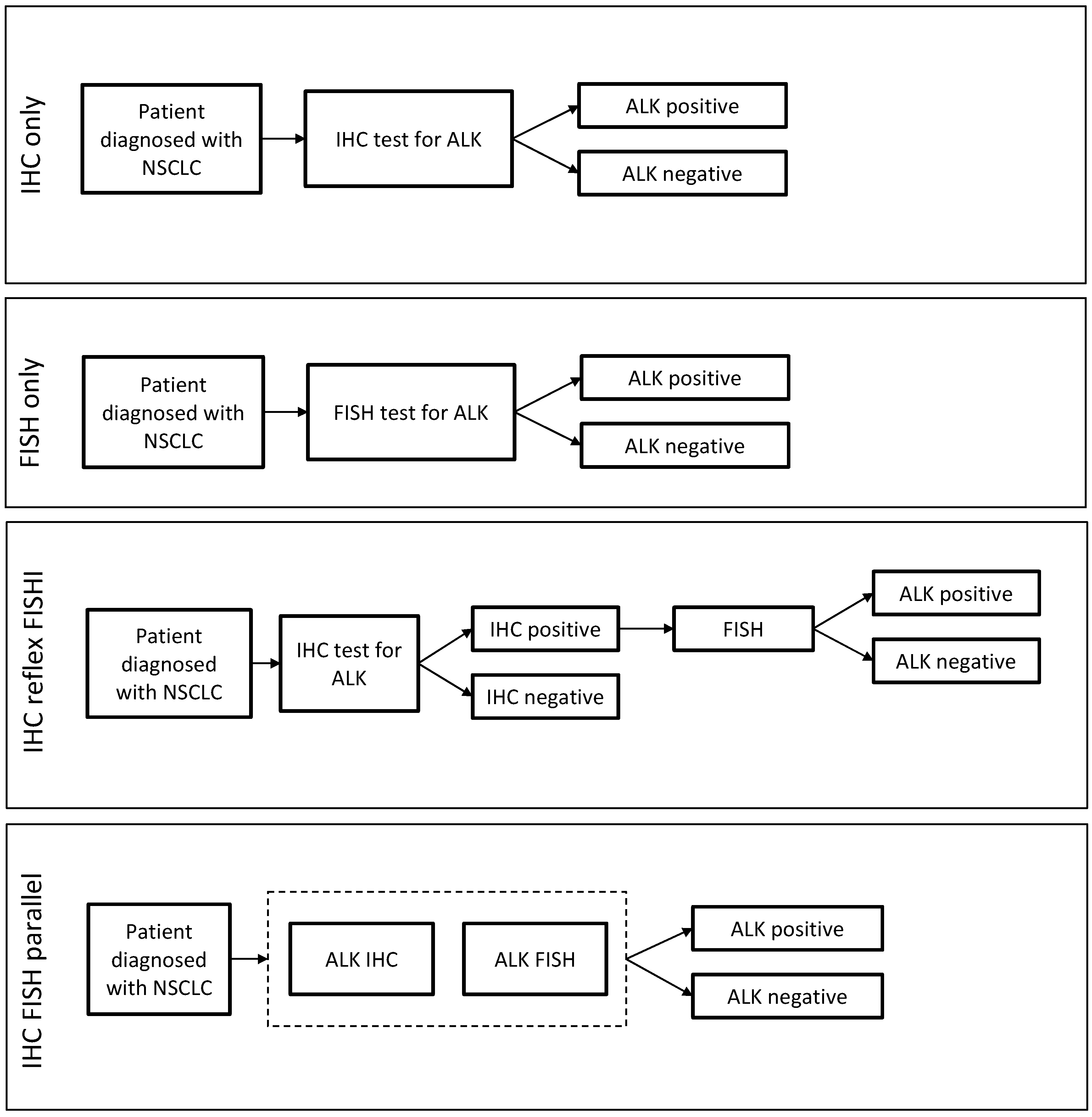
| Testing Strategy | Time to Result (Working Days) | ALK Positivity Rate | US | Europe | ||
|---|---|---|---|---|---|---|
| Average Cost (USD) | Average Reimbursement * (USD) | Average Cost (USD) | Average Reimbursement ** (USD) | |||
| IHC only | 1 to 2 days | 4.0% | $90.07 | $91.55 | $68.69 | $157.37 |
| FISH only | 2 to 5 days | 4.2% | $351.78 | $230.63 | $210.77 | $165.76 |
| IHC reflex FISH | 1 to 2 days if IHC−; 3 to 7 days if IHC+ | 3.3% | $104.12 | $100.76 | $77.11 | $157.37 |
| IHC FISH parallel | 2 to 5 days | 4.9% | $441.85 | $322.17 | $279.46 | $157.37 |
3.1. Comparison of Workflow

3.2. Comparison of ALK Testing Costs
3.3. Reimbursement for ALK Testing
3.4. Detection of ALK Positives by Strategy
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Alberg, A.J.; Ford, J.G.; Samet, J.M. Epidemiology of lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 2007, 132, 29S–55S. [Google Scholar] [CrossRef] [PubMed]
- Rodrigo, D.; Martinez, P.; Felip, E. Personalizing therapy with targeted agents in non-small cell lung cancer. Oncotarget 2011, 2, 165–177. [Google Scholar]
- Tsao, M.S.; Hirsch, F.R.; Yatabe, Y. IASLC Atlas of ALK Testing in Lung Cancer; IASLC Publication: Aurora, CO, USA, 2013. [Google Scholar]
- Shaw, A.T.; Yeap, B.Y.; Solomon, B.J.; Riely, G.J.; Gainor, J.; Engelman, J.A.; Shapiro, G.I.; Costa, D.B.; Ou, S.H.; Butaney, M.; et al. Effect of crizotinib on overall survival in patients with advanced non-small-cell lung cancer harbouring ALK gene rearrangement: A retrospective analysis. Lancet Oncol. 2011, 12, 1004–1012. [Google Scholar] [CrossRef]
- Shaw, A.; Kim, D.W.; Nakagawa, K.; Seto, T.; Crinó, L.; Ahn, M.J.; de Pas, T.; Besse, B.; Solomon, B.J.; Blackhall, F.; et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N. Engl. J. Med. 2013, 368, 2385–2394. [Google Scholar] [CrossRef] [PubMed]
- Felip, E.; Kim, D.; Mehra, R.; Tan, D.S.W.; Chow, L.Q.; Camidge, D.R.; Vansteenkiste, J.F.; Sharma, S.; de Pas, T.; Riely, G.J.; et al. Efficacy and Safety of Ceritinib in Patients (pts) with Advanced Anaplastic Lymphoma Kinase (ALK)-rearranged (ALK+) Non-small Cell Lung Cancer (NSCLC): An Update of ASCEND-1. Abstract #1295P. In Proceedings of the European Society of Clinical Oncology (ESMO) 2014 Congress, Madrid, Spain, 26–30 September 2014.
- Shaw, A.T.; Mehra, R.; Tan, D.S.W.; Felip, E.; Chow, L.Q.; Camidge, D.R.; Vansteenkiste, J.; Sharma, S.; de Pas, T.; Riely, G.J.; et al. Evaluation of Ceritinib-treated Patients (pts) with Anaplastic Lymphoma Kinase rearranged (ALK+) Non-small Cell Lung Cancer (NSCLC) and Brain Metastases in the ASCEND-1 study. Abstract #1293P. In Proceedings of the European Society of Clinical Oncology (ESMO) 2014 Congress, Madrid, Spain, 26–30 September 2014.
- Stallard, J. Lung Cancer Patients Will Benefit from New Molecular Testing Guideline. Available online: https://www.mskcc.org/blog/lung-patients-will-benefit-new-molecular-testing-guideline (accessed on 3 November 2015).
- Lindeman, N.I.; Cagle, P.T.; Beasley, M.B.; Chitale, D.A.; Dacic, S.; Giaccone, G.; Jenkins, R.B.; Kwiatkowski, D.J.; Saldivar, J.S.; Squire, J.; et al. Molecular testing guideline for selection of lung cancer patients for EGFR and ALK tyrosine kinase inhibitors: Guideline from CAP, IASLC and AMP. J. Thorac. Oncol. 2013, 8, 823–859. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. Available online: http://www.nccn.org/professionals/physician_gls/recently_updated.asp (accessed on 3 November 2015).
- Kerr, K.M.; Bubendorf, L.; Edelman, M.J.; Marchetti, A.; Mok, T.; Novello, S.; O’Byrne, K.; Stahel, R.; Peters, S.; Felip, E.; et al. Second ESMO consensus conference on lung cancer: Pathology and molecular biomarkers for non-small-cell lung cancer. Ann. Oncol. 2014, 25, 1681–1690. [Google Scholar] [CrossRef] [PubMed]
- Abbott Receives FDA Approval for ALK Gene Test for Lung Cancer Therapy Selection. Available online: http://www.fiercebiotech.com/press-releases/abbott-receives-fda-approval-ALK-gene-test-lung-cancer-therapy-selectionn (accessed on 3 November 2015).
- VP 2000 Processor. Available online: https://www.abbottmolecular.com/us/products/vp-2000.html (accessed on 3 November 2015).
- Takeuchi, K.; Choi, Y.L.; Togashi, Y.; Soda, M.; Hatano, S.; Inamura, K.; Takada, S.; Ueno, T.; Yamashita, Y.; Satoh, Y.; et al. KIF5B-ALK, a novel fusion oncokinase identified by an immunohistochemistry-based diagnostic system for ALK-positive lung cancer. Clin. Cancer Res. 2009, 15, 3143–3149. [Google Scholar] [CrossRef] [PubMed]
- Togashi, Y.; Soda, M.; Sakata, S.; Sugawara, E.; Hatano, S.; Asaka, R.; Nakajima, T.; Mano, H.; Takeuchi, K. KLC1-ALK: A novel fusion in lung cancer identified using a formalin-fixed paraffinembedded tissue only. PLoS ONE 2012, 7, e31323. [Google Scholar] [CrossRef] [PubMed]
- RBRVS: Resource-Based Relative Value Scale. Available online: http://www.ama-assn.org/ama/pub/physician-resources/solutions-managing-your-practice/coding-billing-insurance/medicare/the-resource-based-relative-value-scale.page (accessed on 3 November 2015).
- Paik, J.H.; Choi, C.M.; Kim, H.; Jang, S.J.; Choe, G.; Kim, D.K.; Kim, H.J.; Yoon, H.; Lee, C.T.; Jheon, S.; et al. Clinicopathologic implication of ALK rearrangement in surgically resected lung cancer: A proposal of diagnostic algorithm for ALK-rearranged adenocarcinoma. Lung Cancer 2012, 76, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Cabillic, F.; Gros, A.; Dugay, F.; Begueret, H.; Mesturoux, L.; Chiforeanu, D.C.; Dufrenot, L.; Jauffret, V.; Dachary, D.; Corre, R.; et al. Parallel FISH and immunohistochemical studies of ALK status in 3244 non–small-cell lung cancers reveal major discordances. J. Thorac. Oncol. 2014, 9, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Ali, G.; Proietti, A.; Pelliccioni, S.; Niccoli, C.; Lupi, C.; Sensi, E.; Giannini, R.; Borrelli, N.; Menghi, M.; Chella, A.; et al. ALK Rearrangement in a large series of consecutive non-small cell lung cancers: Comparison between a new immunohistochemical approach and fluorescent in situ hybridization for the screening of patients eligible for crizotinib treatment. Arch. Pathol. Lab Med. 2014, 138, 1449–1458. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, H.C.; Fisher, K.E.; Hoffa, A.L.; Wang, J.; Saxe, D.; Siddiqui, M.T.; Cohen, C. The role of immunohistochemical analysis in the evaluation of EML4-ALK gene rearrangement in lung cancer. Appl. Immunohistochem. Mol. Morphol. 2015, 23, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Zhao, J.; Sun, K.; Wang, B.; Wang, L.; Chen, X.; Zheng, J.; You, Q.; Wang, X.; Ding, W. Accurate and economical detection of ALK positive lung adenocarcinoma with semiquantitative immunohistochemical screening. PLoS ONE 2014, 9, e92828. [Google Scholar] [CrossRef] [PubMed]
- Dolan, M.; Snover, D. Comparison of immunohistochemical and fluorescence in situ hybridization assessment of HER-2 status in routine practice. Am. J. Clin. Pathol. 2005, 123, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Physician Fee Schedule. Centers for Medicare & Medicaid Services. Available online: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/index.html?redirect=/physicianfeesched/ (accessed on 3 November 2015).
- Blackhall, F.H.; Peters, S.; Bubendorf, L.; Dafni, U.; Kerr, K.M.; Hager, H.; Soltermann, A.; O’Byrne, K.J.; Dooms, C.; Sejda, A.; et al. Prevalence and clinical outcomes for patients with ALK-positive resected stage I to III adenocarcinoma: Results from the European Thoracic Oncology Platform Lungscape Project. J. Clin. Oncol. 2014, 32, 2780–2787. [Google Scholar] [CrossRef] [PubMed]
- Rodig, S.J.; Mino-Kenudson, M.; Dacic, S.; Yeap, B.Y.; Shaw, A.; Barletta, J.A.; Stubbs, H.; Law, K.; Lindeman, N.; Mark, E.; et al. Unique clinicopathologic features characterize ALK-rearranged lung adenocarcinoma in the western population. Clin. Cancer Res. 2009, 15, 5216–5223. [Google Scholar] [CrossRef] [PubMed]
- Mino-Kenudson, M.; Chirieac, L.R.; Law, K.; Hornick, J.L.; Lindeman, N.; Mark, E.J.; Cohen, D.W.; Johnson, B.E.; Jänne, P.A.; Iafrate, A.J.; et al. A novel, highly sensitive antibody allows for the routine detection of ALK-rearranged lung adenocarcinomas by standard immunohistochemistry. Clin. Cancer Res. 2010, 16, 1561–1571. [Google Scholar] [CrossRef] [PubMed]
- Selinger, C.I.; Rogers, T.M.; Russell, P.A.; O’Toole, S.; Yip, P.; Wright, G.M.; Wainer, Z.; Horvath, L.G.; Boyer, M.; McCaughan, B.; et al. Testing for ALK rearrangement in lung adenocarcinoma: A multicenter comparison of immunohistochemistry and fluorescent in situ hybridization. Mod. Pathol. 2013, 26, 1545–1553. [Google Scholar] [CrossRef] [PubMed]
- Wynes, M.W.; Sholl, L.M.; Dietel, M.; Schuuring, E.; Tsao, M.S.; Yatabe, Y.; Tubbs, R.R.; Hirsch, F.R. An international interpretation study using the ALK IHC antibody D5F3 and a sensitive detection kit demonstrates high concordance between ALK IHC and ALK FISH and between evaluators. J. Thorac. Oncol. 2014, 9, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Parker, D.; Belaud-Rotureau, M.A. Micro-cost Analysis of ALK Rearrangement testing by FISH to determine eligibility for crizotinib therapy in NSCLC: Implications for cost effectiveness of testing and treatment. Clin. Med. Insights Oncol. 2014, 8, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.A.; Bubendorf, L.; Stahel, R.; Peters, S. Testing for anaplastic lymphoma kinase rearrangement to target crizotinib therapy; oncology, pathology and health economic perspectives. Expert Rev. Anticancer Ther. 2013, 13, 625–636. [Google Scholar] [CrossRef] [PubMed]
- Atherly, A.J.; Camidge, D.R. The cost-effectiveness of screening lung cancer patients for targeted drug sensitivity markers. Br. J. Cancer 2012, 106, 1100–1106. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doshi, S.; Ray, D.; Stein, K.; Zhang, J.; Koduru, P.; Fogt, F.; Wellman, A.; Wat, R.; Mathews, C. Economic Analysis of Alternative Strategies for Detection of ALK Rearrangements in Non Small Cell Lung Cancer. Diagnostics 2016, 6, 4. https://doi.org/10.3390/diagnostics6010004
Doshi S, Ray D, Stein K, Zhang J, Koduru P, Fogt F, Wellman A, Wat R, Mathews C. Economic Analysis of Alternative Strategies for Detection of ALK Rearrangements in Non Small Cell Lung Cancer. Diagnostics. 2016; 6(1):4. https://doi.org/10.3390/diagnostics6010004
Chicago/Turabian StyleDoshi, Shivang, David Ray, Karen Stein, Jie Zhang, Prasad Koduru, Franz Fogt, Axel Wellman, Ricky Wat, and Charles Mathews. 2016. "Economic Analysis of Alternative Strategies for Detection of ALK Rearrangements in Non Small Cell Lung Cancer" Diagnostics 6, no. 1: 4. https://doi.org/10.3390/diagnostics6010004