
Long-Term Comparison of Two- and Three-Dimensional Computed Tomography Analyses of Cranial Bone Defects in Severe Parietal Thinning
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Computed Tomography Imaging
2.2. Application of Quantification Methods for Image Analyses
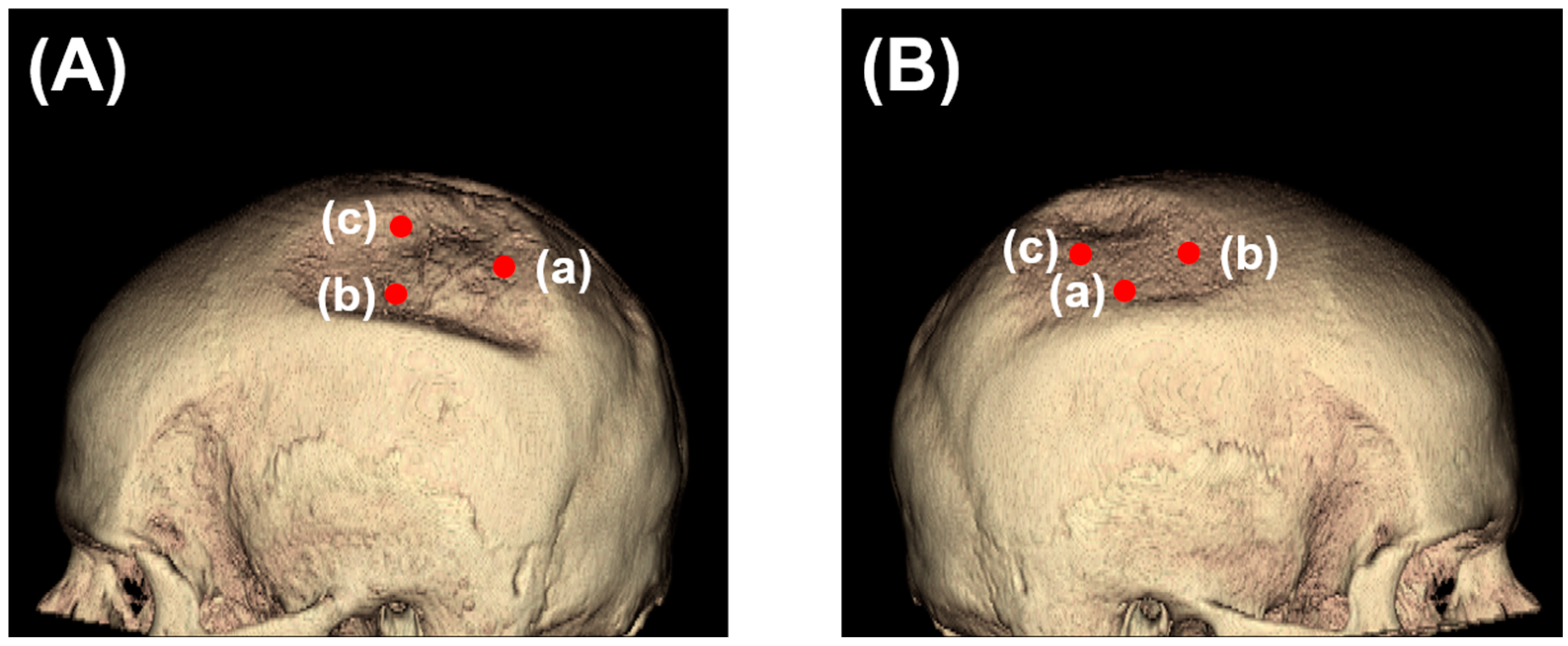
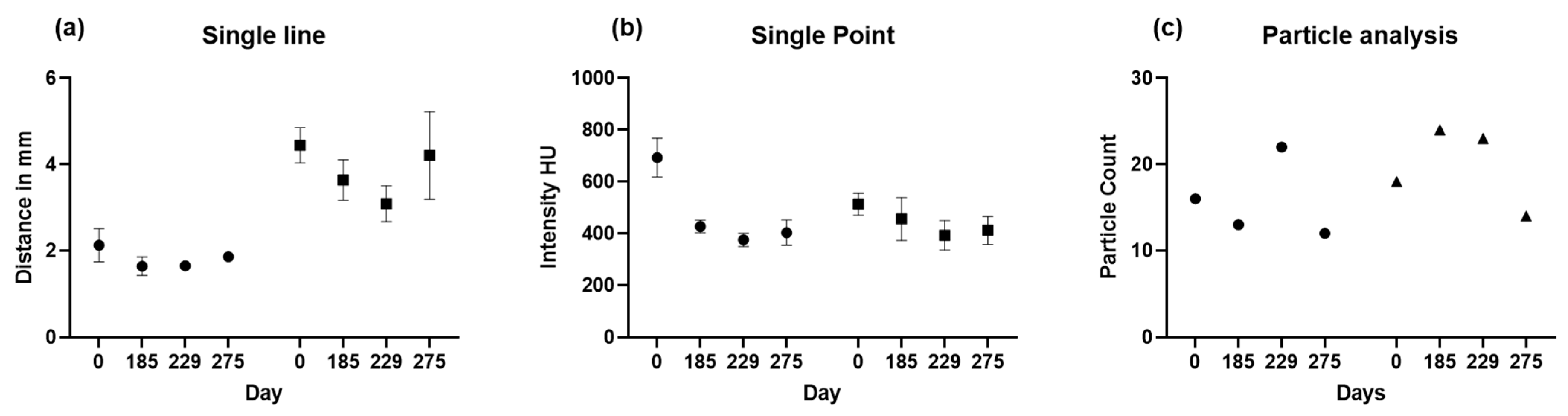
2.2.1. Two-Dimensional (2D) Measurement Methods
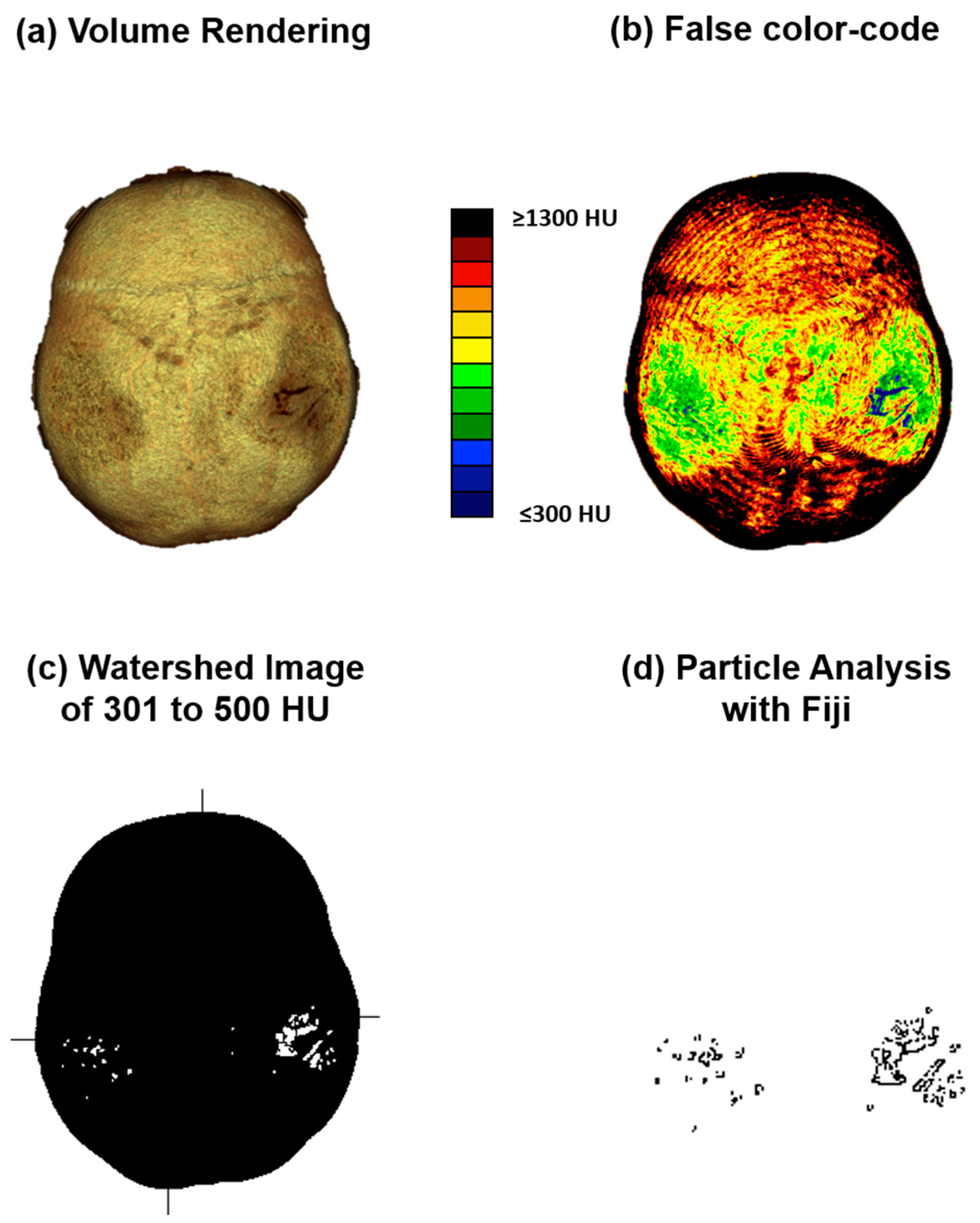
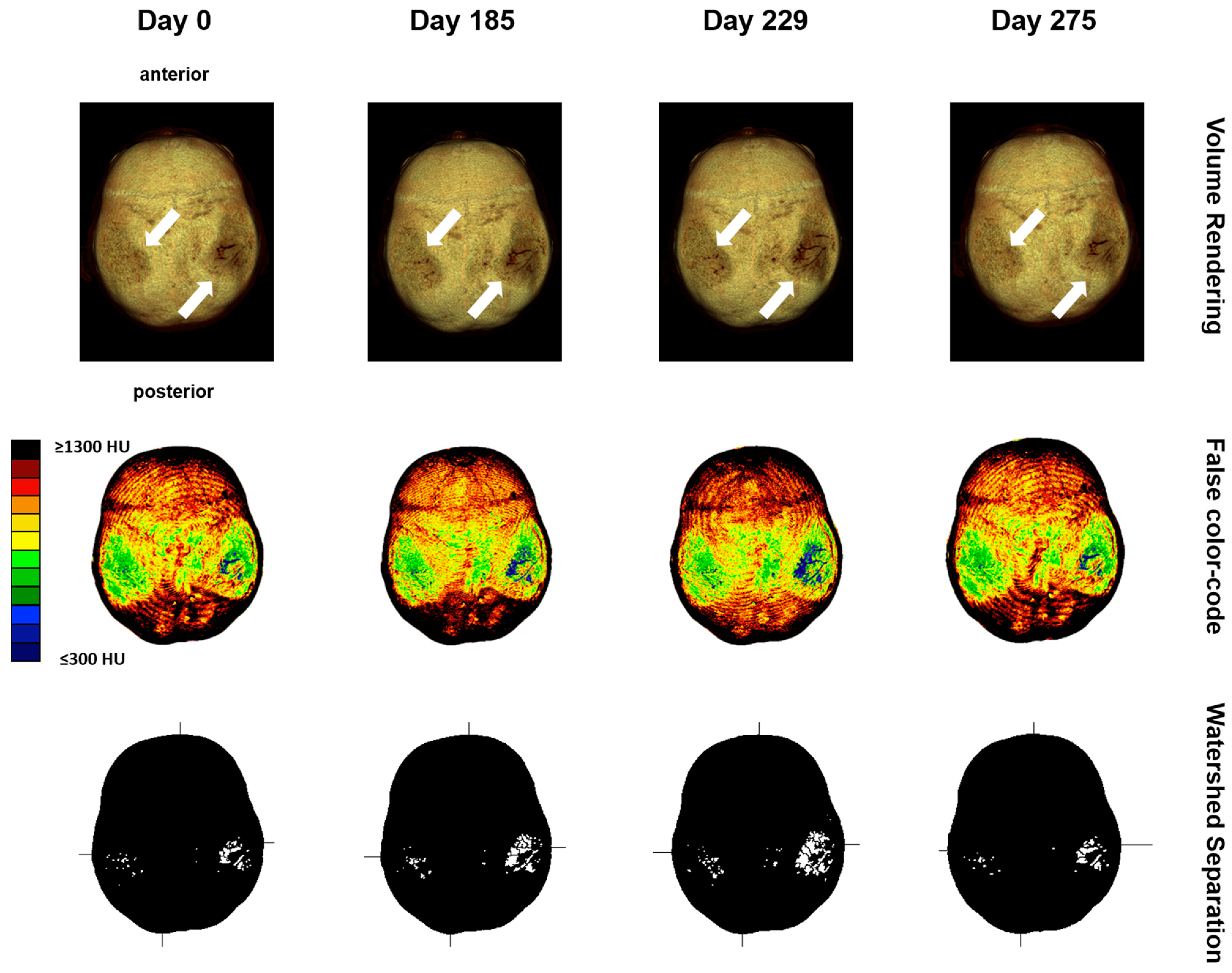
2.2.2. Computed Tomography Osteoabsorptiometry
2.2.3. Analysis of Densitogram Patterns
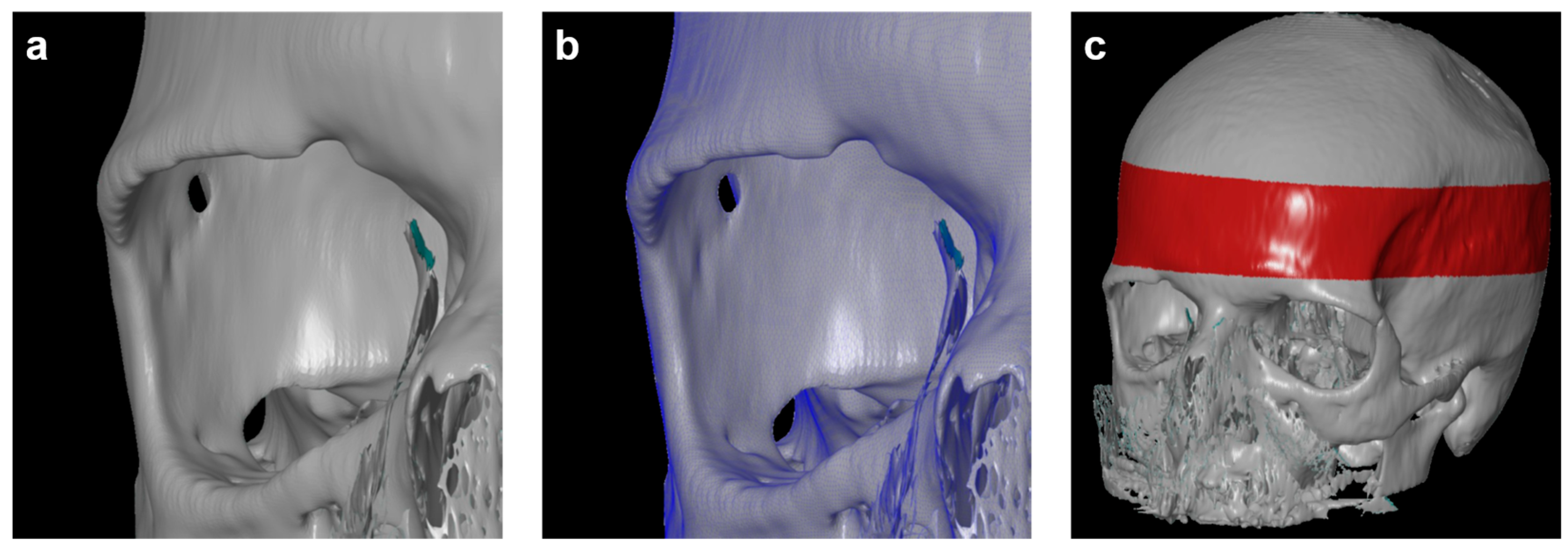
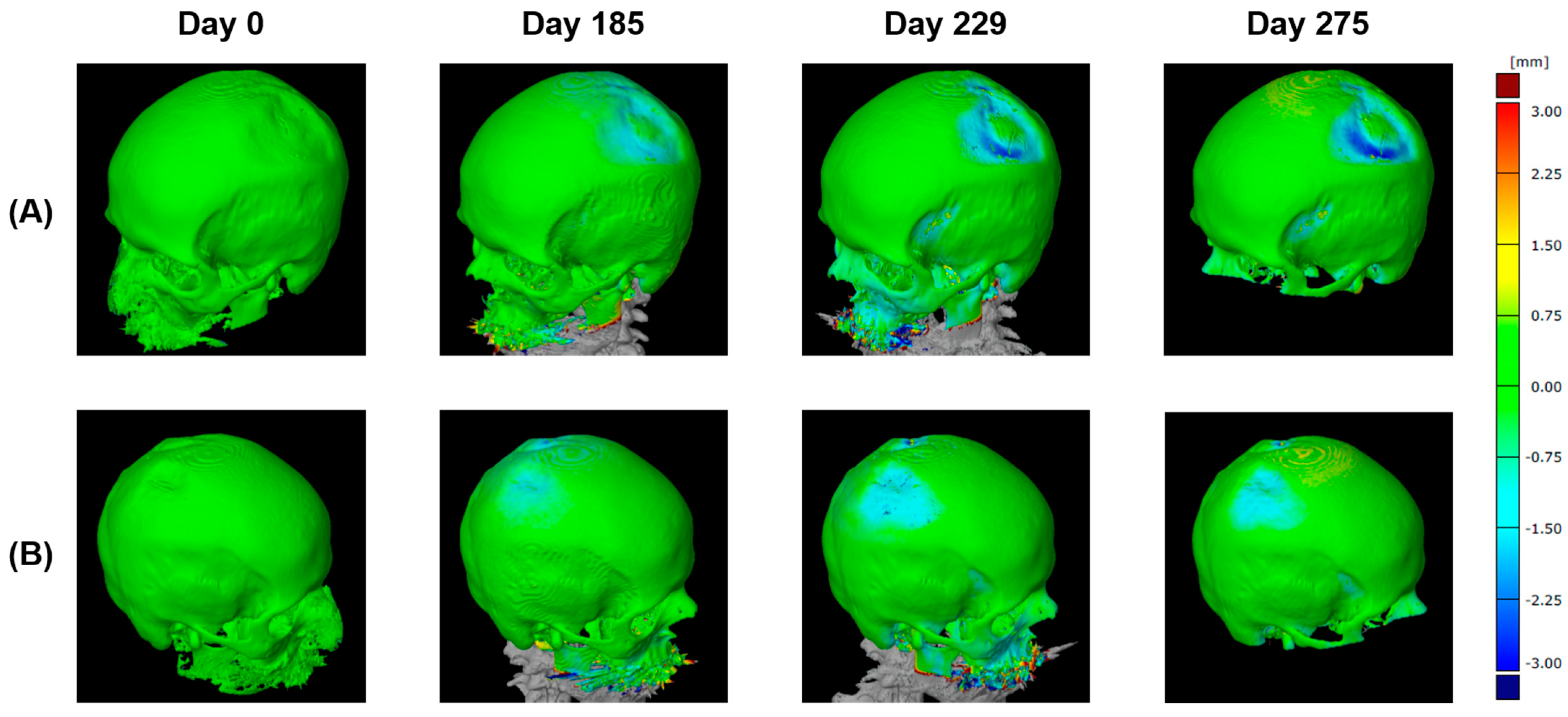
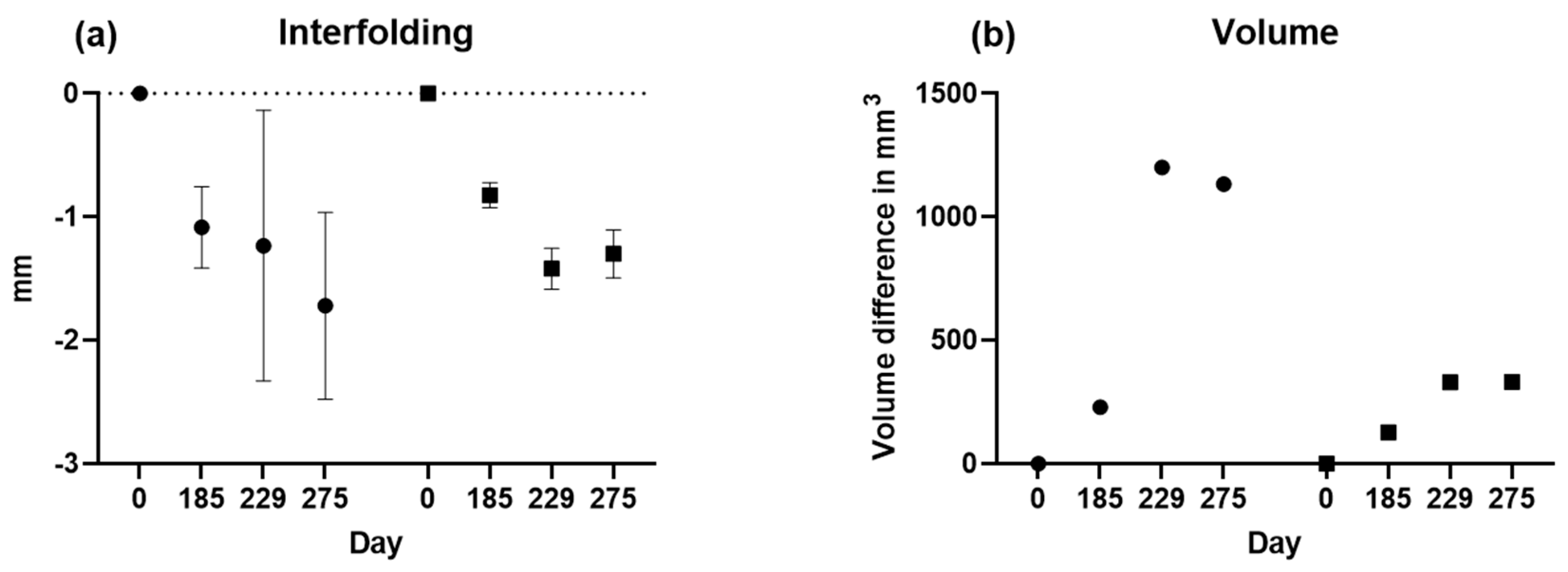
2.2.4. Three-Dimensional (3D) Measurement Method
2.3. Statistical Analyses
3. Results
3.1. Patient’s Assessment and Follow-Up with Multimodal Diagnostics
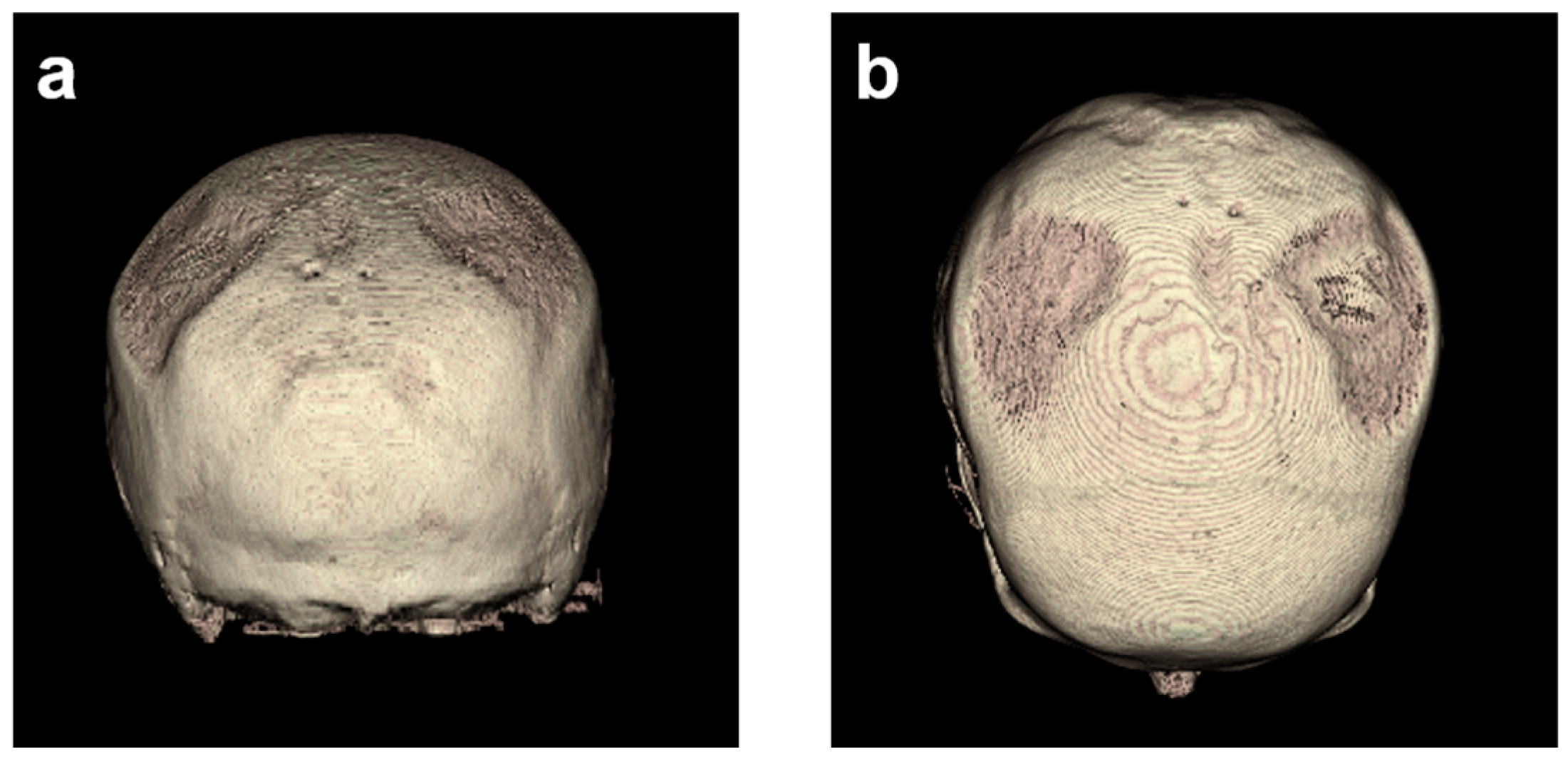
3.2. Descriptive Imaging Reports before and after 3D Reconstruction
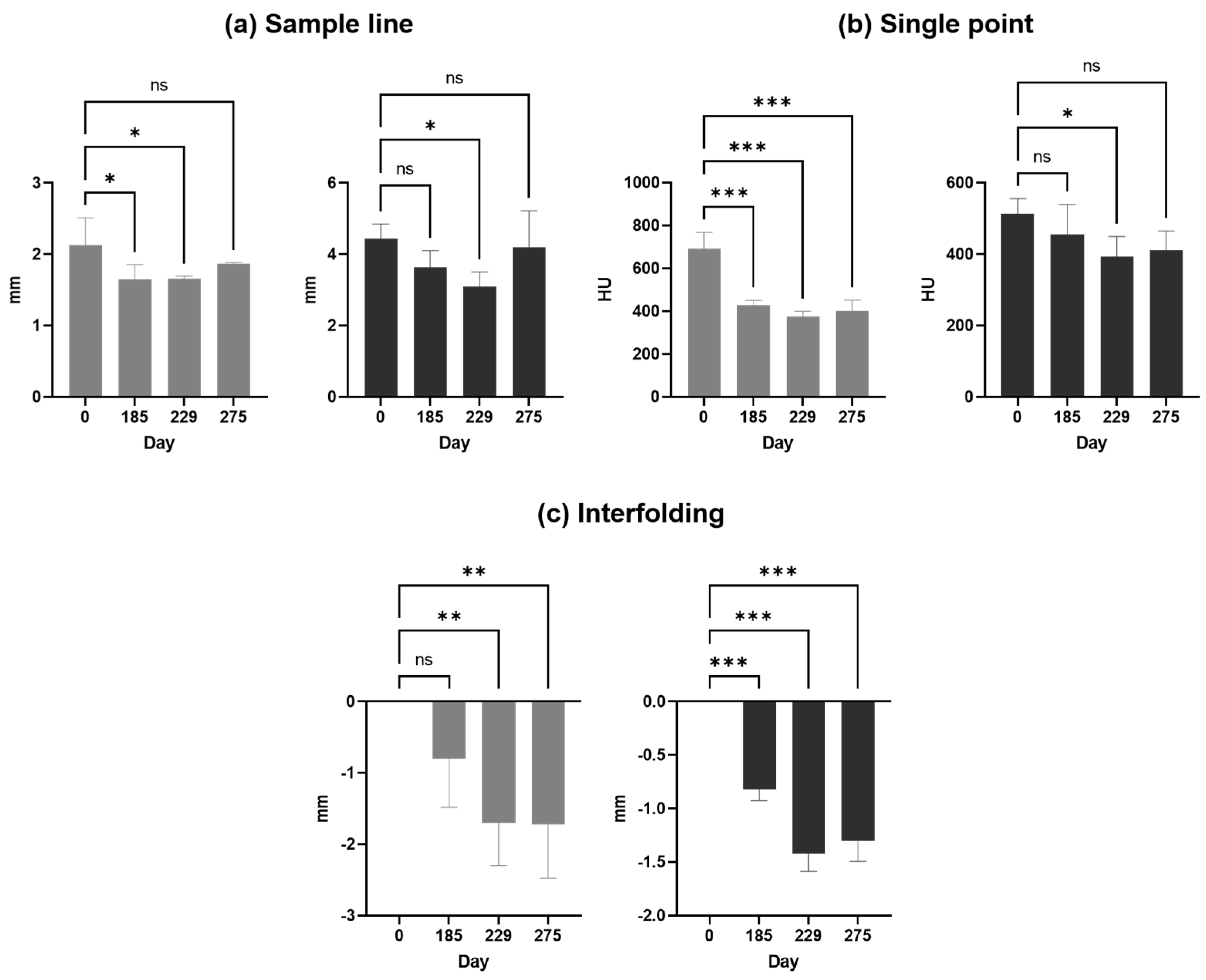
3.3. Two-Dimensional (2D) Measurements of Biparietal Thinning
3.4. Three-Dimensional (3D) Measurements of Biparietal Thinning
3.5. Comparisons of Changes in Bone Loss over Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bruyn, G.W.; Bots, G.T.A.M. Biparietal osteodystrophy. Clin. Neurol. Neurosurg. 1978, 80, 125–148. [Google Scholar] [CrossRef] [PubMed]
- Cvetković, D.; Bracanović, D.; Djonić, D.; Živković, V.; Djurić, M.; Nikolić, S. Biparietal osteodystrophy: Macroscopic appearance, computed tomography imaging and microarchitectural analysis. Leg. Med. 2022, 55, 102025. [Google Scholar] [CrossRef] [PubMed]
- Cederlund, C.G.; Andrén, L.; Olivecrona, H. Progressive bilateral thinning of the parietal bones. Skelet. Radiol. 1982, 8, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Camp, J.D.; Nash, L.A. Developmental Thinness of the Parietal Bones. Radiology 1944, 42, 42–47. [Google Scholar] [CrossRef]
- Barnes, E. Developmental Defects of the Axial Skeleton in Paleopathology; University Press of Colorado: Louisville, CO, USA, 1994. [Google Scholar]
- Poor, G.; Donath, J.; Fornet, B.; Cooper, C. Epidemiology of Paget’s disease in Europe: The prevalence is decreasing. J. Bone Miner. Res. 2006, 21, 1545–1549. [Google Scholar] [CrossRef] [PubMed]
- von Rokitansky, C. Handbuch der Allgemeinen Pathologischen Anatomie; Braumüller & Seidel: Vienna, Austria, 1842. [Google Scholar]
- Greig, D.M. On symmetrical thinness of the parietal bones. Edinb. Med. J. 1926, 33, 645. [Google Scholar] [PubMed]
- Grainger, R.G.; Allison, D.J. Grainger & Allison’s Diagnostic Radiology: A Textbook of Medical Imaging; Churchill Livingstone: London, UK, 1997; Volume 1. [Google Scholar]
- Nashold, B.S., Jr.; Netsky, M.G. Foramina, Fenestrae, and Thinness of Parietal Bone*. J. Neuropathol. Exp. Neurol. 1959, 18, 432–441. [Google Scholar] [CrossRef]
- De Stefano, G.F.; Hauser, G.; Guidotti, A.; Rossi, S.; Russo, E.G.; Gualandi, P.B. Reflections on interobserver differences in scoring non-metric cranial traits (with practical examples). J. Hum. Evol. 1984, 13, 349–355. [Google Scholar] [CrossRef]
- Tsutsumi, S.; Yasumoto, Y.; Ito, M. Idiopathic calvarial thinning. Neurol. Med. Chir. 2008, 48, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, N.; Hadi, M.S.; Lillard, J.C.; Passias, P.G.; Linzey, J.R.; Saadeh, Y.S.; LaBagnara, M.; Park, P. Alternatives to DEXA for the assessment of bone density: A systematic review of the literature and future recommendations. J. Neurosurg. Spine 2023, 38, 436–445. [Google Scholar] [CrossRef]
- Martel, D.; Monga, A.; Chang, G. Osteoporosis Imaging. Radiol. Clin. N. Am. 2022, 60, 537–545. [Google Scholar] [CrossRef]
- Poilliot, A.; Doyle, T.; Kurosawa, D.; Toranelli, M.; Zhang, M.; Zwirner, J.; Müller-Gerbl, M.; Hammer, N. Computed tomography osteoabsorptiometry-based investigation on subchondral bone plate alterations in sacroiliac joint dysfunction. Sci. Rep. 2021, 11, 8652. [Google Scholar] [CrossRef]
- Müller-Gerbl, M. The Subchondral Bone Plate; Springer: Berlin/Heidelberg, Germany, 1998. [Google Scholar] [CrossRef]
- Hoechel, S.; Wirz, D.; Müller-Gerbl, M. Density and strength distribution in the human subchondral bone plate of the patella. Int. Orthop. 2012, 36, 1827–1834. [Google Scholar] [CrossRef] [PubMed]
- Serrano, N.; Kissling, M.; Krafft, H.; Link, K.; Ullrich, O.; Buck, F.M.; Mathews, S.; Serowy, S.; Gascho, D.; Grüninger, P.; et al. CT-based and morphological comparison of glenoid inclination and version angles and mineralisation distribution in human body donors. BMC Musculoskelet. Disord. 2021, 22, 849. [Google Scholar] [CrossRef] [PubMed]
- Gay, M.H.; Born, G.; Mehrkens, A.; Wittig, H.; Müller-Gerbl, M. Computed tomography osteoabsorptiometry for imaging of degenerative disc disease. N. Am. Spine Soc. J. 2022, 9, 100102. [Google Scholar] [CrossRef] [PubMed]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Stefaniak, J.; Kubicka, A.M.; Wawrzyniak, A.; Romanowski, L.; Lubiatowski, P. Reliability of humeral head measurements performed using two- and three-dimensional computed tomography in patients with shoulder instability. Int. Orthop. 2020, 44, 2049–2056. [Google Scholar] [CrossRef]
- Pfeil, A.; Lehmann, G.; Lange, U. Update DVO-Leitlinie 2017 “Prophylaxe, Diagnostik und Therapie der Osteoporose bei postmenopausalen Frauen und Männern”. Z. Für Rheumatol. 2018, 77, 759–763. [Google Scholar] [CrossRef] [PubMed]
- Aiba, H.; Nakazato, T.; Matsuo, H.; Kimura, H.; Saito, S.; Sakai, T.; Murakami, H.; Kawai, J.; Kawasaki, S.; Imamura, Y. Bone Metastases from Gastric Cancer Resembling Paget’s Disease: A Case Report. J. Clin. Med. 2022, 11, 7306. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| p-Values Based on One-Way ANOVA | ||||||
|---|---|---|---|---|---|---|
| Hemisphere | Name | Units | 0 vs. 185 | 0 vs. 229 | 0 vs. 275 | 229 vs. 275 |
| Right | Single line | mm | 0.1559 ns | 0.0300 * | 0.6581 ns | 0.0614 ns |
| Single point | HU | 0.2840 ns | 0,0420 * | 0,0755 ns | 0.7166 ns | |
| Particle analysis | Counts | n.a. | n.a. | n.a. | n.a. | |
| Interfolding | mm | <0.0001 *** | <0.0001 *** | <0.0001 *** | 0.3148ns | |
| Volume | mm | n.a. | n.a. | n.a. | n.a. | |
| Left | Single line | mm | 0.0263 * | 0.0287 * | 0.1747 ns | 0.2745 ns |
| Single point | HU | 0.0001 *** | <0.0001 *** | <0.0001 *** | 0.4904 ns | |
| Particle analysis | Counts | n.a. | n.a. | n.a. | n.a. | |
| Interfolding | mm | 0.1356 ns | 0.0075 *** | 0.0072 *** | 0.9786 ns | |
| Volume | mm | n.a. | n.a. | n.a. | n.a. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pallua, J.D.; Pallua, A.K.; Streif, W.; Spiegl, H.; Halder, C.; Arora, R.; Schirmer, M. Long-Term Comparison of Two- and Three-Dimensional Computed Tomography Analyses of Cranial Bone Defects in Severe Parietal Thinning. Diagnostics 2024, 14, 446. https://doi.org/10.3390/diagnostics14040446
Pallua JD, Pallua AK, Streif W, Spiegl H, Halder C, Arora R, Schirmer M. Long-Term Comparison of Two- and Three-Dimensional Computed Tomography Analyses of Cranial Bone Defects in Severe Parietal Thinning. Diagnostics. 2024; 14(4):446. https://doi.org/10.3390/diagnostics14040446
Chicago/Turabian StylePallua, Johannes Dominikus, Anton Kasper Pallua, Werner Streif, Harald Spiegl, Clemens Halder, Rohit Arora, and Michael Schirmer. 2024. "Long-Term Comparison of Two- and Three-Dimensional Computed Tomography Analyses of Cranial Bone Defects in Severe Parietal Thinning" Diagnostics 14, no. 4: 446. https://doi.org/10.3390/diagnostics14040446