
Unusual Rapid Growth of Primary Splenic Diffuse Large B-Cell Lymphoma with Extensive Necrosis


1
Division of Internal Medicine, Yuan-Lin Christian Hospital, 456 Ju-Guang Road, Yuan-Lin City 510012, Taiwan
2
Division of Radiology, Changhua Christian Hospital, 135 Nan-Xiao Street, Changhua City 50006, Taiwan
3
Division of Gastroenterology, Changhua and Yuan-Lin Christian Hospital, 135 Nanxiao Street, Changhua City 50006, Taiwan
4
Department of Hospitality Management, MingDao University, 3 Lane 138 Tai-An 2nd Street, Changhua City 50006, Taiwan
*
Author to whom correspondence should be addressed.
Diagnostics 2023, 13(1), 35; https://doi.org/10.3390/diagnostics13010035
Submission received: 5 November 2022
/
Revised: 10 December 2022
/
Accepted: 17 December 2022
/
Published: 22 December 2022
(This article belongs to the Special Issue Advances in the Diagnosis and Treatment of Hepatogastroenterology)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:The primary splenic lymphoma is extremely uncommon with an incidence rate of <1% of all the lymphomas under the strict criteria for diagnosis expounded by Das Gupta et al. Clinical presentations of nonspecific symptoms are weight loss, weakness, fever, and left upper quadrant pain or discomfort due to enlarged spleen. Abdominal ultrasound and CT are the most widely used imaging modality for the assessment of lymphoma. The imaged features of splenic lymphoma are nonspecific; typical lymphoma presents as a diffusely enlarged spleen. The abdominal CT scan in our case showed a large cystic splenic mass measuring 14 cm without enhancement after contrast medium. Lymphoma is often described as an aggressive tumor because its rapid doubling time can quickly increase the size of a tumor. In our case, the tumor grew to more than 100 times its original size in 4 months. So, we present this unusual rapid growth of primary splenic lymphoma.
A 36-year-old man working as a nurse in our hospital presented with left upper quadrant (LUQ) pain, which had persisted for 1 week. He denied any past systemic disease, but the patient had undergone an abdominal ultrasound during a routine examination 4 months earlier, which had revealed a 3 cm hypoechoic splenic nodule (Figure 1). At that time, the treating physician had suggested a follow-up examination 6 months later.
Physical examination revealed a large palpable mass with local tenderness over the LUQ. The patient’s white blood cell count was 17,000/μL, with segment neutrophil 83% and lymphocyte 10%, and platelet: 475,000/mL. An abdominal computed tomographic (CT) scan revealed a large cystic splenic mass measuring 14 cm without enhancement after contrast medium (Figure 2). The mass was pushing the left kidney inward and down (Figure 3). During the initial diagnosis, a pancreatic pseudocyst involving the spleen was suspected, and the patient received an emergency splenectomy because of the rapid growth of the mass and severe pain.
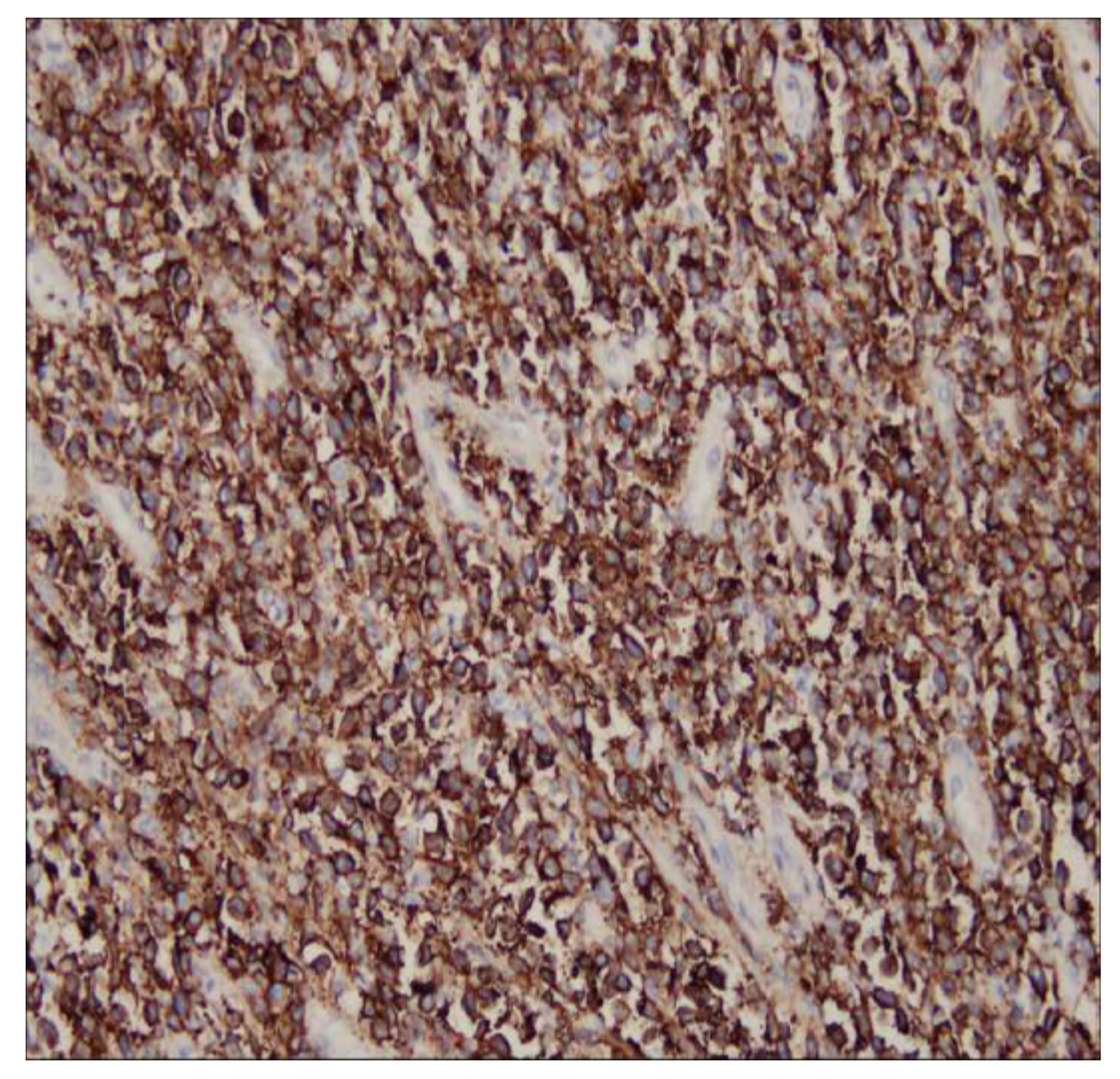
The splenectomy operation removed a large solid splenic tumor. The histology exhibited a diffuse proliferation of a monotonous population of large neoplastic lymphoid cells and extensive necrosis (Figure 4). Immunohistochemical testing revealed a positive result for CD20, CD79a, BCL6, and BCL2, and a Ki-67 index greater than 90% (Figure 5). Immunohistochemical testing was also negative for CD3 and CD10. The patient was discharged without complications 1 week later. A subsequent bone marrow examination and positron emission tomography–computed tomography scan were negative. A diagnosis of primary splenic diffuse large B-cell lymphoma was recorded. The patient received CHOP regimen chemotherapy. The patient was asymptomatic upon follow-up examination and exhibited no recurrence 6 months after chemotherapy.
Lymphoma is the most common malignancy of the spleen, but primary lymphoma of the spleen is very rare with an incidence rate of <1% under the strict criteria for diagnosis expounded by Das Gupta et al. According to their criteria, diagnosis of primary splenic lymphoma should only be made when the disease is confined to the spleen but may also involve the hilar lymph nodes with no recurrence of the disease after splenectomy [1,2,3]. In our case, the patient presented with a large splenic cystic tumor that did not affect other organs, and there was no occurrence after splenectomy and chemotherapy.
Clinical presentations of nonspecific symptoms are weight loss, weakness, fever, and left upper quadrant pain or discomfort due to an enlarged spleen. CT is the most widely used imaging modality for the assessment of lymphoma. The imaged features of splenic lymphoma are nonspecific; typical lymphoma presents as a diffusely enlarged spleen. Focal lesions appear as low-density areas in the imaging with little or no enhancement following injection of intravenous contrast medium. Ahmann classified lymphomatous involvement of the spleen into the following four categories: (1) homogeneous enlargement without masses, (2) miliary masses, (3) 2–10 cm masses, and (4) a large solitary mass [4,5,6,7]. Significant necrosis may also occur with a large tumor but extensive necrosis like the necrosis observed in our case is extremely rare.
Lymphoma is often described as an aggressive tumor because its rapid doubling time can quickly increase the size of a tumor [7,8,9,10]. In our case, the tumor grew to more than 100 times its original size in 4 months, and the doubling time was only 17 days. Fortunately, the tumor in our case responded well to splenectomy with chemotherapy.
Author Contributions
Conceptualization, Y.-Y.C.; writing—original draft preparation, Y.-Y.C., Y.-R.C. and H.-K.W.; writing—review and editing, Y.-Y.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
The patient informed consent was obtained before the paper was written.
Data Availability Statement
We did not report any data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Das Gupta, T.; Goombes, B.; Brosfeld, R.D. Primary malignant neoplasms of the spleen. Surg. Gynecol. Obstet. 1969, 120, 947–960. [Google Scholar]
- Ahmann, D.L.; Kiely, J.M.; Harrison, E.G.; Payne, W.S. Malignant lymphoma of the spleen. A review of 49 cases in which the diagnosis was made at splenectomy. Cancer 1966, 19, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Ingle, S.B.; Hinge Ingle, C.R. Primary splenic lymphoma: Current diagnostic trends. World J. Clin. Cases 2016, 4, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Kamaya, A.; Weinstein, S.; Desser, T.S. Multiple lesions of the spleen: Differential diagnosis of cystic and solid lesions. Semin. Ultrasound CT MR 2006, 27, 389–403. [Google Scholar] [CrossRef] [PubMed]
- Yocum, B.P.; Hwang, M.; Mesa, H.; Collins, K. Differential Diagnosis of Cystic Lesions of the Spleen: A Review of Clinical, Imaging and Pathological Findings. Int. J. Surg. Pathol. 2022. [CrossRef] [PubMed]
- Taibi, S.; Jabi, R.; Kradi, Y.; Miry, N.; Bouziane, M. Diffuse Large B-Cell Lymphoma Revealed by Splenic Abscess: A Case Report. Cureus 2021, 13, e18771. [Google Scholar] [CrossRef] [PubMed]
- Kehoe, J.; Straus, D.J. Primary lymphoma of the spleen: Clinical features and outcome after splenectomy. Cancer 1988, 62, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- Bairey, O.; Shvidel, L.; Perry, C.; Dann, E.J.; Ruchlemer, R.; Tadmor, T.; Goldschmidt, N. Characteristics of primary splenic diffuse large B-cell lymphoma and role of splenectomy in improving survival. Cancer 2015, 121, 2909–2916. [Google Scholar] [CrossRef] [PubMed]
- Isaacson, P.G. Primary splenic lymphoma. Cancer Surv. 1997, 30, 193–212. [Google Scholar] [PubMed]
- Carboni, F.; Covello, R.; Valle, M. Primary Splenic Lymphoma. J. Gastrointest. Surg. 2021, 25, 2423–2425. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Abdominal ultrasound revealed a 3 cm hypoechoic splenic nodule during a routine examination 4 months earlier.
Figure 1.
Abdominal ultrasound revealed a 3 cm hypoechoic splenic nodule during a routine examination 4 months earlier.

Figure 2.
Abdominal CT scan revealed a large cystic splenic mass measuring 14 cm without enhancement.
Figure 2.
Abdominal CT scan revealed a large cystic splenic mass measuring 14 cm without enhancement.

Figure 3.
Abdominal CT scan showed the mass was pushing the left kidney inward and down.
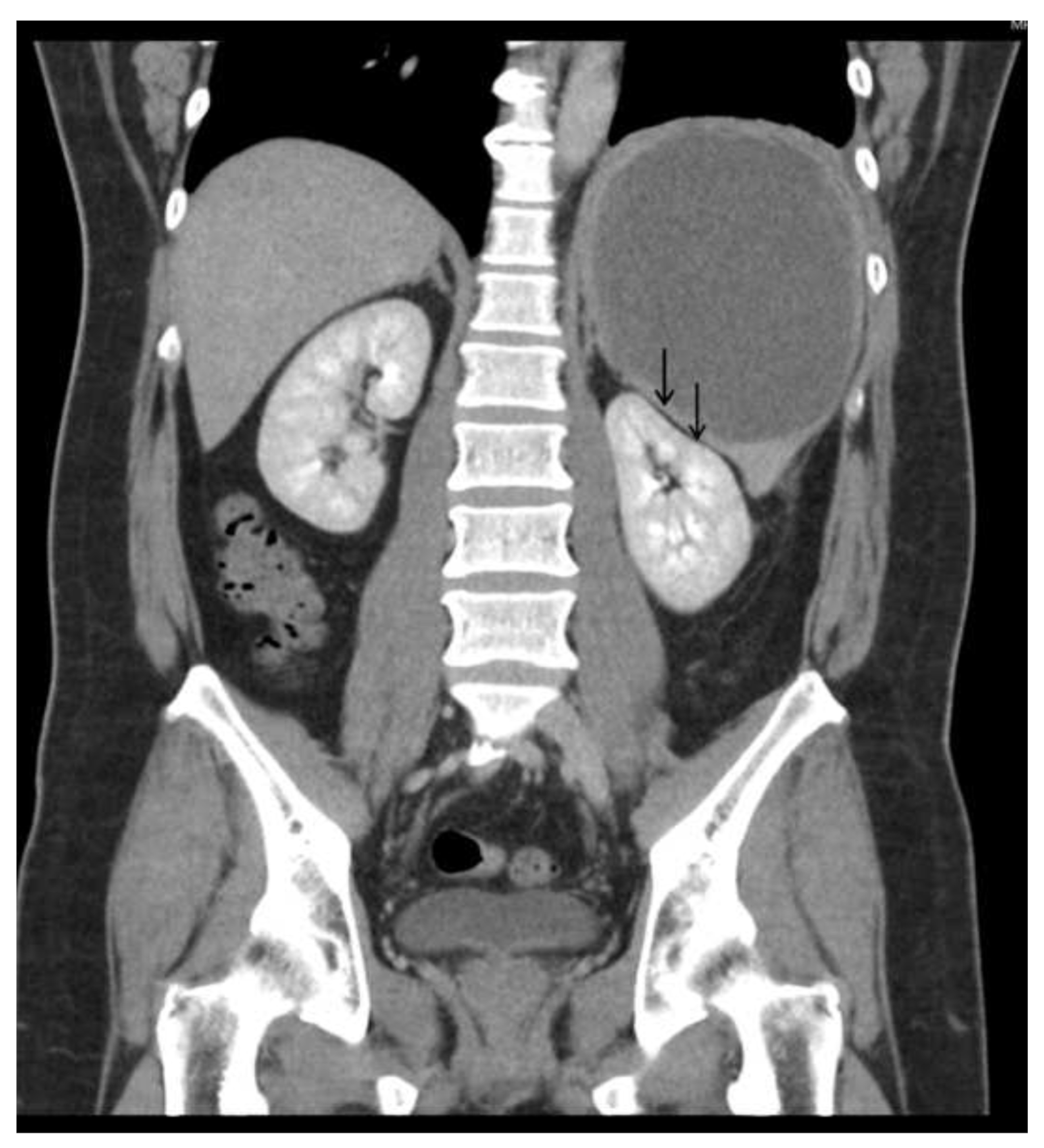
Figure 4.
The histology revealed a diffuse proliferation of a monotonous population of large neoplastic lymphoid cells and extensive necrosis.
Figure 4.
The histology revealed a diffuse proliferation of a monotonous population of large neoplastic lymphoid cells and extensive necrosis.
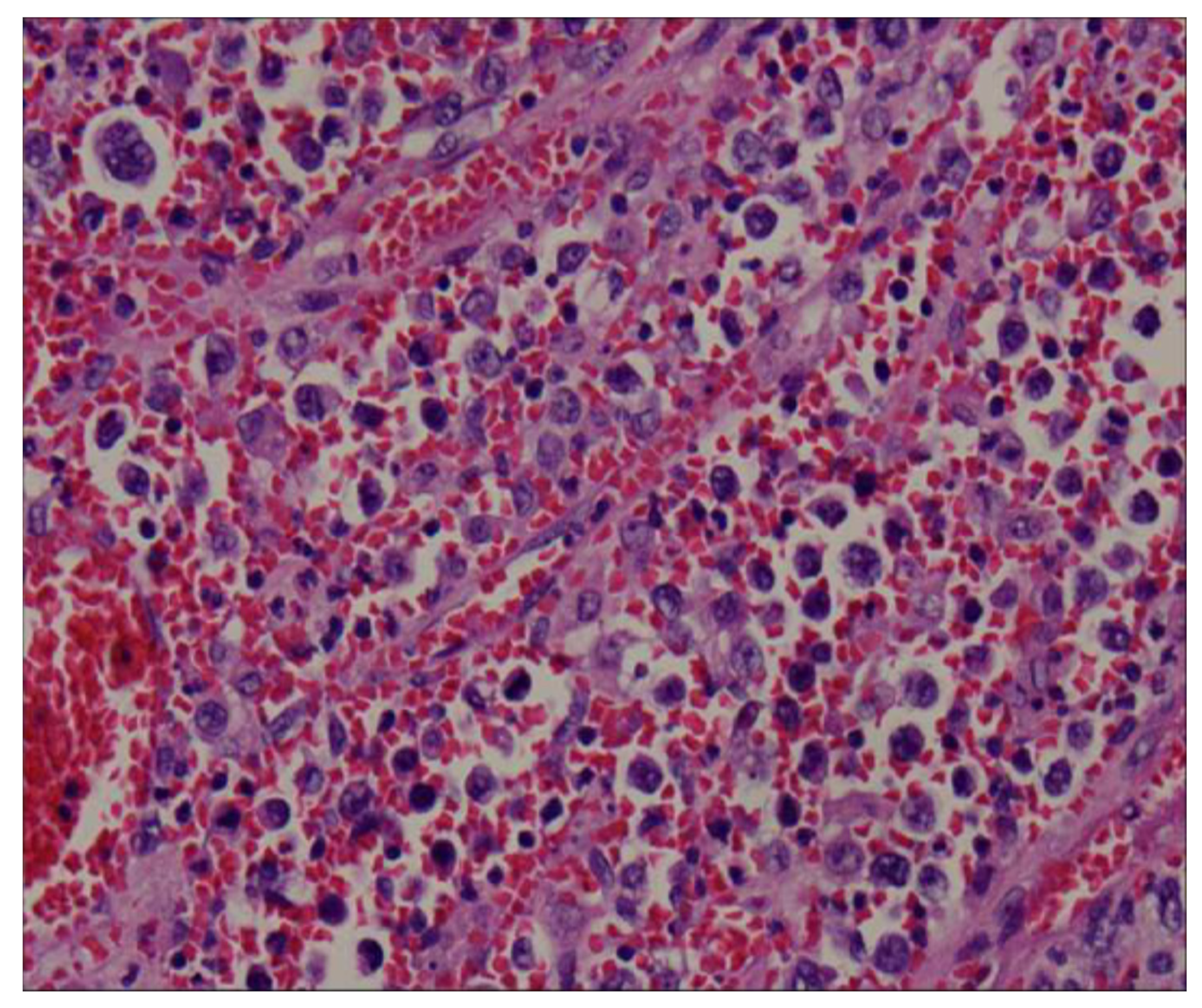
Figure 5.
Immunohistochemical testing was positive for CD20.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Chen, Y.-R.; Wu, H.-K.; Chen, Y.-Y. Unusual Rapid Growth of Primary Splenic Diffuse Large B-Cell Lymphoma with Extensive Necrosis. Diagnostics 2023, 13, 35. https://doi.org/10.3390/diagnostics13010035
AMA Style
Chen Y-R, Wu H-K, Chen Y-Y. Unusual Rapid Growth of Primary Splenic Diffuse Large B-Cell Lymphoma with Extensive Necrosis. Diagnostics. 2023; 13(1):35. https://doi.org/10.3390/diagnostics13010035
Chicago/Turabian StyleChen, Yue-Ren, Hwa-Koon Wu, and Yang-Yuan Chen. 2023. "Unusual Rapid Growth of Primary Splenic Diffuse Large B-Cell Lymphoma with Extensive Necrosis" Diagnostics 13, no. 1: 35. https://doi.org/10.3390/diagnostics13010035
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.