
Cause of Death in Charred Bodies: Reflections and Operational Insights Based on a Large Cases Study

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
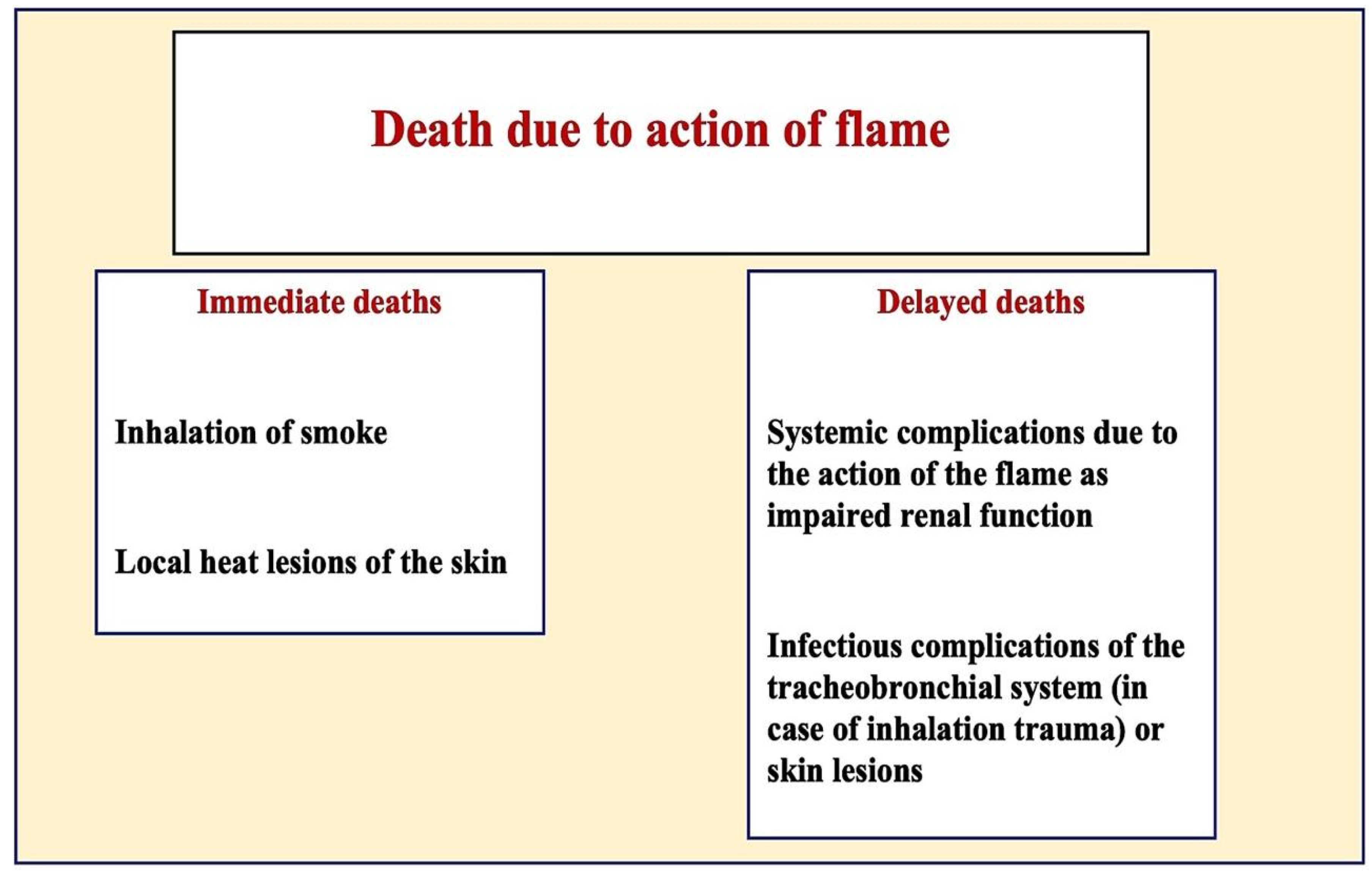
- Cyanide toxicity—depending on the material burnt, cyanide toxicity may develop very rapidly, so elevated COHb (carboxyhemoglobin) concentrations may not be detected;
- Deflagration—death may occur by respiratory arrest due to laryngeal spasm, bronchial spasm, vagus reflexes, or heat shock on inhalation;
- Oxygen deprivation—deprivation of oxygen at the source of the fire can lead to death;
- Heat shock—a redistribution of circulating blood volume due to the heat exposure of the skin;
- Heat rigor—impairment of respiratory function due to sudden thermal rigidity in the chest.
2. Materials and Methods
- Inspection;
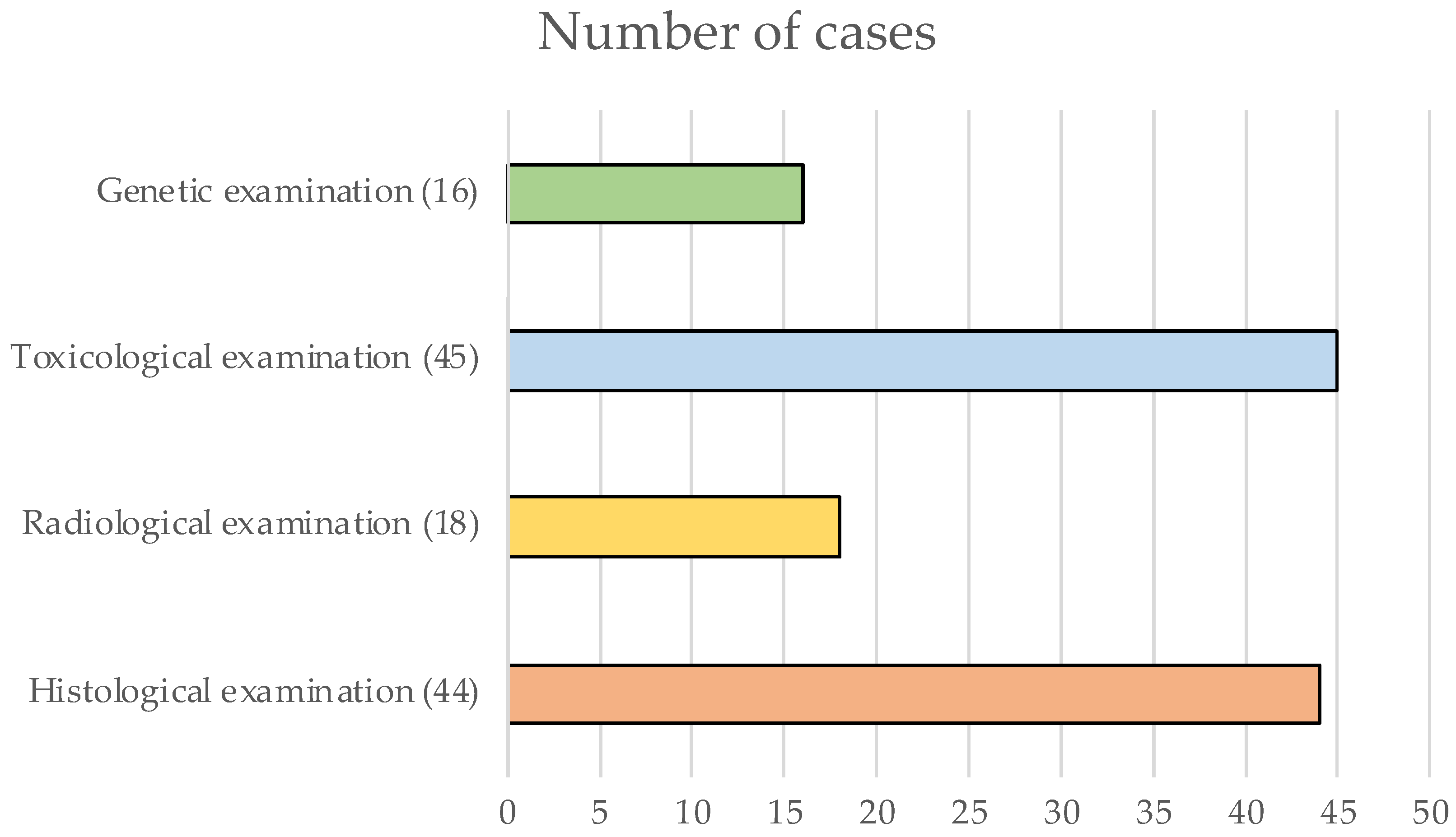
- Radiological examination;
- Autopsy examination or external examination;
- Histological or immunohistochemical examinations;
- Toxicological examinations;
- Genetic examination.
2.1. Inspection
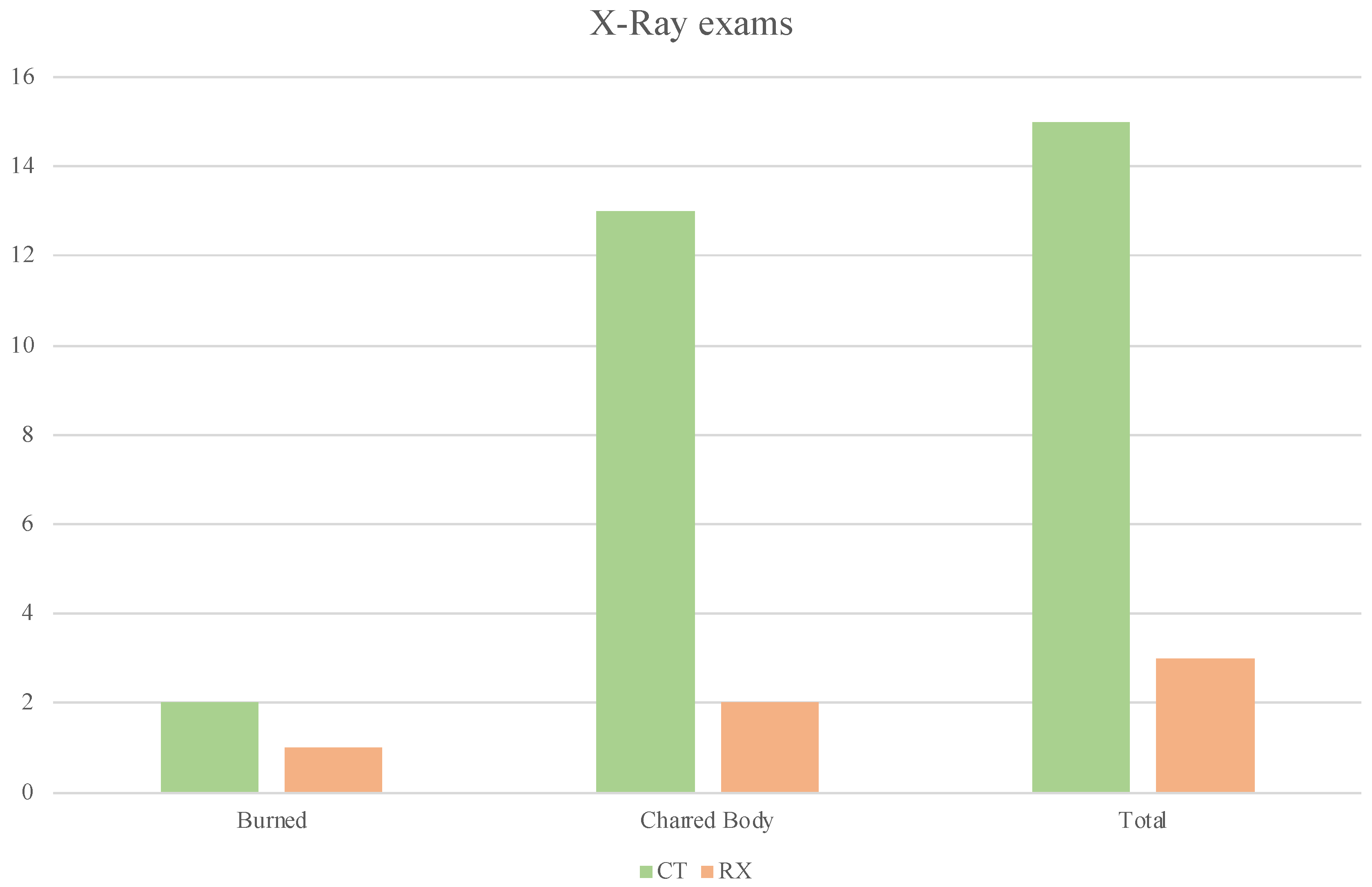
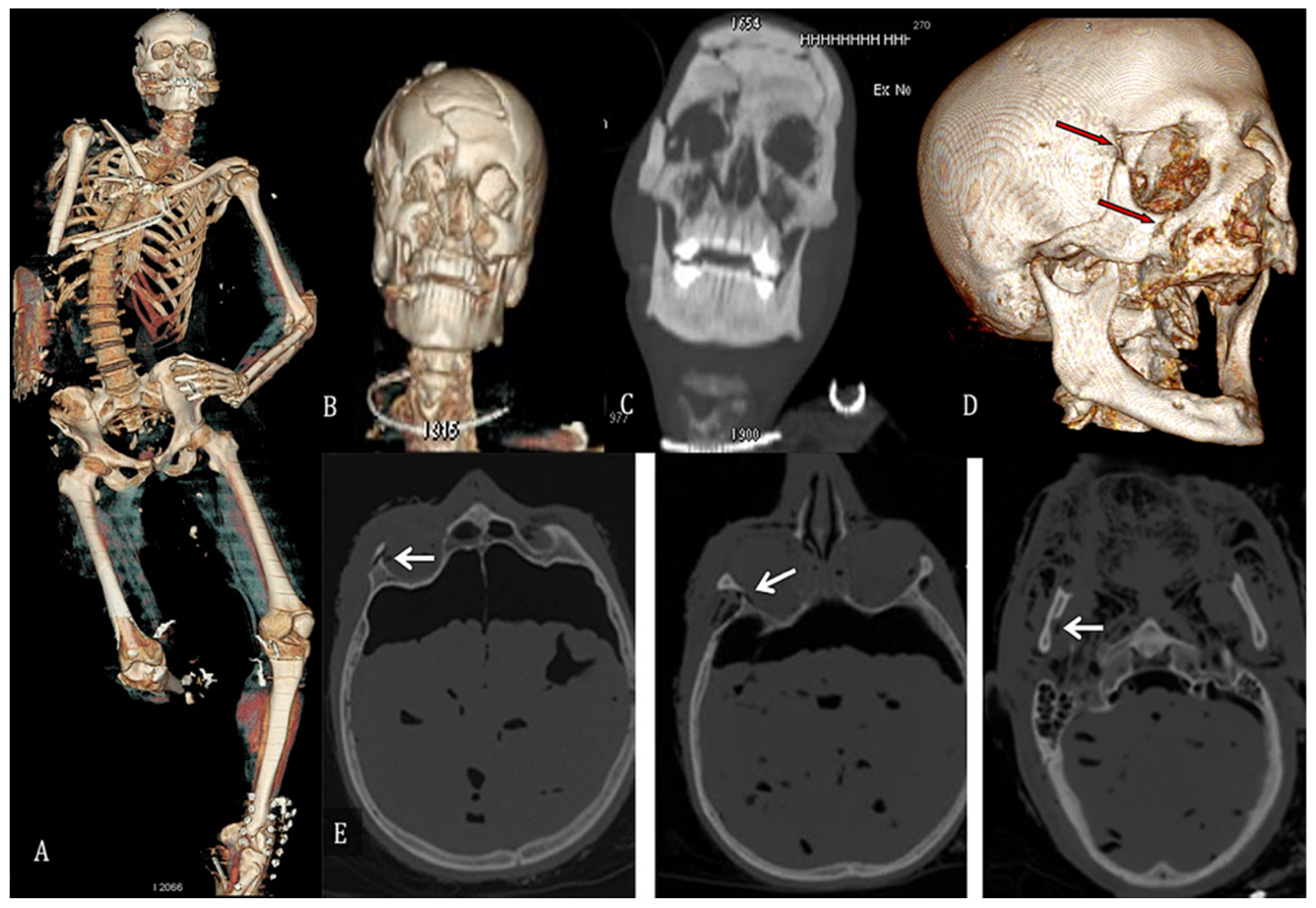
2.2. Radiological Investigations
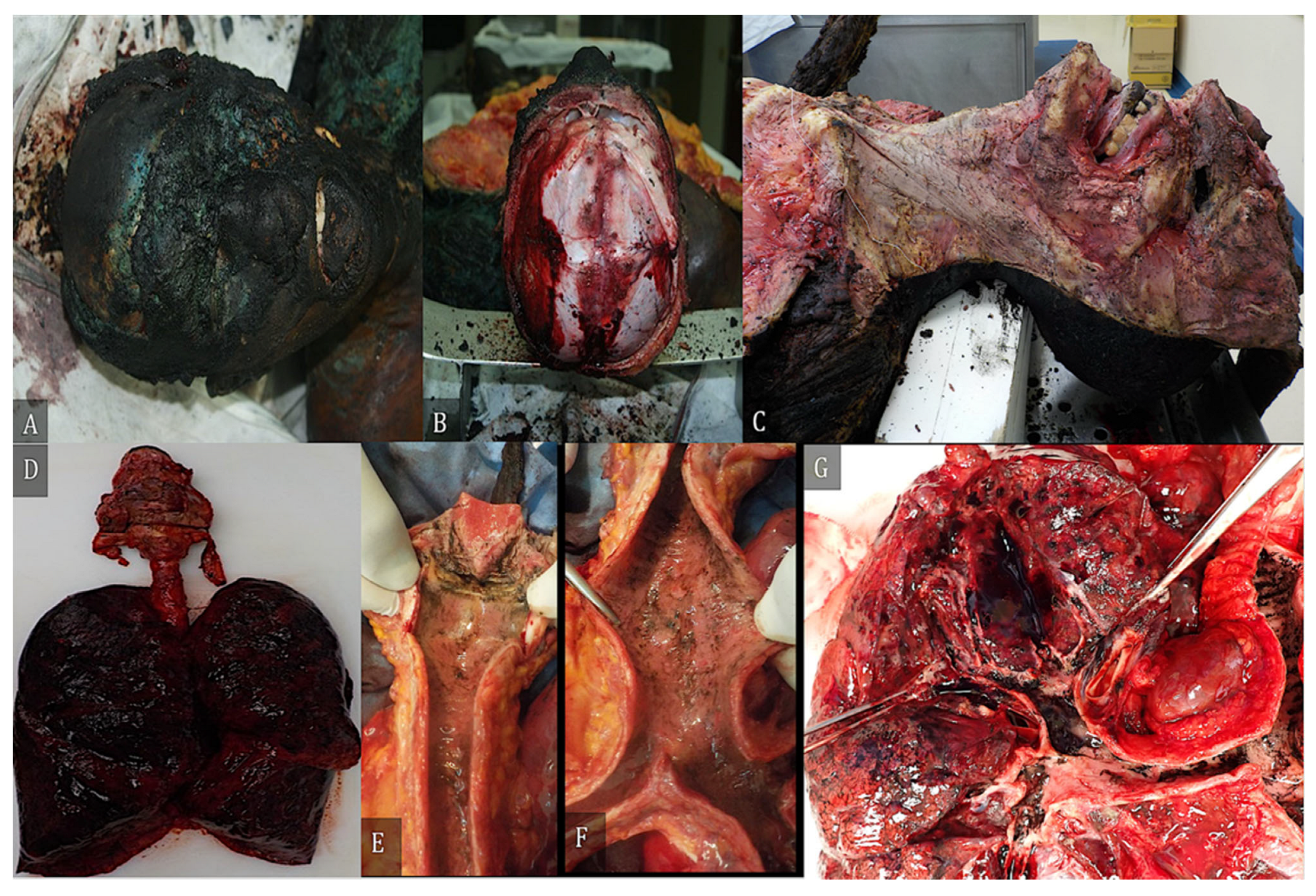
2.3. Autopsy Examination or External Examination
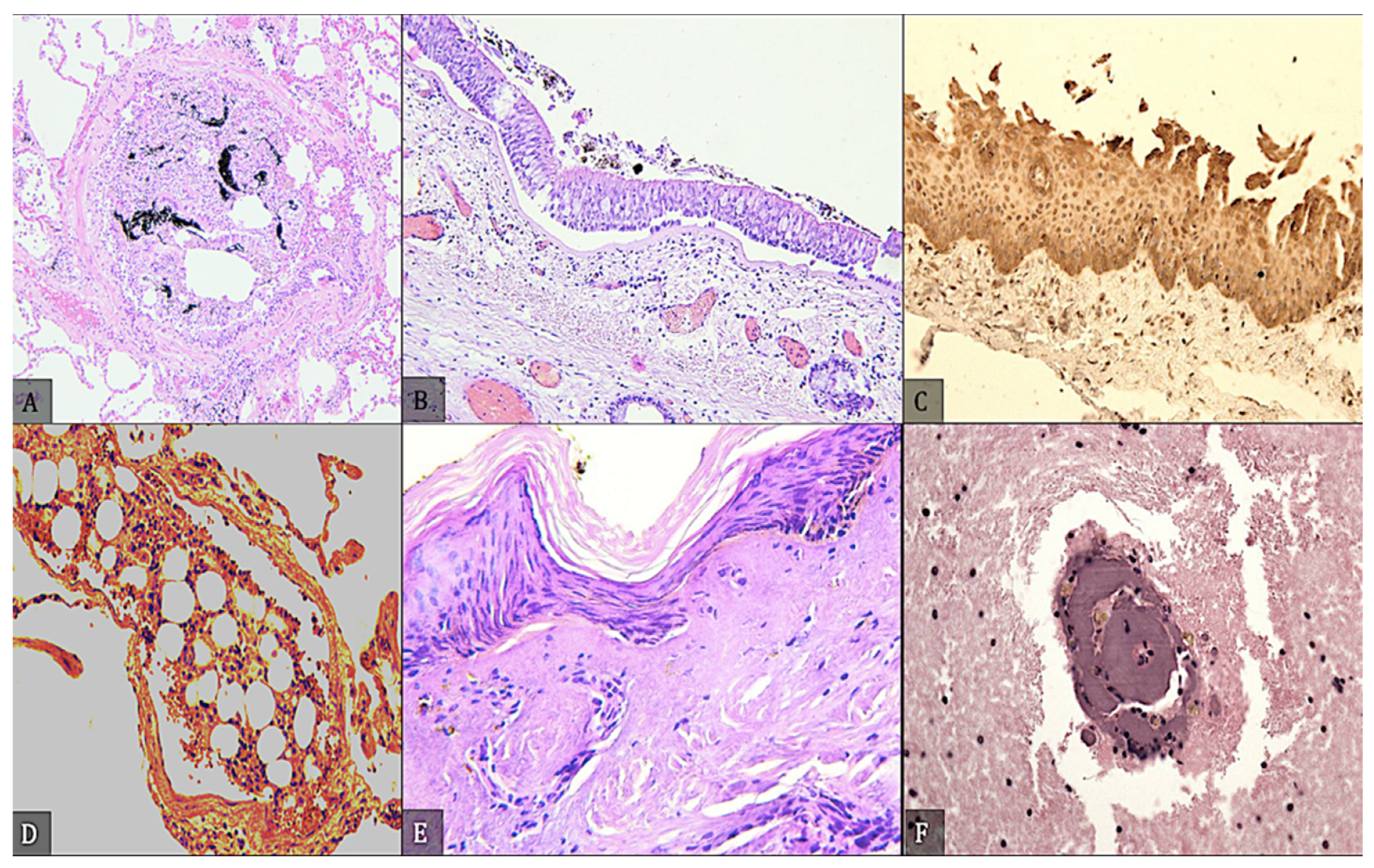
2.4. Histological and Immunohistochemical Examination
2.5. Toxicological Examination
2.6. Genetic Investigation
2.7. Diagnosis of Death
3. Results
4. Discussion
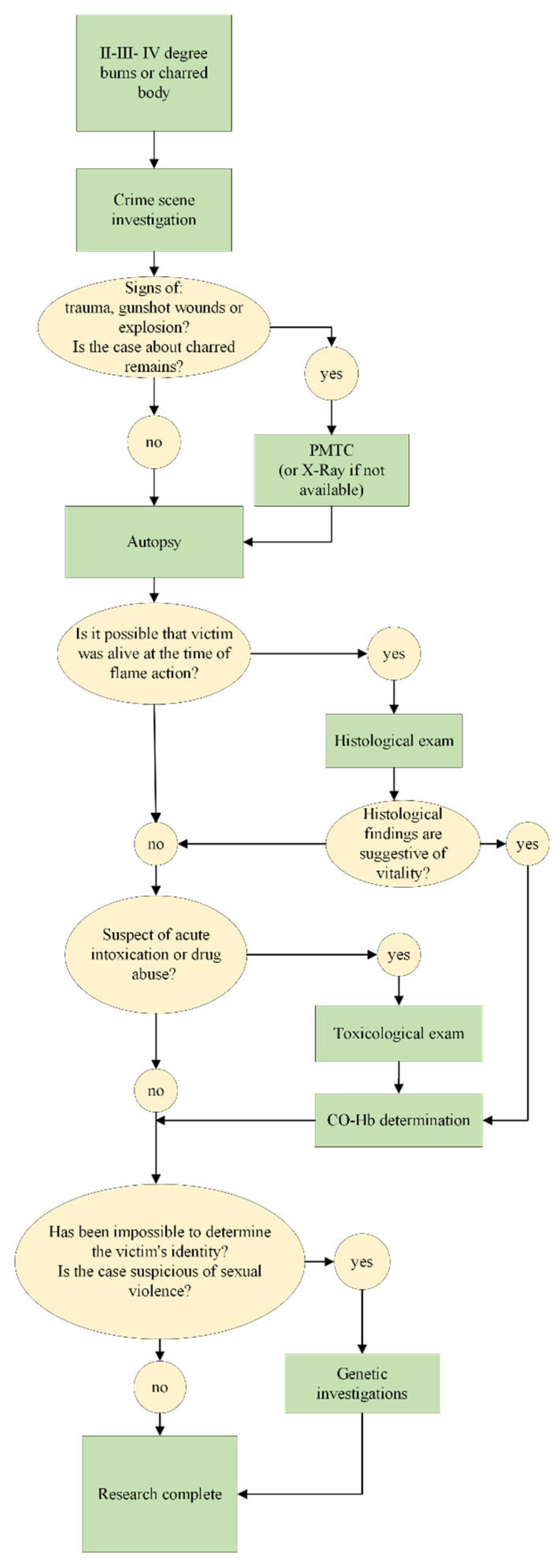
5. Conclusions
- Crime scene investigation is always appropriate;
- Radiologic examination (PMTC or radiography) should be performed in all cases where gunshot wounds, explosions, trauma, charred remains, or the bodies of children are suspected;
- An autopsy should always be indicated from second-degree injuries;
- Histology and immunohistochemistry are always required when there is doubt about post-fatal charring;
- Toxicological analysis is imperative to prove or confirm that the person was alive at the time of the charring, or when the previous steps have led to the suspicion of acute intoxication. Long hospitalizations may result in unusable results;
- Genetic analysis should be performed when the previous steps fail to identify the body or when violence is suspected.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moritz, A.R. Studies of thermal injury III. The pathology and pathogenesis of cutaneous burns. An experimental study. Am. J. Pathol. 1947, 23, 915–941. [Google Scholar] [PubMed]
- Moritz, A.R.; Henriques, F.C. Studies of thermal injury II. The relative importance of time and surface temperature in the causation of cutaneous burns. Am. J. Pathol. 1947, 23, 695–720. [Google Scholar] [PubMed]
- Moritz, A.R.; Henriques, F.C.; Dutra, F.R.; Weisiger, J.R. Studies of thermal injury IV. An exploration of the casualty-producing attributes of conflagrations; local and systemic effects of general cutaneous exposure to excessive circumambient (air) and circumradiant heat of varying duration and intensity. Am. J. Pathol. 1947, 43, 466–488. [Google Scholar]
- Richards, N.F. Fire investigation—Destruction of corpses. Med. Sci. Law 1977, 17, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Bohnert, M.; Rost, T.; Pollak, S. The degree of destruction of human bodies in relation to the duration of the fire. Forensic Sci. Int. 1998, 95, 11–21. [Google Scholar] [CrossRef]
- Taylor, C.R.; Rudbeck, L. (Eds.) Immunohistochemical Staining Methods, 6th ed.; Agilent Dako: Santa Clara, CA, USA, 2013; pp. 36–44. [Google Scholar]
- Madea, B. (Ed.) Handbook of Forensic Medicine; Wiley Blackwell: Hoboken, NJ, USA, 2014; pp. 422–467. [Google Scholar]
- Cusack, D.; Ferrara, S.D.; Keller, E.; Ludes, B.; Mangin, P.; Väli, M.; Vieira, N. European Council of Legal Medicine (ECLM) principles for on-site forensic and medico-legal scene and corpse investigation. Int. J. Leg. Med. 2017, 131, 1119–1122. [Google Scholar] [CrossRef]
- Cittadini, F.; Polacco, M.; D’Alessio, P.; Tartaglione, T.; De Giorgio, F.; Oliva, A.; Zobel, B.; Pascali, V.L. Virtual autopsy with multidetector computed tomography of three cases of charred bodies. Med. Sci. Law 2010, 50, 211–216. [Google Scholar] [CrossRef]
- Coty, J.B.; Nedelcu, C.; Yahya, S.; Dupont, V.; Rougé-Maillart, C.; Verschoore, M.; Ridereau Zins, C.; Aubé, C. Burned bodies: Post-mortem computed tomography, an essential tool for modern forensic medicine. Insights Imaging 2018, 9, 731–743. [Google Scholar] [CrossRef]
- Brogdon’s Forensic Radiology, 2nd ed.; Thali, M.J.; Viner, M.D.; Brogdon, B.G. (Eds.) CRC Press: Boca Raton, FL, USA, 2011; pp. 215–216. [Google Scholar]
- Sano, R.; Hirawasa, S.; Kobayashi, S.; Shimada, T.; Awata, S.; Takei, H.; Otake, H.; Takahashi, K.; Takahashi, Y.; Kominato, Y. Use of postmortem computed tomography to reveal an intraoral gunshot injury in a charred body. Leg. Med. 2011, 13, 286–288. [Google Scholar] [CrossRef]
- Levy, A.D.; Harcke, H.T.; Getz, J.M.; Mallak, C.T. Multidetector Computed Tomography Findings in Deaths with Severe Burns. Am. J. Forensic Med. Pathol. 2009, 30, 137–141. [Google Scholar] [CrossRef]
- Jackowski, C.; Aghayev, E.; Sonnenschein, M.; Dirnhofer, R.; Thali, M.J. Maximum intensity projection of cranial computed tomography data for dental identification. Int. J. Leg. Med. 2006, 120, 165–167. [Google Scholar] [CrossRef] [PubMed]
- Jackowski, C.; Lussi, A.; Classens, M.; Kilchoer, T.; Bolliger, S.; Aghayev, E.; Criste, A.; Dirnhofer, R.; Thali, M.J. Extended CT scale overcomes restoration caused streak artifacts for dental identification in CT–3D color encoded automatic discrimination of dental restorations. J. Comput. Assist. Tomogr. 2006, 30, 510–513. [Google Scholar] [CrossRef] [PubMed]
- Jackowski, C.; Wyss, M.; Persson, A.; Classens, M.; Thali, M.J.; Lussi, A. Ultra-high-resolution dual-source CT for forensic dental visualization-discrimination of ceramic and composite fillings. Int. J. Leg. Med. 2008, 122, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Pfaeffli, M.; Vock, P.; Dirnhofer, R.; Braun, M.; Bolliger, S.A.; Thali, M.J. Post-mortem radiological CT identification based on classical ante-mortem X-ray examinations. Forensic Sci. Int. 2007, 171, 111–117. [Google Scholar] [CrossRef]
- Sidler, M.; Jackowski, C.; Dirnhofer, R.; Vock, P.; Thali, M.J. Use of multislice computed tomography in disaster victim identification—Advantages and limitations. Forensic Sci. Int. 2007, 169, 118–128. [Google Scholar] [CrossRef]
- Kawasumi, Y.; Usui, A.; Hosokai, Y.; Sato, M.; Funayama, M. Heat haematoma: Post-mortem computed tomography findings. Clin. Radiol. 2013, 68, e95–e97. [Google Scholar] [CrossRef]
- Peterson, G.F.; Clark, S.C.; National Association of Medical Examiners. Forensic autopsy performance standards. Am. J. Forensic Med. Pathol. 2006, 27, 200–225. [Google Scholar] [CrossRef]
- Thali, M.J.; Markwalder, T.; Jackowski, C.; Sonnenschein, M.; Dirnhofer, R. Dental CT imaging as a screening tool for dental profiling: Advantages and limitations. J. Forensic Sci. 2006, 51, 113–119. [Google Scholar] [CrossRef]
- Thali, M.J.; Yen, K.; Plattner, T.; Schweitzer, W.; Vock, P.; Ozdoba, C.; Dirnhofer, R. Charred body: Virtual autopsy with multi-slice computed tomography and magnetic resonance imaging. J. Forensic Sci. 2014, 47, 1326–1331. [Google Scholar] [CrossRef]
- Bohnert, M.; Hejna, P. Tongue protrusion in burned bodies. Int. J. Leg. Med. 2016, 130, 1253–1255. [Google Scholar] [CrossRef]
- Turillazzi, E.; Riezzo, I.; Neri, M.; Pomara, C.; Cecchi, R.; Fineschi, V. The diagnosis of fatal pulmonary fat embolism using quantitative morphometry and confocal laser scanning microscopy. Pathol. Res. Pract. 2008, 204, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Fineschi, V.; D’Errico, S.; Neri, M.; Panarese, F.; Ricci, P.A.; Turillazzi, E. Heat stroke in an incubator: An immunohistochemical study in a fatal case. Int. J. Leg. Med. 2005, 119, 94–97. [Google Scholar] [CrossRef] [PubMed]
- Pircher, R.; Pollak, S.; Vogt, S.; Epting, T.; Kramer, L.; Geisenberger, D. A special type of scald caused by prolonged exposure to slowly heated water. Forensic Sci. Int. 2016, 263, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Brinkmann, B.; Püschel, K. Heat injuries to the respiratory system. Virchows Arch. A Pathol. Anat. Histol. 1978, 379, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Foerster, A. Experimentelle Untersuchungen über Veränderungen an den Atmungsorganen bei plötzlicher Einwirkung hoher Temperaturen. Dtsch. Z. Gesamte Gerichtl. Med. 1933, 20, 445–446. [Google Scholar] [CrossRef]
- Cecchi, R.; Sestili, C.; Prosperini, G.; Cecchetto, G.; Vicini, E.; Viel, G.; Muciaccia, B. Markers of mechanical asphyxia: Immunohistochemical study on autoptic lung tissues. Int. J. Leg. Med. 2014, 128, 117–125. [Google Scholar] [CrossRef]
- Maiese, A.; Manetti, A.C.; Iacoponi, N.; Mezzetti, E.; Turillazzi, E.; Di Paolo, M.; La Russa, R.; Frati, P.; Fineschi, V. State-of-the-Art on Wound Vitality Evaluation: A Systematic Review. Int. J. Mol. Sci. 2022, 23, 6881. [Google Scholar] [CrossRef]
- Bohnert, M.; Anderson, J.; Rothschild, M.A.; Böhm, J. Immunohistochemical expression of fibronection in the lungs of fire victims proves intravital reaction in fatal burns. Int. J. Leg. Med. 2010, 124, 583–588. [Google Scholar] [CrossRef]
- Marschall, S.; Rothschild, M.A.; Bohnert, M. Expression of heat-shock protein 70 (HSP 70) in the respiratory tract and lungs of fire victims. Int. J. Leg. Med. 2006, 120, 355–359. [Google Scholar] [CrossRef]
- Neuhaus, G.A. Kohlenoxyd (CO). In Klinik und Therapie der Vergiftungen; Moeschlin, S., Ed.; George Thieme Verlag: Stuttgart, Germany, 1986; pp. 276–277. [Google Scholar]
- Baselt, R.C. Disposition of Toxic Drugs and Chemicals in Man, 9th ed.; Biomedical Publishing: Foster City, CA, USA, 2011. [Google Scholar]
- Flanagan, R.J.; Taylor, A.; Watson, I.D.; Whelpton, R. Fundamentals of Analytical Toxicology; Wiley: Chichester, UK, 2007. [Google Scholar]
- Barceloux, D.G. Medical Toxicology of Drug Abuse: Synthesized Chemicals and Psychoactive Plants, 1st ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012. [Google Scholar]
- Saukko, P.; Knight, B. Forensic Pathology, Knight’s Fourth ed.; CRC Press: Boca Raton, FL, USA, 2016; Volume 11, pp. 311–324. [Google Scholar]
- Speicher, M.R.; Antonarakis, S.E.; Motulsky, A.G. Volgel and Motulsky’s Human Genetics, 4th ed.; Spinger: Berlin/Heidelberg, Germany, 2010; Volume 2, pp. 31–55. [Google Scholar]
- Old, B.; Schweers, B.A.; Boonlayangoor, P.W.; Reich, K.A. Developmental validation of RSID-saliva: A lateral flow immunochromatographic strip test for the forensic detection of saliva. J. Forensic Sci. 2009, 54, 866–873. [Google Scholar] [CrossRef]
- Buel, E.; Schwartz, M.B.; La Fountain, M.J. Capillary electrophoresis STR analysis: Comparison to gel-based systems. J. Forensic Sci. 1998, 43, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.M. Short tandem repeat typing technologies used in human identity testing. Biotechniques 2007, 43, ii–v. [Google Scholar] [CrossRef]
- Iwase, H.; Yamada, Y.; Ootani, S.; Sasaki, Y.; Nagao, M.; Iwadate, K.; Takatori, T. Evidence for an antemortem injury of a burned head dissected from a burned body. Forensic Sci. Int. 1998, 94, 9–14. [Google Scholar] [CrossRef]
- Imaizumi, K.; Taniguchi, K.; Ogawa, Y. DNA survival and physical and histological properties of heat induced alterations in burnt bones. Int. J. Leg. Med. 2014, 128, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Turillazzi, E.; La Rocca, G.; Anzalone, R.; Corrao, S.; Neri, M.; Pomara, C.; Riezzo, I.; Karch, S.B.; Fineschi, V. Heterozygous nonsense SCN5A mutation W822X explains a simultaneous sudden infant death syndrome. Virchows Arch. 2008, 453, 209–216. [Google Scholar] [CrossRef]
- Malik, M.O.A. Problems in the Diagnosis of the Causes of Death in Burned Bodies. J. Forensic Sci. Soc. 1971, 11, 21–28. [Google Scholar] [CrossRef]
- Spitz, W.U. Spitz and Fisher’s Medicolegal Investigation of Sudden Death. Guidelines for the Application of Pathology to Crime Investigation, 3rd ed.; Charles C Thomas: Springfield, IL, USA, 1993; pp. 413–443. [Google Scholar]
- De Matteis, A.; dell’Aquila, M.; Maiese, A.; Frati, P.; La Russa, R.; Bolino, G.; Fineschi, V. The Troponin-I fast skeletal muscle is reliable marker for the determination of vitality in the suicide hanging. Forensic Sci. Int. 2019, 301, 284–288. [Google Scholar] [CrossRef]
- Maiese, A.; Bolino, G.; Mastracchio, A.; Frati, P.; Fineschi, V. An immunohistochemical study of the value of TREM-1 as a marker for fatal sepsis cases. Biotech. Histochem. 2019, 94, 159–166. [Google Scholar] [CrossRef]
- Simonit, F.; Da Broi, U.; Furioso, C.; Desinan, L. A burned body with a gunshot wound in the mouth and a suicide note: A complex or complicated suicide? J. Forensic Leg. Med. 2020, 72, 101958. [Google Scholar] [CrossRef]
- Maiese, A.; Scopetti, M.; Santurro, A.; La Russa, R.; Manetti, F.; D’Errico, S.; De Matteis, A.; Cingolani, M.; Neri, M.; Pinchi, E.; et al. Corpse dismemberment: A case series. Solving the puzzle through an integrated multidisciplinary approach. J. Forensic Leg. Med. 2020, 74, 102005. [Google Scholar] [CrossRef]
- Esen Melez, İ.; Arslan, M.N.; Melez, D.O.; Gürler, A.S.; Büyük, Y. Manner of death determination in fire fatalities. Am. J. Forensic Med. Pathol. 2017, 38, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Maiese, A.; Gitto, L.; dell’Aquila, M.; Bolino, G. When the hidden features become evident: The usefulness of PMCT in a strangulation-related death. Leg. Med. 2014, 16, 364–366. [Google Scholar] [CrossRef] [PubMed]
- de Bakker, H.M.; Roelandt, G.H.J.; Soerdjbalie-Maikoe, V.; van Rijn, R.R.; de Bakker, B.S. The value of post-mortem computed tomography of burned victims in a forensic setting. Eur. Radiol. 2019, 29, 1912–1921. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Cheng, M.; Xu, J.; Chen, L.; Li, J.; Li, Q.; Xie, X.; Wang, Q. MiR-711 and miR-183-3p as potential markers for vital reaction of burned skin. Forensic Sci. Res. 2020, 1–7. [Google Scholar] [CrossRef]
- Gitto, L.; Bonaccorso, L.; Maiese, A.; dell’Aquila, M.; Arena, V.; Bolino, G. A scream from the past: A multidisciplinary approach in a concealment of a corpse found mummified. J. Forensic Leg. Med. 2015, 32, 53–58. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Type of Heat Injury | Forensic Inspection | Type of Forensic Exam | Histological Examination | Radiological Examination | Toxicological Examination | Genetic Examination |
|---|---|---|---|---|---|---|---|
| Case 1 | Charring | X | A | X | X | ||
| Case 2 | Charring | X | A | X | X | ||
| Case 3 | Charring | X | A | X | X | X | |
| Case 4 | Charring | X | A | X | X | X | |
| Case 5 | Charring | A | X | ||||
| Case 6 | III–IV | X | A | X | |||
| Case 7 | Charring | X | A | X | |||
| Case 8 | III | A | |||||
| Case 9 | III | X | EE | ||||
| Case 10 | II–III | A | |||||
| Case 11 | III | EE | X | ||||
| Case 12 | II–III | A | |||||
| Case 13 | Charring | A | X | ||||
| Case 14 | Charring | A | X | X | |||
| Case 15 | III | A | X | ||||
| Case 16 | Charring | A | X | ||||
| Case 17 | Charring | A | X | X | X | ||
| Case 18 | Charring | X | A | X | X | X | X |
| Case 19 | Charring | X | A | X | X | X | X |
| Case 20 | II–III | X | A | X | |||
| Case 21 | Charring | A | X | ||||
| Case 22 | Charring | X | A | X | X | ||
| Case 23 | II–III | X | A | X | |||
| Case 24 | Charring | X | A | X | X | X | |
| Case 25 | Charring | A | X | X | |||
| Case 26 | Charring | A | X | X | |||
| Case 27 | Charring | A | X | ||||
| Case 28 | Charring | X | A | X | X | ||
| Case 29 | III | A | X | ||||
| Case 30 | III | A | X | ||||
| Case 31 | II–III | A | |||||
| Case 32 | II–III | X | A | X | |||
| Case 33 | Charring | A | |||||
| Case 34 | Charring | A | X | ||||
| Case 35 | Charring | EE | |||||
| Case 36 | III | A | X | ||||
| Case 37 | Charring | A | X | X | |||
| Case 38 | Charring | A | X | X | X | ||
| Case 39 | Charring | A | X | X | |||
| Case 40 | Charring | A | X | X | |||
| Case 41 | Charring | A | X | ||||
| Case 42 | Charring | A | X | X | |||
| Case 43 | Charring | A | X | X | |||
| Case 44 | Charring | X | A | X | |||
| Case 45 | Charring | A | X | X | X | ||
| Case 46 | Charring | A | X | X | X | ||
| Case 47 | Charring | A | X | X | X | ||
| Case 48 | Charring | A | X | X | X | ||
| Case 49 | Charring | A | X | X | X | ||
| Case 50 | Charring | A | X | X | X | ||
| Case 51 | Charring | A | X | X | X | ||
| Case 52 | Charring | A | X | X | X | ||
| Case 53 | Charring | A | X | X | X | ||
| Case 54 | Charring | A | X | X | X | ||
| Case 55 | Charring | A | X | X | X | ||
| Case 56 | Charring | EE | |||||
| Case 57 | II, III, IV | A | X | X | |||
| Case 58 | II, III, IV | A | |||||
| Case 59 | II, III, IV | A | X | X | |||
| Case 60 | II, III, IV | A | X | X | |||
| Case 61 | II, III, IV | A | X | X | |||
| Case 62 | II, III, IV | A | |||||
| Case 63 | II, III, IV | EE | |||||
| Case 64 | II, III, IV | EE | |||||
| Case 65 | II, III, IV | EE | |||||
| Case 66 | II, III, IV | A | X | X | |||
| Case 67 | II, III, IV | EE | |||||
| Case 68 | II, III, IV | EE | |||||
| Case 69 | II, III, IV | EE | |||||
| Case 70 | II, III, IV | EE | |||||
| Case 71 | II–III | EE | |||||
| Case 72 | II–III | EE | |||||
| Case 73 | II–III | EE | |||||
| Case 74 | II–III | EE | |||||
| Case 75 | II–III | EE | |||||
| Case 76 | Charring | A | X | ||||
| Case 77 | Charring | X | A | X | X | X | X |
| Case 78 | II, III, IV | X | A | X | X | ||
| Case 79 | Charring | X | A | X | X | X | X |
| Case 80 | II, III, IV | X | A | X | X | ||
| Case 81 | II–III | X | A | ||||
| Case 82 | Charring | EE | X | X | X |
| Case | Site Inspection |
|---|---|
| Case 1 | Completely charred body found lying on its back in a field with its arms, legs, and neck tied with wire. |
| Case 2 | Carbonized body found in a “wrestling position” in a partially burned reed, lying in a bluff near a railroad line. |
| Case 3 | Carbonized body found sitting in the driver’s seat in a car completely destroyed in the front part at a motorway service area. (A3 motorway) |
| Case 4 | Partially charred body found completely naked and lying crossways on its back in its own bed with legs spread and covered and a cut to the neck. |
| Case 6 | Partially charred body found in the fuselage of an ultralight aircraft crashed in a field. The trunk was protruding from the cockpit and the legs were trapped. Near another lifeless body (Case 7). |
| Case 7 | Partially charred body found in the carcass of an ultralight aircraft that had crashed in a field. He was lying on his back with his legs trapped. Near another lifeless body (Case 6). |
| Case 9 | Almost completely charred body found in a field after a helicopter crash. |
| Case 18 | Almost completely charred body found in a car, sitting in the driver’s seat, arms cuffed behind the back with steel handcuffs. Another charred body on the rear seat. The car had numerous pistol and rifle holes. In the adjacent 7 casings (7.65 caliber) and some cartridges (12 caliber) found. |
| Case 19 | Almost completely charred body inside the car, lying on the floor between the front and rear seats. Arms were bound behind the back with duct tape. The legs were stretched out on the passenger seat and the rest of the body was on the floor of the car. The car had numerous pistol and rifle holes. In the adjacent 7 shell casings (caliber 7.65) and some cartridges (caliber 12) found. |
| Case 20 | Almost completely charred body found lying on its back on the bathroom floor. The apartment showed signs of a recent fire. |
| Case 22 | Partially charred body found lying on its back in a “wrestling position” in an industrial unit with fresh burn marks. |
| Case 23 | Partially charred body found lying on his back in his own bedroom. The apartment had fresh burn marks. |
| Case 24 | Partially charred body found in partially burned brushwood covered ground near a roadway. |
| Case 28 | Partially charred body found lying on its back in a “wrestling position” in its own apartment in a country house. |
| Case 32 | Charred body found lying on its back in a charred mattress in a country house. Near the body a half full glass bottle with wine. |
| Case 44 | Charred male body found in a dwelling. The body was lying on its back in a charred bed with the left wrist raised and tied to the headboard. A coin covered the left eye and another coin lay to the side of the right eye. |
| Case 77 | Body segments belonging to a single subject and signed with the letters ABCD were found behind a military aircraft (C 103 J) in a field near a railway line. |
| Case 78 | Body found in the driver’s seat of a military aircraft (C 103 J) with seat belt fastened in a field near the railway line. |
| Case 79 | The fourth lifeless body was found almost completely submerged in liquid material, identified as fuel, near the fuselage of a military aircraft (C 103 J) in a ditch adjacent to the rail line. |
| Case 80 | Another body was found embedded in the fuselage of the military aircraft (C 103 J). |
| Case 81 | The body was found in a field near the access road to an olive plantation, near a completely burnt car. The body, lying on its back, was naked, with its right arm stretched out between the trunk and the pavement and covered with a green cloth. Remnants of green cloth on the back of the neck. Numerous rocks smeared with reddish liquid (blood). |
| Case | Type of Exam | Instrumental Findings |
|---|---|---|
| Case 1 | CT total body |
|
| Case 3 | CT total body |
|
| Case 4 | CT total body |
|
| Case 5 | CT total body |
|
| Case 11 | RX head, left hand, and wrist |
|
| Case 17 | CT total body |
|
| Case 18 | CT total body |
|
| Case 19 | CT total body |
|
| Case 21 | CT total body |
|
| Case 22 | RX total body |
|
| Case 24 | CT total body |
|
| Case 38 | CT total body |
|
| Case 44 | CT total body |
|
| Case 77 | CT total body |
|
| Case 78 | CT total body |
|
| Case 79 | CT total body |
|
| Case 80 | CT total body |
|
| Case 82 | RX total body |
|
| Case | Autopsy Results |
|---|---|
| Case 1 | In the neck, a copper wire wound with three turns was found, reaching the thorax and abdomen. Removing the copper, a skin sulcus was documented. The I and II finger were amputated by the fire. Additionally, the ankle was tied by copper wire. In the right front- temporal region, there was a bone fracture. No soot was found in the respiratory system. |
| Case 2 | In the larynx, there was a very slight presence of soot. There was an absence of soot in the trachea and bronchi. |
| Case 3 | Presence of heat amputation (radius and ulna, because of the fire). There was soot in the larynx, trachea, and bronchi. |
| Case 4 | In the anterior region of the neck, there was a continuous solution, in an ecchymotic context, which affects all the muscles of the supra-hyoid region, deepening up to the fibromuscular planes and affecting the vascular structures. No injuries were found in the carotid arteries and jugular veins. |
| Case 5 | There were bone fractures in the upper limbs, lower limbs, ribs, and sternum, with evident hemorrhagic infiltration. No signs of smoke inhalation were found in the trachea. The pericardial sac was torn, leading to the exposure of the heart. There was laceration of the heart, with opening of the right ventricular and atrial cavities. The lower third of the left ventricle presented two lacerations. A further full-thickness laceration was found in the ascending aorta. |
| Case 6 | Occipital fracture and multiple rib fractures with hemorrhagic infiltration were found. There were numerous displaced and exposed fractures of legs. There was a rupture of the pericardium, leading to the exposure of the myocardial wall (because of heat). Laceration of the anterior wall of the right ventricle. Two more tears in both atria. Hemothorax. |
| Case 11 | There was an absence of soot in the respiratory tract. A thickened area in the lower lobe of the right lung was found, along with cardiac hypertrophy and diffuse atherosclerosis. |
| Case 13 | Exposure of the intra-abdominal organs was found. Partial amputation of the upper and lower limbs occurred. There was soot in the bronchial branches. |
| Case 14 | The presence of heat fractures was detected. |
| Case 15 | There were multiple fractures of ribs, and multiple subpleural petechiae bilaterally. Heavy lungs, with areas of contusion, were found mostly on the right. A yellowish secretion was present the level of the right bronchial branches. |
| Case 16 | There was a tear in the left parieto-occipital region. A laceration on the second finger of the left hand was found, as was hemorrhagic infiltration of the internal side of the scalp in the parieto-occipital area. There were multiple rib fractures. There was no presence of sooty material in the tracheal lumen. In the lungs, areas of contusion were found at the level of the bilateral mediastinal face and an interscissural hemorrhagic infiltration was found on the right. |
| Case 17 | Upper airway smoking was found. No residual dust or fumes in the distal middle third of the trachea and bronchus. |
| Case 18 | There was exposed thoraco-abdominal viscera, and fractures in the upper and lower limbs. Complete amputation of the bone and muscle structures of the right thigh occurred. In the clavicle, there was a fragment of the entrance of a bullet. In the larynx and trachea, there was little blackish material. In the left limb there was the entrance of a bullet. |
| Case 19 | There was a fracture between D12 and L1, and a complete absence of bones of the chest. The absence of the abdominal wall and the abdominal and pelvic organs was found. Amputation of the upper and lower limbs occurred bilaterally. At the level of the residue of the right clavicle, the entrance of a bullet was found. At the edge of the right ventricle, there was a continuous full-thickness solution of the ventricular wall. In the lower lobe of the left lung and in the right iliac spine, the entrance of a bullet was found. |
| Case 20 | There was abundant sooty material in the oral cavity and respiratory orifices. The epiglottis and bronchi were covered with abundant brownish sooty material. |
| Case 21 | Exposure of thoraco-abdominal organs was found, with extreme friability of soft tissues. There was no organ damage. |
| Case 22 | There was the exposure of the intestinal packet and loss of joint relations bilaterally at the level of the knee. The presence of hyperemia of the epiglottis and sooty material in the airways were found. |
| Case 23 | There was abundant sooty residues mixed with blood on the tongue. Abundant sooty material was mixed with mucus in the larynx. There was soot and blood in the trachea and bronchi. |
| Case 24 | An ecchymotic area was found at the level of the neck. Hematic infarction at the level of the platysma, sternocleidomastoid, and thyroid-hyoid muscles was identified. There was preternatural motility of the right greater horn of the hyoid bone, and of the upper right and left horns of the thyroid cartilage; there was blood infiltration of neighboring tissues. Hematic material and rare soot were found in the respiratory tract. |
| Case 25 | Laceration was found in the head. There was soot in the larynx, trachea, and in the initial portion of the main bronchi. Hyperemic mucosa in large, medium, and small bronchi with the presence of soot was found. |
| Case 26 | There was soot and food material in the esophagus, and blood and soot in the trachea and inside the bronchi. |
| Case 27 | Loss of substance in the right hemisome and the anterior surface of the lower limbs was found, along with protrusion of the intestinal loops. There was a biosseous fracture in the right wrist. At the epiglottis, there was abundant mucus and soot. There was Diffuse mucosal hyperemia of trachea and bronchi, with soot and cherry red blood in lungs. |
| Case 28 | Exposure of the bony structures of the head and of the thoracic and abdominal viscera was found. There was a fracture of the hyoid bone in the absence of blood infiltration. Soot and blood were found in the airways and bronchi. |
| Case 29 | At the opening of the larynx, trachea and bronchi, soot mixed with blood was found. Lungs were red and expanded. There was edema and soot in the hilum and bronchi. |
| Case 30 | Abundant soot mixed with blood was found in the larynx, trachea, and bronchi. Lungs were red and expanded. Edema and soot were found in the hilum and bronchi. |
| Case 31 | No soot was found in the first respiratory tract. Diffuse hyperemia of the larynx was observed, as well as plate occluding lumen of the circumflex coronary and the right coronary. In the lateral wall, there was a discolored area. In the anterior wall, there was an area with hemorrhagic punctuation. The cardiac parenchyma was affected by diffuse areas of adipose infiltration and myocardiosclerosis. |
| Case 32 | There was soot in the airway (larynx, trachea, bronchi, and upper tract of esophagus). |
| Case 33 | There was soot the in airway (larynx, trachea, and bronchi). |
| Case 34 | The mucosa of larynx, trachea, and bronchi presented oedema, hyperemia, and soot. Increased volume of lungs was found, with a cherry red color. In airways the presence of soot and foam was found, along with hyperemic and cherry red colored mucosa of the bronchi. |
| Case 36 | Abundant sooty material was found in the larynx and trachea; there was soot and blood in the bronchi. Bright red lungs were identified, along with oedema and sooty residues in the hilum and bronchial branches. There was oedema and organs congestion, and a bright red coloring of the blood. |
| Case 37 | In the larynx and trachea abundant mucoid material and red mucosa were found. There was no soot in the bronchial branches. |
| Case 38 | No carbonaceous material was found in the larynx, trachea, and bronchi. |
| Case 39 | In the trachea, there was the presence of blackish mucus and partially digested food material. There was no soot in the bronchial branches. |
| Case 40 | There was exposed intestinal skein, as well as coronarosclerosis and left ventricular hypertrophy. |
| Case 41 | A lacerated bruised lesion was found in the left frontal region. Ecchymosis was found in the jugular vein region. There was multiple bruising in both forearms. The distal phalanx of the third finger of the right hand was sub-amputated. In the larynx and trachea, there was abundant soot mixed with mucus and foam. In the bronchi, the presence of blackish color particles was detected. |
| Case 42 | In the occipital, right posterior parietal and right temporal region, there was a bone breach, with the release of encephalic material completely undone by the heat. Exposure of the intestinal skein occurred. There was an absence of deposits of soot in the respiratory tract. |
| Case 43 | Corpse remains consisted of a trunk and limbs. The right lung was charred. There was no soot in the esophagus and trachea. |
| Case 44 | In the left fronto-temporal region, there was a diamond-shaped continuous solution with clear margins. In the right frontotemporal region, there was a millimeter cutaneous incisura. The wick of a candle protrudes between the lips. In the neck, superficial laceration interesting the soft tissues was found. In the head, there was the presence of two holes, affecting the cranial theca, the first in the right frontal region, and the second in the frontal bone on the left. The two frontal hemispheres are affected by lacerative/hemorrhagic lesions in correspondence with the other cranial lesions. There was a massive bilateral hemothorax. At the hemithorax, two large breaches were found bilaterally. On the mediastinum, circular laceration corresponding to a perforative pericardial lesion was found. Hemopericardium occurred. There were lacerative lesion through the right ventricle of the heart. No foreign material was found in the bronchi. At the loops of the tenuous, three circular lacerations with hemorrhagic infiltration of the tissue were found. There was a circular laceration at the level of the mesentery. There was one laceration in the left colonic flexure and a circular laceration between L4-L5. The first bullet was in the right periscapular soft tissues; the second bullet was at the L4 lamina. |
| Case 45 | There was abundant soot in larynx, trachea, and bronchi. |
| Case 46 | Abundant soot was found in the larynx, trachea, and bronchi. Intracranial hemorrhage occurred because of fire. Abundant soot was found in the trachea and bronchi. |
| Case 47 | Rhymes of heat fractures, and complete loss of the jaw occurred. Exposure of the frontal sinuses occurred. There were Multiple IV fractures. Both lungs were coated by the action of heat, with a charred surface. There was soot in the airway, and a compact parenchyma of the section. |
| Case 48 | Soot and foam were found in the larynx and trachea. |
| Case 49 | Skeletonization of the right tibia and femur occurred, along with disarticulation of the left knee. Blackish material was found in the trachea and in the bronchial branches. |
| Case 50 | Diffuse hemorrhagic infiltration of the prevertebral fascia of the lower part of the cervical spine with “burst” fracture of the soma of C7 occurred. |
| Case 51 | There was no soot in the respiratory tract. There was a fracture of D12 and L1. |
| Case 52 | There was soot in the bronchial branches. |
| Case 53 | Skull fractures occurred because of the fire. Externalization of the intestinal skin, the liver, and the right lung occured. Mutilated upper limbs were observed. Fracture of lower limbs occurred because of fire. Lungs are coated and charred, and there was a “cooked” parenchyma; there was soot in the bronchi. |
| Case 54 | Externalization of the thoraco-abdominal viscera occurred. There were multiple heat fractures in the limbs. Soot was found in the trachea. In the bronchi, rosacea foam and traces of soot were found. |
| Case 55 | No soot was found in the respiratory tract. In the esophagus, larynx, and trachea, a minimal amount of gastric contents was found. Laceration of the left hemidiaphragm occurred. |
| Case 57 | Absence of the distal phalanx of the index finger of the right hand and of the distal portion of the last phalanx of the middle finger was observed. The larynx, esophagus, and trachea were injury-free. |
| Case 58 | The larynx, esophagus, and trachea were injury-free. |
| Case 59 | There was nothing to the esophagus, trachea, and larynx. There was an asence of soot in the bronchi. A congested and edematous lung parenchyma was observed. |
| Case 60 | There was no soot in the bronchi. A congested and edematous lung parenchyma was observed. |
| Case 61 | There was no soot in the bronchi. A congested and edematous lung parenchyma was observed. |
| Case 66 | There was no soot in the bronchi. A congested and edematous lung parenchyma was observed. |
| Case 76 | Soot was found in small quantities in the larynx and trachea. Coerced and charred lungs were observed. There was a blackish punctuation of the parenchyma in the most spared areas. |
| Case 77 | Residues of body segments consisting of the head, neck, thorax, upper limbs, lower limbs, and abdominal-pelvic visceral parts were observed. There was disruption of the skull, with the absence of brain structures and the loss of somatic features. Wide continuous solution to the face and skull was observed, and there was continuous solution in the left mandibular region. A fragmented face occurred. There was a left sterno-costal fracture focus with diastatic fracture of the sternum in the middle third. Multi-fragmentation of the clavicle and all the ribs of the thorax occurred. Multiple lung lacerations were observed. There was continuous endo-myocardial solution in the left ventricle. There was preternatural mobility of the cervical spine in C6–C7; section at the body of D12. The rupture of the bladder, prostate, sigmoid, and tract of colon and small intestine occurred. |
| Case 78 | Multiple bilateral rib fractures with hemorrhagic infiltration of the soft tissues occurred. Laceration of the intercostal muscles and the left parietal pleura was observed. In the heart, there were multiple contusive subepicardial areas in the upper third of the right ventricle and diffuse epicardial hemorrhagic punctuation in the atrial and ventricular area at the base of the right auricle, endocardial laceration, with hemorrhagic infiltration. Paravertebral hemorrhagic infiltration occurred, as did a fracture of L1. |
| Case 79 | In the head, the presence of the burning of the dura with stratification of blood material was found. No carbon residues or blood were found inside the trachea. There were multiple bilateral rib fractures. There was a fracture of the body of the sternum. Bilateral hemothorax occurred, as did “Cooked” lungs. |
| Case 80 | Multiple fractures in the skull were found. Dura mater was lacerated in the fracture. In the brain, blunt hemorrhagic focus in the right hemisphere occurred, as did skull base fractures. There were multiple bilateral rib fractures with blood infiltration of soft tissues. |
| Case 81 | The brain had a “cooked” appearance. There was soot in the trachea. The heart had increased consistency and volume; the common trunk of the left coronary artery had a stenosis of about 50% of its caliber, as did the proximal tract of the anterior descending; the right coronary artery had an eccentric stenosis of 50% of its caliber proximally, as well as marked left ventricular hypertrophy and right ventricular dilatation. In the lungs there was the presence of soot in the bronchi. |
| Case | Histology | Immunohistochemistry |
|---|---|---|
| Case 1 | In the lungs, alveolar hyperdistention, rupture of alveolar walls, and moderate interalveolar oedema occurred. In the striated muscle tissue of the cervical region, there were areas of dissociation of fibers because of extensive hemorrhagic spread. Fragments of skin and subcutaneous tissues showed rare leukocyte elements and red blood cells. | Fibronectin −; hsp 70 +/−, CD62P −. |
| Case 2 | In the heart, a large-scale connectivity replaces large muscle tracts, with residual myocyte islands embedded in this connectivity-like tissue. Fibroblasts and newly formed capillaries are seen within this loose connective tissue. The presence of neutrophilic granulocytes with both vascular and interstitial margins was observed. Microcirculation characterized by diffuse and mediointimal sclerosis with luminal stenosis that assumes aspects of severe functional criticality was observed. | |
| Case 3 | In the lungs, there was a widespread presence of large optic voids, secondary to fusion of multiple alveoli by the rupture of alveolar septa. A blackish, anthracotic, inert, and powdery material is observed inside some alveoli, which is also present inside foamy macrophages. The bronchial lumen is occupied by soot particles mixed with amorphous eosinophilic material, as well as the decay of the lining epithelium. | |
| Case 4 | In the lungs, focal interstitial oedema, capillary congestion, and hemorrhagic extravasation were observed in the presence of some neutrophilic granulocytes mixed with histiocytic elements in the alveolar spaces. | Fibronectin −; hsp 70 −, CD62P +/−. |
| Case 6 | In the lungs, the presence of areas of endoalveolar and parenchymal hemorrhage of a contusive nature was observed. | |
| Case 7 | In the lungs, areas of endoalveolar and parenchymal hemorrhage consistent with traumatic genesis were observed. | |
| Case 14 | In the lungs, presence of areas of acute and chronic emphysema with septa, characterized by fissures with edges that look like a “tuft of a brush” and a “drumstick” were observed. | |
| Case 15 | In the lungs, the presence of areas of acute emphysema with septa characterized by fissures with margins that look like a “tuft of brush” were observed. The endoalveolar spaces and the septal spaces were occupied by eosinophilic material studded with red blood cells and white line cells. | |
| Case 16 | Elongation of the cell nuclei of trachea occurred. In the lungs, adipose emboli were present. The endoalveolar spaces and the septal spaces were occupied by very abundant red blood cells, macrophages, and polymorphonuclear cells. Hemorrhages in the liver and spleen were present. | Anti HSP27 ++ |
| Case 17 | The neck’s skin shows changes due to autolytic phenomena and normal architecture of the papillary component, with greater preservation of the reticular component and fatty infiltration of the dermis itself. | [N] anti-HSP27 and anti-HSP70 ++, anti-HSP90 +/−, anti-tryptase +/−. [S] thigh: HSP27 −, HSP70 −, HSP90 −, tryptase −. HIF-1α +++. |
| Case 18 | In the lungs, endoalveolar oedema, acute stasis, and heat changes were observed. | |
| Case 19 | In the lungs, autolytic destructive phenomena occurred due to the heat. Pulmonary circulation shows the presence of abundant conglutinated blood material within the lumen, and elective staining for fats (Sudan III) shows complete negativity. | |
| Case 24 | In the lungs, multiple fields of empty optic spaces occurred because of the fusion of multiple alveoli due to rupture of septa that were thinned and stretched. Presence of erythrocytes within the alveolar spaces was observed. There we significant hemorrhagic spurs and the presence of neutrophils in platysma and right sternocleidomastoid muscle. Discontinuity of bone tissue with the dislocation of fragments with hemorrhagic spurs are present in greater right horn of hyoid bone and superior horns of thyroid cartilage | |
| Case 25 | In the lungs, parenchyma shows the presence of a modest, inert, and powdery material of a blackish color. This material is rarely present at the level of the lining epithelium of the alveolar cavities and is mainly contained in numerous foamy macrophages in the intralveolar region. | |
| Case 26 | In the lungs, parenchyma shows the presence of a modest inert powdery material with a blackish color. | |
| Case 37 | In the brain, oedema and cerebral stasis were observed. In the lungs, intense pulmonary stasis, and oedema with signs of acute emphysema were observed. High grade myocardial and hepatic stasis, with aspects of red blood cell adhesions, were also observed. | |
| Case 38 | In the brain, oedema, and parenchymatous congestion occurred. Heat hematoma was observed. In the trachea, epithelial flaking and sporadic inflammatory submucosal lympho-monocytic infiltrates were observed. Bronchi show a cellular sloughing of the epithelium and intense leukocyte infiltration in the submucosa, with some eosinophilic granulocytes. At the cardiac level, there were areas of disseminated myocardiosclerosis with localization at the septal level and in the right ventricle, as well as disarray, myocyte hypertrophy and signs of myofiber dissolution. | |
| Case 39 | In the brain, stasis and edema were observed. In the lungs, severe stasis, acute emphysema, evidence of anthracosis, and chronic bronchitis were apparent. In the heart, stasis and evidence of incipient coronary artery disease were found. Steatosis and hepatitis in a picture consistent with alcoholic liver disease were observed. In the skin, heat damage was of a manifestly post-factitious nature. | |
| Case 40 | In the lungs, areas of chronic emphysema and oedema with overt endoalveolar hemorrhagic aspects were observed. In the heart, myocardiosclerosis and significant coronary atherosclerosis occurred, with foci of coagulation and myocytolysis. | |
| Case 41 | In the lungs, incongruous blackish particles sometimes confluent in bronchial structures were observed in the terminal bronchioles and alveoli. In the trachea, the endoluminal presence of incongruous blackish material was found, adhering to the epithelium. | |
| Case 42 | In the lungs, areas of acute emphysema alternating with areas of coarctation of the parenchyma were found; overt endoalveolar hemorrhagic aspects were present, with evidence of adipose-medullary embolization. In the trachea, there was an absence of incongruous material suggestive of inhaled charcoal particles. There was post-fatal heat damage to all organs. | Fibronectin −; hsp 70 +/−, CD62P −. |
| Case 43 | In the lungs, areas of acute emphysema alternating with areas of coarctation of the parenchyma were observed; there were endoalveolar hemorrhagic aspects; there was evidence of adipose-medullary embolization. | |
| Case 45 | In the lungs, congestion and foci of atelectasis and emphysema were observed. In the trachea, congestion and the presence of blackish material on the mucosal surface were observed. | Fibronectin ++; hsp 70 +/−, CD62P ++. |
| Case 46 | In the lungs, congestion, oedema, and intralveolar hemorrhage were observed. | Fibronectin +; hsp 70 ++, CD62P +. |
| Case 47 | In the lungs, pulmonary parenchyma with congestion and oedema was present. | Fibronectin ++; hsp 70 +/−, CD62P ++. |
| Case 48 | In the trachea, there was a tracheal wall with congestion. In the lungs, there was congestion and alveolar oedema. | Fibronectin +; hsp 70 ++, CD62P +. |
| Case 49 | In the lungs, congestion and alveolar oedema were found. | Fibronectin ++; hsp 70 ++, CD62P ++. |
| Case 50 | In the lungs, congestion, oedema, and alveolar hemorrhage were present; there were micronodules of fibrosis in subpleural area. Intraepidermal blisters in skin were observed. | Fibronectin ++; hsp 70 +/−, CD62P ++. |
| Case 51 | In the trachea, congestion occurred. In the lungs, congestion and oedema occurred. | Fibronectin +; hsp 70 +/−, CD62P ++. |
| Case 52 | In the trachea, there was a deposition of blackish material (soot). In the lungs, there was marked congestion and massive oedema. Hyperkeratosis of the skin and presence of blackish material in the stratum corneum was observed. | Fibronectin +; hsp 70 +/−, CD62P +. |
| Case 53 | In the lungs, marked congestion, oedema, and alveolar hemorrhage were observed. | Fibronectin +; hsp 70 +, CD62P ++. |
| Case 54 | In the heart, scarring of myocardial infarction was present. In the lungs, parenchyma with congestion, endoalveolar oedema and microhemorrhages were observed. | Fibronectin +; hsp 70 +, CD62P +. |
| Case 55 | In the lungs, congestion, oedema and intralveolar microhemorrhages were observed. | Fibronectin +; hsp 70 ++, CD62P ++. |
| Case 57 | In the trachea and lungs, congestion and oedema were present. Subepidermal blistering of skin was apparent. | |
| Case 59 | Polyvisceral congestion was observed. | |
| Case 60 | In the lungs congestion, oedema and alveolar microhemorrhages were apparent. Polyvisceral congestion was observed. | |
| Case 61 | Polyvisceral congestion was observed. | |
| Case 66 | Polyvisceral congestion was observed. | |
| Case 76 | In the lungs, there was a massive edema in smoker’s lung. There was evidence of probable alcohol-related liver disease. | |
| Case 77 | In the lungs, there was an alternation of areas dominated by bleeding events with areas of acute emphysema. There was no lack of peribronchial inflammatory infiltrates. Chronic emphysema was observed. In the skin, there was an almost complete loss of stratum corneum with small hemorrhagic foci immediately below; there was abundant incongruous blackish material adherent to the skin surface (lesion with vital signs). In left thigh, there were muscle interruptions of the fibers with modest signs and hemorrhagic spreads. In the right thigh skin, there was no epidermis, a completely burned dermis; hemorrhagic changes were observed in the underlying fat. | |
| Case 78 | In the lungs, abundant hemorrhages with signs of acute and chronic emphysema were observed. In the school child’s brain, there was a small hemorrhagic focus, probably of blunt origin. The left ventricle of the heart contained areas of contraction band necrosis and hemorrhagic microfoci. | |
| Case 79 | In the lungs, there were alternating areas of edema, hemorrhagic edema, acute emphysema, and atelectasis. In the arterioles, there was embolic material of adipose-medullary origin. In some areas, material of obvious food origin was found within the alveoli. Skin fragments strongly altered by heat exposure with areas of vacuolization were observed. | |
| Case 80 | In the lungs, advanced changes, probably due to heat exposure, with homogenization of the parenchyma were observed. Areas of severe edema, even hemorrhagic, and areas of atelectasis were present. In the heart, advanced changes with homogenization of the parenchyma were apparent. | |
| Case 81 | In the lungs, there was discrete fibrous enhancement with discrete anthracotic imprint. Occasional inflammatory infiltrates of chronic significance were observed. There was acute and chronic emphysema, predominantly in the subpleural region. In the left ventricle myocardium, aspects of marked myocytic hypertrophy were present, along with areas of fibrous replacement of various sizes, and myocytes with vacuolar appearance. Subendocardial contraction band necrosis was observed, as was multi-organ congestion. |
| Case | COHb, HCN | Substances of Abuse |
|---|---|---|
| Case 2 | CoHb: 5–10% | Central blood ethyl alcohol: 0.75 g/L, peripheral blood: 0.69 g/dL, content gastric: 0.70 g/dL. |
| Case 3 | CoHb: 60% | Cocaine in the blood: 5 ng/mL, in the urine: 105 ng/mL; benzoylecgonine: in blood 250 ng/mL; in urine 13,800 ng/mL. |
| Case 4 | - | Central blood ethyl alcohol: 3.18 g/L. |
| Case 13 | CoHb: 60–62% | Negative for each substance |
| Case 14 | CoHb: 28–30% | Negative for each substance |
| Case 17 | CoHb: 9.48% | 7-aminoclonazepam in the brain, hair, and pubic hair +; Alprazolam in brain, liver, kidney, hair and pubic hair samples +; α-hydroxialprazolam in the brain, liver and kidney +; Oxacarbazepine in the brain, liver and pubic hair +; Ethylglucuronide in hair and pubic hair samples +. |
| Case 18 | Negative | Negative for each substance |
| Case 19 | Negative | Negative for each substance |
| Case 20 | CoHb: 45.3% | Negative for each substance |
| Case 22 | CoHb: 6% | Negative for each substance |
| Case 23 | CoHb: 56% | Negative for each substance |
| Case 24 | CoHb: 3.9% | Negative for each substance |
| Case 25 | CoHb: 19% | Negative for each substance |
| Case 26 | CoHb: 83% | Negative for each substance |
| Case 27 | CoHb: 48% | Negative for each substance |
| Case 28 | CoHb: 22% | Negative for each substance |
| Case 29 | CoHb: 53% | Negative for each substance |
| Case 30 | CoHb: 49% | Negative for each substance |
| Case 32 | CoHb: 60% | Central blood ethyl alcohol: 3.5 g/L |
| Case 34 | CoHb: 56% | Negative for each substance |
| Case 36 | CoHb: 63% | Negative for each substance |
| Case 37 | Negative | Negative for each substance |
| Case 38 | Negative | Venlafaxine, O-desmethyl-venlafaxine: positive. |
| Case 39 | Negative | Central blood ethyl alcohol: 3 g/L |
| Case 40 | Negative | Negative for each substance |
| Case 42 | Negative | Negative for each substance |
| Case 43 | Negative | Negative for each substance |
| Case 45 | CoHb: 12.79%; HCN: 0.78 mg/L | Negative for each substance |
| Case 46 | CoHb: 31.87%; HCN: 1.11 mg/L | Negative for each substance |
| Case 47 | CoHb: 2.96%; HCN: 1.50 mg/L | Negative for each substance |
| Case 48 | CoHb: 11.9%; HCN: 0.91 mg/L | Negative for each substance |
| Case 49 | COHb: 14.3%. HCN: 1.07 mg/L | Negative for each substance |
| Case 50 | COHb: 11.16%; HCN: 1.08 mg/L | Negative for each substance |
| Case 51 | COHb: 6.0%; HCN: 1.09 mg/L. | Negative for each substance |
| Case 52 | COHb: 10.88%; HCN: 0.95 mg/L. | Negative for each substance |
| Case 53 | COHb: 21.42%; HCN: 1.57 mg/L. | Negative for each substance |
| Case 54 | COHb: 1.23%; HCN: 1.44 mg/L | Negative for each substance |
| Case 55 | COHb: 13.9%; HCN: 1.09 mg/L | Negative for each substance |
| Case 57 | COHb: 4.72%; HCN: 1.43 mg/L | Negative for each substance |
| Case 59 | COHb: 11.35% HCN: 1.08 mg/L | Negative for each substance |
| Case 60 | COHb: 12.00%; HCN: 1.23 mg/L | Negative for each substance |
| Case 61 | COHb: 6.13%; HCN: 1.11 mg/L | Negative for each substance |
| Case 66 | COHb: 5.27%; HCN: 1.14 mg/L | Negative for each substance |
| Case 76 | COHb: 1.6%; | Negative for each substance |
| Case 82 | Negative | Negative for each substance |
| Case | Cause of Death | Exams Performed | Flame Action | Timing of Death |
|---|---|---|---|---|
| Case 1 | Violent mechanical asphyxia consistent with strangulation due to compression of the neck, associated with a large multiple blunt fracture trauma | F-A-H-R | PM | |
| Case 2 | Acute myocardial infarction at the level of the lateral portion of the left ventricle, in a patient with severe impairment of the myocardial microcirculation | F-A-H-T | PM | |
| Case 3 | Acute CO intoxication with diffuse body charring from flame exposure | F-A-H-R-T | AM | |
| Case 4 | Acute carbon monoxide poisoning associated with extensive body charring from flame exposure, and acute methemorrhagic anemia from slaughter, associated with violent mechanical asphyxia from internal submersion by inhalation of blood in the respiratory tract, in a subject in a state of acute alcohol intoxication | F-A-H-R-T | PM | |
| Case 5 | Polytraumatism | F-A-H-R-T | PM | |
| Case 6 | Polytraumatism | A-R | I | |
| Case 7 | Polytraumatism | F-A-H | PM | |
| Case 8 | Pathophysiological consequences of deep burns affecting 18% of the body surface area | F-A-H | D | |
| Case 9 | Acute respiratory failure in a patient with burn shock and burns III, involving 90% of body surface area | A | D | |
| Case 10 | Multi-organ failure in patients with II, III (and IV)-grade burns on almost all body surface area | F-EE | D | |
| Case 11 | Pathophysiologic sequelae of deep burns affecting 95% of body surface area | A | I | |
| Case 12 | Multi-organ failure in patients with II, III, and IV-grade burns on almost all body surface area | EE-R | D | |
| Case 13 | Acute cardio-respiratory failure due to charring on a living object after a burn | A | AM | |
| Case 14 | Acute cardio-respiratory failure due to burns (I-, II-, III-degree) and charring of the head, trunk, and four limbs | A-T | AM | |
| Case 15 | Septic shock with multiple organ dysfunction syndrome secondary to burns (III degrees) affecting 20–29% of the body surface | A-H-T | D | |
| Case 16 | Pathophysiological consequences of deep burns affecting in polytraumatism | A-T | PM | |
| Case 17 | Violent mechanical asphyxiation | A-H | PM | |
| Case 18 | Osteo-visceral injuries from two gunshots to the neck and left upper extremity | A-H | PM | |
| Case 19 | Osteo-visceral injuries due to 3 shots to the thorax and pelvic region | A-H-R-T | PM | |
| Case 20 | Acute exogenous intoxication due to inhalation of gasses and vapors in individuals with I- and II-degree burns that extended to more than 50% of the body surface area. | F-A-H-R-T-G | ||
| Case 21 | Damage caused by thermal energy consistent with direct exposure of the body to flammable liquids | F-A-H-R-T-G | AM | |
| Case 22 | Damage caused by thermal energy compatible with direct exposure of the body to flammable liquids | F-A-T | AM | |
| Case 23 | Violent mechanical asphyxia (strangulation), performed by a copper rope, associated with a large multiple blunt fracture trauma | A-R | ||
| Case 24 | Acute myocardial infarction at the level of the lateral portion of the left ventricle, in a patient with severe impairment of the myocardial microcirculation | F-A-R-T | PM | |
| Case 25 | Acute exogenous carbon monoxide and hydrogen cyanide intoxication associated with II- and III-degree flame burns extending over large portions of the body surface | F-A-T | AM | |
| Case 26 | Violent mechanical asphyxia consistent with strangulation due to compression of the neck | F-A-H-R-T | AM | |
| Case 27 | Charring due to flame exposure | A-H-T | AM | |
| Case 28 | Acute CO intoxication | A-H-T | AM | |
| Case 29 | Acute CO and HCN intoxication with diffuse body charring from flame exposure | A-T | ||
| Case 30 | Charring due to flame exposure | F-A-T-G | ||
| Case 31 | Acute CO and HCN intoxication with diffuse body charring from flame exposure | A-T | ||
| Case 32 | Acute CO and HCN intoxication with diffuse body charring from flame exposure | A-T | ||
| Case 33 | Acute myocardial infarction | A | AM | |
| Case 34 | Acute carbon monoxide intoxication | F-A-T | AM | |
| Case 35 | Neurogenic shock from thermal energy, consistent with direct exposure of the soma to flame | A | AM | |
| Case 36 | Acute CO and HCN intoxication with diffuse body charring from flame exposure | A-T | ||
| Case 37 | Charring due to flame exposure | A-R-T | PM | |
| Case 38 | Acute myocardial infarction | A-H-R-T | PM | |
| Case 39 | Sudden death of an epileptic patient (SUDEP) | A-H-T | PM | |
| Case 40 | Acute cardiac pump failure developed on a substrate, characterized by a significant degree of myocardiosclerosis and coronary atherosclerosis | A-H-T | PM | |
| Case 41 | Charring due to flame exposure | A-H | AM | |
| Case 42 | Polytrauma | A-H-T | PM | |
| Case 43 | Polytrauma | A-H-T | PM | |
| Case 44 | Osteo-visceral injuries due to three gunshots to the head, chest, and abdomen | F-A-R | PM | |
| Case 45 | Acute CO and HCN intoxication | A-H-R-T | AM | |
| Case 46 | Acute CO and HCN intoxication | A-H-T-G | AM | |
| Case 47 | Acute CO and HCN intoxication | A-H-T-G | AM | |
| Case 48 | Acute CO and HCN intoxication | A-H-T-G | AM | |
| Case 49 | Acute CO and HCN intoxication | A-H-T-G | AM | |
| Case 50 | Acute CO and HCN intoxication | A-H-T-G | AM | |
| Case 51 | Acute CO and HCN intoxication | A-H-T-G | AM | |
| Case 52 | Acute CO and HCN intoxication | A-H-T-G | AM | |
| Case 53 | Acute CO and HCN intoxication | A-H-T-G | AM | |
| Case 54 | Acute CO and HCN intoxication | A-H-T-G | AM | |
| Case 55 | Acute CO and HCN intoxication | A-H-T-G | AM | |
| Case 56 | Not identifiable | EE | ||
| Case 57 | Multi-organ failure in patients with II-, III-, and IV-degree burns over nearly the entire body surface area | A-H-T | D | |
| Case 58 | Cardiorespiratory failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | A | D | |
| Case 59 | Cardiorespiratory failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | A-H-T | D | |
| Case 60 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | A-H-T | D | |
| Case 61 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area. | A-H-T | D | |
| Case 62 | Acute respiratory failure with shock-lung syndrome and signs of inhalation injury; acute renal failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area. | A | D | |
| Case 63 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area. | EE | D | |
| Case 64 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | EE | D | |
| Case 65 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | EE | D | |
| Case 66 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | A-H-T | D | |
| Case 67 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | EE | D | |
| Case 68 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | EE | D | |
| Case 69 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | EE | D | |
| Case 70 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | EE | D | |
| Case 71 | Respiratory failure after escharotomy surgery in patients with extensive II- and III-degree external burns on 80% of the body surface | EE | D | |
| Case 72 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | EE | D | |
| Case 73 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | EE | D | |
| Case 74 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | EE | D | |
| Case 75 | Multi-organ failure in patients with II-, III-, and IV-grade burns over nearly the entire body surface area | EE | D | |
| Case 76 | Charring due to flame exposure | A-H | PM | |
| Case 77 | Multi-layered traumatic injuries causing body impoverishment | F-A-H-R-T-G | PM | |
| Case 78 | Cranioencephalic lesions | F-A-H-R | I | |
| Case 79 | Mechanical injuries and thermal injuries | F-A-H-R-T-G | PM | |
| Case 80 | Cranioencephalic lesions | F-A-H-R | I | |
| Case 81 | Cardiac failure in persons with deep II- and III-degree burns extending over almost the entire body surface | F-A | ||
| Case 82 | Not identifiable | EE-R-T |
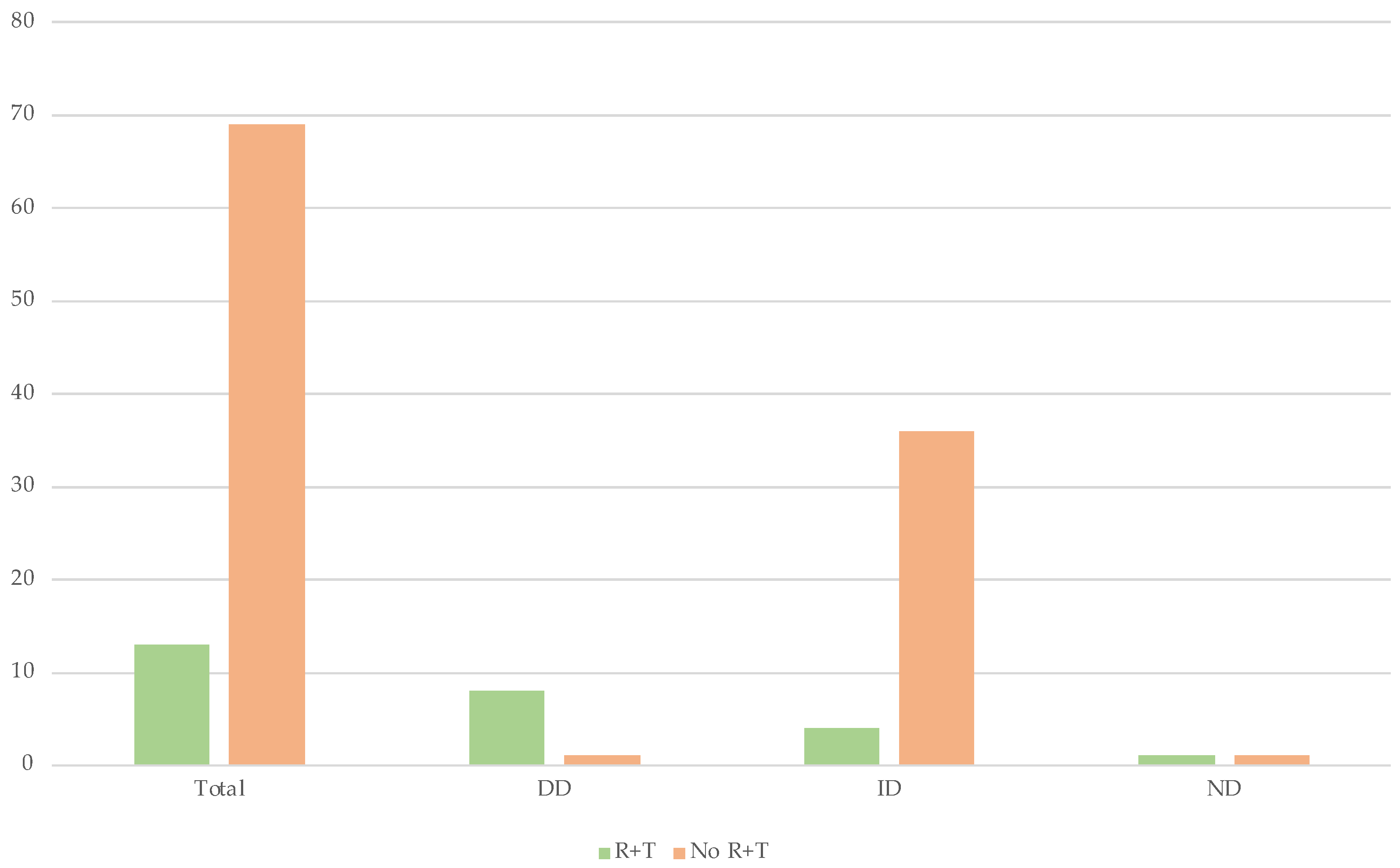
| Total | R + T | No. R + T | ||||
|---|---|---|---|---|---|---|
| 82 | 13 (15.9%) | 69 (84.1%) | ||||
| DD | ID | ND | DD | ID | ND | |
| 8 (61.5%) | 4 (30.77%) | 1 (7.9%) | 32 (46.4%) | 36 (52.2%) | 1 (1.4%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maiese, A.; Ciallella, C.; dell’Aquila, M.; De Matteis, A.; Toni, C.; Scatena, A.; La Russa, R.; Mezzetti, E.; Di Paolo, M.; Turillazzi, E.; et al. Cause of Death in Charred Bodies: Reflections and Operational Insights Based on a Large Cases Study. Diagnostics 2022, 12, 1986. https://doi.org/10.3390/diagnostics12081986
Maiese A, Ciallella C, dell’Aquila M, De Matteis A, Toni C, Scatena A, La Russa R, Mezzetti E, Di Paolo M, Turillazzi E, et al. Cause of Death in Charred Bodies: Reflections and Operational Insights Based on a Large Cases Study. Diagnostics. 2022; 12(8):1986. https://doi.org/10.3390/diagnostics12081986
Chicago/Turabian StyleMaiese, Aniello, Costantino Ciallella, Massimiliano dell’Aquila, Alessandra De Matteis, Chiara Toni, Andrea Scatena, Raffaele La Russa, Eleonora Mezzetti, Marco Di Paolo, Emanuela Turillazzi, and et al. 2022. "Cause of Death in Charred Bodies: Reflections and Operational Insights Based on a Large Cases Study" Diagnostics 12, no. 8: 1986. https://doi.org/10.3390/diagnostics12081986